
A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
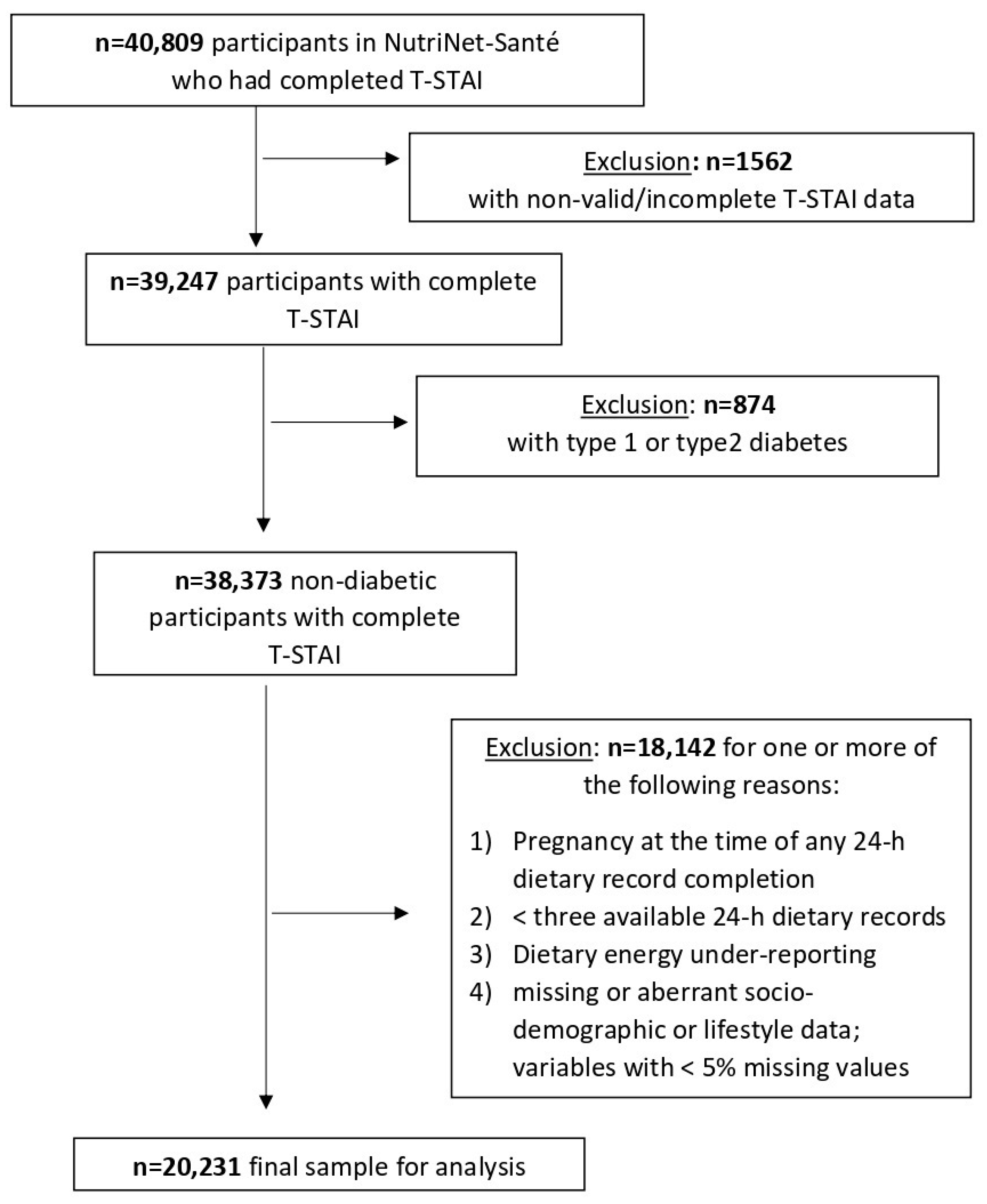
2.1. Study Population
2.2. Sugar Intake
2.3. Trait Anxiety
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Description of the Study Population
3.2. Comparison of Sugar Intake Across Trait Anxiety Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Remes, O.; Brayne, C.; van der Linde, R.; LaFortune, L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 2016, 6, e00497. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analy-sis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialog. Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef]
- Tully, P.J.; Harrison, N.J.; Cheung, P.; Cosh, S. Anxiety and cardiovascular disease risk: A review. Curr. Cardiol. Rep. 2016, 18, 120. [Google Scholar] [CrossRef]
- Saghafian, F.; Malmir, H.; Saneei, P.; Keshteli, A.H.; Hosseinzadeh-Attar, M.J.; Afshar, H.; Siassi, F.; Esmaillzadeh, A.; Adibi, P. Consumption of fruit and vegetables in relation with psychological disorders in Iranian adults. Eur. J. Nutr. 2018, 57, 2295–2306. [Google Scholar] [CrossRef]
- Wu, S.; Fisher-Hoch, S.P.; Reininger, B.M.; McCormick, J.B. Association between fruit and vegetable intake and symptoms of mental health conditions in Mexican Americans. Health Psychol. 2018, 37, 1059–1066. [Google Scholar] [CrossRef]
- Hosseinzadeh, M.; Vafa, M.; Esmaillzadeh, A.; Feizi, A.; Majdzadeh, R.; Afshar, H.; Keshteli, A.H.; Adibi, P. Empirically derived dietary patterns in relation to psychological disorders. Public Health Nutr. 2016, 19, 204–217. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Mykletun, A.; Berk, M.; Bjelland, I.; Tell, G.S. The association between habitual diet quality and the common mental disorders in community-dwelling adults. Psychosom. Med. 2011, 73, 483–490. [Google Scholar] [CrossRef]
- Mörkl, S.; Wagner-Skacel, J.; Lahousen, T.; Lackner, S.; Holasek, S.J.; Bengesser, S.A.; Painold, A.; Holl, A.K.; Reininghaus, E. The role of nutrition and the gut-brain axis in psychiatry: A review of the literature. Neuropsychobiology 2018, 79, 80–88. [Google Scholar] [CrossRef]
- Tsenkova, V.K.; Albert, M.A.; Georgiades, A.; Ryff, C.D. Trait anxiety and glucose metabolism in people without diabetes: Vulnerabilities among black women. Diabet. Med. 2012, 29, 803–806. [Google Scholar] [CrossRef] [Green Version]
- Knüppel, A.; Shipley, M.J.; Llewellyn, C.H.; Brunner, E.J. Sugar intake from sweet food and beverages, common mental disorder and depression: Prospective findings from the Whitehall II study. Sci. Rep. 2017, 7, 6287. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Villegas, A.; Zazpe, I.; Santiago, S.; Perez-Cornago, A.; Martinez-Gonzalez, M.A.; Lahortiga-Ramos, F. Added sugars and sugar-sweetened beverage consumption, dietary carbohydrate index and depression risk in the Seguimiento Universidad de Navarra (SUN) Project. Br. J. Nutr. 2018, 119, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Gangwisch, J.E.; Hale, L.; Garcia, L.; Malaspina, L.; Opler, M.G.; Payne, M.E.; Rossom, R.C.; Lane, R. High glycemic index diet as a risk factor for depression: Analyses from the Women’s Health Initiative. Am. J. Clin. Nutr. 2015, 102, 454–463. [Google Scholar] [CrossRef] [Green Version]
- Moffitt, T.E.; Harrington, H.; Caspi, A.; Kim-Cohen, J.; Goldberg, D.; Gregory, A.M.; Poulton, R. Depression and generalized anxiety disorder. Arch. Gen. Psychiatry 2007, 64, 651–660. [Google Scholar] [CrossRef]
- Liu, S.; Manson, J.E.; Buring, J.E.; Stampfer, M.J.; Willett, W.C.; Ridker, P.M. Relation between a diet with a high glycemic load and plasma concentrations of high-sensitivity C-reactive protein in middle-aged women. Am. J. Clin. Nutr. 2002, 75, 492–498. [Google Scholar] [CrossRef]
- Capuron, L.; Miller, A.H. Immune system to brain signaling: Neuropsychopharmacological implications. Pharmacol. Ther. 2011, 130, 226–238. [Google Scholar] [CrossRef] [Green Version]
- Ulrich-Lai, Y.M. Self-medication with sucrose. Curr. Opin. Behav. Sci. 2016, 9, 78–83. [Google Scholar] [CrossRef] [Green Version]
- Freeman, C.R.; Zehra, A.; Ramirez, V.; Wiers, C.E.; Volkow, N.D.; Wang, G.J. Impact of sugar on the body brain and behavior. Front. Biosci. 2018, 23, 2255–2266. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, X.; Xiao, Y.; Jing, D.; Huang, Y.; Chen, L.; Luo, D.; Chen, X.; Shen, M. Daily intake of soft drinks is associated with symptoms of anxiety and depression in Chinese adolescents. Public Health Nutr. 2019, 22, 2553–2560. [Google Scholar] [CrossRef]
- Masana, M.F.; Tyrovolas, S.; Kollia, N.; Chrysohoou, C.; Skoumas, J.; Haro, J.M.; Tousoulis, D.; Papageorgiou, C.; Pitsavos, C.; Panagiotakos, D.B. Dietary patterns and their association with anxiety symptoms among older adults: The ATTICA study. Nutrients 2019, 11, 1250. [Google Scholar] [CrossRef] [Green Version]
- Wattick, R.A.; Hagedorn, R.L.; Olfert, M.D. Relationship between diet and mental health in a young adult Appalachian college population. Nutrients 2018, 10, 957. [Google Scholar] [CrossRef] [Green Version]
- Haghighatdoost, F.; Azadbakht, L.; Keshteli, A.H.; Feinle-Bisset, C.; Daghaghzadeh, H.; Afshar, H.; Feizi, A.; Esmaillzadeh, A.; Adibi, P. Glycemic index, glycemic load, and common psychological disorders. Am. J. Clin. Nutr. 2016, 103, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Hercberg, S.; Castetbon, K.; Czernichow, S.; Malon, A.; Méjean, C.; Kesse, E.; Touvier, M.; Galan, P. The NutriNet-Santé study: A web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health 2010, 10, 242. [Google Scholar] [CrossRef]
- Touvier, M.; Kesse-Guyot, E.; Méjean, C.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Comparison between an interactive web-based self-administered 24 h dietary record and an interview by a dietitian for large-scale epidemiological studies. Br. J. Nutr. 2011, 105, 1055–1064. [Google Scholar] [CrossRef]
- Lassale, C.; Castetbon, K.; Laporte, F.; Deschamps, V.; Vernay, M.; Camilleri, G.M.; Faure, P.; Hercberg, S.; Galan, P.; Kesse-Guyot, E. Correlations between fruit, vegetables, fish, vitamins, and fatty acids estimated by web-based nonconsecutive dietary records and respective biomarkers of nutritional status. J. Acad. Nutr. Diet. 2016, 116, 427–438.e5. [Google Scholar] [CrossRef]
- Le Moullec, N.; Deheeger, M.; Hercberg, S.; Preziosi, P.; Monteiro, P. Validation du manuel photos utilisées pour l’enquête alimentaire de l’étude SU.VI.MAX [Validation of the photo manual used for the food survey of the SU.VI.MAX study]. Cah. Nutr. Diet. 1996, 31, 158–164. [Google Scholar]
- NutriNet-Santé, E. Table de Composition des Aliments [Food Composition Table]; Economica: Paris, France, 2013. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake/basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Chambers, J.A.; Power, K.G.; Durham, R.C. The relationship between trait vulnerability and anxiety and depressive diagnoses at long-term follow-up of generalized anxiety disorder. J. Anxiety Disord. 2004, 18, 587–607. [Google Scholar] [CrossRef]
- Langevin, V.; Boini, S.; François, M.; Riou, A. Inventaire d’anxiété état-trait forme Y [State-Trait Anxiety Inventory (STAI-Y)]. Ref. Sante Trav. 2012, 131, 161–164. [Google Scholar]
- Harrison, L.K.; Turpin, G. Implicit memory bias and trait anxiety: A psychophysiological analysis. Biol. Psychol. 2003, 62, 97–114. [Google Scholar] [CrossRef]
- Vergnaud, A.C.; Touvier, M.; Méjean, C.; Kesse-Guyot, E.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Agreement between web-based and paper versions of a socio-demographic questionnaire in the nutrinet-santé study. Int. J. Public Health 2011, 56, 407–417. [Google Scholar] [CrossRef]
- International Physical Activity Questionnaire Group. IPAQ Scoring Protocol. Available online: http://www.ipaq.ki.se (accessed on 30 April 2021).
- Touvier, M.; Méjean, C.; Kesse-Guyot, E.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Comparison between web-based and paper versions of a self-administered anthropometric questionnaire. Eur. J. Epidemiol. 2010, 25, 287–296. [Google Scholar] [CrossRef] [Green Version]
- Andreeva, V.A.; Deschamps, V.; Salanave, B.; Castetbon, K.; Verdot, C.; Kesse-Guyot, E.; Hercberg, S. Comparison of the socio-demographic characteristics of the large NutriNet-Santé e-cohort with French Census data: The issue of volunteer bias revisited. J. Epidemiol. Community Health 2016, 69, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Dubé, L.; Lebel, J.L.; Lü, J. Affect asymmetry and comfort food consumption. Physiol. Behav. 2005, 86, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Kadel, P.; Schneider, S.; Mata, J. Soft drink consumption and mental health problems: Longitudinal relations in children and adolescents. Soc. Sci. Med. 2020, 258, 113123. [Google Scholar] [CrossRef] [PubMed]
- Di Rienzi, S.C.; Britton, R.A. Adaptation of the gut microbiota to modern dietary sugars and sweeteners. Adv. Nutr. 2020, 11, 616–629. [Google Scholar] [CrossRef] [Green Version]
- Strandwitz, P. Neurotransmitter modulation by the gut microbiota. Brain Res. 2018, 1693 Pt B, 128–133. [Google Scholar] [CrossRef]


{kind=link}
| Full Sample n = 20,231 | Low Trait Anxiety (T-STAI < 40) n = 12,289 | High Trait Anxiety (T-STAI ≥ 40) n = 7942 | p Value 1 | ||||
|---|---|---|---|---|---|---|---|
| T-STAI score 2, mean (SD) | 37.9 | (10.0) | 31.4 | (5.2) | 48.0 | (6.9) | <0.0001 |
| Sex | <0.0001 | ||||||
| Male | 5198 | (25.7) | 3782 | (30.8) | 1416 | (17.8) | |
| Female | 15,033 | (74.3) | 8507 | (69.2) | 6526 | (82.2) | |
| Age, years, mean (SD) | 53.7 | (13.6) | 55.1 | (13.3) | 51.6 | (13.9) | <0.0001 |
| Age category | <0.0001 | ||||||
| <35 y | 2358 | (11.7) | 1181 | (9.6) | 1177 | (14.8) | |
| 35–54 y | 7109 | (35.1) | 4036 | (32.8) | 3073 | (38.7) | |
| 55–64 y | 5472 | (27.0) | 3441 | (28.0) | 2031 | (25.6) | |
| ≥65 y | 5292 | (26.2) | 3631 | (29.6) | 1661 | (20.9) | |
| Educational level | 0.80 | ||||||
| Less than high school | 2908 | (14.4) | 1755 | (14.3) | 1153 | (14.5) | |
| High school diploma or equivalent | 3586 | (17.7) | 2188 | (17.8) | 1398 | (17.6) | |
| College, undergraduate degree | 5461 | (27.0) | 3286 | (26.7) | 2175 | (27.4) | |
| Graduate degree | 6988 | (34.5) | 4271 | (34.8) | 2717 | (34.2) | |
| Not reported | 1288 | (6.4) | 789 | (6.4) | 499 | (6.3) | |
| Socio-professional category | <0.0001 | ||||||
| Homemaker/disabled/ | 2255 | (11.2) | 1157 | (9.4) | 1098 | (13.8) | |
| unemployed/student/trainee | 6726 | (33.3) | 3802 | (30.9) | 2924 | (36.8) | |
| Manual/blue collar/office | 4714 | (23.3) | 2909 | (23.7) | 1805 | (22.7) | |
| Professional/executive staff Retired | 6536 | (32.3) | 4421 | (36.0) | 2115 | (26.6) | |
| Marital status | <0.0001 | ||||||
| Living alone (single, divorced, widowed) | 4827 | (23.9) | 2716 | (22.1) | 2116 | (26.6) | |
| Married/cohabiting | 15,404 | (76.1) | 9573 | (77.9) | 5831 | (73.4) | |
| Physical activity 3 | <0.0001 | ||||||
| Low | 3588 | (17.7) | 2001 | (16.3) | 1587 | (20.0) | |
| Moderate | 7541 | (37.3) | 4549 | (37.0) | 2992 | (37.7) | |
| High | 6589 | (17.7) | 4354 | (35.4) | 2236 | (28.1) | |
| Not reported | 2513 | (12.4) | 1385 | (11.3) | 1128 | (14.2) | |
| Body Mass Index (BMI,kg/m2), mean (SD) | 23.6 | (3.9) | 23.7 | (3.7) | 23.4 | (4.1) | <0.0001 |
| BMI category | <0.0001 | ||||||
| Underweight (<18.5) | 917 | (4.5) | 455 | (3.7) | 462 | (5.8) | |
| Normal weight (18.5–24.9) | 13,401 | (66.2) | 8171 | (66.5) | 5230 | (65.9) | |
| Overweight (25.0–29.9) | 4693 | (23.2) | 2945 | (24.0) | 1748 | (22.0) | |
| Obese (≥30) | 1220 | (6.0) | 718 | (5.8) | 502 | (6.3) | |
| Smoking status | <0.0001 | ||||||
| Never smoker | 10,234 | (50.6) | 6098 | (49.6) | 4136 | (52.1) | |
| Former smoker | 7867 | (38.9) | 4993 | (40.6) | 2874 | (36.2) | |
| Current smoker | 2130 | (10.5) | 1198 | (9.8) | 932 | (11.7) | |
| Alcohol use,g ethanol/d, mean (SD) | 8.5 | (11.5) | 9.1 | (11.9) | 7.5 | (10.8) | <0.0001 |
| Total energy intake,Kcal/d, mean (SD) | 1910.5 | (441.5) | 1933.5 | (449.0) | 1874.9 | (427.1) | <0.0001 |
| Number of 24-h dietary record, mean (SD) | 7.0 | (2.8) | 7.1 | (2.8) | 6.8 | (2.8) | <0.0001 |
| Model 1 1 | Model 2 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T-STAI 3 < 40 | T-STAI 3 ≥ 40 | p Value | T-STAI 3 < 40 | T-STAI 3 ≥ 40 | p Value | |||||
| n = 2902 | n = 2598 | n = 2902 | n = 2598 | |||||||
| LSmean | SE | LSmean | SE | LSmean | SE | LSmean | SE | |||
| Percentage energy from carbohydrates | 42.05 | 0.11 | 42.19 | 0.12 | 0.40 | 42.57 | 0.81 | 42.71 | 0.81 | 0.36 |
| Total carbohydrates (g/d) | 198.86 | 0.53 | 199.30 | 0.56 | 0.58 | 201.71 | 3.78 | 202.16 | 3.80 | 0.53 |
| Complex carbohydrates (g/d) | 104.54 | 0.43 | 104.49 | 0.45 | 0.94 | 105.53 | 3.28 | 105.54 | 3.31 | 0.97 |
| Simple sugars (g/d) | 93.73 | 0.43 | 94.21 | 0.45 | 0.50 | 95.60 | 3.15 | 96.03 | 3.17 | 0.46 |
| Added simple sugars (g/d) | 41.40 | 0.33 | 43.15 | 0.35 | 0.0003 | 42.33 | 2.50 | 43.92 | 2.51 | 0.0007 |
| Sweet food/beverage group (g/d) | 429.08 | 3.02 | 427.08 | 3.19 | 0.65 | 398.28 | 22.85 | 396.31 | 22.97 | 0.64 |
| Sweet food/beverage group except fresh fruit (g/d) | 272.69 | 2.52 | 274.40 | 2.67 | 0.46 | 248.36 | 19.45 | 250.43 | 19.55 | 0.57 |
| Fresh fruit (g/d) | 157.39 | 2.36 | 152.67 | 2.50 | 0.17 | 149.92 | 18.14 | 145.88 | 18.24 | 0.23 |
| Model 1 1 | Model 2 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T-STAI 3 < 40 | T-STAI 3 ≥ 40 | p Value | T-STAI 3 < 40 | T-STAI 3 ≥ 40 | p Value | |||||
| n = 9387 | n = 5344 | n = 9387 | n = 5344 | |||||||
| LSmean | SE | LSmean | SE | LSmean | SE | LSmean | SE | |||
| Percentage energy from carbohydrates | 40.88 | 0.07 | 41.06 | 0.09 | 0.11 | 41.09 | 0.09 | 41.23 | 0.11 | 0.15 |
| Total carbohydrates (g/d) | 195.83 | 0.33 | 196.40 | 0.44 | 0.30 | 196.73 | 0.45 | 197.04 | 0.51 | 0.51 |
| Complex carbohydrates (g/d) | 102.32 | 0.26 | 103.22 | 0.34 | 0.04 | 104.23 | 0.40 | 104.91 | 0.45 | 0.10 |
| Simple sugars (g/d) | 92.92 | 0.25 | 92.59 | 0.33 | 0.43 | 91.93 | 0.37 | 91.55 | 0.42 | 0.32 |
| Added simple sugars (g/d) | 35.02 | 0.17 | 35.61 | 0.23 | 0.04 | 35.12 | 0.27 | 35.56 | 0.31 | 0.12 |
| Sweet food/beverage group (g/d) | 427.80 | 1.69 | 421.55 | 2.25 | 0.03 | 420.08 | 2.59 | 414.06 | 2.94 | 0.03 |
| Sweet food/beverage group except fresh fruit (g/d) | 200.32 | 1.14 | 200.30 | 1.52 | 0.99 | 200.53 | 1.81 | 200.10 | 2.05 | 0.82 |
| Fresh fruit (g/d) | 227.48 | 1.46 | 221.25 | 1.95 | 0.01 | 219.54 | 2.29 | 213.97 | 2.59 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kose, J.; Cheung, A.; Fezeu, L.K.; Péneau, S.; Debras, C.; Touvier, M.; Hercberg, S.; Galan, P.; Andreeva, V.A. A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study. Nutrients 2021, 13, 1526. https://doi.org/10.3390/nu13051526
Kose J, Cheung A, Fezeu LK, Péneau S, Debras C, Touvier M, Hercberg S, Galan P, Andreeva VA. A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study. Nutrients. 2021; 13(5):1526. https://doi.org/10.3390/nu13051526
Chicago/Turabian StyleKose, Junko, Adrienne Cheung, Léopold K. Fezeu, Sandrine Péneau, Charlotte Debras, Mathilde Touvier, Serge Hercberg, Pilar Galan, and Valentina A. Andreeva. 2021. "A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study" Nutrients 13, no. 5: 1526. https://doi.org/10.3390/nu13051526
APA StyleKose, J., Cheung, A., Fezeu, L. K., Péneau, S., Debras, C., Touvier, M., Hercberg, S., Galan, P., & Andreeva, V. A. (2021). A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study. Nutrients, 13(5), 1526. https://doi.org/10.3390/nu13051526