
Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. COVID-19 and Health Behaviors Questionnaire
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Demographics and Household Characteristics
3.2. COVID-19-Related Household Changes
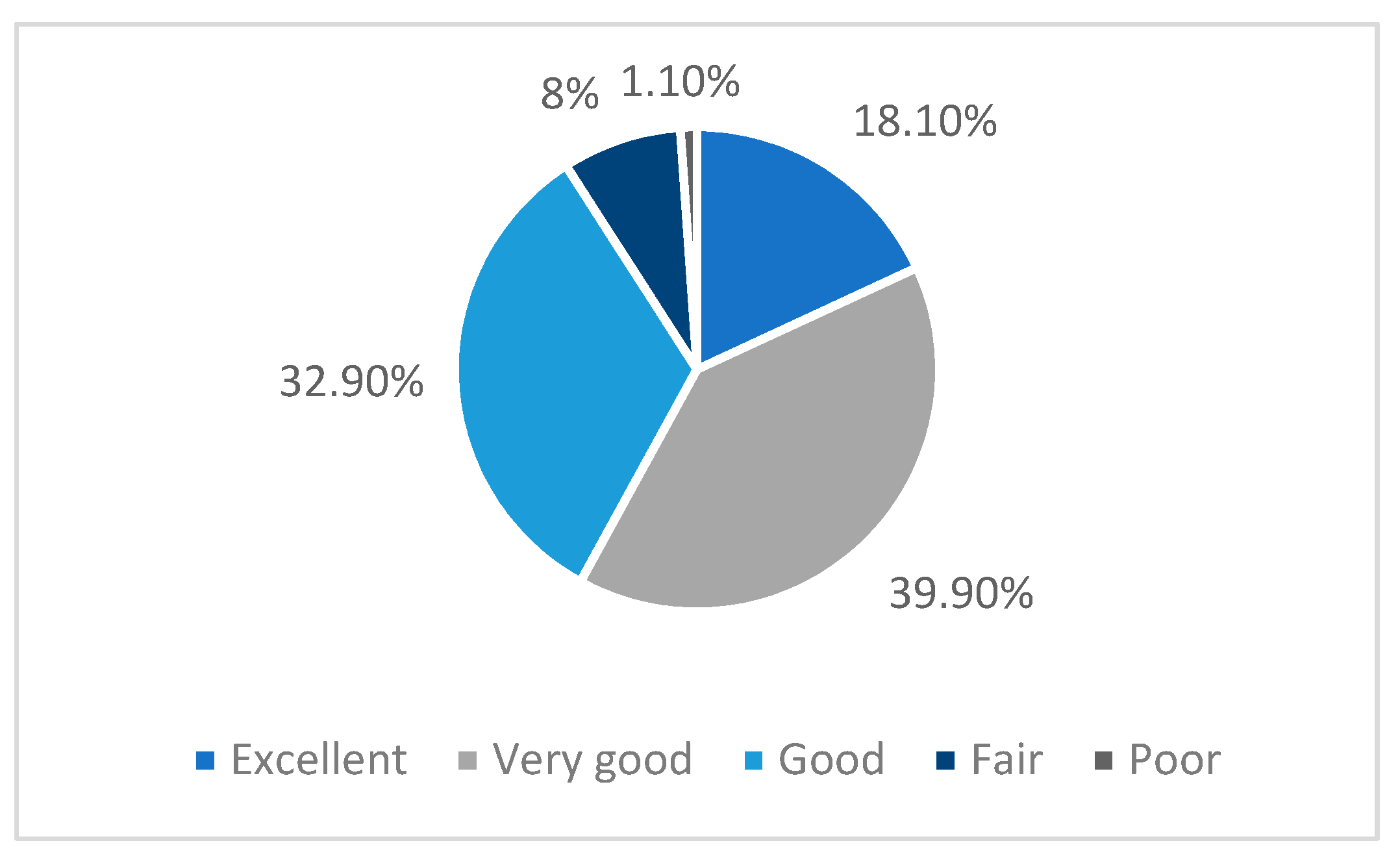
3.3. COVID-19-Related Health Situation
3.4. COVID-19-Related Food Behavior Changes
3.4.1. Food Security
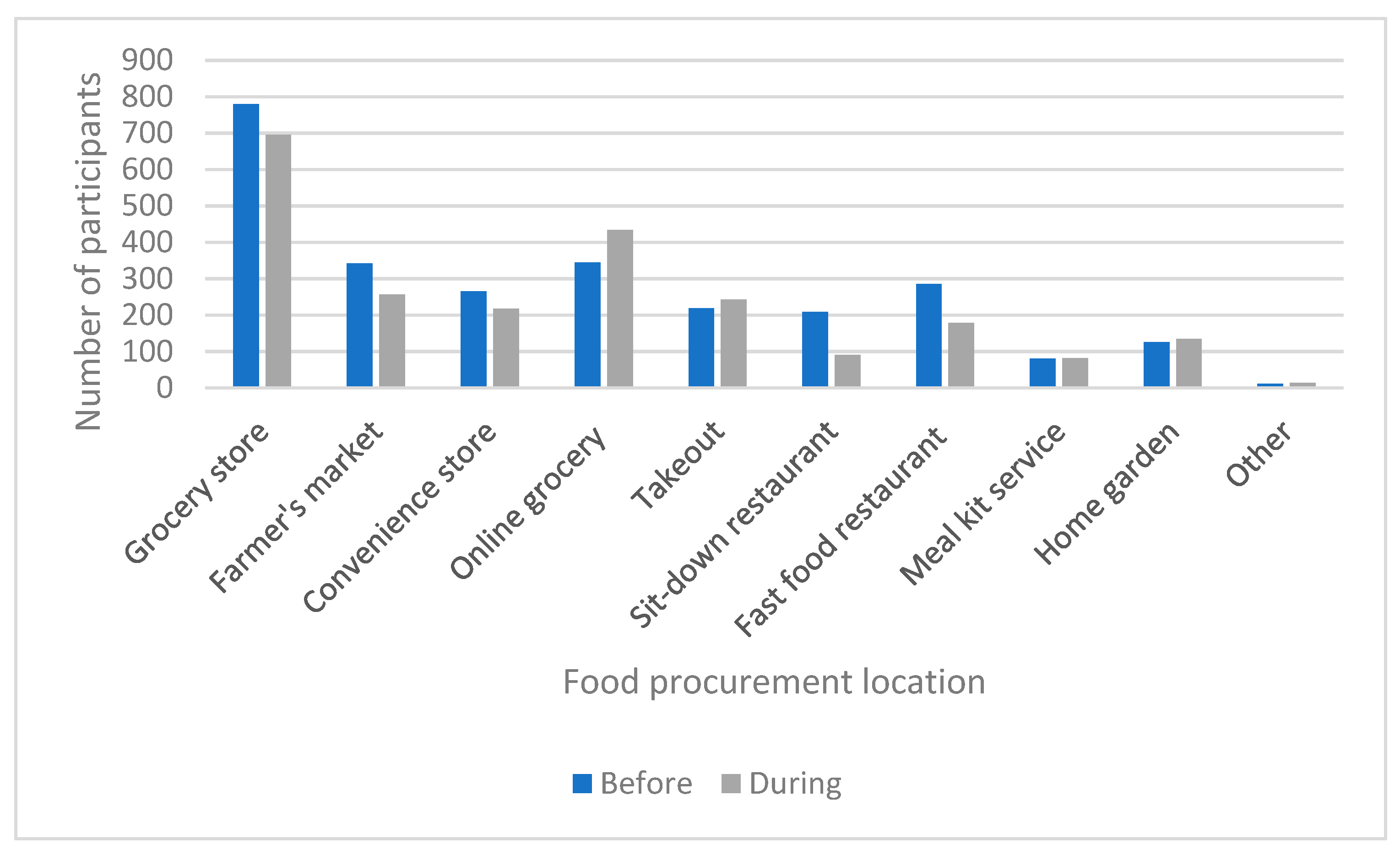
3.4.2. Food Procurement
3.4.3. Changes in Grocery Shopping Habits by Food Category
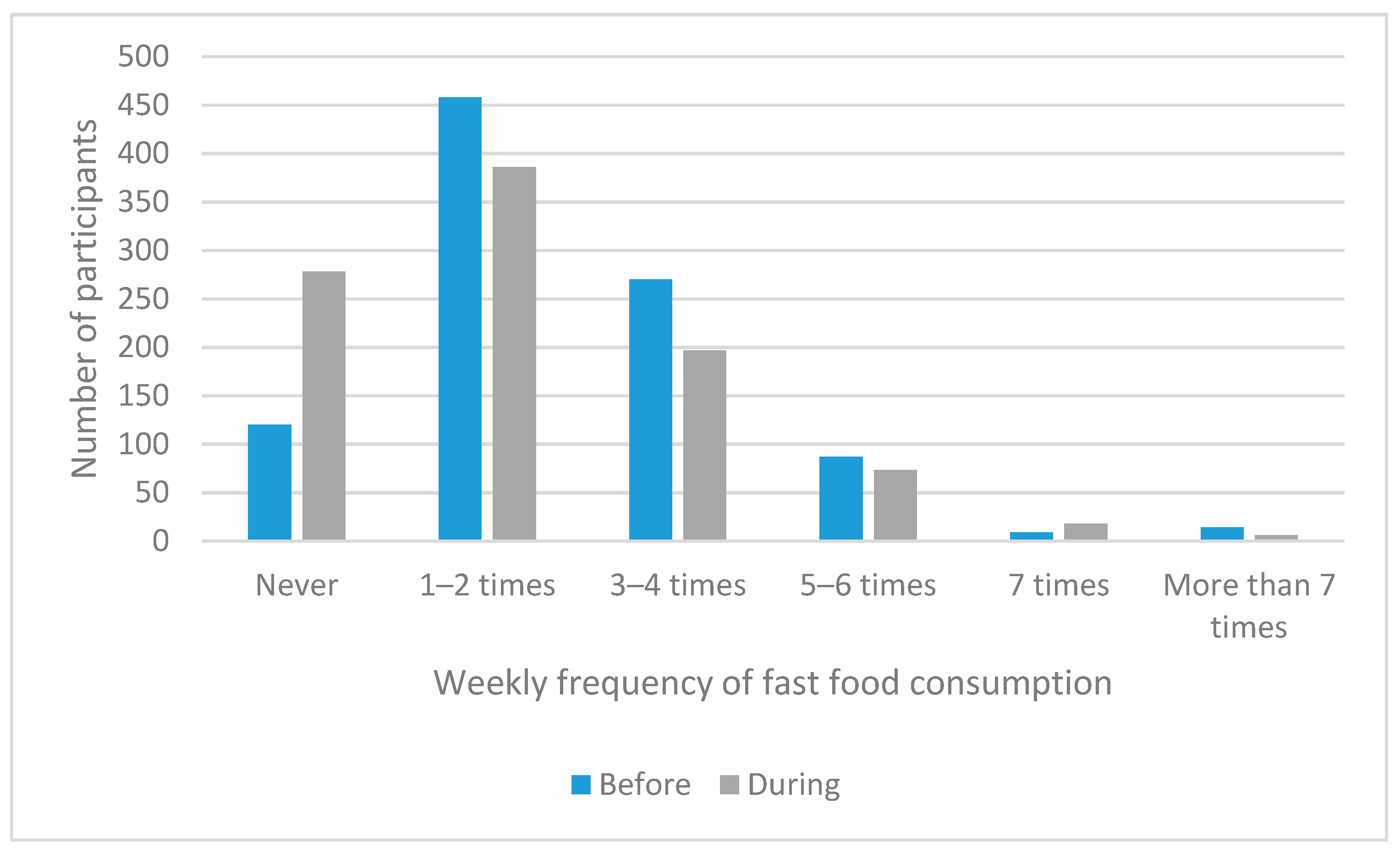
3.4.4. Fast Food Consumption
3.4.5. Food Advertisements
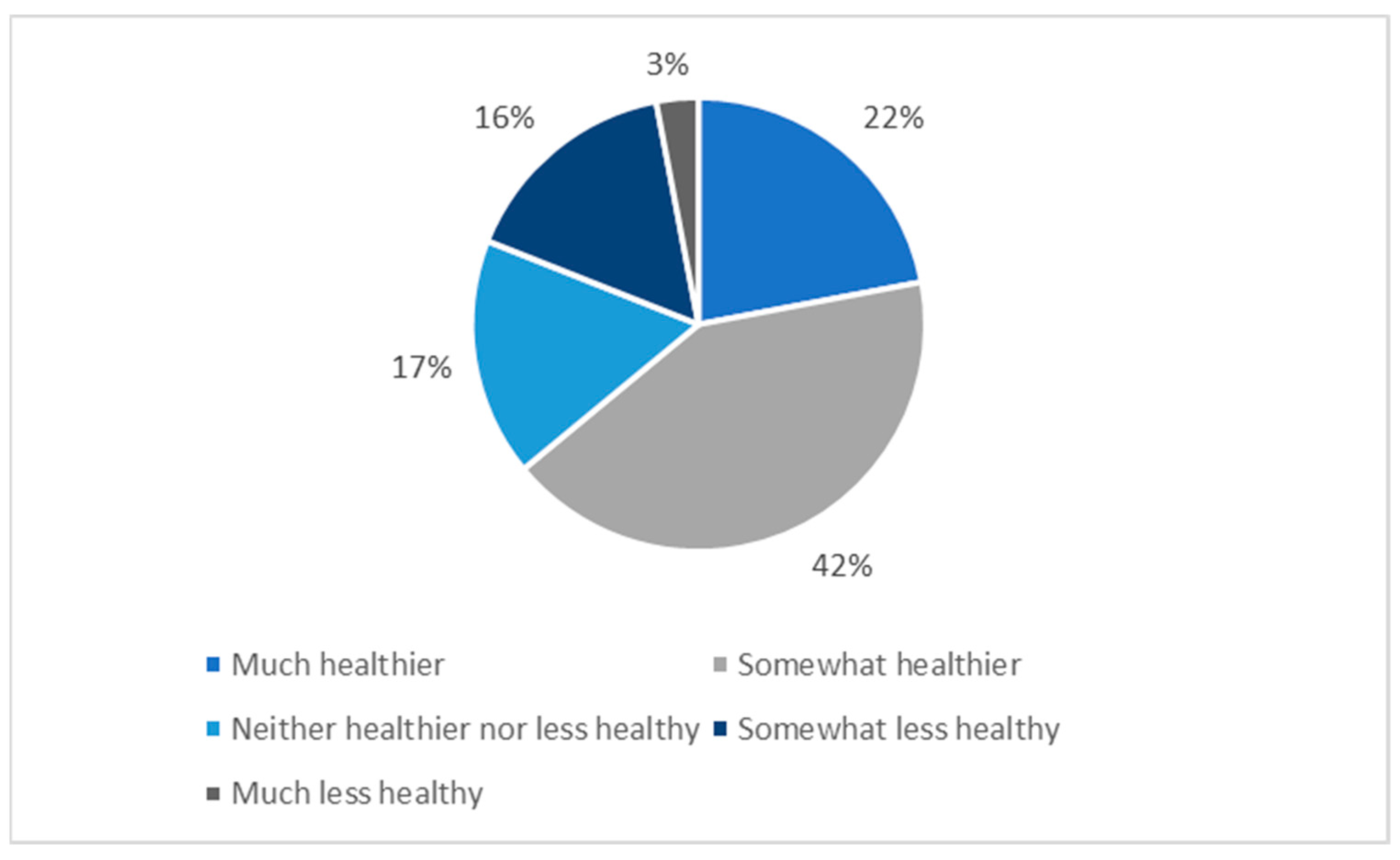
3.4.6. Change in Dietary Habits
3.5. Predictors of a Perceived Increase in Dietary Healthfulness
3.5.1. Subgroup Analyses According to Sex
3.5.2. Subgroup Analyses According to Age Group
3.5.3. Associations of COVID-19-Related Income Loss with Reasons for Dietary Change
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.; Zhang, T.; Zhang, Y.; Wang, Q. Statewide Stay-At-Home Directives on the Spread of COVID-19 in Metropolitan and Nonmetropolitan Counties in the United States. J. Rural Health 2020, 37, 222–223. [Google Scholar] [CrossRef]
- Belzunegui-Eraso, A.; Erro-Garcés, A. Teleworking in the context of the Covid-19 crisis. Sustainability 2020, 12, 3662. [Google Scholar] [CrossRef]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.L.; Haines, J. The impact of covid-19 on health behavior, stress, financial and food security among middle to high income canadian families with young children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef] [PubMed]
- Grashuis, J.; Skevas, T.; Segovia, M.S. Grocery shopping preferences during the COVID-19 pandemic. Sustainability 2020, 12, 5369. [Google Scholar] [CrossRef]
- Raghupathi, W.; Raghupathi, V. An empirical study of chronic diseases in the united states: A visual analytics approach. Int. J. Environ. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Prompetchara, E.; Ketloy, C.; Palaga, T. Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic. Asian Pac. J. Allergy Immunol. 2020, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jayawardena, R.; Misra, A. Balanced diet is a major casualty in COVID-19. Diabetes Metab. Syndr. 2020, 14, 1085–1086. [Google Scholar] [CrossRef]
- Liu, X.; Raghuvanshi, R.; Ceylan, F.D.; Bolling, B.W. Quercetin and Its Metabolites Inhibit Recombinant Human Angiotensin-Converting Enzyme 2 (ACE2) Activity. J. Agric. Food Chem. 2020, 68, 13982–13989. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, M.A.; Magdalena, G.; Ewa, M. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Kapczinski, F.; de Azevedo Cardoso, T.; Atienza-Carbonell, B.; Rosa, A.R.; Mota, J.C.; De Boni, R.B. The assessment of lifestyle changes during the COVID-19 pandemic using a multidimensional scale. Rev. Psiquiatr. Salud Ment. 2021, 14, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Russell, B.S.; Fendrich, M.; Finkelstein-Fox, L.; Hutchison, M.; Becker, J. Americans’ COVID-19 Stress, Coping, and Adherence to CDC Guidelines. J. Gen. Intern. Med. 2020, 35, 2296–2303. [Google Scholar] [CrossRef]
- Sims, R.; Gordon, S.; Garcia, W.; Clark, E.; Monye, D.; Callender, C.; Campbell, A. Perceived stress and eating behaviors in a community-based sample of African Americans. Eat. Behav. 2008, 9, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Ellison, B.; McFadden, B.; Rickard, B.J.; Wilson, N.L.W. Examining Food Purchase Behavior and Food Values During the COVID-19 Pandemic. Appl. Econ. Perspect. Policy 2021, 43, 58–72. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Leung, C.W. Food insecurity and COVID-19: Disparities in early effects for us adults. Nutrients 2020, 12, 1648. [Google Scholar] [CrossRef]
- Leung, C.W.; Epel, E.S.; Ritchie, L.D.; Crawford, P.B.; Laraia, B.A. Food Insecurity Is Inversely Associated with Diet Quality of Lower-Income Adults. J. Acad. Nutr. Diet. 2014, 114, 1943–1953. [Google Scholar] [CrossRef]
- Balanzá–Martínez, V.; Atienza–Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19—Time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the lifestyle changes during covid-19 pandemic in the residents of northern italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef]
- Hu, Z.; Lin, X.; Chiwanda Kaminga, A.; Xu, H. Impact of the COVID-19 Epidemic on Lifestyle Behaviors and Their Association With Subjective Well-Being Among the General Population in Mainland China: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e21176. [Google Scholar] [CrossRef] [PubMed]
- Oktaviani, J. Impact of lockdown due to COVID-19 outbreak: Lifestyle changes and Public Health Concerns in India Subhro. Sereal Untuk 2018, 51, 51. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Citores, M.G.; Bárbara, G.H.; Ruiz-Litago, F.; Sáenz, L.C.; Arija, V.; López-Sobaler, A.M.; de Victoria, E.M.; Ortega, R.M.; Partearroyo, T.; et al. Patterns of change in dietary habits and physical activity during lockdown in spain due to the covid-19 pandemic. Nutrients 2021, 13, 300. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Psychological responses and lifestyle changes among pregnant women with respect to the early stages of COVID-19 pandemic. Int. J. Soc. Psychiatry 2020, 67, 344–350. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.D.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2020, 16, e12731. [Google Scholar] [CrossRef]
- Lee, E.H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. (Korean. Soc. Nurs. Sci) 2012, 6, 121–127. [Google Scholar] [CrossRef] [Green Version]
- US Census Household Pulse Survey: Measuring Social and Economic Impacts during the Coronavirus Pandemic. Available online: https://www2.census.gov/programs-surveys/demo/technical-documentation/hhp/Phase3_Questionnaire_11_4_20_English.pdf (accessed on 20 November 2020).
- Cosgrove, K.; Vizcaino, M.; Wharton, C. COVID-19-related changes in perceived household food waste in the united states: A cross-sectional descriptive study. Int. J. Environ. Res. Public Health 2021, 18, 1104. [Google Scholar] [CrossRef] [PubMed]
- Paolacci, G.; Chandler, J.; Ipeirotis, P.G. Running experiments on Amazon mechanical turk. Judgm. Decis. Mak. 2010, 5, 411–419. [Google Scholar]
- Husain, W.; Ashkanani, F. Does COVID-19 change dietary habits and lifestyle behaviours in Kuwait: A community-based cross-sectional study. Environ. Health Prev. Med. 2020, 25, 1–13. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the ECLB-COVID19 multicenter study. Biol. Sport 2021, 38, 9–21. [Google Scholar] [CrossRef]
- Cransac-Miet, A.; Zeller, M.; Chagué, F.; Faure, A.S.; Bichat, F.; Danchin, N.; Boulin, M.; Cottin, Y. Impact of COVID-19 lockdown on lifestyle adherence in stay-at-home patients with chronic coronary syndromes: Towards a time bomb. Int. J. Cardiol. 2021, 323, 285–287. [Google Scholar] [CrossRef]
- Marty, L.; de Lauzon-Guillain, B.; Labesse, M.; Nicklaus, S. Food choice motives and the nutritional quality of diet during the COVID-19 lockdown in France. Appetite 2021, 157, 105005. [Google Scholar] [CrossRef] [PubMed]
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Song, M. Psychological stress responses to COVID-19 and adaptive strategies in China. World Dev. 2020, 136, 105107. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.D.U.; Bodrud-Doza, M.; Khan, R.M.; Haque, M.A.; Mamun, M.A. Exploring COVID-19 stress and its factors in Bangladesh: A perception-based study. Heliyon 2020, 6, e04399. [Google Scholar] [CrossRef]
- Peters, A.; Rospleszcz, S.; Greiser, K.H.; Dallavalle, M.; Berger, K. The Impact of the COVID-19 Pandemic on Self-Reported Health. Dtsch. Arztebl. Int. 2020, 117, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Recchi, E.; Ferragina, E.; Helmeid, E.; Pauly, S.; Safi, M.; Sauger, N.; Schradie, J. The “Eye of the Hurricane” Paradox: An Unexpected and Unequal Rise of Well-Being During the Covid-19 Lockdown in France. Res. Soc. Stratif. Mobil. 2020, 68, 100508. [Google Scholar] [CrossRef]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Heal. Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Huyghe, E.; Verstraeten, J.; Geuens, M.; Van Kerckhove, A. Clicks as a Healthy Alternative to Bricks: How Online Grocery Shopping Reduces Vice Purchases. J. Mark. Res. 2017, 54, 61–74. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Hung, P.; Alberg, A.J.; Hair, N.L.; Liu, J. Variations in health behaviors among pregnant women during the COVID-19 pandemic. Midwifery 2021, 95, 102929. [Google Scholar] [CrossRef] [PubMed]
- Driessen, G. The Coronavirus Relief Fund (CARES Act, Title V): Background and State and Local Allocations. Available online: https://crsreports.congress.gov/product/pdf/R/R46298 (accessed on 15 March 2021).
- Raifman, J.; Bor, J.; Venkataramani, A. Association Between Receipt of Unemployment Insurance and Food Insecurity Among People Who Lost Employment During the COVID-19 Pandemic in the United States. JAMA Netw. Open 2021, 4, e2035884. [Google Scholar] [CrossRef]
- Carlson, A.; Frazão, E. Food costs, diet quality and energy balance in the United States. Physiol. Behav. 2014, 134, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Kuhns, A.; Volpe, R. Assessing the Impact of the Great Recession on Healthfulness of Food Purchase Choices. In Proceedings of the Agricultural & Applied Economics Association’s 2014 AAEA Annual Meeting, Minneapolis, Minnesota, 27–29 July 2014. [Google Scholar] [CrossRef]
- Todd, J.; Morrison, R.M. Less Eating Out, Improved Diets, and More Family Meals in the Wake of the Great Recession. Available online: https://www.ers.usda.gov/amber-waves/2014/march/less-eating-out-improved-diets-and-more-family-meals-in-the-wake-of-the-great-recession/ (accessed on 23 March 2021).
- Cawley, J. The economics of childhood obesity. Health Aff. 2010, 29, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, L.M.; Szczypka, G.; Chaloupka, F.J.; Braunschweig, C.L. Nutritional content of television food advertisements seen by children and adolescents in the United States. Pediatrics 2007, 120, 576–583. [Google Scholar] [CrossRef]
- Halford, J.C.G.; Boyland, E.J.; Hughes, G.M.; Stacey, L.; McKean, S.; Dovey, T.M. Beyond-brand effect of television food advertisements on food choice in children: The effects of weight status. Public Health Nutr. 2008, 11, 897–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, B.J. Food for health-The use of nutrient content, health, and structure/function claims in food advertisements. J. Advert. 2003, 32, 47–55. [Google Scholar] [CrossRef]
- Khaled, K.; Tsofliou, F.; Hundley, V.; Helmreich, R.; Almilaji, O. Perceived stress and diet quality in women of reproductive age: A systematic review and meta-analysis. Nutr. J. 2020, 19, 92. [Google Scholar] [CrossRef]
- Mayasari, N.R.; Ho, D.K.N.; Lundy, D.J.; Skalny, A.V.; Tinkov, A.A.; Teng, I.C.; Wu, M.C.; Faradina, A.; Mohammed, A.Z.M.; Park, J.M.; et al. Impacts of the COVID-19 pandemic on food security and diet-related lifestyle behaviors: An analytical study of google trends-based query volumes. Nutrients 2020, 12, 3103. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency | Percentage | |
|---|---|---|
| Sex | ||
| Male | 491 | 51.3 |
| Female | 467 | 48.7 |
| Age range (years) | ||
| 18–29 | 205 | 21.4 |
| 30–39 | 331 | 34.6 |
| 40–49 | 200 | 20.9 |
| 50–59 | 120 | 12.5 |
| 60+ | 102 | 10.6 |
| Education | ||
| Less than high school | 3 | 0.3 |
| Some high school | 1 | 0.1 |
| High school graduate | 51 | 5.3 |
| Some college | 109 | 11.4 |
| Associate’s degree | 83 | 8.7 |
| Bachelor’s degree | 564 | 58.9 |
| Graduate degree | 147 | 15.3 |
| Marital status | ||
| Married | 627 | 65.4 |
| Widowed | 24 | 2.5 |
| Divorced | 63 | 6.6 |
| Separated | 15 | 1.6 |
| Never married | 229 | 23.9 |
| Frequency | Percentage | |
|---|---|---|
| Household income | ||
| Less than $25,000 | 125 | 13.0 |
| $25,000–$34,999 | 91 | 9.5 |
| $35,000–$49,999 | 173 | 18.1 |
| $50,000–$74,999 | 276 | 28.8 |
| $75,000–$99,999 | 156 | 16.3 |
| $100,000–$149,999 | 97 | 10.1 |
| $150,000–$199,999 | 23 | 2.4 |
| $200,000+ | 17 | 1.8 |
| Household size | ||
| 1 | 130 | 13.6 |
| 2 | 220 | 23.0 |
| 3 | 184 | 19.2 |
| 4 | 278 | 29.0 |
| 5+ | 144 | 15.0 |
| Number of children | ||
| 0 | 366 | 38.2 |
| 1 | 264 | 27.6 |
| 2 | 248 | 25.9 |
| 3 | 41 | 4.3 |
| 4+ | 39 | 4.1 |
| Independent Variable | B | S.E. | Wald | p-Value | OR (95% CI) |
|---|---|---|---|---|---|
| Sex | −0.16 | 0.14 | 1.22 | 0.27 | 0.85 (0.65–1.13) |
| Household income (2019) | 0.02 | 0.04 | 0.28 | 0.597 | 1.02 (0.94–1.12) |
| Change in frequency meals with family in front of the TV | 0.17 | 0.06 | 6.79 | 0.009 | 1.18 (1.04–1.34) * |
| COVID-19 income loss | 0.50 | 0.15 | 10.91 | <0.001 | 1.64 (1.22–2.21) * |
| Shift to telecommuting | 0.10 | 0.09 | 1.03 | 0.309 | 1.10 (0.92–1.32) |
| Change in food ad exposure | 0.42 | 0.07 | 35.70 | <0.001 | 1.52 (1.32–1.74) * |
| Perceived stress scale score | 0.04 | 0.01 | 12.39 | <0.001 | 1.04 (1.02–1.07) * |
| Perceived current health | 0.42 | 0.09 | 24.45 | <0.001 | 1.53 (1.29–1.81) * |
| Model χ2 = 153.14, p < 0.001 Hosmer and Lemeshow χ2 = 5.93, p = 0.655 Pseudo R2 = 0.197 n = 958 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosgrove, K.; Wharton, C. Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study. Nutrients 2021, 13, 2097. https://doi.org/10.3390/nu13062097
Cosgrove K, Wharton C. Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study. Nutrients. 2021; 13(6):2097. https://doi.org/10.3390/nu13062097
Chicago/Turabian StyleCosgrove, Kelly, and Christopher Wharton. 2021. "Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study" Nutrients 13, no. 6: 2097. https://doi.org/10.3390/nu13062097
APA StyleCosgrove, K., & Wharton, C. (2021). Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study. Nutrients, 13(6), 2097. https://doi.org/10.3390/nu13062097