
Revisiting Konzo Risk Factors in Three Areas Differently Affected by Spastic Paraparesis in Eastern Democratic Republic of the Congo Discloses a Prominent Role of the Nutritional Status—A Comparative Cross-Sectional Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Areas
2.2. Study Design and Ethics
2.3. Participants
2.4. Data Collection
2.4.1. General Data and Anthropometric Measures
2.4.2. Cassava-Derived Cyanide Exposure
2.5. Data Processing and Analysis
2.5.1. Data Processing
2.5.2. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Nutritional Indices
3.3. Cyanide Exposure from Cassava Products
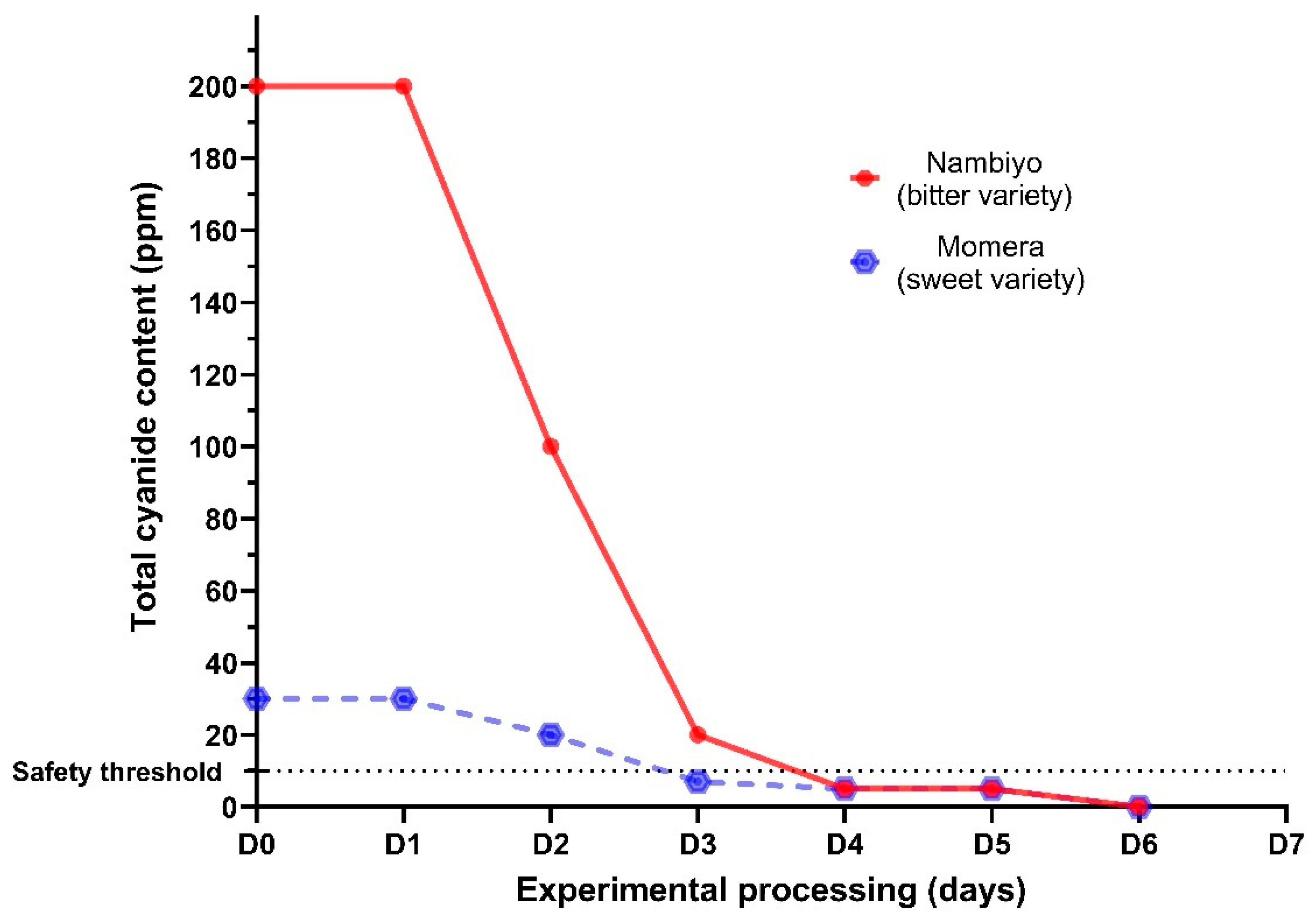
3.3.1. Cyanide Content of Cassava Roots and Flour
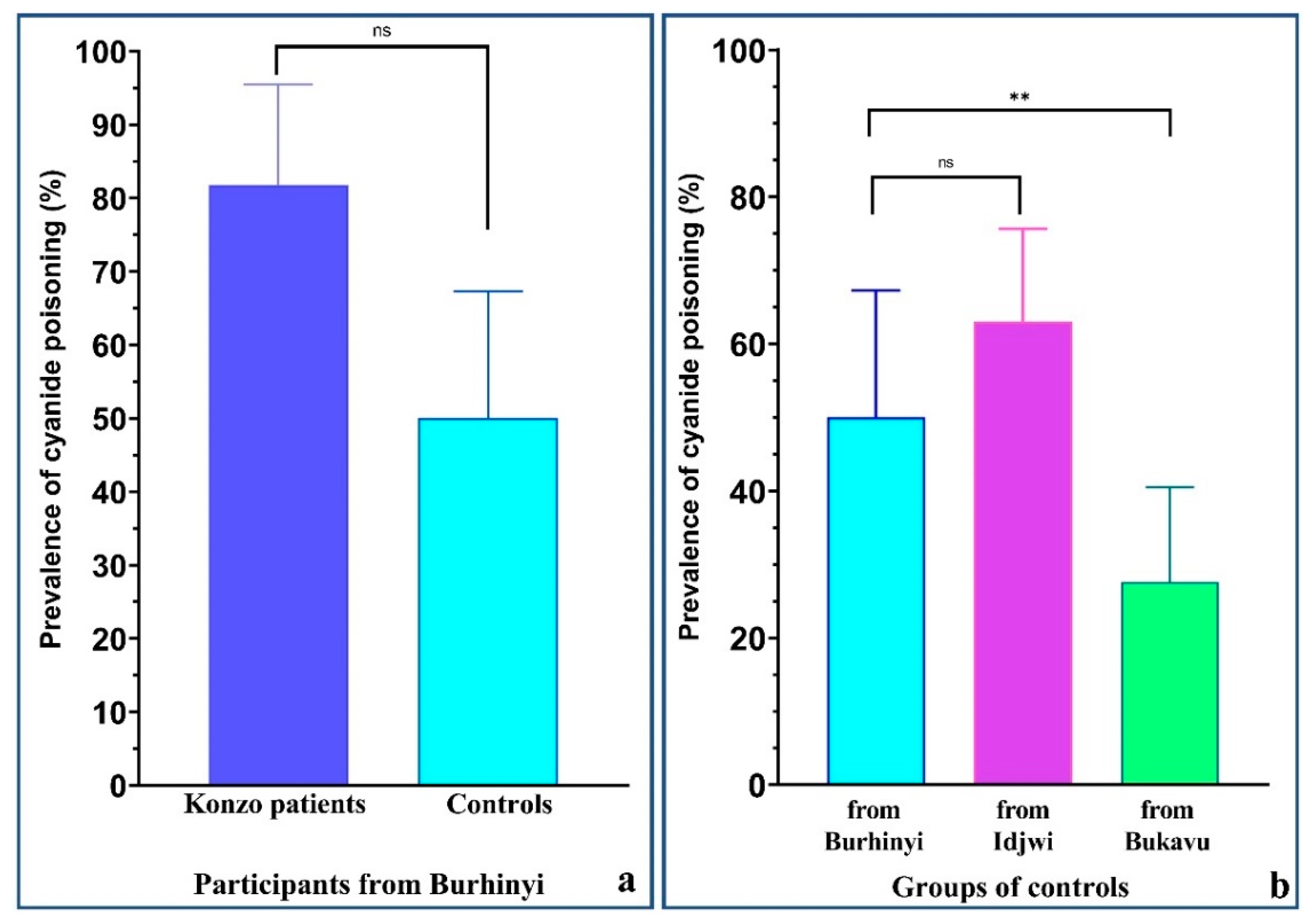
3.3.2. Urinary Thiocyanate Concentration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Konzo—A distinct type of upper motoneuron disease. Wkly. Epidemiol. Rec. 1996, 71, 225–228. [Google Scholar]
- Diasolua Ngudi, D.; Banea-Mayambu, J.P.; Lambein, F.; Kolsteren, P. Konzo and dietary pattern in cassava-consuming populations of Popokabaka, Democratic Republic of Congo. Food Chem. Toxicol. 2011, 49, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Nzwalo, H.; Cliff, J. Konzo: From poverty, cassava, and cyanogen intake to toxico-nutritional neurological disease. PLoS Negl. Trop. Dis. 2011, 5, e1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baguma, M.; Nzabara, F.; Balemba, G.M.; Malembaka, E.B.; Migabo, C.; Mudumbi, G.; Bito, V.; Cliff, J.; Rigo, J.-M.; Chabwine, J.N. Konzo risk factors, determinants and etiopathogenesis: What is new? A systematic review. Neurotoxicology 2021, 85, 54–67. [Google Scholar] [CrossRef]
- Oluwole, O.S.A. Cyclical konzo epidemics and climate variability. Ann. Neurol. 2015, 77, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Rosling, H.; Gessain, A.; de Thé, G.; Ebondo, N.; Banea, M.; Bikangi, N.; Kinjanja, K.; Nunga, K. Tropical and epidemic spastic paraparesis are different. Lancet 1988, 28, 1222–1223. [Google Scholar] [CrossRef]
- Boivin, M.J.; Okitundu, D.; Makila-Mabe Bumoko, G.; Sombo, M.-T.; Mumba, D.; Tylleskar, T.; Page, C.F.; Tamfum Muyembe, J.-J.; Tshala-Katumbay, D. Neuropsychological effects of konzo: A neuromotor disease associated with poorly processed cassava. Pediatrics 2013, 131, e1231–e1239. [Google Scholar] [CrossRef] [Green Version]
- Banea, J.P.; Bradbury, J.H.; Mandombi, C.; Nahimana, D.; Denton, I.C.; Foster, M.P.; Kuwa, N.; Tshala Katumbay, D. Konzo prevention in six villages in the DRC and the dependence of konzo prevalence on cyanide intake and malnutrition. Toxicol. Rep. 2015, 2, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Chabwine, J.; Masheka, C.; Balol’ebwami, Z.; Maheshe, B.; Balegamire, S.; Rutega, B.; Wa Lola, M.; Mutendela, K.; Bonnet, M.-J.; Shangalume, O.; et al. Appearance of konzo in South-Kivu, a wartorn area in the Democratic Republic of Congo. Food Chem. Toxicol. 2011, 49, 644–649. [Google Scholar] [CrossRef]
- Baguma, M.; Nzabara, F.; Bwenge, E.; Mudumbi, G.; Maheshe, G.; Cliff, J.; Rigo, J.M.; Chabwine, J.N. Seasonal variation but not processing methods differently affect cassava-derived cyanide exposure in two areas with different konzo prevalence in south-kivu (D.R. Congo). IBRO Rep. 2019, 7, 50. [Google Scholar] [CrossRef]
- Chuma, G.B.; Mondo, J.M.; Ndeko, A.B.; Mugumaarhahama, Y.; Bagula, E.M.; Blaise, M.; Valérie, M.; Jacques, K.; Karume, K.; Mushagalusa, G.N. Forest cover affects gully expansion at the tropical watershed scale: Case study of Luzinzi in Eastern DR Congo. Trees For. People 2021, 4, 100083. [Google Scholar] [CrossRef]
- Ivory, S.J.; McGlue, M.M.; Peterman, C.; Baldwin, P.; Lucas, J.; Cohen, A.; Russell, J.; Saroni, J.; Msaky, E.; Kimirei, I.; et al. Climate, vegetation, and weathering across space and time in Lake Tanganyika (tropical eastern Africa). Quat. Sci. Adv. 2021, 3, 100023. [Google Scholar] [CrossRef]
- Coghlan, B.; Brennan, R.J.; Ngoy, P.; Dofara, D.; Otto, B.; Clements, M.; Stewart, T. Mortality in the Democratic Republic of Congo: A nationwide survey. Lancet 2006, 367, 44–51. [Google Scholar] [CrossRef]
- Congo Research Group. Congo, Forgotten: The Numbers Behind Africa’s Longest Humanitarian Crisis. 2019. Available online: https://reliefweb.int/report/democratic-republic-congo/congo-forgotten-numbers-behind-africa-s-longest-humanitarian-crisis (accessed on 15 June 2021).
- Montagnac, J.A.; Davis, C.R.; Tanumihardjo, S.A. Nutritional value of cassava for use as a staple food and recent advances for improvement. Compr. Rev. Food Sci. Food Saf. 2009, 8, 181–194. [Google Scholar] [CrossRef]
- Kuvibidila, S.; Vuvu, M. Unusual low plasma levels of zinc in non-pregnant Congolese women. Br. J. Nutr. 2009, 101, 1783–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey-Leeson, S.; Karakochuk, C.D.; Hawes, M.; Tugirimana, P.L.; Bahizire, E.; Akilimali, P.Z.; Michaux, K.D.; Lynd, L.D.; Whitfield, K.C.; Moursi, M.; et al. Anemia and Micronutrient Status of Women of Childbearing Age and Children 6–59 Months in the Democratic Republic of the Congo. Nutrients 2016, 8, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ermans, A.M.; Delange, F.; Van der Velden, M.; Kinthaert, J. Goitrogenic action of cyanogenic glucosides present in cassava: A possible etiologic factor of endemic goiter in the Idjwi island. Acta Endocrinol. Suppl. 1973, 179, 31. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- WHO Growth Reference Data for 5–19 Years (WHO 2007). Available online: https://www.who.int/growthref/en/%0Ahttp://www.who.int/growthref/en/%0Awww.who.int/growthref/en/1/2%0Ahttp://www.who.int/growthref/en (accessed on 15 January 2019).
- Bradbury, M.G.; Egan, S.V.; Bradbury, J.H. Picrate paper kits for determination of total cyanogens in cassava roots and all forms of cyanogens in cassava products. J. Sci. Food Agric. 1999, 79, 593–601. [Google Scholar] [CrossRef]
- Haque, M.R.; Bradbury, J.H. Simple method for determination of thiocyanate in urine. Clin. Chem. 1999, 45, 1459–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UCL–LTAP Thiocyanates: Urine. Available online: https://www.toxi.ucl.ac.be/documents/thiocyanate_u.htm (accessed on 29 September 2018).
- Ministry of Health Mozambique. Mantakassa: An epidemic of spastic paraparesis associated with chronic cyanide intoxication in a cassava staple area of Mozambique. 1. Epidemiology and clinical and laboratory findings in patients. Bull. World Health Organ. 1984, 62, 477–484. [Google Scholar]
- Cliff, J.; Lundqvist, P.; Martensson, J.; Rosling, H.; Sorbo, B. Association of high cyanide and low sulphur intake in cassava-induced spastic paraparesis. Lancet 1985, 2, 1211–1213. [Google Scholar] [CrossRef]
- Tylleskär, T.; Rosling, H.; Banea, M.; Bikangi, N.; Cooke, R.D.; Poulter, N.H. Cassava cyanogens and konzo, an upper motoneuron disease found in Africa. Lancet 1992, 339, 208–211. [Google Scholar] [CrossRef]
- Bumoko, G.M.M.; Sadiki, N.H.; Rwatambuga, A.; Kayembe, K.P.; Okitundu, D.L.; Mumba Ngoyi, D.; Muyembe, J.T.J.T.; Banea, J.P.; Boivin, M.J.; Tshala-katumbay, D.; et al. Lower serum levels of selenium, copper, and zinc are related to neuromotor impairments in children with konzo. J. Neurol. Sci. 2015, 349, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Banea, J.P.; Tylleskar, T.; Gitebo, N.; Matadi, N.; Gebre-Medhin, M.; Rosling, H. Geographical and seasonal association between linamarin and cyanide exposure from cassava and the upper motor neurone disease konzo in former Zaire. Trop. Med. Int. Health 1997, 2, 1143–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashala-Abotnes, E.; Okitundu, D.; Mumba, D.; Boivin, M.J.; Tylleskär, T.; Tshala-Katumbay, D. Konzo: A distinct neurological disease associated with food (cassava) cyanogenic poisoning. Brain Res. Bull. 2019, 145. [Google Scholar] [CrossRef] [PubMed]
- Tor-Agbidye, J.; Palmer, V.S.; Sabri, M.I.; Craig, A.M.; Blythe, L.L.; Spencer, P.S. Dietary deficiency of cystine and methionine in rats alters thiol homeostasis required for cyanide detoxification. J. Toxicol. Environ. Health Part A 1998, 55, 583–595. [Google Scholar] [CrossRef]
- Oluwole, O.S.A.; Oludiran, A. Normative concentrations of urine thiocyanate in cassava eating communities in Nigeria. Int. J. Food Sci. Nutr. 2013, 64, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Ngudi, D.D.; Kuo, Y.H.; Lambein, F. Food safety and amino acid balance in processed cassava “Cossettes”. J. Agric. Food Chem. 2002, 50, 3042–3049. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Konzo Patients n (%) | Controls from Burhinyi n (%) | p 1 |
|---|---|---|---|
| overall malnutrition (either wasting or stunting) | |||
| Yes | 9 (81.8) | 9 (30.0) | 0.0046 |
| No | 2 (18.2) | 21 (70.0) | |
| acute malnutrition (wasting) | |||
| Yes | 6 (54.5) | 1 (3.3) | 0.0006 |
| No | 5 (45.5) | 29 (96.7) | |
| chronic malnutrition (stunting) | |||
| Yes | 8 (72.7) | 8 (26.7) | 0.0119 |
| No | 3 (27.3) | 22 (73.3) | |
| Variables | Controls from Burhinyi n (%) | Controls from Idjwi n (%) | Controls from Bukavu n (%) | p |
|---|---|---|---|---|
| overall malnutrition (either wasting or stunting) | ||||
| Yes | 9 (30.0) | 12 (26.1) | 10 (17.2) | 0.341 1 |
| No | 21 (70.0) | 34 (73.9) | 48 (82.8) | |
| acute malnutrition (wasting) | ||||
| Yes | 1 (3.3) | 3 (6.5) | 4 (6.9) | 0.902 2 |
| No | 29 (96.7) | 43 (93.5) | 54 (93.1) | |
| chronic malnutrition (stunting) | ||||
| Yes | 8 (26.7) | 11 (23.9) | 7 (12.1) | 0.165 1 |
| No | 22 (73.3) | 35 (76.1) | 51 (87.9) | |
| Locations | Health Status | Prevalence of Risk Factors | ||
|---|---|---|---|---|
| Malnutrition | Cyanide Poisoning | |||
| Wasting | Stunting | |||
| Burhinyi | Konzo patients | High | High | High |
| Controls | Low | Intermediate | High | |
| Idjwi | Controls | Low | Intermediate | High |
| Bukavu | Controls | Low | Low | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baguma, M.; Malembaka, E.B.; Bahizire, E.; Mudumbi, G.Z.; Shamamba, D.B.; Matabaro, A.-N.; Rigo, J.-M.; Njamnshi, A.K.; Chabwine, J.N. Revisiting Konzo Risk Factors in Three Areas Differently Affected by Spastic Paraparesis in Eastern Democratic Republic of the Congo Discloses a Prominent Role of the Nutritional Status—A Comparative Cross-Sectional Study. Nutrients 2021, 13, 2628. https://doi.org/10.3390/nu13082628
Baguma M, Malembaka EB, Bahizire E, Mudumbi GZ, Shamamba DB, Matabaro A-N, Rigo J-M, Njamnshi AK, Chabwine JN. Revisiting Konzo Risk Factors in Three Areas Differently Affected by Spastic Paraparesis in Eastern Democratic Republic of the Congo Discloses a Prominent Role of the Nutritional Status—A Comparative Cross-Sectional Study. Nutrients. 2021; 13(8):2628. https://doi.org/10.3390/nu13082628
Chicago/Turabian StyleBaguma, Marius, Espoir Bwenge Malembaka, Esto Bahizire, Germain Zabaday Mudumbi, Dieudonné Bahati Shamamba, Alain-Narcisse Matabaro, Jean-Michel Rigo, Alfred Kongnyu Njamnshi, and Joelle Nsimire Chabwine. 2021. "Revisiting Konzo Risk Factors in Three Areas Differently Affected by Spastic Paraparesis in Eastern Democratic Republic of the Congo Discloses a Prominent Role of the Nutritional Status—A Comparative Cross-Sectional Study" Nutrients 13, no. 8: 2628. https://doi.org/10.3390/nu13082628
APA StyleBaguma, M., Malembaka, E. B., Bahizire, E., Mudumbi, G. Z., Shamamba, D. B., Matabaro, A. -N., Rigo, J. -M., Njamnshi, A. K., & Chabwine, J. N. (2021). Revisiting Konzo Risk Factors in Three Areas Differently Affected by Spastic Paraparesis in Eastern Democratic Republic of the Congo Discloses a Prominent Role of the Nutritional Status—A Comparative Cross-Sectional Study. Nutrients, 13(8), 2628. https://doi.org/10.3390/nu13082628