Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy and Study Selection
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Risk of Bias and Study Quality Assessment
2.6. Statistical Analysis
3. Results
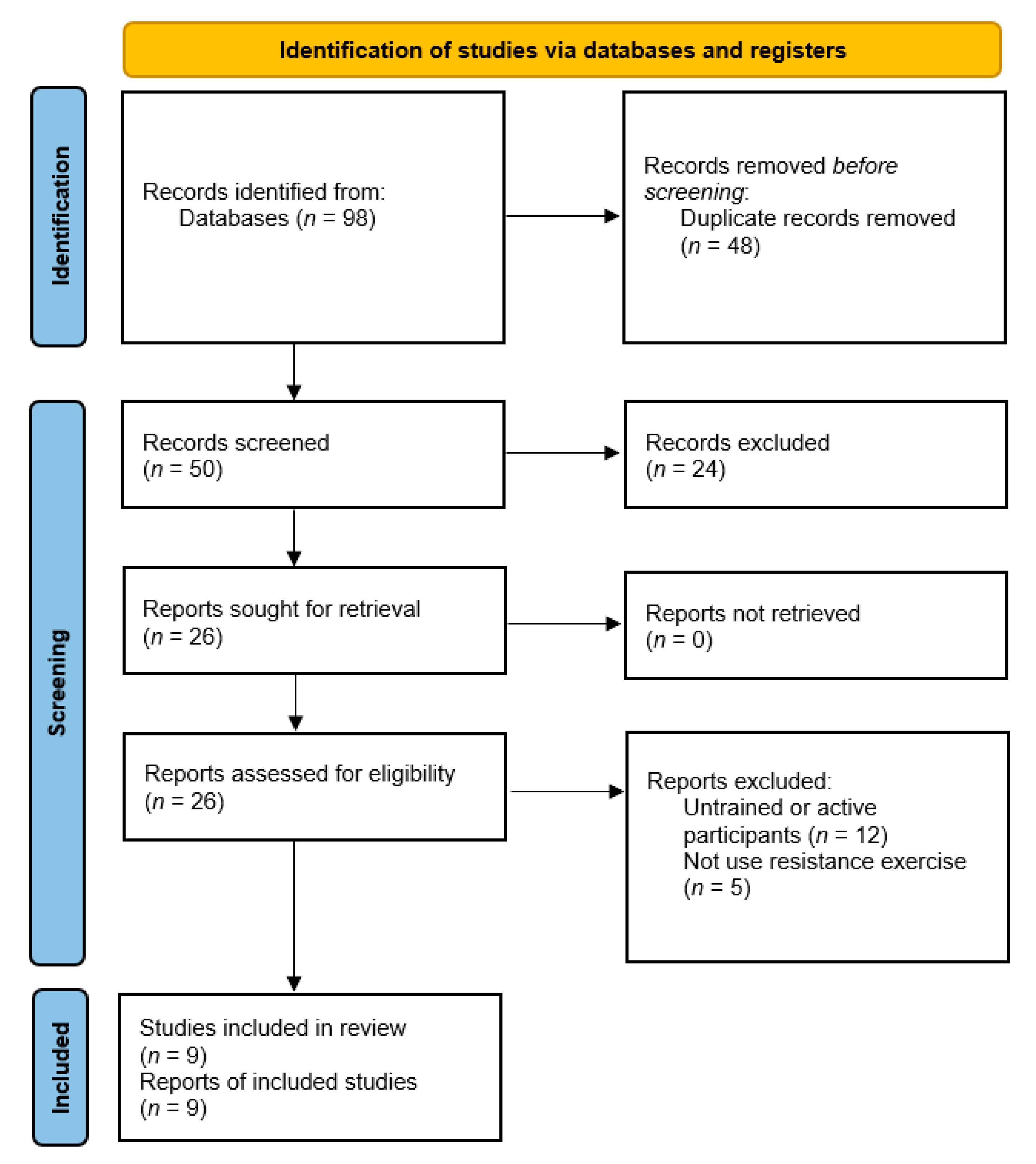
3.1. Literature Search
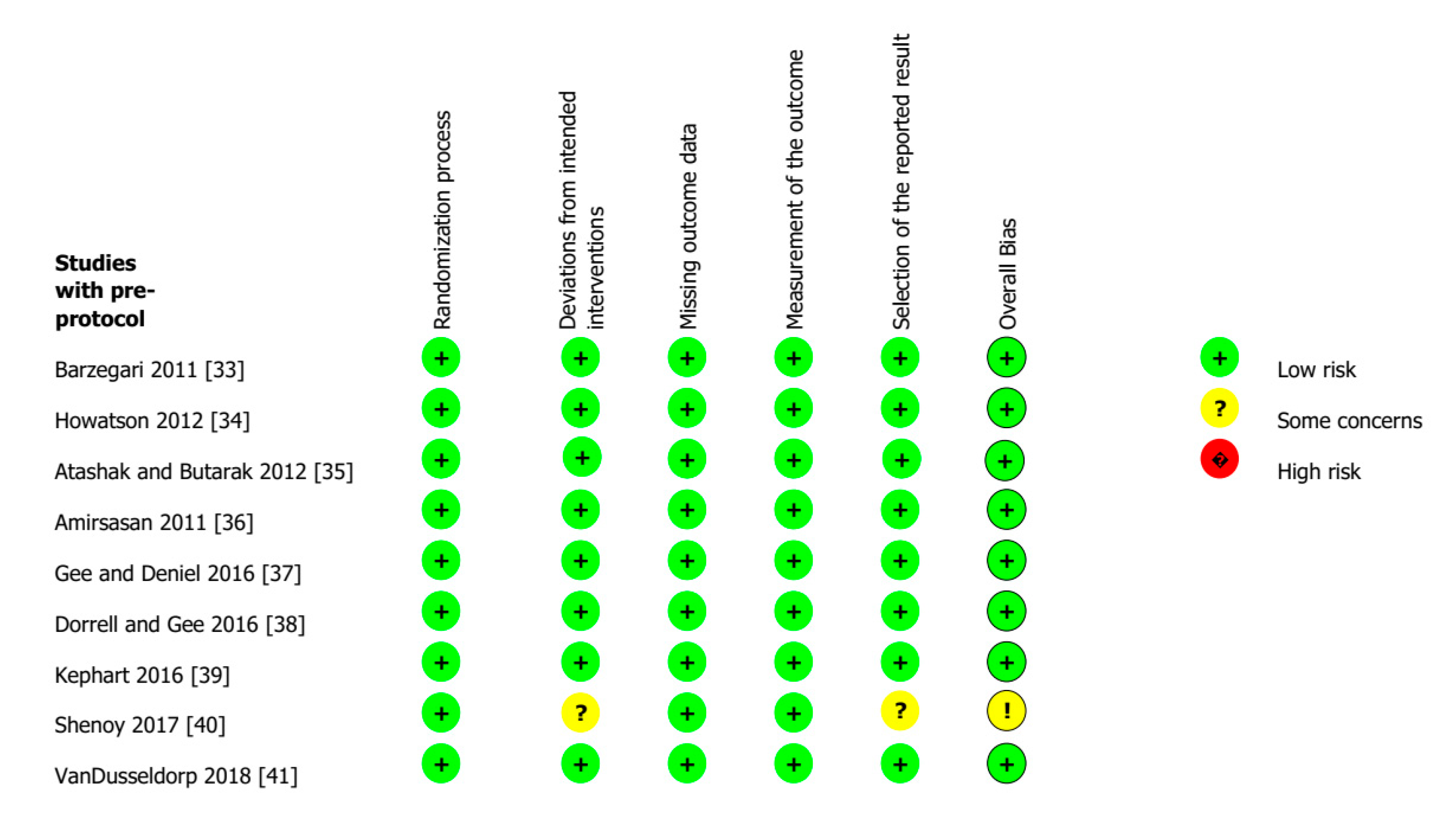
3.2. Risk of Bias Assessment
3.3. Studies Characteristics
3.4. BCAAs Supplementation
3.5. Resistance Exercise Intervention
3.6. Muscle Damage and Soreness Outcomes
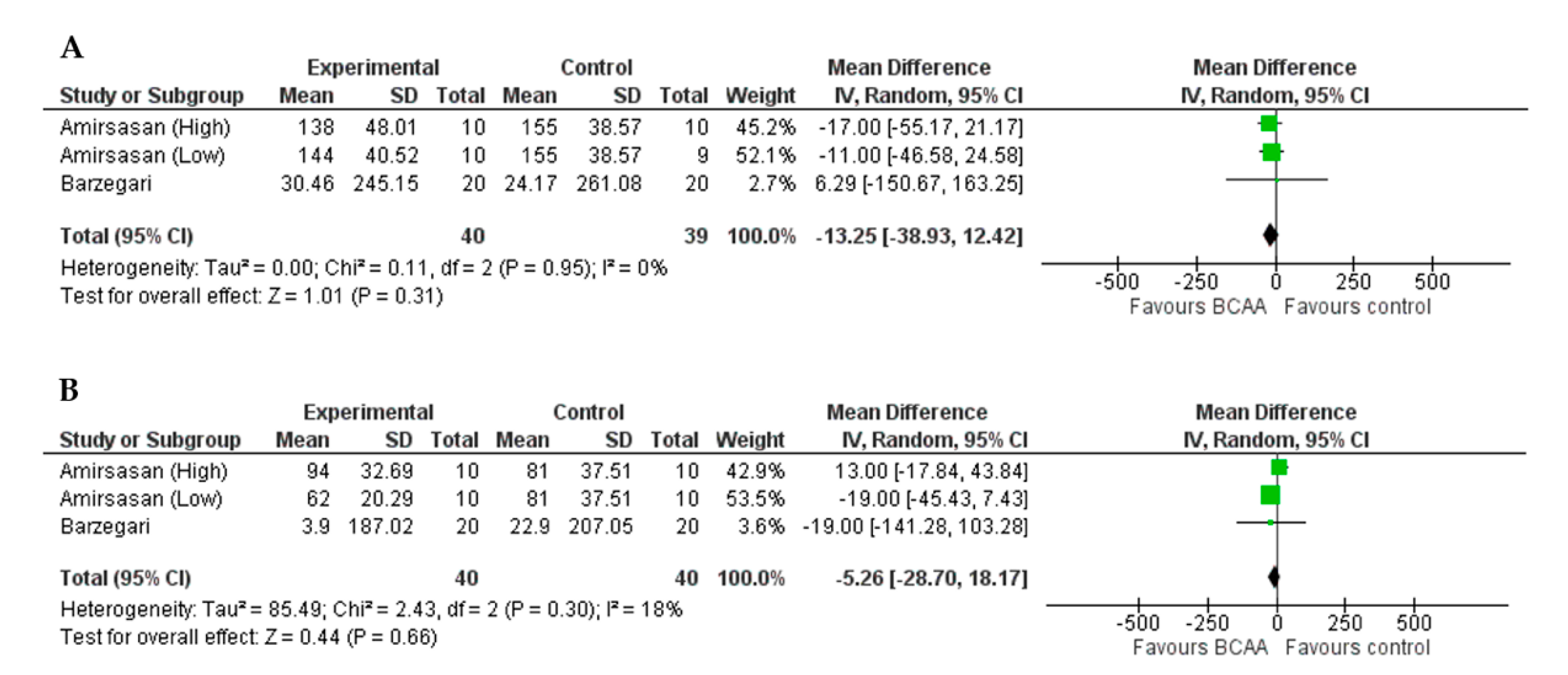
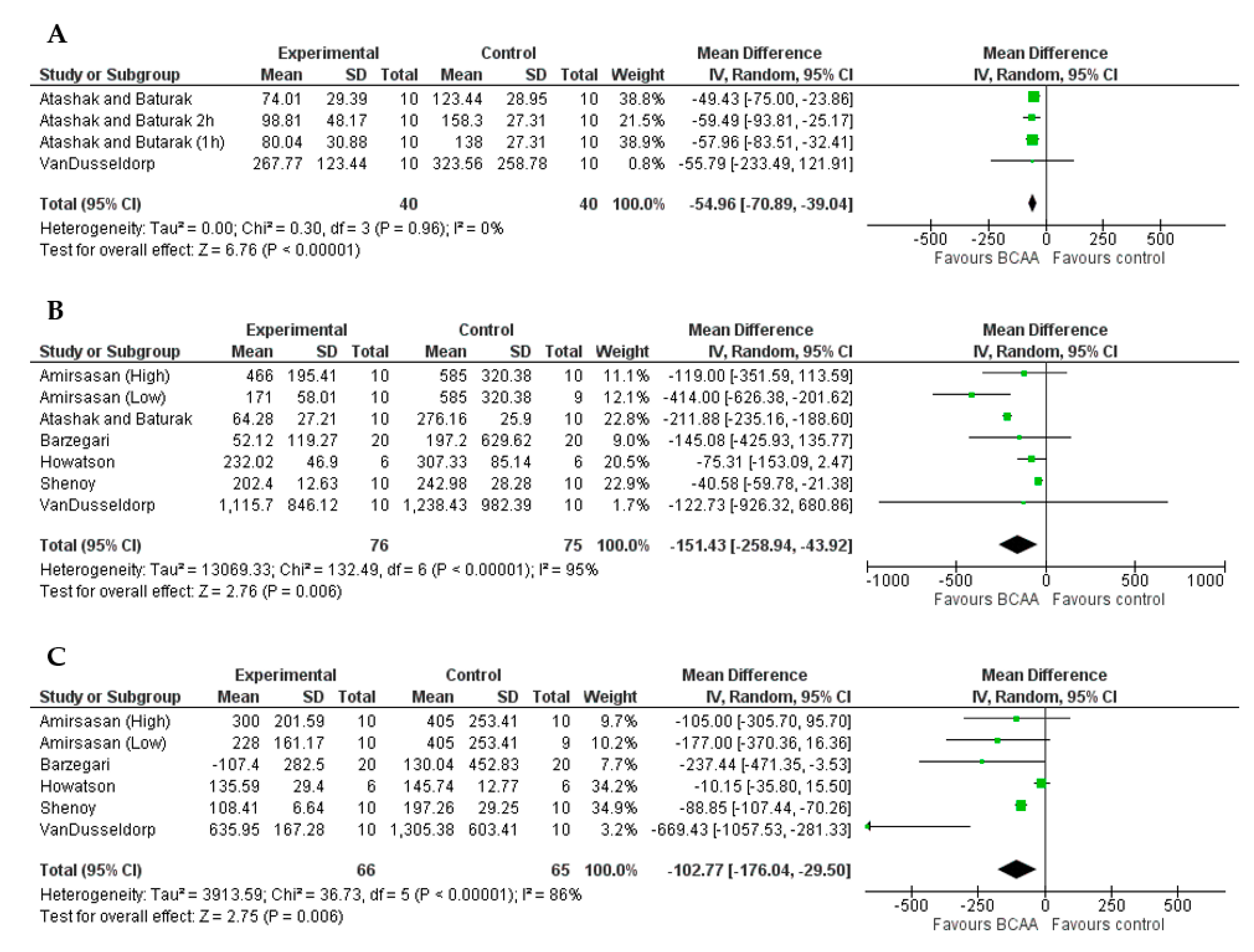
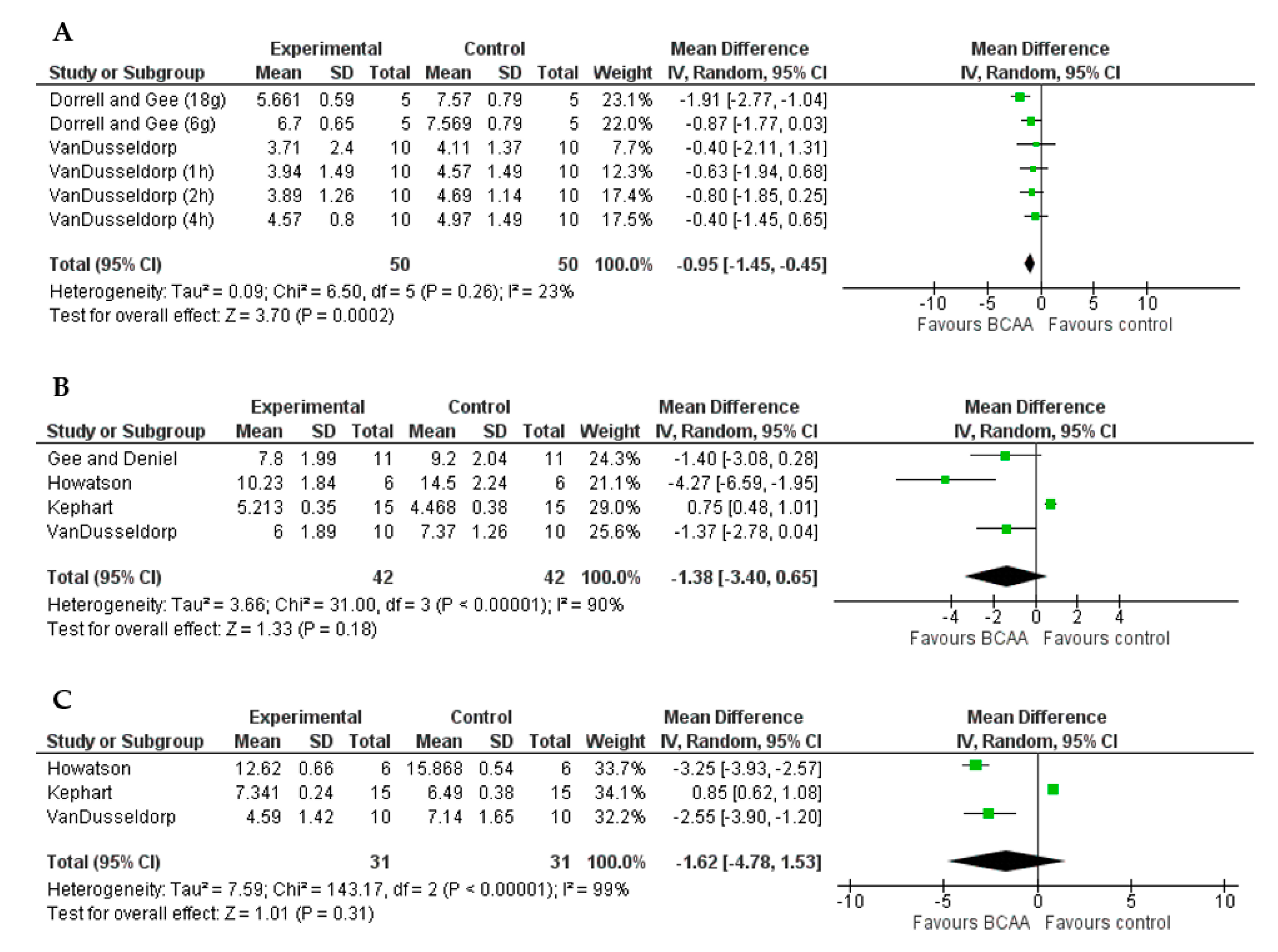
3.7. Effect of BCAAs Supplementation on Muscle Damage and Soreness Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clarkson, P.M.; Hubal, M.J. Exercise-induced muscle damage in humans. Am. J. Phys. Med. Rehabil. 2002, 81, S52–S69. [Google Scholar] [CrossRef]
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef]
- Nosaka, K.; Sakamoto, K. Effect of elbow joint angle on the magnitude of muscle damage to the elbow flexors. Med. Sci. Sports Exerc. 2001, 33, 22–29. [Google Scholar] [CrossRef]
- Chapman, D.; Newton, M.; Sacco, P.; Nosaka, K. Greater muscle damage induced by fast versus slow velocity eccentric exercise. Int. J. Sports. Med. 2006, 27, 591–598. [Google Scholar] [CrossRef]
- Howatson, G.; van Someren, K.A. The prevention and treatment of exercise-induced muscle damage. Sports Med. 2008, 38, 483–503. [Google Scholar] [CrossRef] [PubMed]
- Tidball, J.G. Regulation of muscle growth and regeneration by the immune system. Nat. Rev. Immunol. 2017, 17, 165. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Twist, C.; Eston, R. Neuromuscular function after exercise-induced muscle damage. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef]
- Coombes, J.; McNaughton, L. Effects of branched-chain amino acid supplementation on serum creatine kinase and lactate dehydrogenase after prolonged exercise. J. Sports Med. Phys. Fitness 2000, 40, 240. [Google Scholar] [PubMed]
- Koba, T.; Hamada, K.; Sakurai, M.; Matsumoto, K.; Hayase, H.; Imaizumi, K.; Tsujimoto, H.; Mitsuzono, R. Branched-chain amino acids supplementation attenuates the accumulation of blood lactate dehydrogenase during distance running. J. Sports Med. Phys. Fitness 2007, 47, 316. [Google Scholar]
- Paulsen, G.; Ramer Mikkelsen, U.; Raastad, T.; Peake, J.M. Leucocytes, cytokines and satellite cells: What role do they play in muscle damage and regeneration following eccentric exercise? Exerc. Immunol. Rev. 2012, 18, 42–97. [Google Scholar]
- Brancaccio, P.; Limongelli, F.; Maffulli, N. Monitoring of serum enzymes in sport. Br. J. Sports Med. 2006, 40, 96–97. [Google Scholar] [CrossRef] [Green Version]
- Koch, A.; Pereira, R.; Machado, M. The creatine kinase response to resistance exercise. J. Musculoskelet. Neuronal. Interact. 2014, 14, 68–77. [Google Scholar]
- Yu, J.-G.; Fürst, D.O.; Thornell, L.-E. The mode of myofibril remodelling in human skeletal muscle affected by DOMS induced by eccentric contractions. Histochem. Cell. Biol. 2003, 119, 383–393. [Google Scholar] [CrossRef]
- Blomstrand, E.; Eliasson, J.; Karlsson, H.K.; Köhnke, R. Branched-chain amino acids activate key enzymes in protein synthesis after physical exercise. J. Nutr. 2006, 136, 269S–273S. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, S.H.; Phillips, S.M. Branched-chain amino acids (leucine, isoleucine, and valine) and skeletal muscle. In Nutrition and Skeletal Muscle; Academic Press: Cambridge, MA, USA, 2019; pp. 283–298. [Google Scholar]
- Millward, D.J.; Layman, D.K.; Tomé, D.; Schaafsma, G. Protein quality assessment: Impact of expanding understanding of protein and amino acid needs for optimal health. Am. J. Clin. Nutr. 2008, 87, 1576S–1581S. [Google Scholar] [CrossRef]
- Harper, A.; Miller, R.; Block, K. Branched-chain amino acid metabolism. Annu. Rev. Nutr. 1984, 4, 409–454. [Google Scholar] [CrossRef]
- Nicastro, H.; Da Luz, C.R.; Chaves, D.F.S.; Bechara, L.R.G.; Voltarelli, V.A.; Rogero, M.M.; Lancha, A.H. Does branched-chain amino acids supplementation modulate skeletal muscle remodeling through inflammation modulation? Possible mechanisms of action. J. Nutr. Metab. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International society of sports nutrition position stand: Protein and exercise. J. Int. Soc. Sports. Nutr. 2017, 14, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tom, A.; Nair, K.S. Assessment of branched-chain amino acid status and potential for biomarkers. J. Nutr. 2006, 136, 324S–330S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Luz, C.R.; Nicastro, H.; Zanchi, N.E.; Chaves, D.F.; Lancha, A.H. Potential therapeutic effects of branched-chain amino acids supplementation on resistance exercise-based muscle damage in humans. J. Int. Soc. Sports Nutr. 2011, 8, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fouré, A.; Bendahan, D. Is branched-chain amino acids supplementation an efficient nutritional strategy to alleviate skeletal muscle damage? A systematic review. Nutrients 2017, 9, 1047. [Google Scholar] [CrossRef] [Green Version]
- Rahimi, M.H.; Shab-Bidar, S.; Mollahosseini, M.; Djafarian, K. Branched-chain amino acid supplementation and exercise-induced muscle damage in exercise recovery: A meta-analysis of randomized clinical trials. Nutrition 2017, 42, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Hormoznejad, R.; Zare, J.A.; Mansoori, A. Effect of BCAA supplementation on central fatigue, energy metabolism substrate and muscle damage to the exercise: A systematic review with meta-analysis. Sport Sci. Health 2019, 15, 265–279. [Google Scholar] [CrossRef]
- Rahimlou, M.; Ahmadi, A.H.R.; Palimi, E.; Mahdipour, M.; Poodeh, B.M. Reduction of muscle injuries and improved post-exercise recovery by branched-chain amino acid supplementation: A systematic review and meta-analysis. J. Nutr. Fasting Health 2020, 8, 1–16. [Google Scholar] [CrossRef]
- Dieli-Conwright, C.M.; Spektor, T.M.; Rice, J.C.; Schroeder, E.T. Hormone therapy attenuates exercise-induced skeletal muscle damage in postmenopausal women. J. Appl. Physiol. 2009, 107, 853–858. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Brit. Med. J. 2021, 372. [Google Scholar] [CrossRef]
- Brown, P.B.K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hicks, N.J.; Moody, J. How to formulate research recommendations. Brit. Med. J. 2006, 333, 804–806. [Google Scholar] [CrossRef] [Green Version]
- Kadic, A.J.; Vucic, K.; Dosenovic, S.; Sapunar, D.; Puljak, L. Extracting data from figures with software was faster, with higher interrater reliability than manual extraction. J. Clin. Epidemiol. 2016, 74, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. Brit. Med. J. 2019, 366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 21 February 2021).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Brit. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barzegari, A. Effect of 450 Mg.kg−1 branched-chain amino acid supplement on muscle serum damage indices. World Appl. Sci. J. 2011, 15, 1082–1085. [Google Scholar]
- Howatson, G.; Hoad, M.; Goodall, S.; Tallent, J.; Bell, P.G.; French, D.N. Exercise-induced muscle damage is reduced in resistance-trained males by branched chain amino acids: A randomized, double-blind, placebo controlled study. J. Int. Soc. Sports. Nutr. 2012, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Atashak, S.; Baturak, K. The effect of BCAA supplementation on serum C-reactive protein and creatine kinase after acute resistance exercise in soccer players. Ann. Biol. Res. 2012, 3, 1569–1576. [Google Scholar]
- Amirsasan, R.; Nikookheslat, S.; Sari-Sarraf, V.; Kaveh, B.; Letafatkar, A. The effects of two different dosages of BCAA supplementation on a serum indicators of muscle damage in wrestlers. Int. J. Wrestl. Sci. 2014, 1, 32–36. [Google Scholar] [CrossRef]
- Gee, T.I.; Deniel, S. Branched-chain aminoacid supplementation attenuates a decrease in power-producing ability following acute strength training. J. Sports Med. Phys. Fitness 2016, 56, 1511–1517. [Google Scholar]
- Dorrell, H.F.; Gee, T.I. The acute effects different quantities of branched-chain amino acids have on recovery of muscle function. Sports Nutr. Ther. 2016, 1. [Google Scholar] [CrossRef]
- Kephart, W.C.; Mumford, P.W.; McCloskey, A.E.; Holland, A.M.; Shake, J.J.; Mobley, C.B.; Jagodinsky, A.E.; Weimar, W.H.; Oliver, G.D.; Young, K.C.; et al. Post-exercise branched chain amino acid supplementation does not affect recovery markers following three consecutive high intensity resistance training bouts compared to carbohydrate supplementation. J. Int. Soc. Sports Nutr. 2016, 13, 30. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, S.; Dhawan, M.; Sandhu, J.S. Effect of chronic supplementation of branched chain amino acids on exercise-induced muscle damage in trained athletes. J. Sports Sci. 2017, 5. [Google Scholar] [CrossRef]
- VanDusseldorp, T.A.; Escobar, K.A.; Johnson, K.E.; Stratton, M.T.; Moriarty, T.; Cole, N.; McCormick, J.J.; Kerksick, C.M.; Vaughan, R.A.; Dokladny, K.; et al. Effect of branched-chain amino acid supplementation on recovery following acute eccentric exercise. Nutrients 2018, 10, 1389. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, J.F.T.; Lamb, K.L.; Twist, C. Exercise-induced muscle damage and recovery in young and middle-aged males with different resistance training experience. Sports 2019, 7, 132. [Google Scholar] [CrossRef] [Green Version]
- Malm, C. Exercise-induced muscle damage and inflammation: Fact or fiction? Acta Physiol. Scand. 2001, 171, 233–239. [Google Scholar] [CrossRef]
- Raizel, R.; Tirapegui, J. Role of glutamine, as free or dipeptide form, on muscle recovery from resistance training: A review study. Nutrire 2018, 43. [Google Scholar] [CrossRef]
- Street, B.; Byrne, C.; Eston, R. Glutamine supplementation in recovery from eccentric exercise attenuates strength loss and muscle soreness. J. Exerc. Sci. Fit. 2011, 9, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Davies, R.W.; Carson, B.P.; Jakeman, P.M. The effect of whey protein supplementation on the temporal recovery of muscle function following resistance training: A systematic review and meta-analysis. Nutrients 2018, 10, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, F.C.; Khan, T.M.; Faidah, H.; Haseeb, A.; Khan, A.H. Effectiveness of whey protein supplements on the serum levels of amino acid, creatinine kinase and myoglobin of athletes: A systematic review and meta-analysis. Syst. Rev. 2019, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- White, J.P.; Wilson, J.M.; Austin, K.G.; Greer, B.K.; St John, N.; Panton, L.B. Effect of carbohydrate-protein supplement timing on acute exercise-induced muscle damage. J. Int. Soc. Sports. Nutr. 2008, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Cooke, M.B.; Rybalka, E.; Stathis, C.G.; Cribb, P.J.; Hayes, A. Whey protein isolate attenuates strength decline after eccentrically-induced muscle damage in healthy individuals. J. Int. Soc. Sports. Nutr. 2010, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lott, D.J.; Taivassalo, T.; Cooke, K.D.; Park, H.; Moslemi, Z.; Batra, A.; Forbes, S.C.; Byrne, B.J.; Walter, G.A.; Vandenborne, K. Safety, feasibility, and efficacy of strengthening exercise in Duchenne muscular dystrophy. Muscle Nerve 2021, 63, 320–332. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Population | Trained males Athletes |
| Intervention | BCAAs supplementation |
| Comparators | Placebo or control group |
| Outcomes | LDH, CK, VAS |
| Study design | Randomized Controlled Trials |
| Author, Year | Participants Exp, Con (Study design) | Exercise Intervention | Supplementation Strategies | Follow-up Times | Outcome Measured |
|---|---|---|---|---|---|
| Barzegari, 2011 [33] | 20, 20 (Parallel) | 4 sets × 10 reps at 80% 1RM of seven multi-joints exercises | 68 mg/kg for 6 days before and 450 mg/kg at pre- and post-exercise LEU/ISO/VAL (2:1:1) Placebo: Dextrin | Pre, 24, 48 h | CK LDH |
| Howatson, 2012 [34] | 6, 6 (Parallel) | 5 sets × 20 reps of drop jumps | 20 g for 11 days and 20 g at pre- and post-exercise LEU/ISO/VAL (2:1:1) Placebo: Artificial sweetener | Pre, 24, 48, 72, 96 h | CK VAS |
| Atashak, 2012 [35] | 20, 20 (Parallel) | 7 reps of 100% 1RM until volitional fatigue | 200 mg/kg at pre-exercise LEU/ISO/VAL (2:1:1) Placebo: Omega-3 Fatty acids | Pre, Post-Im, 1, 2, 24 h | CK |
| Amirsasan, 2014 [36] | 10 High dose 10 Low dose 9 Con (Parallel) | 3 sets × 10 reps at 80% 1RM of seven exercises multi and single-joint | 68 mg/kg for 6 days before and 210 mg/kg (low) or 450mg/kg (high) at pre- and post-exercise LEU/ISO/VAL (2:1:1) Placebo: Dextrin | Pre, 24, 48 h | CK LDH |
| Gee, 2016 [37] | 11 (Crossover) | 4 sets × 8 reps at 80% 1RM of multi-joint barbell exercises | 10 g at pre- and post-exercise LEU/ISO/VAL (2:1:1) Placebo: Apple and blackcurrant juice | Pre, 24 h | VAS |
| Dorrell, 2016 [38] | 5 High/Low dose (Crossover) | 4 sets × 8 reps at 75% 1RM of multi-joint barbell exercises | 6 g or 18 g at pre- and post-exercise LEU/ISO/VAL (2:1:1) Placebo: Artificial sweetener | Pre, Post-Im | VAS |
| Kephart, 2016 [39] | 15, 15 (Parallel) | 10 sets × 5 reps at 80% 1RM of barbell back squat | 12 g for 3 consecutive exercise days LEU/ISO/VAL (3:1:2) Placebo: Carbohydrate | Pre, 24, 48 h | VAS |
| Shenoy, 2017 [40] | 10, 10 (Parallel) | 5 sets × 20 reps of drop jump | 20 g for 4 weeks at pre-exercise LEU/ISO/VAL (2:1:1) Placebo: Aspartame | Pre, 24, 48 h | CK |
| VanDusseldorp, 2018 [41] | 10, 10 (Parallel) | 10 sets × 8 reps at 70% 1RM of squat + 5 sets × 20 reps split jump | 0.22 g/kg/day for 8 days at pre-exercise LEU/ISO/VAL (3:1:2) Placebo: Maltodextrin | Pre, 4, 24, 48, 72 h | CK VAS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khemtong, C.; Kuo, C.-H.; Chen, C.-Y.; Jaime, S.J.; Condello, G. Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 1880. https://doi.org/10.3390/nu13061880
Khemtong C, Kuo C-H, Chen C-Y, Jaime SJ, Condello G. Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2021; 13(6):1880. https://doi.org/10.3390/nu13061880
Chicago/Turabian StyleKhemtong, Chutimon, Chia-Hua Kuo, Chih-Yen Chen, Salvador J. Jaime, and Giancarlo Condello. 2021. "Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials" Nutrients 13, no. 6: 1880. https://doi.org/10.3390/nu13061880
APA StyleKhemtong, C., Kuo, C. -H., Chen, C. -Y., Jaime, S. J., & Condello, G. (2021). Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials. Nutrients, 13(6), 1880. https://doi.org/10.3390/nu13061880