
COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
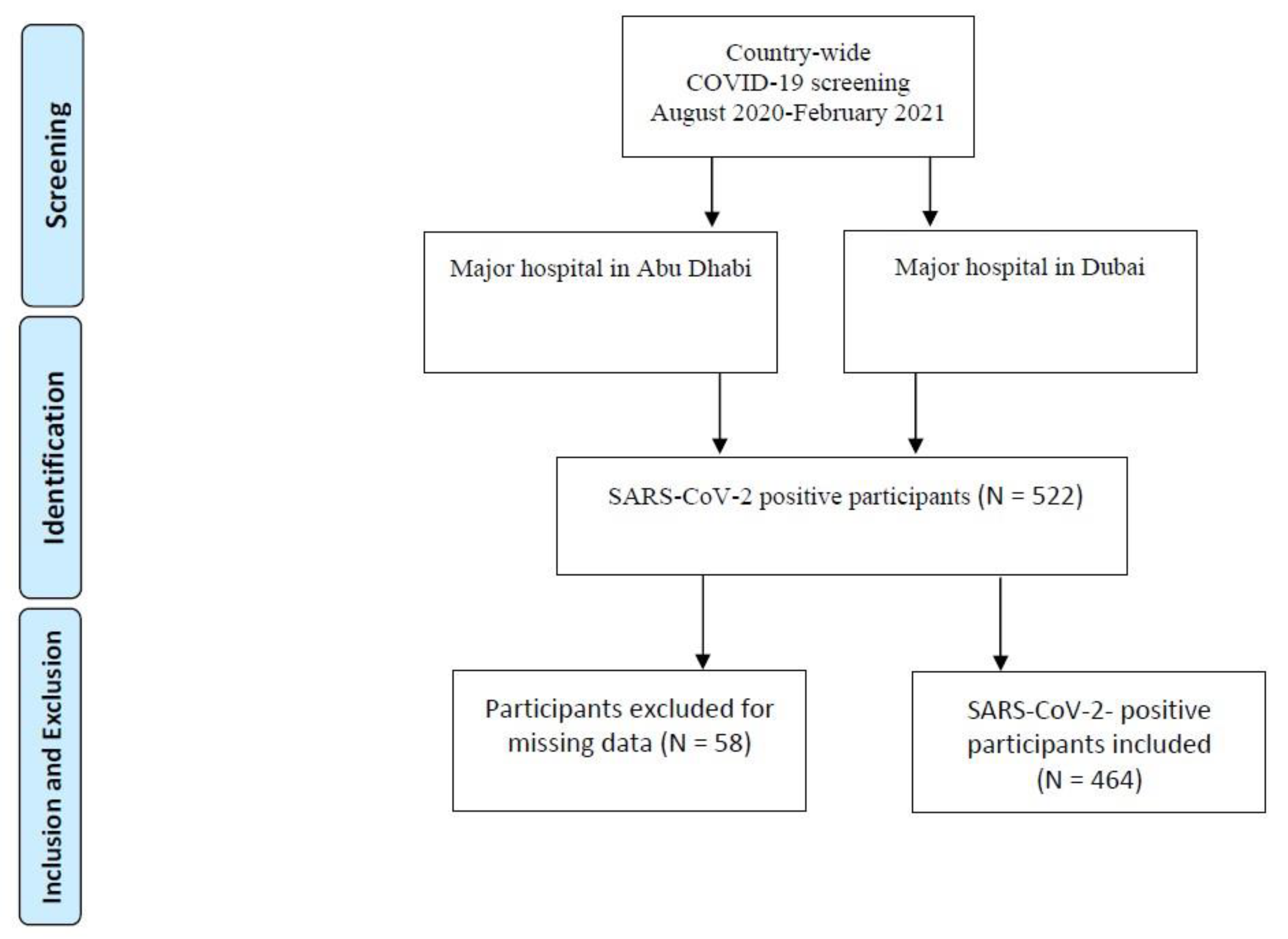
2.1. Participants and Collecting Samples
2.2. Collecting Demographic Data
2.3. Extracting and Quantifying SARS-CoV-2 Viral RNA
2.4. Measuring Serum 25(OH)D Levels
2.5. Defining Severity of Infection
2.6. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussein, T.; Löndahl, J.; Thuresson, S.; Alsved, M.; Al-Hunaiti, A.; Saksela, K.; Aqel, H.; Junninen, H.; Mahura, A.; Kulmala, M. Indoor Model Simulation for COVID-19 Transport and Exposure. Int. J. Environ. Res. Public Health 2021, 18, 2927. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Global epidemic of coronavirus—Covid-19: What can we do to minimize risks. Eur. J. Biomed. Pharm. Sci. 2020, 7, 432–438. [Google Scholar]
- Thompson, R. Pandemic potential of 2019-nCoV. Lancet Infect. Dis. 2020, 20, 280. [Google Scholar] [CrossRef] [Green Version]
- Butt, Y.; Kurdowska, A.; Allen, T.C. Acute Lung Injury: A Clinical and Molecular Review. Arch. Pathol. Lab. Med. 2016, 140, 345–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, K.T.; Beasley, M.B. Pulmonary Manifestations of Acute Lung Injury: More Than Just Diffuse Alveolar Damage. Arch. Pathol. Lab. Med. 2016, 141, 916–922. [Google Scholar] [CrossRef] [Green Version]
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Scali, E.; Patruno, C.; Nisticò, S.P. Role of Vitamins in Skin Health: A Systematic Review. Curr. Nutr. Rep. 2020, 9, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Mercola, J.; Grant, W.B.; Wagner, C.L. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients 2020, 12, 3361. [Google Scholar] [CrossRef]
- Teymoori-Rad, M.; Shokri, F.; Salimi, V.; Marashi, S.M. The interplay between vitamin D and viral infections. Rev. Med. Virol. 2019, 29, e2032. [Google Scholar] [CrossRef]
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466. [Google Scholar] [CrossRef]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Dastoli, S.; Bennardo, L.; Patruno, C.; Nisticò, S.P. Are erythema multiforme and urticaria related to a better outcome of COVID-19? Dermatol. Ther. 2020, 33, e13681. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Kenny, R.A. Editorial: Low population mortality from COVID-19 in countries south of latitude 35 degrees North supports vitamin D as a factor determining severity. Aliment. Pharmacol. Ther. 2020, 51, 1434–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordelon, P.; Ghetu, M.V.; Langan, R.C. Recognition and management of vitamin D deficiency. Am. Fam. Physician 2009, 80, 841–846. [Google Scholar]
- Watkins, R.R.; Lemonovich, T.L.; Salata, R.A. An update on the association of vitamin D deficiency with common infectious diseases. Can. J. Physiol. Pharmacol. 2015, 93, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Science, M.; Maguire, J.L.; Russell, M.L.; Smieja, M.; Walter, S.D.; Loeb, M. Low serum 25-hydroxyvitamin D level and risk of upper respiratory tract infection in children and adolescents. Clin. Infect. Dis. 2013, 57, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glinsky, G.V. Tripartite combination of candidate pandemic mitigation agents: Vitamin D, quercetin, and estradiol manifest properties of medicinal agents for targeted mitigation of the COVID-19 pandemic defined by genomics-guided tracing of SARS-CoV-2 targets in human cells. Biomedicines 2020, 8, 129. [Google Scholar]
- Gois, P.H.F.; Ferreira, D.; Olenski, S.; Seguro, A.C. Vitamin D and Infectious Diseases: Simple Bystander or Contributing Factor? Nutrients 2017, 9, 651. [Google Scholar] [CrossRef] [Green Version]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. In Proceedings of the Mayo Clinic Proceedings; Elsevier BV: Amsterdam, The Netherlands, 2013; Volume 88, pp. 720–755. [Google Scholar]
- Kuba, K.; Imai, Y.; Penninger, J.M. Angiotensin-converting enzyme 2 in lung diseases. Curr. Opin. Pharmacol. 2006, 6, 271–276. [Google Scholar] [CrossRef]
- Rodríguez-Puertas, R. ACE2 activators for the treatment of COVID 19 patients. J. Med. Virol. 2020, 92, 1701–1702. [Google Scholar] [CrossRef]
- Xudong, X.; Junzhu, C.; Xingxiang, W.; Furong, Z.; Yanrong, L. Age- and gender-related difference of ACE2 expression in rat lung. Life Sci. 2006, 78, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Ilie, P.C.; Stefanescu, S.; Smith, L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin. Exp. Res. 2020, 32, 1195–1198. [Google Scholar] [CrossRef]
- Sasabe, J.; Suzuki, M.; Imanishi, N.; Aiso, S. Activity of D-amino acid oxidase is widespread in the human central nervous system. Front. Synaptic Neurosci. 2014, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Castillo, M.E.; Costa, L.M.E.; Barrios, J.M.V.; Díaz, J.F.A.; Miranda, J.L.; Bouillon, R.; Gomez, J.M.Q. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Charoenngam, N.; Shirvani, A.; Reddy, N.; Vodopivec, D.M.; Apovian, C.M.; Holick, M.F. Association of Vitamin D Status With Hospital Morbidity and Mortality in Adult Hospitalized Patients With COVID-19. Endocr. Pr. 2021, 27, 271–278. [Google Scholar] [CrossRef]
- Braun, A.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Liu, Y.; Giovannucci, E.; Christopher, K.B. Association of low serum 25-hydroxyvitamin D levels and mortality in the critically ill. Crit. Care Med. 2011, 39, 671–677. [Google Scholar] [CrossRef] [Green Version]
- De Haan, K.; Groeneveld, A.J.; de Geus, H.R.; Egal, M.; Struijs, A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: Systematic review and meta-analysis. Crit. Care 2014, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.A.; Bearden, A.; Striker, R. Vitamin D and the anti-viral state. J. Clin. Virol. 2011, 50, 194–200. [Google Scholar] [CrossRef]
- Gunville, C.F.; Mourani, P.M.; Ginde, A.A. The role of vitamin D in prevention and treatment of infection. Inflamm. Allergy-Drug Targets 2013, 12, 239–245. [Google Scholar] [CrossRef]
- Graham, B.S. Rapid COVID-19 vaccine development. Science 2020, 368, 945–946. [Google Scholar] [CrossRef]
- Alanouti, F.; Thomas, J.; Abdel-Wareth, L.; Rajah, J.; Grant, W.B.; Haq, A. Vitamin D deficiency and sun avoidance among university students at Abu Dhabi, United Arab Emirates. Dermato-Endocrinol. 2011, 3, 235–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haq, A.; Svobodová, J.; Imran, S.; Stanford, C.; Razzaque, M.S. Vitamin D deficiency: A single centre analysis of patients from 136 countries. J. Steroid Biochem. Mol. Biol. 2016, 164, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drincic, A.T.; Armas, L.A.; van Diest, E.E.; Heaney, R.P. Volumetric Dilution, Rather Than Sequestration Best Explains the Low Vitamin D Status of Obesity. Obesity 2012, 20, 1444–1448. [Google Scholar] [CrossRef] [PubMed]
- Van der Weele, T.J. Principles of confounder selection. Eur. J. Epidemiol. 2019, 34, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System—Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Gröber, U.; Holick, M.F. The coronavirus disease (COVID-19)—A supportive approach with selected micronutrients. Int. J. Vitam. Nutr. Res. 2021, 1–22. [Google Scholar] [CrossRef]
- Rossetti, M.; Martucci, G.; Starchl, C.; Amrein, K. Micronutrients in Sepsis and COVID-19: A Narrative Review on What We Have Learned and What We Want to Know in Future Trials. Medicina 2021, 57, 419. [Google Scholar] [CrossRef]
- Biesalski, H.K. Vitamin D deficiency and co-morbidities in COVID-19 patients—A fatal relationship? NFS J. 2020, 20, 10–21. [Google Scholar] [CrossRef]
- Zierer, J.; Menni, C.; Kastenmüller, G.; Spector, T.D. Integration of ‘omics’ data in aging research: From biomarkers to systems biology. Aging Cell 2015, 14, 933–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jazwinski, S.M.; Yashin, A.I. Aging and health—A systems biology perspective. Introduction. Interdiscip. Top. Gerontol. 2015, 40, VII–XII. [Google Scholar]
- Cohen, A.A. Complex systems dynamics in aging: New evidence, continuing questions. Biogerontology 2016, 17, 205–220. [Google Scholar] [CrossRef] [Green Version]
- Fulop, T.; McElhaney, J.; Pawelec, G.; Cohen, A.A.; Morais, J.A.; Dupuis, G.; Baehl, S.; Camous, X.; Witkowski, J.M.; Larbi, A. Frailty, Inflammation and Immunosenescence. Frailty Aging 2015, 41, 26–40. [Google Scholar]
- Pawelec, G. Does the human immune system ever really become “senescent”? F1000Research 2017, 6. [Google Scholar] [CrossRef]
- Franceschi, C.; Salvioli, S.; Garagnani, P.; de Eguileor, M.; Monti, D.; Capri, M. Immunobiography and the Heterogeneity of Immune Responses in the Elderly: A Focus on Inflammaging and Trained Immunity. Front. Immunol. 2017, 8, 982. [Google Scholar] [CrossRef]
- Xu, W.; Larbi, A. Markers of T Cell Senescence in Humans. Int. J. Mol. Sci. 2017, 18, 1742. [Google Scholar] [CrossRef] [Green Version]
- Goronzy, J.J.; Fang, F.; Cavanagh, M.M.; Fengqin, F.; Weyand, C.M. Naive T Cell Maintenance and Function in Human Aging. J. Immunol. 2015, 194, 4073–4080. [Google Scholar] [CrossRef]
- Yanes, R.E.; Gustafson, C.E.; Weyand, C.M.; Goronzy, J.J. Lymphocyte generation and population homeostasis throughout life. Semin. Hematol. 2017, 54, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Kleinnijenhuis, J.; Quintin, J.; Preijers, F.; Joosten, L.A.B.; Ifrim, D.C.; Saeed, S.; Jacobs, C.; van Loenhout, J.; de Jong, D.; Stunnenberg, H.G.; et al. Bacille Calmette-Guerin induces NOD2-dependent nonspecific protection from reinfection via epigenetic reprogramming of monocytes. Proc. Natl. Acad. Sci. USA 2012, 109, 17537–17542. [Google Scholar] [CrossRef] [Green Version]
- Netea, M.G.; van der Meer, J.W. Trained immunity: An ancient way of remembering. Cell Host Microbe 2017, 21, 297–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fülöp, T., Jr.; Foris, G.; Worum, I.; Leövey, A. Age-dependent alterations of Fc gamma receptor-mediated effector functions of human polymorphonuclear leucocytes. Clin. Exp. Immunol. 1985, 61, 425. [Google Scholar] [PubMed]
- Fülöp, T.; Dupuis, G.; Witkowski, J.M.; Larbi, A. The Role of Immunosenescence in the Development of Age-Related Diseases. Rev. Investig. Clin. 2016, 68, 84–91. [Google Scholar]
- Bayramoğlu, E.; Akkoç, G.; Ağbaş, A.; Akgün, Ö.; Yurdakul, K.; Duru, H.N.S.; Elevli, M. The association between vitamin D levels and the clinical severity and inflammation markers in pediatric COVID-19 patients: Single-center experience from a pandemic hospital. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–7. [Google Scholar] [CrossRef]
- Smolders, J.; Ouweland, J.V.D.; Geven, C.; Pickkers, P.; Kox, M. Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence. Metab. Clin. Exp. 2021, 115, 154434. [Google Scholar] [CrossRef]
- Dalamaga, M.; Christodoulatos, G.S.; Karampela, I.; Vallianou, N.; Apovian, C.M. Understanding the Co-Epidemic of Obesity and COVID-19: Current Evidence, Comparison with Previous Epidemics, Mechanisms, and Preventive and Therapeutic Perspectives. Curr. Obes. Rep. 2021, 1–30. [Google Scholar] [CrossRef]
- Ekiz, T.; Pazarlı, A.C. Relationship between COVID-19 and obesity. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 761–763. [Google Scholar] [CrossRef]
- Hamer, M.; Gale, C.R.; Kivimäki, M.; Batty, G.D. Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc. Natl. Acad. Sci. USA 2020, 117, 21011–21013. [Google Scholar] [CrossRef]
- Sattar, N.; McInnes, I.B.; McMurray, J.J. Obesity is a risk factor for severe COVID-19 infection: Multiple potential mechanisms. Circulation 2020, 142, 4–6. [Google Scholar] [CrossRef]
- Al Saleh, Y.; Beshyah, S.A.; Hussein, W.; Almadani, A.; Hassoun, A.; Al Mamari, A.; Ba-Essa, E.; Al-Dhafiri, E.; Hassanein, M.; Fouda, M.A.; et al. Diagnosis and management of vitamin D deficiency in the Gulf Cooperative Council (GCC) countries: An expert consensus summary statement from the GCC vitamin D advisory board. Arch. Osteoporos. 2020, 15, 1–8. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Kazemi, A.; Mohammadi, V.; Aghababaee, S.K.; Golzarand, M.; Clark, C.C.; Babajafari, S. Association of Vitamin D status with SARS-CoV-2 infection or COVID-19 severity: A systematic review and meta-analysis. Adv. Nutr. 2021. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef]
- Guan, S.P.; Seet, R.C.S.; Kennedy, B.K. Does eNOS derived nitric oxide protect the young from severe COVID-19 complications? Ageing Res. Rev. 2020, 64, 101201. [Google Scholar] [CrossRef]
- Åkerström, S.; Mousavi-Jazi, M.; Klingström, J.; Leijon, M.; Lundkvist, A.; Mirazimi, A. Nitric Oxide Inhibits the Replication Cycle of Severe Acute Respiratory Syndrome Coronavirus. J. Virol. 2005, 79, 1966–1969. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Cader, M.S.; Amarasinghe, A.; Abdul-Careem, M.F. Activation of toll-like receptor signaling pathways leading to nitric oxide-mediated antiviral responses. Arch. Virol. 2016, 161, 2075–2086. [Google Scholar] [CrossRef]
- Andrukhova, O.; Slavic, S.; Zeitz, U.; Riesen, S.C.; Heppelmann, M.S.; Ambrisko, T.D.; Markovic, M.; Kuebler, W.M.; Erben, R.G. Vitamin D Is a Regulator of Endothelial Nitric Oxide Synthase and Arterial Stiffness in Mice. Mol. Endocrinol. 2014, 28, 53–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, R.B.; Wang, Y.; He, J.; Maddux, F.W.; Usvyat, L.; Zhang, H.; Feelisch, M.; Kotanko, P. Does Incident Solar Ultraviolet Radiation Lower Blood Pressure? J. Am. Hear. Assoc. 2020, 9, e013837. [Google Scholar] [CrossRef]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Cohen, A.G.; Green, I.; Frenkel-Morgenstern, M. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693–3702. [Google Scholar] [CrossRef]
- Abrishami, A.; Dalili, N.; Torbati, P.M.; Asgari, R.; Arab-Ahmadi, M.; Behnam, B.; Sanei-Taheri, M. Possible association of vitamin D status with lung involvement and outcome in patients with COVID-19: A retrospective study. Eur. J. Nutr. 2020, 1–9. [Google Scholar] [CrossRef]
- Alguwaihes, A.M.; Sabico, S.; Hasanato, R.; Al-Sofiani, M.E.; Megdad, M.; Albader, S.S.; Alsari, M.H.; Alelayan, A.; Alyusuf, E.Y.; Alzahrani, S.H.; et al. Severe vitamin D deficiency is not related to SARS-CoV-2 infection but may increase mortality risk in hospitalized adults: A retrospective case–control study in an Arab Gulf country. Aging Clin. Exp. Res. 2021, 33, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Amer, O.E.; Alotaibi, N.H.; Aldisi, D.A.; Enani, M.A.; Sheshah, E.; Aljohani, N.J.; Alshingetti, N.; Alomar, S.Y.; Alfawaz, H.; et al. Vitamin D status of Arab Gulf residents screened for SARS-CoV-2 and its association with COVID-19 infection: A multi-centre case-control study. J. Transl. Med. 2021, 19, 1–8. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Baggerly, L.L.; Garland, C.F.; Gorham, E.D.; Hollis, B.W.; Trump, D.L.; Lappe, J.M. Breast cancer risk markedly lower with serum 25-hydroxyvitamin D concentrations ≥60 vs <20 ng/mL (150 vs 50 nmol/L): Pooled analysis of two randomized trials and a prospective cohort. PLoS ONE 2018, 13, e0199265. [Google Scholar] [CrossRef] [Green Version]
- Mirhosseini, N.; Vatanparast, H.; Kimball, S.M. The Association between Serum 25(OH)D Status and Blood Pressure in Participants of a Community-Based Program Taking Vitamin D Supplements. Nutrients 2017, 9, 1244. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Severity | Mortality | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Asymptomatic | Mild | Moderate | High | p | Alive | Deceased | p | |
| Total | 464 | 91 (19.6) | 99 (21.3) | 129 (27.8) | 145 (31.3) | 438 (94.4) | 26 (5.6) | ||
| Age (years) | 46.6 ± 14.9 | 34.3 ± 7.2 | 41.6 ± 13.7 | 49.0 ± 13.0 | 55.7 ± 14.1 | <0.001 | 45.7 ± 14.5 | 62.5 ± 13.1 | <0.001 |
| Sex | |||||||||
| Female | 92 (19.8) | 27 (29.3) | 20 (21.7) | 14 (15.2) | 31 (33.7) | 0.006 | 89 (96.7) | 3 (3.3) | 0.28 |
| Male | 372 (80.2) | 64 (17.2) | 79 (21.2) | 115 (30.9) | 114 (30.6) | 349 (93.8) | 23 (6.2) | ||
| BMI (kg/m2) | 28.1 ± 5.9 | 25.6 ± 4.0 | 27.0 ± 5.4 | 28.3 ± 5.4 | 30.2 ± 6.8 | <0.001 | 28.0 ± 5.7 | 30.2 ± 8.5 | 0.07 |
| Obesity (BMI > 30 kg/m2) | |||||||||
| Obese | 136 (29.3) | 11 (8.1) | 23 (16.9) | 44 (32.4) | 58 (42.6) | <0.001 | 128 (94.1) | 8 (5.9) | 0.89 |
| Not obese | 328 (70.7) | 80 (24.4) | 76 (23.2) | 85 (25.9) | 87 (26.5) | 310 (94.5) | 18 (5.5) | ||
| Nationality | |||||||||
| UAE | 65 (14) | 0 (0) | 13 (20) | 27 (41.5) | 25 (38.5) | <0.001 | 59 (90.8) | 6 (9.2) | 0.25 |
| Arab (Middle Eastern) | 103 (22.2) | 8 (7.8) | 41 (39.8) | 17 (16.5) | 37 (35.9) | 97 (94.2) | 6 (5.8) | ||
| Asian | 276 (59.5) | 81 (29.3) | 44 (15.9) | 79 (28.6) | 72 (26.1) | 264 (95.7) | 12 (4.3) | ||
| Others | 20 (4.3) | 2 (10) | 1 (5) | 6 (30) | 11 (55) | 18 (90) | 2 (10) | ||
| Current Smoker | |||||||||
| Yes | 50 (10.8) | 13 (26) | 23 (46) | 11 (22) | 3 (6) | <0.001 | 50 (100) | 0 (0) | 0.10 |
| No | 414 (89.2) | 78 (18.8) | 76 (18.4) | 118 (28.5) | 142 (34.3) | 388 (93.7) | 26 (6.3) | ||
| 25(OH)D Level (ng/mL) | |||||||||
| <12 | 127 (27.4) | 21 (16.5) | 28 (22) | 34 (26.8) | 44 (34.6) | 0.07 | 117 (92.1) | 10 (7.9) | 0.32 |
| 12–20 | 182 (39.2) | 48 (26.4) | 36 (19.8) | 53 (29.1) | 45 (24.7) | 175 (96.2) | 7 (3.8) | ||
| ≥20 | 155 (33.4) | 22 (14.2) | 35 (22.6) | 42 (27.1) | 56 (36.1) | 146 (94.2) | 9 (5.8) | ||
| Cardiac Disease | |||||||||
| Yes | 54 (11.6) | 0 (0) | 10 (18.5) | 16 (29.6) | 28 (51.9) | <0.001 | 44 (81.5) | 10 (18.5) | <0.001 |
| No | 410 (88.4) | 91 (22.2) | 89 (21.7) | 113 (27.6) | 117 (28.5) | 394 (96.1) | 16 (3.9) | ||
| Chronic Lung Disease | |||||||||
| Yes | 24 (5.2) | 0 (0) | 2 (8.3) | 8 (33.3) | 14 (58.3) | 0.004 | 20 (83.3) | 4 (16.7) | 0.04 |
| No | 439 (94.8) | 91 (20.7) | 97 (22.1) | 120 (27.3) | 131 (29.8) | 417 (95) | 22 (5) | ||
| Diabetes | |||||||||
| Yes | 152 (32.8) | 4 (2.6) | 23 (15.1) | 56 (36.8) | 69 (45.4) | <0.001 | 136 (89.5) | 16 (10.5) | 0.001 |
| No | 312 (67.2) | 87 (27.9) | 76 (24.4) | 73 (23.4) | 76 (24.4) | 302 (96.8) | 10 (3.2) | ||
| Renal Disease | |||||||||
| Yes | 41 (8.8) | 0 (0) | 3 (7.3) | 12 (29.3) | 26 (63.4) | <0.001 | 33 (80.5) | 8 (19.5) | <0.001 |
| No | 423 (91.2) | 91 (21.5) | 96 (22.7) | 117 (27.7) | 119 (28.1) | 405 (95.7) | 18 (4.3) | ||
| Metabolic Disease | |||||||||
| Yes | 27 (5.8) | 1 (3.7) | 4 (14.8) | 8 (29.6) | 14 (51.9) | 0.04 | 23 (85.2) | 4 (14.8) | 0.06 |
| No | 437 (94.2) | 90 (20.6) | 95 (21.7) | 121 (27.7) | 131 (30) | 415 (95) | 22 (5) | ||
| Liver Disease | |||||||||
| Yes | 7 (1.5) | 0 (0) | 1 (14.3) | 2 (28.6) | 4 (57.1) | 0.41 | 6 (85.7) | 1 (14.3) | 0.33 |
| No | 457 (98.5) | 91 (19.9) | 98 (21.4) | 127 (27.8) | 141 (30.9) | 432 (94.5) | 25 (5.5) | ||
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Adjusted | ||||
| Predictor | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Age | 1.08 (1.07, 1.10) | <0.001 | 1.08 (1.07, 1.10) | <0.001 | 1.07 (1.06, 1.09) | <0.001 |
| Male | 1.39 (0.91, 2.14) | 0.13 | 1.22 (0.78, 1.91) | 0.38 | 1.23 (0.78, 1.94) | 0.38 |
| Smoker | 0.34 (0.21, 0.57) | <0.001 | 0.60 (0.35, 1.02) | 0.06 | 0.60 (0.35, 1.02) | 0.06 |
| Obese (BMI > 30 kg/m2) | 2.42 (1.68, 3.49) | <0.001 | ||||
| Cardiac Disease | 3.11 (1.84, 5.26) | <0.001 | 0.72 (0.38, 1.37) | 0.32 | ||
| Chronic Lung Disease | 3.96 (1.81, 8.67) | 0.001 | 1.64 (0.68, 3.93) | 0.27 | ||
| Diabetes | 3.68 (2.56, 5.29) | <0.001 | 1.27 (0.82, 1.97) | 0.28 | ||
| Renal Disease | 5.13 (2.71, 9.73) | <0.001 | 1.66 (0.80, 3.48) | 0.18 | ||
| Metabolic Disease | 2.79 (1.35, 5.75) | 0.005 | 1.34 (0.60, 2.99) | 0.45 | ||
| Liver Disease | 3.35 (0.81, 13.85) | 0.10 | 2.99 (0.54, 16.52) | 0.21 | ||
| 25(OH)D < 12 ng/mL | 1.22 (0.84, 1.76) | 0.29 | 1.79 (1.21, 2.64) | 0.003 | 1.76 (1.19, 2.61) | 0.005 |
| 25(OH)D < 20 ng/mL | 0.71 (0.50, 1.00) | 0.051 | 1.17 (0.80, 1.71) | 0.41 | 1.14 (0.78, 1.66) | 0.51 |
| Model (1) | Model (2) | |||||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Adjusted | ||||
| Predictor | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Age | 1.08 (1.05, 1.11) | <0.001 | 1.08 (1.05, 1.12) | 0.001 | 1.07 (1.03, 1.11) | 0.001 |
| Male | 1.96 (0.57, 6.66) | 0.28 | 1.67 (0.46, 6.02) | 0.43 | 1.84 (0.47, 7.25) | 0.38 |
| Smoker | NA | |||||
| Obese (BMI > 30 kg/m2) | 1.08 (0.46, 2.54) | 0.87 | ||||
| Cardiac Disease | 5.60 (2.39, 13.08) | <0.001 | 1.66 (0.57, 4.83) | 0.35 | ||
| Chronic Lung Disease | 3.79 (1.19, 12.04) | 0.02 | 1.12 (0.28, 4.41) | 0.87 | ||
| Diabetes | 3.55 (1.57, 8.03) | 0.002 | 0.99 (0.38, 2.58) | 0.98 | ||
| Renal Disease | 5.45 (2.21, 13.49) | <0.001 | 1.33 (0.45, 3.95) | 0.60 | ||
| Metabolic Disease | 3.28 (1.04, 10.31) | 0.04 | 2.45 (0.64, 9.34) | 0.19 | ||
| Liver Disease | 2.88 (0.33, 24.85) | 0.34 | 1.66 (0.16, 17.41) | 0.67 | ||
| 25(OH)D < 12 ng/mL | 1.71 (0.76, 3.89) | 0.20 | 2.55 (1.03, 6.33) | 0.04 | 2.58 (1.01, 6.62) | 0.048 |
| 25(OH)D < 20 ng/mL | 0.94 (0.41, 2.17) | 0.89 | 1.72 (0.68, 4.34) | 0.25 | 1.71 (0.66, 4.43) | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlSafar, H.; Grant, W.B.; Hijazi, R.; Uddin, M.; Alkaabi, N.; Tay, G.; Mahboub, B.; Al Anouti, F. COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents. Nutrients 2021, 13, 1714. https://doi.org/10.3390/nu13051714
AlSafar H, Grant WB, Hijazi R, Uddin M, Alkaabi N, Tay G, Mahboub B, Al Anouti F. COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents. Nutrients. 2021; 13(5):1714. https://doi.org/10.3390/nu13051714
Chicago/Turabian StyleAlSafar, Habiba, William B. Grant, Rafiq Hijazi, Maimunah Uddin, Nawal Alkaabi, Guan Tay, Bassam Mahboub, and Fatme Al Anouti. 2021. "COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents" Nutrients 13, no. 5: 1714. https://doi.org/10.3390/nu13051714
APA StyleAlSafar, H., Grant, W. B., Hijazi, R., Uddin, M., Alkaabi, N., Tay, G., Mahboub, B., & Al Anouti, F. (2021). COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents. Nutrients, 13(5), 1714. https://doi.org/10.3390/nu13051714