
Detraining Effects on Muscle Quality in Older Men with Osteosarcopenia. Follow-Up of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST)

 ,
, 
Abstract
:1. Introduction
2. Methods
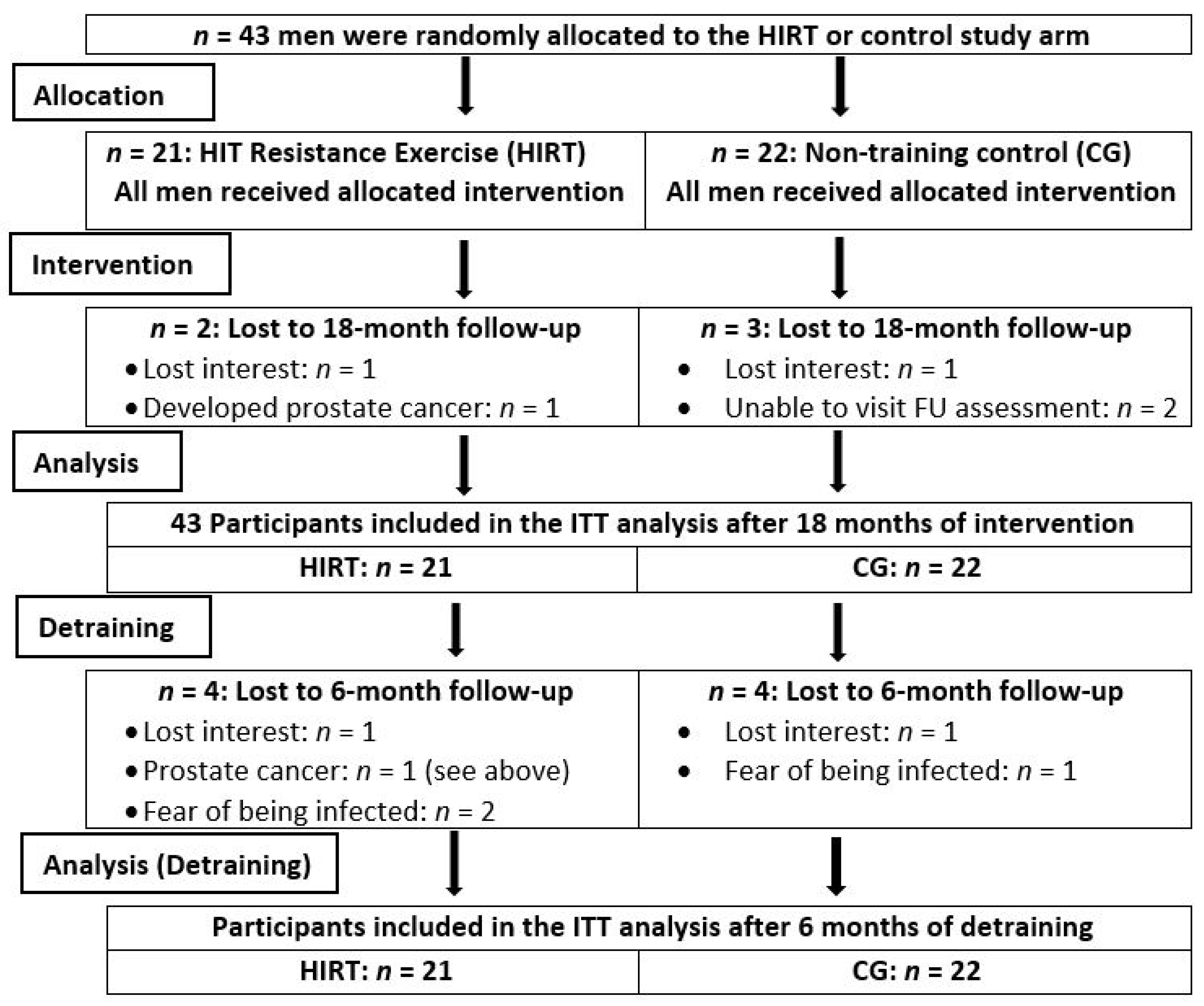
2.1. Participants
2.2. Randomization and Blinding Procedures
2.3. Training and Detraining
2.4. Supplements
2.5. Study Outcomes
2.5.1. Primary Study Outcome
- Muscle quality, defined as maximum hip/leg extensor strength (MILES) per unit of mid-thigh intra-fascia volume as determined by MRI during detraining.
2.5.2. Secondary Study Outcome
- Muscle quality, defined as MILES per unit of thigh muscle mass as determined by DXA during detraining.
2.6. Assessments
2.7. Isokinetic Strength Testing
2.8. Body Composition and Muscle Quality
2.9. Statistical Analysis
3. Results
3.1. Study Outcomes
3.2. Confounding Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Beckwee, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.J.; Liao, C.D.; Tsai, M.W.; Chen, C.N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Morley, J.E.; Schols, A.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; et al. Sarcopenia: A Time for Action. An SCWD Position Paper. J. Cachexia Sarcopenia Muscle 2019, 10, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Eichberg, S.; Rott, C. Sportverhalten im mittleren und höheren Erwachsenenalter. J. Public Health 2004, 12, 93–104. [Google Scholar] [CrossRef]
- Hakkinen, K.; Alen, M.; Kallinen, M.; Newton, R.U.; Kraemer, W.J. Neuromuscular adaptation during prolonged strength training, detraining and re-strength-training in middle-aged and elderly people. Eur. J. Appl. Physiol. 2000, 83, 51–62. [Google Scholar] [CrossRef]
- Ivey, F.M.; Tracy, B.L.; Lemmer, J.T.; NessAiver, M.; Metter, E.J.; Fozard, J.L.; Hurley, B.F. Effects of strength training and detraining on muscle quality: Age and gender comparisons. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, B152–B157. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, M.J.; Marques, E.; Mota, J. Training and detraining effects on functional fitness after a multicomponent training in older women. Gerontology 2009, 55, 41–48. [Google Scholar] [CrossRef]
- Harris, C.; DeBeliso, M.; Adams, K.J.; Irmischer, B.S.; Spitzer Gibson, T.A. Detraining in the older adult: Effects of prior training intensity on strength retention. J. Strength Cond. Res. 2007, 21, 813–818. [Google Scholar] [CrossRef]
- Kemmler, W.; Kohl, M.; Frohlich, M.; Schoene, D.; von Stengel, S. Detraining effects after 18 months of high intensity resistance training on osteosarcopenia in older men-Six-month follow-up of the randomized controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). Bone 2021, 142, 115772. [Google Scholar] [CrossRef]
- Cederholm, T.E.; Bauer, J.M.; Boirie, Y.; Schneider, S.M.; Sieber, C.C.; Rolland, Y. Toward a definition of sarcopenia. Clin. Geriatr Med. 2011, 27, 341–353. [Google Scholar] [CrossRef]
- Barbat-Artigas, S.; Rolland, Y.; Zamboni, M.; Aubertin-Leheudre, M. How to assess functional status: A new muscle quality index. J. Nutr. Health Aging 2012, 16, 67–77. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of sarcopenia: Old evidence and new insights. Eur. Radiol. 2020, 30, 2199–2208. [Google Scholar] [CrossRef]
- Reginster, J.Y.; Beaudart, C.; Buckinx, F.; Bruyere, O. Osteoporosis and sarcopenia: Two diseases or one? Curr Opin Clin Nutr Metab Care 2016, 19, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemmler, W.; Kohl, M.; Frohlich, M.; Engelke, K.; von Stengel, S.; Schoene, D. Effects of High-Intensity Resistance Training on Fitness and Fatness in Older Men With Osteosarcopenia. Front. Physiol. 2020, 11, 1014. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of A WHO Study Group; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Steele, J.; Fisher, J.; Giessing, J.; Gentil, P. Clarity in Reporting Terminology and Definitions of Set End Points in Resistance Training. Muscle Nerve 2017, 56, 368–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenberg, T.; von Stengel, S.; Sieber, C.; Kemmler, W. The favorable effects of a high-intensity resistance training on sarcopenia in older community-dwelling men with osteosarcopenia: The randomized controlled FrOST study. Clin. Interv. Aging 2019, 14, 2173–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemmler, W.; Kohl, M.; Frohlich, M.; Jakob, F.; Engelke, K.; von Stengel, S.; Schoene, D. Effects of High Intensity Resistance Training on Osteopenia and Sarcopenia parameters in Older Men with Osteosarcopenia—One-year results of the randomized controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). J. Bone Miner. Res. 2020, 35, 1634–1644. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Kohl, M.; Jakob, F.; Engelke, K.; von Stengel, S. Effects of High Intensity Dynamic Resistance Exercise and Whey Protein Supplements on Osteosarcopenia in Older Men with Low Bone and Muscle Mass. Final Results of the Randomized Controlled FrOST Study. Nutrients 2020, 12, 2341. [Google Scholar] [CrossRef]
- Kemmler, W.; Bebenek, M.; von Stengel, S.; Bauer, J. Peak-bone-mass development in young adults: Effects of study program related levels of occupational and leisure time physical activity and exercise. A prospective 5-year study. Osteoporos. Int. 2015, 26, 653–662. [Google Scholar] [CrossRef]
- Kemmler, W.; Weineck, J.; Kalender, W.A.; Engelke, K. The effect of habitual physical activity, non-athletic exercise, muscle strength, and VO2max on bone mineral density is rather low in early postmenopausal osteopenic women. J. Musculoskelet. Neuronal Interact. 2004, 4, 325–334. [Google Scholar] [PubMed]
- Chaudry, O.; Friedberger, A.; Grimm, A.; Uder, M.; Nagel, A.M.; Kemmler, W.; Engelke, K. Segmentation of the fascia lata and reproducible quantification of intermuscular adipose tissue (IMAT) of the thigh. Magn. Reson. Mater. Phys. Biol. Med. 2020. [Google Scholar] [CrossRef]
- Honaker, J.; King, G.; Blackwell, M. Amelia II: A program for missing data. J. Stat. Softw. 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Correa, C.S.; Baroni, B.M.; Radaelli, R.; Lanferdini, F.J.; Cunha Gdos, S.; Reischak-Oliveira, A.; Vaz, M.A.; Pinto, R.S. Effects of strength training and detraining on knee extensor strength, muscle volume and muscle quality in elderly women. Age 2013, 35, 1899–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weineck, J. Optimales Trainin; Spitta: Erlangen-Nürnberg, Germany, 2019. [Google Scholar]
- Fatouros, I.G.; Kambas, A.; Katrabasas, I.; Nikolaidis, K.; Chatzinikolaou, A.; Leontsini, D.; Taxildaris, K. Strength training and detraining effects on muscular strength, anaerobic power, and mobility of inactive older men are intensity dependent. Br. J. Sports Med. 2005, 39, 776–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemikaram, M.; Chaudry, O.; Nagel, A.M.; Uder, M.; Jakob, F.; Kemmler, W.; Kohl, M.; Engelke, K. Effects of 16 months of high intensity resistance training on thigh muscle fat infiltration in elderly men with osteosarcopenia. Geroscience 2021. [Google Scholar] [CrossRef]
- Blocquiaux, S.; Gorski, T.; Van Roie, E.; Ramaekers, M.; Van Thienen, R.; Nielens, H.; Delecluse, C.; De Bock, K.; Thomis, M. The effect of resistance training, detraining and retraining on muscle strength and power, myofibre size, satellite cells and myonuclei in older men. Exp. Gerontol. 2020, 133, 110860. [Google Scholar] [CrossRef]
- Henwood, T.R.; Taaffe, D.R. Detraining and retraining in older adults following long-term muscle power or muscle strength specific training. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 751–758. [Google Scholar] [CrossRef] [Green Version]
- Snijders, T.; Leenders, M.; de Groot, L.; van Loon, L.J.C.; Verdijk, L.B. Muscle mass and strength gains following 6 months of resistance type exercise training are only partly preserved within one year with autonomous exercise continuation in older adults. Exp. Gerontol. 2019, 121, 71–78. [Google Scholar] [CrossRef]


{kind=link}
| Variable | CG (n = 22) MV ± SD | HIRT (n = 21) MV ± SD |
|---|---|---|
| Age (years) | 80.8 ± 4.7 | 79.6 ± 3.6 |
| Body mass index (kg/m2) | 24.6 ± 2.1 | 24.8 ± 3.0 |
| Total body fat (%) | 32.2 ± 5.5 | 33.5± 4.3 |
| More than two diseases (n) | 13 | 9 |
| Metabolic syndrome (n) a | 12 | 9 |
| Diabetes mellitus type II (n) | 1 | 1 |
| Habitual physical activity (Index) b | 4.32 ± 1.44 | 4.51 ± 1.27 |
| Exercise volume (min/week) | 54 ± 56 | 52 ± 50 |
| 25-OHD level (ng/mL) c | 29.6 ± 5.8 | 28.1 ± 5.8 |
| Calcium intake (mg/d) | 852 ± 266 | 827 ± 291 |
| Energy intake (kcal/d) d | 2242 ± 639 | 2197 ± 508 |
| Dietary protein intake (g/kg/d) d | 1.25 ± 0.23 | 1.15 ± 0.27 |
| Baseline (SE) | Δ Training a (SE) | Δ Detraining b (SE) | Δ Overall a (SE) | ||
|---|---|---|---|---|---|
| MILES/intra-fascia volume (N/cm3) | CG | 1.55 (0.07) | 0.01 (0.05) | 0.04 (0.04) | 0.05 (0.04) |
| HIRT | 1.47 (0.11) | 0.49 (0.05) | −0.18 (0.05) | 0.30 (0.05) | |
| p | 0.54 | 0.001 | 0.001 | 0.004 | |
| MILES/thigh LBM (N/kg) | CG | 195 (10) | 1.8 (4.8) | 0.5 (3.2) | 2.2 (2.9) |
| HIRT | 176 (13) | 50.5 (4.6) | −14.0 (3.8) | 36.5 (5.1) | |
| p | 0.25 | 0.001 | 0.001 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghasemikaram, M.; Engelke, K.; Kohl, M.; von Stengel, S.; Kemmler, W. Detraining Effects on Muscle Quality in Older Men with Osteosarcopenia. Follow-Up of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). Nutrients 2021, 13, 1528. https://doi.org/10.3390/nu13051528
Ghasemikaram M, Engelke K, Kohl M, von Stengel S, Kemmler W. Detraining Effects on Muscle Quality in Older Men with Osteosarcopenia. Follow-Up of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). Nutrients. 2021; 13(5):1528. https://doi.org/10.3390/nu13051528
Chicago/Turabian StyleGhasemikaram, Mansour, Klaus Engelke, Matthias Kohl, Simon von Stengel, and Wolfgang Kemmler. 2021. "Detraining Effects on Muscle Quality in Older Men with Osteosarcopenia. Follow-Up of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST)" Nutrients 13, no. 5: 1528. https://doi.org/10.3390/nu13051528
APA StyleGhasemikaram, M., Engelke, K., Kohl, M., von Stengel, S., & Kemmler, W. (2021). Detraining Effects on Muscle Quality in Older Men with Osteosarcopenia. Follow-Up of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). Nutrients, 13(5), 1528. https://doi.org/10.3390/nu13051528