
Consumption of Monounsaturated Fatty Acids Is Associated with Improved Cardiometabolic Outcomes in Four African-Origin Populations Spanning the Epidemiologic Transition


 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Dietary Fiber Intake
1.2. Polyunsaturated Fatty Acids (PUFAs)
1.3. Monounsaturated Fatty Acid Intake
2. Methods
2.1. Study Population and Ethics Approval
2.2. Anthropometry and Biochemical Measures
2.3. Dietary Intake
2.4. Physical Activity Measurement
2.5. Clinical Outcomes
- Waist circumference > 102 cm in males and >88 cm in females;
- Elevated blood pressure (≥130/85 mmHg) or receiving treatment;
- Hypertriglyceridemia (≥150 mg/dL) or receiving treatment;
- Low high-density lipoprotein (HDL) cholesterol (<40 mg/dL in males and <50 mg/dL in female) or receiving treatment;
- Elevated fasting plasma glucose (>100 mg/dL) or receiving treatment.
2.6. Statistical Analyses
3. Results
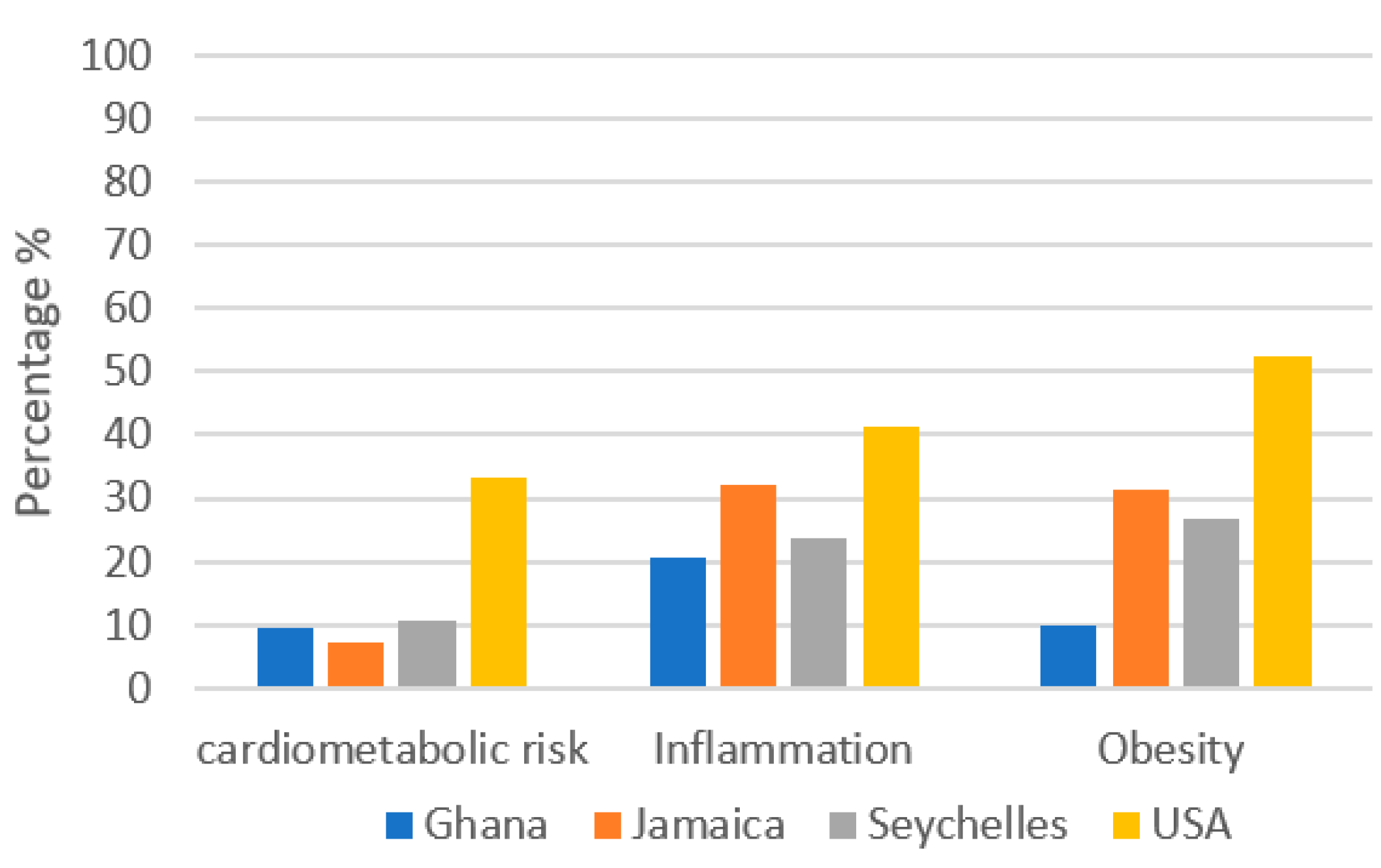
3.1. Cardiometabolic Risk across the Epidemiologic Transition
3.2. Dietary Fiber Analysis
3.3. Omega-3 and Omega-6 Fatty Acid Analysis
3.4. The Association of Monounsaturated Fatty Acids and Cardiometabolic Risk across the Epidemiological Transition
4. Discussion
4.1. Dietary Fiber Intake
4.2. Omega-3 and Omega-6 Fatty Acid Intake
4.3. Monounsaturated Fatty Acid Intake
4.4. Significance of Site
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Nsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity commissioned by the ILSI Europe Metabolic Syndrome and Diabetes Task Force. Br. J. Nutr. 2011, 106, S5–S78. [Google Scholar] [CrossRef] [PubMed]
- Eckert, S. Urbanization and Health in Developing Countries: A Systematic Review. World Health Popul. 2014, 15, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Dugas, L.R.; Forrester, T.E.; Plange-Rhule, J.; Bovet, P.; Lambert, E.V.; Durazo-Arvizu, R.A.; Cao, G.; Cooper, R.S.; Khatib, R.; Tonino, L.; et al. Cardiovascular risk status of Afro-origin populations across the spectrum of economic development: Findings from the Modeling the Epidemiologic Transition Study. BMC Public Health 2017, 17, 438. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.D.; Brashear, M.M.; Gupta, A.K.; Rood, J.C.; Ryan, D.H. Incremental Weight Loss Improves Cardiometabolic Risk in Extremely Obese Adults. Am. J. Med. 2011, 124, 931–938. [Google Scholar] [CrossRef]
- Liu, A.G.; Ford, N.A.; Hu, F.B.; Zelman, K.M.; Mozaffarian, D.; Kris-Etherton, P.M. A healthy approach to dietary fats: Understanding the science and taking action to reduce consumer confusion. Nutr. J. 2017, 16, 1–15. [Google Scholar] [CrossRef]
- Galisteo, M.; Duarte, J.; Zarzuelo, A. Effects of dietary fibers on disturbances clustered in the metabolic syndrome. J. Nutr. Biochem. 2008, 19, 71–84. [Google Scholar] [CrossRef]
- Wong, J.M.W.; de Souza, R.; Kendall, C.W.C.; Emam, A.; Jenkins, D.J.A. Colonic Health: Fermentation and Short Chain Fatty Acids. J. Clin. Gastroenterol. 2006, 40, 235–243. [Google Scholar] [CrossRef]
- Marlett, J.; Slavin, J.L. Position of the American Dietetic Association: Health Implications of Dietary Fiber. J. Am. Diet. Assoc. 1997, 97, 1157–1159. [Google Scholar] [CrossRef]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Weickert, M.O.; Mohlig, M.; Pfeiffer, A.F.H.; Koebnick, C.; Holst, J.J.; Namsolleck, P.; Ristow, M.; Osterhoff, M.; Rochlitz, H.; Rudovich, N.; et al. Impact of cereal fibre on glucose-regulating factors. Diabetologia 2005, 48, 2343–2353. [Google Scholar] [CrossRef]
- Simopoulos, A.P. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef] [Green Version]
- Raheja, B.S.; Sadikot, S.M.; Phatak, R.B.; Rao, M.B. Significane of the n-6/n-3 ratio for insulin action in diabetes. Ann. N. Y. Acad. Sci. 1993, 683, 258–271. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The importance of the omega-6/omega-3 Fatty Acid ratio in cardiovascular disease and other chronic disease. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Lincoff, A.M.; Garcia, M.; Bash, D.; Ballantyne, C.M.; Barter, P.J.; Davidson, M.H.; Kastelein, J.J.P.; Koenig, W.; McGuire, D.K.; et al. Effect of High-Dose Omega-3 Fatty Acids vs. Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk: The STRENGTH Randomized Clinical Trial. JAMA 2020, 324, 2268–2280. [Google Scholar] [CrossRef]
- Dennis, E.A.; Norris, P. Eicosanoid storm in infection and inflammation. Nat. Rev. Immunol. 2015, 15, 511–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balk, E.M.; Lichtenstein, A.H.; Chung, M.; Kupelnick, B.; Chew, P.; Lau, J. Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: A systematic review. Atherosclerosis 2006, 189, 19–30. [Google Scholar] [CrossRef]
- Stanton, A.V.; James, K.; Brennan, M.M.; O’Donovan, F.; Buskandar, F.; Shortall, K.; El-Sayed, T.; Kennedy, J.; Hayes, H.; Fahey, A.G.; et al. Omega-3 index and blood pressure responses to eating foods naturally enriched with omega-3 polyunsaturated fatty acids: A randomized controlled trial. Sci. Rep. 2020, 10, 15444. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Del Gobbo, L.; Tintle, N.L. Te Omega-3 Index and relative risk for coronary heart disease mortality: Estimation from 10 cohort studies. Atherosclerosis 2017, 262, 51–54. [Google Scholar] [CrossRef]
- Harris, W.S.; Harris, W.S. n-3 fatty acids and serum lipoproteins: Human studies. Am. J. Clin. Nutr. 1997, 65, 1645S–1654S. [Google Scholar] [CrossRef]
- Eslick, G.D.; Howe, P.; Smith, C.; Priest, R.; Bensoussan, A. Benefits of fish oil supplementation in hyperlipidemia: A systematic review and meta-analysis. Int. J. Cardiol. 2009, 136, 4–16. [Google Scholar] [CrossRef]
- Adili, R.; Hawley, M.; Holinstat, M. Regulation of platelet function and thrombosis by omega-3 and omega-6 polyunsaturated fatty acids. Prostaglandins Lipid Mediat. 2018, 139, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Monounsaturated Fatty Acids and Risk of Cardiovascular Disease: Synopsis of the Evidence Available from Systematic Reviews and Meta-Analyses. Nutrients 2012, 4, 1989–2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutrition Committee; Kris-Etherton, P.M. AHA Science Advisory: Monounsaturated Fatty Acids and Risk of Cardiovascular Disease. J. Nutr. 1999, 129, 2280–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Strasser, B.; Hoffmann, G. Effects of monounsaturated fatty acids on glycemic control in patients with abnormal glucose metabolism: A systematic review and metaanalysis. Ann. Nutr. Metab. 2011, 58, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Garg, A. High-monounsaturated-fat diets for patients with diabetes mellitus: A meta-analysis. Am. J. Clin. Nutr. 1998, 67, 577S–582S. [Google Scholar] [CrossRef]
- Shah, M.; Adams-Huet, B.; Garg, A. Effect of high-carbohydrate or high-cis-monounsaturated fat diets on blood pressure: A meta-analysis of intervention trials. Am. J. Clin. Nutr. 2007, 85, 1251–1256. [Google Scholar] [CrossRef] [Green Version]
- Miura, K.; Stamler, J.; Brown, I.J. Relationship of dietary monounsaturated fatty acids to blood pressure: The International Study of Macro/Micronutrients and Blood Pressure. J. Hypertens. 2013, 31, 1144–1150. [Google Scholar] [CrossRef] [Green Version]
- Teres, S.; Barceló-Coblijn, G.; Benet, M.; Alvarez, R.; Bressani, R.; Halver, J.E.; Escriba, P.V. Oleic acid content is responsible for the reduction in blood pressure induced by olive oil. Proc. Natl. Acad. Sci. USA 2008, 105, 13811–13816. [Google Scholar] [CrossRef] [Green Version]
- Luke, A.; Bovet, P.; Brage, S.; Ekelund, U.; Steyn, N.P.; Forrester, T.; Lambert, E.V.; Plange-Rhule, J.; Schoeller, D.; Dugas, L.R.; et al. Protocol for the modeling the epidemiologic transition study: A longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public Health 2011, 11, 927. [Google Scholar] [CrossRef] [Green Version]
- Barro, R.J.; Lee, J.W. A New Data Set of Educational Attainment in the World, 1950–2010; The National Bureau of Economic Research: Cambridge, MA, USA, 2011; Available online: http://www.nber.org/papers/w15902 (accessed on 15 May 2018).
- Carriquiry, A.L. Estimation of Usual Intake Distributions of Nutrients and Foods. J. Nutr. 2003, 133, 601S–608S. [Google Scholar] [CrossRef] [Green Version]
- Carriquiry, A.L.; Fuller, W.A.; Goyeneche, J.J.; Dodd, K.W. Estimation of the Usual Intake Distributions of Ratios of Dietary Components; Center for Agricultural and Rural Development, Iowa State University: Ames, IA, USA, 1995. [Google Scholar]
- Guenther, P.; Kott, P.; Carriquiry, A.L. Development of an Approach for Estimating Usual Nutrient Intake Distributions at the Population Level. J. Nutr. 1997, 127, 1106–1112. [Google Scholar] [CrossRef] [Green Version]
- Steyn, N.P.; Nel, J.H.; Parker, W.-A.; Ayah, R.; Mbithe, D. Dietary, social, and environmental determinants of obesity in Kenyan women. Scand. J. Public Health 2010, 39, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Luke, A.; Bovet, P.; Plange-Rhule, J.; Forrester, T.; Lambert, E.V.; Schoeller, D.; Dugas, L.R.; Durazo-Arvizu, R.; Shoham, D.; Cao, G.; et al. A mixed ecologic-cohort comparison of physical activity & weight among young adults from five populations of African origin. BMC Public Health 2014, 14, 397. [Google Scholar] [CrossRef] [Green Version]
- Dugas, L.R.; Bovet, P.; Brage, S.; Ekelund, U.; Luke, A.; Forrester, T.; Lambert, E.V.; Plange-Rhule, J.; Durazo-Arvizu, R.; Shoham, D.; et al. Comparisons of intensity-duration patterns of physical activity in the US, Jamaica and 3 African countries. BMC Public Health 2014, 14, 882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAS Programs for Analyzing NHANES 2003–2004 Accelerometer Data. 2014. Available online: http://appliedresearch.cancer.gov/nhanes_pam/ (accessed on 25 July 2014).
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- National Cholesterol Education Program; Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- American Heart Association; Heart, L.N.; Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.; Gordon, D.J.; Krauss, R.M.; et al. Diagnosis and management of the metabolic syndrome. An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Exec. Summ. Cardiol. Rev. 2006, 13, 322–327. [Google Scholar]
- Ford, E.S.; Giles, W.H.; Mokdad, A.H.; Myers, G.L. Distribution and Correlates of C-Reactive Protein Concentrations among Adult US Women. Clin. Chem. 2004, 50, 574–581. [Google Scholar] [CrossRef]
- Institute of Medicine (U.S.). Panel on Macronutrients. II; QP141.D529 2005; Institute of Medicine (U.S.), Standing Committee on the Scientific Evaluation of Dietary Reference Intakes: Washington, DC, USA, 2005.
- The Global Organisation for EPA and DHA recommendations for EPA and HHA. Available online: https://www.issfal.org/goed-recommendations-for-epa-dha (accessed on 12 July 2021).
- The Facts on Fats. 50 Years of American Heart Association: Dietary Fats Recommendations. Available online: https://www.heart.org/-/media/files/healthy-living/company-collaboration/inap/dietary-fat-recommendations-timeline-pdf-ucm_474998.pdf (accessed on 12 July 2021).
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- GBD 2013 Risk Factors Collaborators; Forouzanfar, M.H.; Alexander, L. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [Green Version]
- Windey, K.; De Preter, V.; Verbeke, K. Relevance of protein fermentation to gut health. Mol. Nutr. Food Res. 2011, 56, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, K.J.; Conlon, M.A.; Young, G.; Topping, D.L.; Hu, Y.; Winter, J.; Bird, A.R.; Cobiac, L.; Kennedy, N.A.; Michael, M.Z.; et al. Dietary Manipulation of Oncogenic MicroRNA Expression in Human Rectal Mucosa: A Randomized Trial. Cancer Prev. Res. 2014, 7, 786–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, K.D.; Van Elswyk, M.E.; Higgins, M.R.; Weatherford, C.A.; Salem, N. Global survey of the omega-3 fatty acids, docosahexaenoic acid and eicosapentaenoic acid in the blood stream of healthy adults. Prog. Lipid Res. 2016, 63, 132–152. [Google Scholar] [CrossRef] [PubMed]
- Kleber, M.E.; Delgado, G.E.; Lorkowski, S.; März, W.; Von Schacky, C. Omega-3 fatty acids and mortality in patients referred for coronary angiography. The Ludwigshafen Risk and Cardiovascular Health Study. Atherosclerosis 2016, 252, 175–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 7th ed.; U.S. Government Printing Office: Washington, DC, USA, 2010.
- Bederska-Łojewska, D.; Orczewska-Dudek, S.; Pieszka, M. Metabolism of arachidonic acid, its concentration in animal products and influence on inflammatory processes in the human body: A review/Metabolizm kwasu arachidonowego, jego stężenie w produktach zwierzęcych i wpływ na procesy zapalne w organizmie człowieka—artykuł przeglądowy. Ann. Anim. Sci. 2013, 13, 177–194. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, M.U.; O’Reilly, E.J.; Heitmann, B.L.; Pereira, M.; Bälter, K.; Fraser, G.E.; Goldbourt, U.; Hallmans, G.; Knekt, P.; Liu, S.; et al. Major types of dietary fat and risk of coronary heart disease: A pooled analysis of 11 cohort studies. Am. J. Clin. Nutr. 2009, 89, 1425–1432. [Google Scholar] [CrossRef]
- Wang, D.D.; Li, Y.; Chiuve, S.E.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Association of Specific Dietary Fats with Total and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1134–1145. [Google Scholar] [CrossRef]
- Rohem, E. The evidence-based Mediterranean diet reduces coronary heart disease risk, and plant-derived monounsaturated fats may reduce coronary heart disease risk. Am. J. Clin. Nutr. 2009, 90, 697–698. [Google Scholar] [CrossRef] [Green Version]
- Gaesser, G. Perspective: Refined Grains and Health: Genuine Risk, or Guilt by Association? Adv. Nutr. 2019, 10, 361–371. [Google Scholar] [CrossRef]
- Odegaard, A.O.; Koh, W.-P.; Arakawa, K.; Yu, M.C.; Pereira, M.A. Soft Drink and Juice Consumption and Risk of Physician-diagnosed Incident Type 2 Diabetes: The Singapore Chinese Health Study. Am. J. Epidemiol. 2010, 171, 701–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M.; Du, S. Dynamics of the Nutrition Transition toward the Animal Foods Sector in China and its Implications: A Worried Perspective. J. Nutr. 2003, 133, 3898S–3906S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M.; Slining, M.M. New dynamics in global obesity facing low- and middle-income countries. Obes. Rev. 2013, 14, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, I.; Keating, S.; Baker, M.; Johnson, N.A. A systematic review and meta-analysis of the effect of aerobic vs. resistance exercise training on visceral fat. Obes. Rev. 2011, 13, 68–91. [Google Scholar] [CrossRef]
- Kang, M.; Park, S.-Y.; Boushey, C.J.; Wilkens, L.R.; Monroe, K.R.; Le Marchand, L.; Kolonel, L.N.; Murphy, S.P.; Paik, H.-Y. Portion Sizes from 24-Hour Dietary Recalls Differed by Sex among Those Who Selected the Same Portion Size Category on a Food Frequency Questionnaire. J. Acad. Nutr. Diet. 2018, 118, 1711–1718. [Google Scholar] [CrossRef]
- Metcalf, R.G.; Cleland, L.G.; Gibson, R.; Roberts-Thomson, K.C.; Edwards, J.R.; Sanders, P.; Stuklis, R.; James, M.J.; Young, G.D. Relation between blood and atrial fatty acids in patients undergoing cardiac bypass surgery. Am. J. Clin. Nutr. 2010, 91, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S.; Tintle, N.L.; Etherton, M.R.; Vasan, R.S. Erythrocyte long-chain omega-3 fatty acid levels are inversely associated with mortality and with incident cardiovascular disease: Te Framingham Heart Study. J. Clin. Lipidol. 2018, 12, 718–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Ghana (n = 487) | Jamaica (n = 398) | Seychelles (n = 484) | United States (n = 444) | |
|---|---|---|---|---|
| Demographics: | ||||
| Female (n, %) | 287 (58.9) | 244 (61.3) | 261 (53.9) | 227 (51.2) |
| Age | 34.2 ± 6.7 | 34.4 ± 6.1 | 36.2 ± 5.6 | 35.3 ± 5.6 |
| Anthropometrics | ||||
| Weight (kg) | 63.4 ± 11.5 | 75.9 ± 17.1 | 75.9 ± 17.0 | 92.2 ± 24.3 |
| Height (cm) | 162.6 ± 8.2 | 168.1 ± 8.9 | 167.2 ± 8.8 | 169.9 ± 9.0 |
| BMI (kg/m2) | 24.1 ± 4.5 | 27.0 ± 6.5 | 27.1 ± 5.6 | 32.0 ± 8.5 |
| Waist circumference (cm) | 81.2 ± 12.0 | 87.1 ± 14.1 | 88.7 ± 12.0 | 99.8 ± 20.4 |
| Systolic blood pressure (mmHg) | 113.8 ± 14.8 | 118.4 ± 14.2 | 116.2 ± 14.7 | 122.6 ± 16.3 |
| Diastolic blood pressure (mmHg) | 67.1 ± 11.3 | 71.7 ± 11.3 | 73.0 ± 10.7 | 80.5 ± 12.7 |
| Biochemical Measures | ||||
| Cholesterol (mg/dL) | 161.3 ± 35.3 | 162.8 ± 33.9 | 170.9 ± 35.4 | 181.0 ± 38.4 |
| HDL-C (mg/dL) | 46.1 ± 14.4 | 46.5 ± 12.1 | 47.7 ± 12.8 | 50.8 ± 14.6 |
| Triglycerides (mg/dL) | 81.8 ± 40.2 | 73.2 ± 36.4 | 79.8 ± 60.6 | 97.5 ± 57.5 |
| Blood glucose (mg/dL) | 100.3 ± 12.3 | 92.9 ± 9.3 | 100.6 ± 29.2 | 103.2 ± 32.9 |
| C-reactive peptide (mg/dL) | 4.7 ± 13.3 | 4.2 ± 6.3 | 3.1 ± 4.5 | 6.0 ± 11.0 |
| Lifestyle habits | ||||
| Smoker or ex-smoker (n, %) | 21 (4.3) | 130 (32.7) | 106 (21.9) | 224 (50.6) |
| Consumes alcohol (n, %) | 66 (13.6) | 160 (40.2) | 204 (42.2) | 206 (46.5) |
| Moderate to vigorous PA (min/day) | 34.3 ± 22.6 | 23.2 ± 19.3 | 28.9 ± 20.9 | 23.3 ± 28.9 |
| Ghana (n = 487) | Jamaica (n = 398) | Seychelles (n = 484) | United States (n = 444) | p-Value | |
|---|---|---|---|---|---|
| Energy (kcal) | 1848.8 ± 496.3 | 1893 ± 582.8 | 1843.6 ± 593.9 | 2294.5 ± 891.8 | <0.0001 |
| % Energy from fat | 21.6 ± 9.1 | 25.7 ± 6.6 | 28.4 ± 7.7 | 36.6 ± 7.0 | <0.0001 |
| % Energy from saturated fat | 7.1 ± 4.1 | 9.5 ± 4.0 | 8.4 ± 2.9 | 11.8 ± 2.9 | <0.0001 |
| % Energy from monounsaturated fat | 8.2 ± 3.7 | 8.5 ± 2.7 | 9.0 ± 3.0 | 13.6 ± 3.1 | <0.0001 |
| % Energy from polyunsaturated fat | 4.6 ± 2.5 | 5.4 ± 2.1 | 8.6 ± 3.4 | 7.9 ± 2.8 | <0.0001 |
| % Energy from carbohydrates | 65.8 ± 10.4 | 58.6 ± 8.4 | 51.3 ± 9.4 | 45.8 ± 9.4 | <0.0001 |
| % Energy from protein | 11.9 ± 4.0 | 14.6 ± 3.9 | 18.4 ± 4.7 | 15.5 ± 4.1 | <0.0001 |
| Dietary fiber | 24.9 ± 9.7 | 15.9 ± 8.3 | 13.6 ± 7.2 | 14.2 ± 7.1 | <0.0001 |
| Soluble fiber (g) | 6.0 ± 2.8 | 4.7 ± 2.6 | 3.9 ± 2.2 | 4.6 ± 2.4 | <0.0001 |
| Insoluble fiber (g) | 18.8 ± 7.5 | 11.2 ± 6.1 | 9.6 ± 5.4 | 9.5 ± 5.4 | <0.0001 |
| Meeting 14 g fiber/1000 kcal (n, %) | 207 (42.5) | 35 (8.8) | 28 (5.8) | 14 (3.2) | <0.0001 |
| Omega 3: | |||||
| Average EPA + DHA g/day | 0.65 ± 0.81 | 0.30 ± 0.40 | 0.69 ± 0.64 | 0.15 ± 2.7 | <0.0001 |
| EPA + DHA > 0.5 g/day (n, %) | 193 (39.6) | 76 (19.1) | 252 (52.1) | 32 (7.2) | <0.0001 |
| AA/EPA + DHA ratio | |||||
| Average AA/EPA + DHA ratio | 10.0 ± 9.5 | 8.3 ± 3.1 | 1.0 ± 2.7 | 6.5 ± 25.2 | <0.0001 |
| AA/EPA + DHA ratio < 4:1 (n, %) | 85 (17.3) | 32 (6.4) | 31 (6.3) | 3 (0.7) | <0.0001 |
| Monounsaturated fatty acids: | |||||
| %TEC | 10.0 ± 4.2 | 10.8 ± 3.1 | 11.4 ± 3.6 | 16.8 ± 3.7 | <0.0001 |
| >15% TEC (n, %) | 66 (13.5) | 32 (8.0) | 76 (15.7) | 309 (69.8) | <0.0001 |
| Total Fiber Analysis | ||||||
| Not Controlled for Site | Controlled for Site | |||||
| Quartiles of Total Fiber | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| 0.0–10.34 g (Q1) | 1.96 (1.25, 3.06) * | 1.70 (1.18, 2.43) * | 2.76 (1.90, 4.02) * | 1.43 (0.85, 2.42) | 1.27 (0.84, 1.93) | 1.05 (0.68, 1.62) |
| 10.34–15.05 g (Q2) | 1.60 (1.05, 2.42) * | 1.67 (1.20, 2.32) * | 2.52 (1.78, 3.57) * | 1.40 (0.86, 2.25) | 1.37 (0.95, 1.99) | 1.23 (0.82, 1.83) |
| 15.05–22.03 (Q3) | 0.97 (0.63, 1.49) | 1.21 (.87, 1.67) | 1.62 (1.14, 2.29) * | .86 (0.54, 1.36) | 1.07 (0.76, 1.51) | 1.01 (0.69, 1.48) |
| >22.03(Q4) | Reference | Reference | Reference | Reference | Reference | Reference |
| Soluble Fiber Analysis | ||||||
| Quartiles of Soluble Fiber | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| 0.0–3.00 g (Q1) | 1.83 (1.17, 2.84) * | 1.25 (0.88, 1.80) | 1.85 (1.28, 2.67) * | 1.59 (0.98, 2.56) | 1.08 (0.74, 1.58) | 1.13 (0.75, 1.67) |
| 3.00–4.34 g (Q2) | 1.37 (0.90, 2.08) | 1.56 (1.12, 2.16) | 1.78 (1.26, 2.51) | 1.19 (0.76, 1.87) | 1.37 (0.97, 1.93) | 1.15 (0.79, 1.67) |
| 4.34–6.00 (Q3) | 1.16 (0.77, 1.76) | 1.08 (0.78, 1.49) | 1.55 (1.11, 2.16) | 1.05 (0.68, 1.61) | 1.01 (0.72, 1.40) | 1.28 (0.90, 1.84) |
| >6.00 (Q4) | Reference | Reference | Reference | Reference | Reference | Reference |
| Insoluble Fiber Analysis | ||||||
| Quartiles of Insoluble Fiber | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM risk Factors | Inflammation | Obesity |
| 0.0–6.99 g (Q1) | 1.80 (1.16, 2.79) * | 1.46 (1.03, 2.07) * | 2.68 (1.86, 3.86) * | 1.25 (0.74, 2.09) | 1.05 (0.70, 1.57) | 1.01 (0.66, 1.55) |
| 6.99–10.57 g (Q2) | 1.52 (1.00, 2.30) * | 1.59 (1.15, 2.20) * | 2.32 (1.65, 3.28) * | 1.24 (0.77, 1.99) | 1.23 (0.85, 1.78) | 1.06 (0.71, 1.58) |
| 10.57–16.29 (Q3) | 1.01 (0.65, 1.56) | 1.04 (0.75, 1.45) | 1.54 (1.08, 2.18) * | 0.95 (0.60, 1.51) | 0.91 (0.64, 1.29) | 1.00 (0.67, 1.46) |
| >16.29 (Q4) | Reference | Reference | Reference | Reference | Reference | Reference |
| Not Controlled for Site | Controlled for Site | |||||
| AA/EPA + DHA 4:1 | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| 4:1 | Reference | Reference | Reference | Reference | Reference | Reference |
| >4:1 | 1.80(1.24, 2.60) * | 1.47 (1.06, 2.03) * | 1.72 (1.25, 2.39) * | 1.03 (0.69, 1.55) | 1.04 (0.74, 1.47) | 0.85 (0.60, 1.22) |
| Quartiles of EPA + DHA | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| 0.0–0.07 g (Q1) | 2.16(1.45, 3.20) * | 1.59 (1.17, 2.16) * | 2.06(1.50, 2.82) * | 1.05 (0.65, 1.70) | 0.98 (0.69, 1.41) | 0.80 (0.54, 1.18) |
| 0.07–0.23 g (Q2) | 1.30 (0.85, 1.97) | 1.08 (0.78, 1.49) | 1.20 (0.87, 1.67) | 0.83 (0.52, 1.34) | 0.82 (0.58, 1.15) | 0.72 (0.49, 1.04) |
| 0.23–0.58 (Q3) | 1.23 (0.80, 1.87) | 0.83 (0.60, 1.15) | 1.04 (0.75, 1.44) | 1.19 (0.77, 1.85) | 0.74 (0.53, 1.03) | 0.85 (0.60, 1.21) |
| >0.58 (Q4) | Reference | Reference | Reference | Reference | Reference | Reference |
| Not Controlled for Site | Controlled for Site | |||||
| % of MUFA Intake | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| <15% | 0.52 (0.38, 0.70) | 0.72 (0.57, 0.91) | 0.50 (0.39, 0.65) | 1.25 (0.86, 1.82) | 0.97 (0.72, 1.31) | 1.12 (0.81, 1.54) |
| 15% | Reference | Reference | Reference | Reference | Reference | Reference |
| Not Controlled for Site | Controlled for Site | |||||
| Quartile of %TEC MUFA Intake | 3/5 CM Risk Factors | Inflammation | Obesity | 3/5 CM Risk Factors | Inflammation | Obesity |
| 0.0–8.9 | 0.39 (0.26, 0.60) | 0.51 (0.36, 0.71) | 0.31 (0.21, 0.45) | 1.08 (0.64, 1.81) | 0.80 (0.54, 1.19) | 0.94 (0.61, 1.45) |
| 8.9–11.8 | 0.42 (0.28, 0.63) | 0.70 (0.51, 0.95) | 0.47 (0.34, 0.65) | 1.16 (0.72, 1.88) | 1.04 (0.72, 1.50) | 1.13 (0.76, 1.68) |
| 11.8–15.30 | 0.60 (0.42, 0.86) | 0.74 (0.55, 1.00) | 0.82 (0.61, 1.11) | 1.15 (0.77, 1.72) | 0.97 (0.70, 1.36) | 1.54 (1.08, 2.20) |
| >15.3 | Reference | Reference | Reference | Reference | Reference | Reference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehta, S.; Ruth Dugas, L.; Choo-Kang, C.; Bovet, P.; Forrester, T.; Bedu-Addo, K.; Lambert, E.V.; Plange-Rhule, J.; Riesen, W.; Korte, W.; et al. Consumption of Monounsaturated Fatty Acids Is Associated with Improved Cardiometabolic Outcomes in Four African-Origin Populations Spanning the Epidemiologic Transition. Nutrients 2021, 13, 2442. https://doi.org/10.3390/nu13072442
Mehta S, Ruth Dugas L, Choo-Kang C, Bovet P, Forrester T, Bedu-Addo K, Lambert EV, Plange-Rhule J, Riesen W, Korte W, et al. Consumption of Monounsaturated Fatty Acids Is Associated with Improved Cardiometabolic Outcomes in Four African-Origin Populations Spanning the Epidemiologic Transition. Nutrients. 2021; 13(7):2442. https://doi.org/10.3390/nu13072442
Chicago/Turabian StyleMehta, Supal, Lara Ruth Dugas, Candice Choo-Kang, Pascal Bovet, Terrence Forrester, Kweku Bedu-Addo, Estelle Vicki Lambert, Jacob Plange-Rhule, Walter Riesen, Wolfgang Korte, and et al. 2021. "Consumption of Monounsaturated Fatty Acids Is Associated with Improved Cardiometabolic Outcomes in Four African-Origin Populations Spanning the Epidemiologic Transition" Nutrients 13, no. 7: 2442. https://doi.org/10.3390/nu13072442
APA StyleMehta, S., Ruth Dugas, L., Choo-Kang, C., Bovet, P., Forrester, T., Bedu-Addo, K., Lambert, E. V., Plange-Rhule, J., Riesen, W., Korte, W., & Luke, A. (2021). Consumption of Monounsaturated Fatty Acids Is Associated with Improved Cardiometabolic Outcomes in Four African-Origin Populations Spanning the Epidemiologic Transition. Nutrients, 13(7), 2442. https://doi.org/10.3390/nu13072442