
Modifiable Determinants of Postpartum Weight Loss in Women with Obesity: A Secondary Analysis of the UPBEAT Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Maternal Variables
2.2. Exposure Variables
2.3. Statistical Analysis
Modifiable Factor Model for Postpartum Weight Retention
3. Results
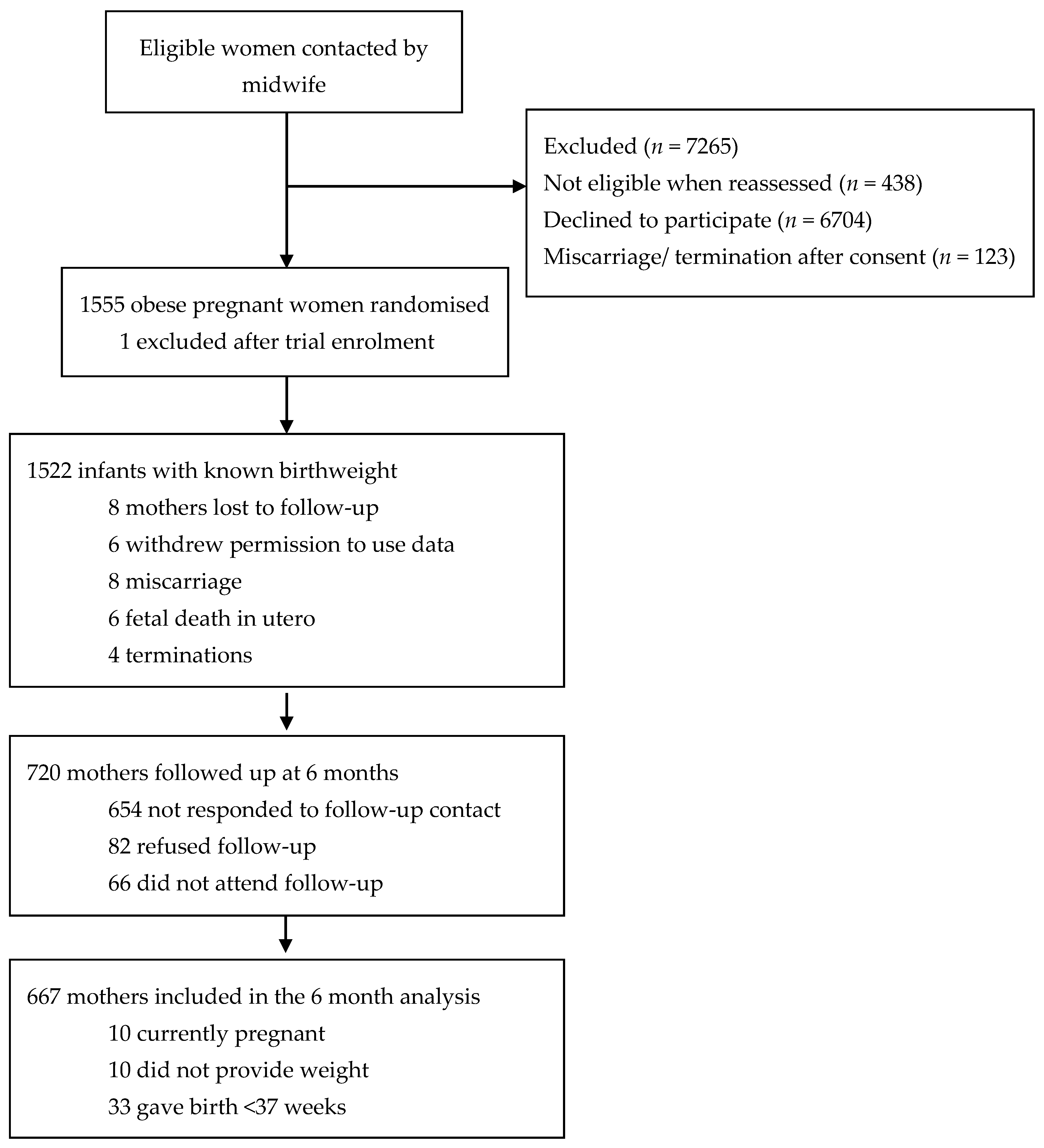
3.1. Six Month Follow-Up
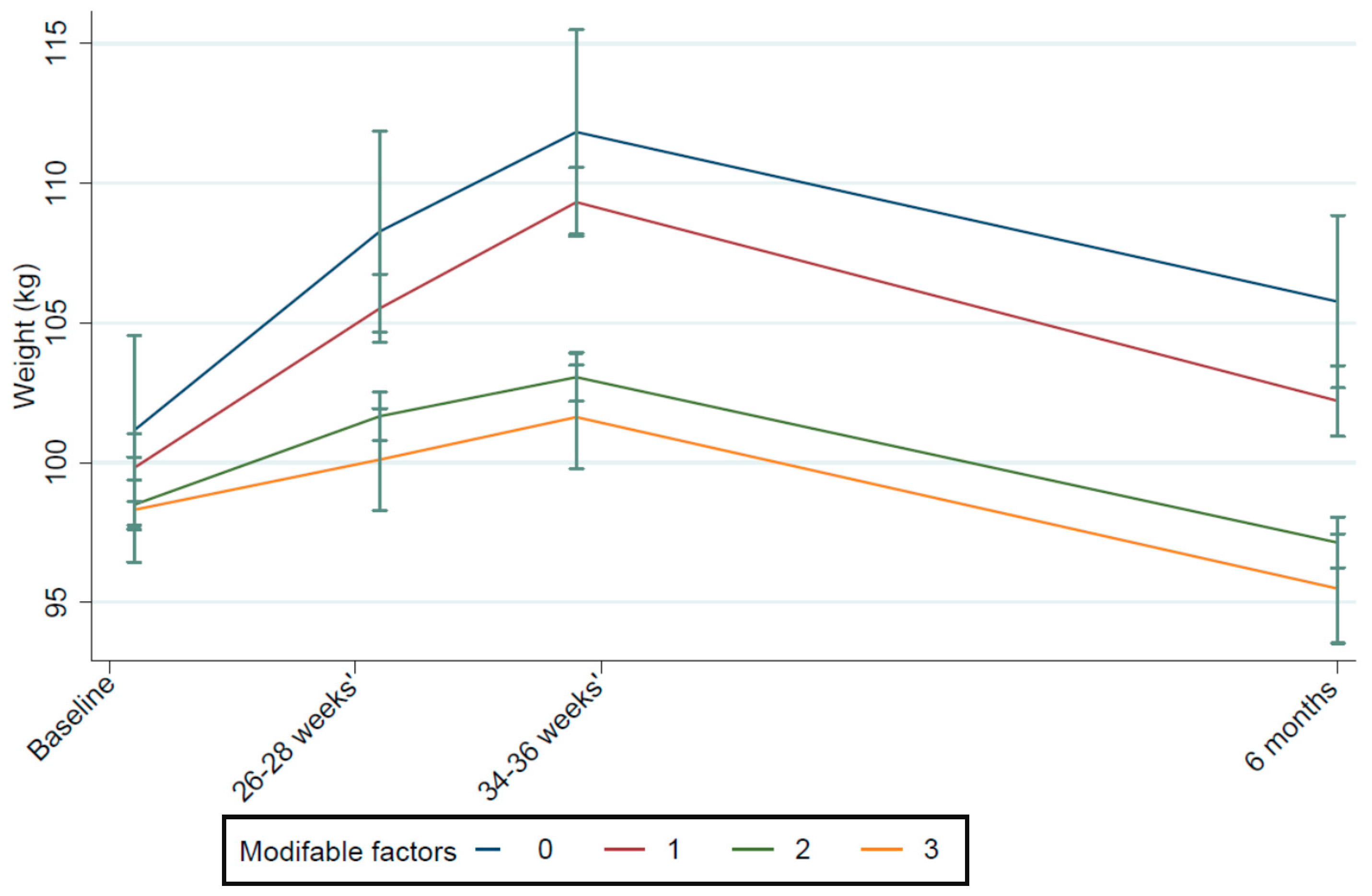
3.2. Modifiable Factor Model for Postpartum Weight Retention
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 13 August 2019).
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Mannan, M.; Doi, S.A.R.; Mamun, A.A. Association between Weight Gain during Pregnancy and Postpartum Weight Retention and Obesity: A Bias-Adjusted Meta-Analysis. Nutr. Rev. 2013, 71, 343–352. [Google Scholar] [CrossRef]
- Walter, J.R.; Perng, W.; Kleinman, K.P.; Rifas-Shiman, M.S.L.; Rich-Edwards, J.W.; Oken, E. Associations of Trimester-Specific Gestational Weight Gain with Maternal Adiposity and Systolic Blood Pressure at 3 and 7 Years Postpartum. Am. J. Obstet. Gynecol. 2015, 212, 499.e1–499.e12. [Google Scholar] [CrossRef] [Green Version]
- Rong, K.; Yu, K.; Han, X.; Szeto, I.M.Y.; Qin, X.; Wang, J.; Ning, Y.; Wang, P.; Ma, D. Pre-Pregnancy BMI, Gestational Weight Gain and Postpartum Weight Retention: A Meta-Analysis of Observational Studies. Public Health Nutr. 2015, 18, 2172–2182. [Google Scholar] [CrossRef]
- Ketterl, T.G.; Dundas, N.J.; Roncaioli, S.A.; Littman, A.J.; Phipps, A.I. Association of Pre-Pregnancy BMI and Postpartum Weight Retention Before Second Pregnancy, Washington State, 2003–2013. Matern. Child Health J. 2018, 22, 1339–1344. [Google Scholar] [CrossRef]
- Gunderson, E.P.; Abrams, B.; Selvin, S. Does the Pattern of Postpartum Weight Change Differ According to Pregravid Body Size? Int. J. Obes. 2001, 25, 853–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.P.; Gavard, J.A.; Rice, J.J.; Catanzaro, R.B.; Artal, R.; Hopkins, S.A. The Impact of Interpregnancy Weight Change on Birthweight in Obese Women. Am. J. Obstet. Gynecol. 2013, 208, 205.e1–205.e7. [Google Scholar] [CrossRef]
- Sha, T.; Cheng, G.; Li, C.; Gao, X.; Li, L.; Chen, C.; Yan, Y. Patterns of Women’s Postpartum Weight Retention and Its Associations with Maternal Obesity-Related Factors and Parity. Int. J. Environ. Res. Public. Health 2019, 16, 4510. [Google Scholar] [CrossRef] [Green Version]
- Phelan, S. Pregnancy: A “Teachable Moment” for Weight Control and Obesity Prevention. Am. J. Obstet. Gynecol. 2010, 202, e1–e135. [Google Scholar] [CrossRef] [Green Version]
- Spencer, L.; Rollo, M.; Hauck, Y.; MacDonald-Wicks, L.; Wood, L.; Hutchesson, M.; Giglia, R.; Smith, R.; Collins, C. The Effect of Weight Management Interventions That Include a Diet Component on Weight-Related Outcomes in Pregnant and Postpartum Women: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 88–98. [Google Scholar] [CrossRef] [Green Version]
- Villamor, E.; Cnattingius, S. Interpregnancy Weight Change and Risk of Adverse Pregnancy Outcomes: A Population-Based Study. Lancet 2006, 368, 1164–1170. [Google Scholar] [CrossRef]
- Kapinos, K.A.; Yakusheva, O.; Weiss, M. Cesarean Deliveries and Maternal Weight Retention. BMC Pregnancy Childbirth 2017, 17, 343. [Google Scholar] [CrossRef] [Green Version]
- Waage, C.W.; Falk, R.S.; Sommer, C.; Mørkrid, K.; Richardsen, K.R.; Baerug, A.; Shakeel, N.; Birkeland, K.I.; Jenum, A.K. Ethnic Differences in Postpartum Weight Retention: A Norwegian Cohort Study. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.-K.; Cameron, C.M.; Hills, A.P.; McClure, R.J.; Scuffham, P.A. Socioeconomic Disparities in Prepregnancy BMI and Impact on Maternal and Neonatal Outcomes and Postpartum Weight Retention: The EFHL Longitudinal Birth Cohort Study. BMC Pregnancy Childbirth 2014, 14, 314. [Google Scholar] [CrossRef] [Green Version]
- Levine, M.D.; Cheng, Y.; Marcus, M.D.; Kalarchian, M.A. Relapse to Smoking and Postpartum Weight Retention among Women Who Quit Smoking during Pregnancy. Obesity 2012, 20, 457–459. [Google Scholar] [CrossRef]
- Boghossian, N.S.; Yeung, E.H.; Lipsky, L.M.; Poon, A.K.; Albert, P.S. Dietary Patterns in Association with Postpartum Weight Retention. Am. J. Clin. Nutr. 2013, 97, 1338–1345. [Google Scholar] [CrossRef]
- Hayes, L.; Bell, R.; Robson, S.; Poston, L. UPBEAT Consortium Association between Physical Activity in Obese Pregnant Women and Pregnancy Outcomes: The UPBEAT Pilot Study. Ann. Nutr. Metab. 2014, 64, 239–246. [Google Scholar] [CrossRef]
- Wang, Q.; Chen, L.; Hu, C.; Shao, Z.; Wang, Y.; Li, L. Influence of physical activity on postpartum weight retention among women, one year after childbirth. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2013, 34, 1077–1079. [Google Scholar]
- McKinley, M.; Allen-Walker, V.; McGirr, C.; Rooney, C.; Woodside, J. Weight Loss after Pregnancy: Challenges and Opportunities. Nutr. Res. Rev. 2018, 31, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neville, C.E.; McKinley, M.C.; Holmes, V.A.; Spence, D.; Woodside, J.V. The Relationship between Breastfeeding and Postpartum Weight Change—A Systematic Review and Critical Evaluation. Int. J. Obes. 2014, 38, 577–590. [Google Scholar] [CrossRef]
- NICE. Weight Management before, during and after Pregnancy (PH27). Available online: https://www.nice.org.uk/guidance/ph27/resources/weight-management-before-during-and-after-pregnancy-pdf-1996242046405 (accessed on 2 March 2021).
- Dalrymple, K.V.; Flynn, A.C.; Relph, S.A.; O’Keeffe, M.; Poston, L. Lifestyle Interventions in Overweight and Obese Pregnant or Postpartum Women for Postpartum Weight Management: A Systematic Review of the Literature. Nutrients 2018, 10, 1704. [Google Scholar] [CrossRef] [Green Version]
- Dodd, J.M.; Deussen, A.R.; O’Brien, C.M.; Schoenaker, D.A.J.M.; Poprzeczny, A.; Gordon, A.; Phelan, S. Targeting the Postpartum Period to Promote Weight Loss: A Systematic Review and Meta-Analysis. Nutr. Rev. 2018, 76, 639–654. [Google Scholar] [CrossRef] [PubMed]
- Briley, A.L.; Barr, S.; Badger, S.; Bell, R.; Croker, H.; Godfrey, K.M.; Holmes, B.; Kinnunen, T.I.; Nelson, S.M.; Oteng-Ntim, E.; et al. A Complex Intervention to Improve Pregnancy Outcome in Obese Women; the UPBEAT Randomised Controlled Trial. BMC Pregnancy Childbirth 2014, 14, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Physical Activity Questionnaire. 2005. Available online: http://www.ipaq.ki.se/ (accessed on 26 January 2021).
- Rasmussen, K.M.; Catalano, P.M.; Yaktine, A.L. New Guidelines for Weight Gain during Pregnancy: What Obstetrician/Gynecologists Should Know. Curr. Opin. Obstet. Gynecol. 2009, 21, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Renfrew, M.; McAndrew, F.; Thompson, J.; Fellows, L.; Large, A.; Speed, M. Infant Feeding Survey 2010. Health and Social Care Information Centre, 2011. Available online: https://sp.ukdataservice.ac.uk/doc/7281/mrdoc/pdf/7281_ifs-uk-2010_report.pdf (accessed on 4 June 2021).
- Patel, N.; Godfrey, K.; Pasupathy, D.; Levin, J.; Flynn, A.; Hayes, L.; Briley, A.; Bell, R.; Lawlor, D.; Oteng-Ntim, E. Infant Adiposity Following a Randomised Controlled Trial of a Behavioural Intervention in Obese Pregnancy. Int. J. Obes. 2017, 41, 1018–1026. [Google Scholar] [CrossRef] [Green Version]
- Endres, L.K.; Straub, H.; McKinney, C.; Plunkett, B.; Minkovitz, C.S.; Schetter, C.D.; Ramey, S.; Wang, C.; Hobel, C.; Raju, T.; et al. Postpartum Weight Retention Risk Factors and Relationship to Obesity at One Year. Obstet. Gynecol. 2015, 125, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Hollis, J.L.; Crozier, S.R.; Inskip, H.M.; Cooper, C.; Godfrey, K.M.; Harvey, N.C.; Collins, C.E.; Robinson, S.M. Modifiable Risk Factors of Maternal Postpartum Weight Retention: An Analysis of Their Combined Impact and Potential Opportunities for Prevention. Int. J. Obes. 2005 2017, 41, 1091–1098. [Google Scholar] [CrossRef] [Green Version]
- Mamun, A.A.; Mannan, M.; Doi, S.A.R. Gestational Weight Gain in Relation to Offspring Obesity over the Life Course: A Systematic Review and Bias-Adjusted Meta-Analysis. Obes. Rev. 2014, 15, 338–347. [Google Scholar] [CrossRef]
- Tahir, M.J.; Haapala, J.L.; Foster, L.P.; Duncan, K.M.; Teague, A.M.; Kharbanda, E.O.; McGovern, P.M.; Whitaker, K.M.; Rasmussen, K.M.; Fields, D.A.; et al. Association of Full Breastfeeding Duration with Postpartum Weight Retention in a Cohort of Predominantly Breastfeeding Women. Nutrients 2019, 11, 938. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Jewell, S.; Grummer-Strawn, L. Maternal Obesity and Breast-Feeding Practices. Am. J. Clin. Nutr. 2003, 77, 931–936. [Google Scholar] [CrossRef] [Green Version]
- Chief Medical Officers. UK Chief Medical Officers’ Physical Activity Guidelines; 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 13 December 2020).
- Evenson, K.R.; Aytur, S.A.; Borodulin, K. Physical Activity Beliefs, Barriers, and Enablers among Postpartum Women. J. Womens Health 2002 2009, 18, 1925–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational Weight Gain and Long-Term Postpartum Weight Retention: A Meta-Analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef]
- Martin, J.E.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. Predictors of Post-Partum Weight Retention in a Prospective Longitudinal Study. Matern. Child Nutr. 2014, 10, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, J.M.; Weiss, M.E.; Ryan, P. Weight-Management Information Needs of Postpartum Women. MCN Am. J. Matern. Child Nurs. 2012, 37, 56–63. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal Demographics | N | Mean (SD)/Median (IQR)/N (%) | |
|---|---|---|---|
| 15–18 weeks gestation (baseline) | |||
| Age at baseline (years) | 667 | 31.2 (5.3) | |
| BMI (kg/m2) | 667 | 35 (32.7–38.7) | |
| Nulliparous | 667 | 330 (49) | |
| Ethnicity | Asian | 667 | 23 (3) |
| Black | 125 (19) | ||
| Other | 42 (6) | ||
| White | 477 (72) | ||
| Any cigarette smoking during pregnancy | 667 | 92 (14) | |
| SES (IMD score) ¥ | 1 (least deprived) | 665 | 31 (5) |
| 2 | 47 (7) | ||
| 3 | 74 (11) | ||
| 4 | 242 (36) | ||
| 5 (most deprived) | 271 (41) | ||
| Years in full time education | 667 | 15.1 (2.84) | |
| Infant demographics | |||
| Gestation at delivery (days) | 667 | 279 (9.0) | |
| Mode of delivery | LSCS in labour | 667 | 128 (19) |
| Operative vaginal | 90 (14) | ||
| Prelabour LSCS | 139 (21) | ||
| Unassisted vaginal | 310 (46) | ||
| Neonate birthweight (g) | 667 | 3525 (474) | |
| Macrosomia (>4 kg) | 667 | 101 (15) | |
| LBW (<2.5 kg) | 667 | 9 (1) | |
| Mode of feeding at hospital discharge | Breastfeeding | 665 | 425 (64) |
| Formula feeding | 133 (20) | ||
| Mixed feeding | 107 (16) | ||
| Maternal antenatal and postpartum characteristics | |||
| Gestational diabetes mellitus ** | 656 | 181 (27) | |
| Gestational weight gain (kg) ¶ | 641 | 7.39 (4.52) | |
| GWG according to IOM Guidelines ¶ | Inadequate | 639 | 194 (30) |
| Adequate | 217 (34) | ||
| Excessive | 230 (36) | ||
| Exclusively breastfeeding ≥ 4 months | 621 | 187 (30) | |
| Postpartum weight retention (kg) | 667 | −0.06 (7.14) | |
| PPWR >5 kg | 667 | 145 (21%) | |
| Physical activity reported at 6 months (METs/week) † | Low | 666 | 92 (14) |
| Moderate | 329 (49) | ||
| High | 245 (37) | ||
| Factors | N | B-Coefficient 95% CI * | p-Value | |
|---|---|---|---|---|
| Smoking in pregnancy | 648 | 1.33 (−0.17 to 2.84) | 0.083 | |
| Breastfeeding ≥4 months | 603 | −2.33 (−3.55 to −1.11) | <0.0001 | |
| IOM GWG ¶ | 193 | Inadequate | −2.06 (−3.32 to −0.80) | 0.001 |
| 216 | Adequate | Ref | ||
| 229 | Excessive | 3.47 (2.26 to 4.67) | <0.0001 | |
| Postpartum physical activity (METs/week) † | 109 | Low | Ref | |
| 276 | Moderate | −1.62 (−3.19 to −0.05) | 0.043 | |
| 278 | vigorous | −1.75 (−3.41 to −0.09) | 0.039 | |
| Unadjusted (n = 595) | Adjusted (n = 587) | ||||
|---|---|---|---|---|---|
| Factors (N (%)) | Mean (SD) PPWR | B-Coef. 95% CI | p-Value | B-Coef. 95% CI | p-Value |
| 0 (19 (3%)) | +6.6 kg (6.85) | Ref | Ref | ||
| 1 (183 (30%)) | +2.4 kg (7.18) | −4.21 (−7.52 to −0.92) | 0.012 | −3.72 (−7.06 to −0.38) | 0.029 |
| 2 (314 (51%)) | −1.0 kg (6.18) | −7.65 (−10.8 to −4.42) | <0.000 | −7.02 (−10.3 to −3.73) | <0.000 |
| 3 (99 (16%)) | −3.1 kg (7.81) | −9.81 (−13.2 to −6.39) | <0.000 | −9.38 (−12.7 to −5.89) | <0.000 |
| Β- trend | −3.06 (−3.80 to −2.31) | <0.000 | −3.00 (−3.76 to −2.25) | <0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalrymple, K.V.; Uwhubetine, O.; Flynn, A.C.; Pasupathy, D.; Briley, A.L.; Relph, S.A.; Seed, P.T.; O’Keeffe, M.; Poston, L. Modifiable Determinants of Postpartum Weight Loss in Women with Obesity: A Secondary Analysis of the UPBEAT Trial. Nutrients 2021, 13, 1979. https://doi.org/10.3390/nu13061979
Dalrymple KV, Uwhubetine O, Flynn AC, Pasupathy D, Briley AL, Relph SA, Seed PT, O’Keeffe M, Poston L. Modifiable Determinants of Postpartum Weight Loss in Women with Obesity: A Secondary Analysis of the UPBEAT Trial. Nutrients. 2021; 13(6):1979. https://doi.org/10.3390/nu13061979
Chicago/Turabian StyleDalrymple, Kathryn V., Onome Uwhubetine, Angela C. Flynn, Dharmintra Pasupathy, Annette L. Briley, Sophie A. Relph, Paul T. Seed, Majella O’Keeffe, and Lucilla Poston. 2021. "Modifiable Determinants of Postpartum Weight Loss in Women with Obesity: A Secondary Analysis of the UPBEAT Trial" Nutrients 13, no. 6: 1979. https://doi.org/10.3390/nu13061979
APA StyleDalrymple, K. V., Uwhubetine, O., Flynn, A. C., Pasupathy, D., Briley, A. L., Relph, S. A., Seed, P. T., O’Keeffe, M., & Poston, L. (2021). Modifiable Determinants of Postpartum Weight Loss in Women with Obesity: A Secondary Analysis of the UPBEAT Trial. Nutrients, 13(6), 1979. https://doi.org/10.3390/nu13061979