
Benefits of Adding an Aquatic Resistance Interval Training to a Nutritional Education on Body Composition, Body Image Perception and Adherence to the Mediterranean Diet in Older Women

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
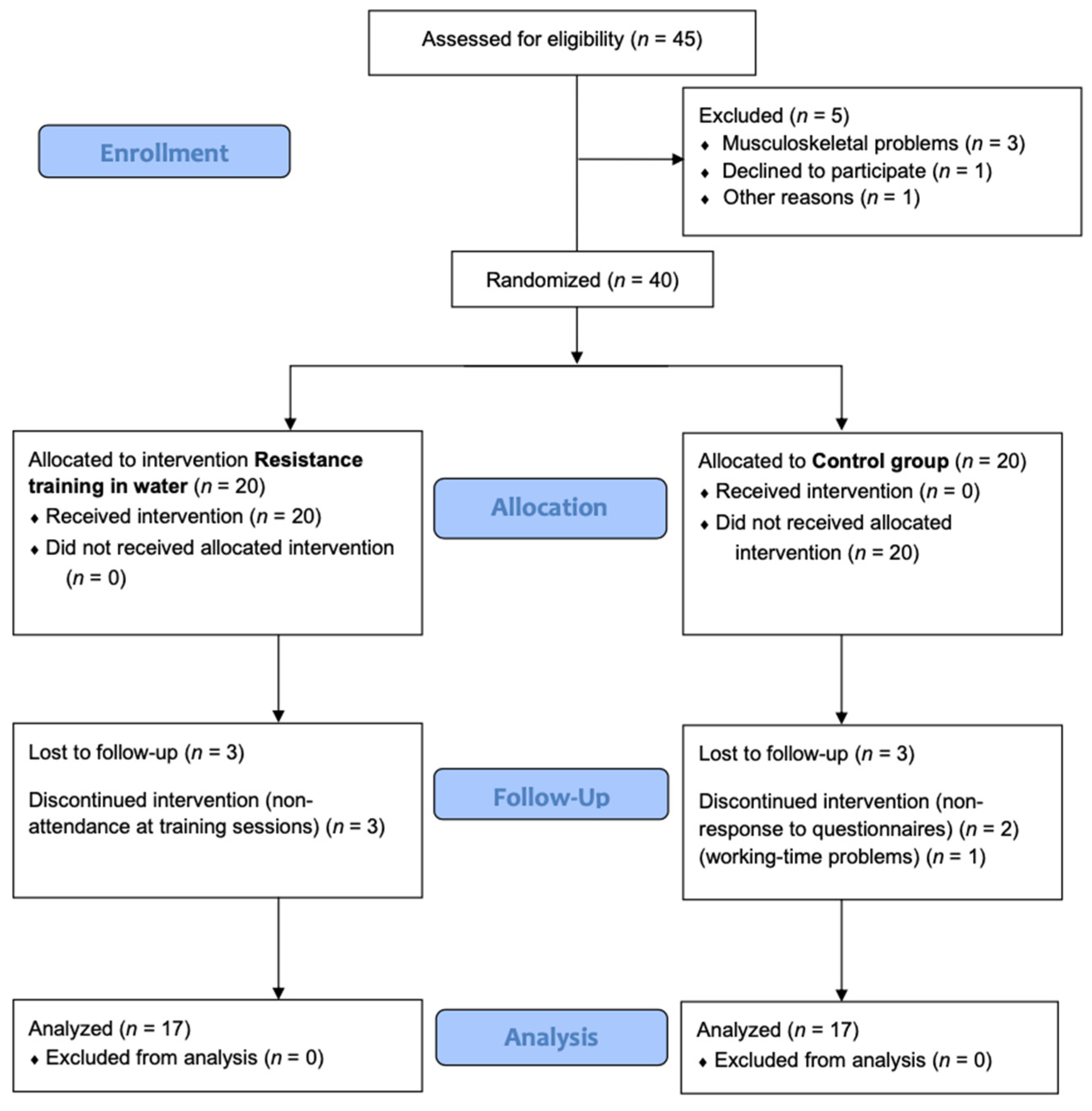
2.1. Study Design
2.2. Participants
2.3. Declarations: Ethical Approval, Consent to Participate and Consent for Publication
2.4. Study Intervention
2.4.1. Aquatic Resistance Interval Training
2.4.2. Nutritional Education
2.5. Outcome Measurements
2.5.1. Body Composition
2.5.2. Body Image
2.5.3. Mediterranean Diet
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buch, A.; Kis, O.; Carmeli, E.; Keinan-Boker, L.; Berner, Y.; Barer, Y.; Shefer, G.; Marcus, Y.; Stern, N. Circuit resistance training is an effective means to enhance muscle strength in older and middle aged adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 37, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Marín-Cascales, E.; Alcaraz, P.E.; Ramos-Campo, D.J.; Rubio-Arias, J.A. Effects of multicomponent training on lean and bone mass in postmenopausal and older women: A systematic review. Menopause 2018, 25, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Colpani, V.; Baena, C.P.; Jaspers, L.; van Dijk, G.M.; Farajzadegan, Z.; Dhana, K.; Tielemans, M.J.; Voortman, T.; Freak-Poli, R.; Veloso, G.G.V.; et al. Lifestyle factors, cardiovascular disease and all-cause mortality in middle-aged and elderly women: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 831–845. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzmán, G. Estrogen deficiency and the origin of obesity during menopause. BioMed Res. Int. 2014, 2014, 757461. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.C.; Wu, S.; Chan, S.G.; Sham, A. Menopausal transition and changes of body composition: A prospective study in Chinese perimenopausal women. Int. J. Obes. 2010, 34, 1265–1274. [Google Scholar] [CrossRef] [Green Version]
- Thompson, K.A.; Bardone-Cone, A.M. Menopausal status and disordered eating and body image concerns among middle-aged women. Int. J. Eat. Disord. 2019, 52, 314–318. [Google Scholar] [CrossRef]
- Simas, V.; Hing, W.; Pope, R.; Climstein, M. Effects of water-based exercise on bone health of middle-aged and older adults: A systematic review and meta-analysis. Open Access J. Sport. Med. 2017, 8, 39–60. [Google Scholar] [CrossRef] [Green Version]
- Perich, T.; Ussher, J.; Meade, T. Menopause and illness course in bipolar disorder: A systematic review. Bipolar Disord. 2017, 19, 434–443. [Google Scholar] [CrossRef]
- Bromberger, J.T.; Epperson, C.N. Depression during and after the perimenopause: Impact of hormones, genetics, and environmental determinants of disease. Obstet. Gynecol. Clin. N. Am. 2018, 45, 663–678. [Google Scholar] [CrossRef]
- Gibbs, Z.; Lee, S.; Kulkarni, J. What factors determine whether a woman becomes depressed during the perimenopause? Arch. Women’s Ment. Health 2012, 15, 323–332. [Google Scholar] [CrossRef]
- Drobnjak, S.; Atsiz, S.; Ditzen, B.; Tuschen-Caffier, B.; Ehlert, U. Restrained eating and self-esteem in premenopausal and postmenopausal women. J. Eat. Disord. 2014, 2, 23. [Google Scholar] [CrossRef]
- Sayón-Orea, C.; Santiago, S.; Cuervo, M.; Martínez-González, M.A.; Garcia, A.; Martínez, J.A. Adherence to Mediterranean dietary pattern and menopausal symptoms in relation to overweight/obesity in Spanish perimenopausal and postmenopausal women. Menopause 2015, 22, 750–757. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; D’Addato, S.; Santi, F.; Ferroni, A.; Borghi, C. Leisure-time physical activity and cardiovascular disease mortality: The brisighella heart study. J. Cardiovasc. Med. 2012, 13, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.J.; Stevinson, C.; Ku, P.W.; Chang, Y.K.; Chu, D.C. Relationships of leisure-time and non-leisure-time physical activity with depressive symptoms: A population-based study of Taiwanese older adults. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- Petersen, C.B.; Severin, M.; Hansen, A.W.; Curtis, T.; Grønbæk, M.; Tolstrup, J.S. A population-based randomized controlled trial of the effect of combining a pedometer with an intervention toolkit on physical activity among individuals with low levels of physical activity or fitness. Prev. Med. 2012, 54, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Nawrocka, A.; Mynarski, W.; Cholewa, J. Adherence to physical activity guidelines and functional fitness of elderly women, using objective measurement. Ann. Agric. Environ. Med. 2017, 24, 632–635. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American college of sports medicine position stand. exercise and physical activity for older adults. Med. Sci. Sports Exerc. 1998, 41, 992–1008. [Google Scholar]
- Pollock, M.L.; Wenger, N.K. Physical activity and exercise training in the elderly: A position paper from the society of geriatric cardiology. Am. J. Geriatr. Cardiol. 1998, 7, 45–46. [Google Scholar] [PubMed]
- Saghaei, M. An overview of randomization and minimization programs for randomized clinical trials. J. Med. Signals Sens. 2011, 1, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Gunnarsson, T.P.; Bangsbo, J. The 10-20-30 training concept improves performance and health profile in moderately trained runners. J. Appl. Physiol. 2012, 113, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Andrade, L.S.; Kanitz, A.C.; Häfele, M.S.; Schaun, G.Z.; Pinto, S.S.; Alberton, C.L. Relationship between oxygen uptake, heart rate, and perceived effort in an aquatic incremental test in older women. Int. J. Environ. Res. Public Health 2020, 17, 8324. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work. Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef]
- Norton, K.I. Standards for Anthropometry Assessment. In Kinanthropometry and Exercise Physiology; Routledge: London, UK, 2019; pp. 68–137. [Google Scholar]
- Ross, W.D.; Kerr, D.A. Fraccionamiento de la Masa Corporal: Un Nuevo Método para Utilizar en Nutrición, Clínica y Medicina Deportiva. Revista de Actualización en Ciencias del Deporte. 1993, 3, 1. [Google Scholar]
- Carter, J.E.L. The Heath-Carter Anthropometric Somatotype-Instruction Manual-Somatotype Instruction Manual 2 Part 1: The Heath-Carter Anthropometric Somatotype-Instruction Manual; TeP and ROSSCRAFT: Surrey, BC, Canada, 2002. [Google Scholar]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Christopher, G.; Fairbum, M.D. The development and validation of the body shape questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item mediterranean diet assessment tool and obesity indexes among high-risk subjects: The predimed trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [Green Version]
- Gignac, G.E.; Szodorai, E.T. Effect size guidelines for individual differences researchers. Pers. Individ. Differ. 2016, 102, 74–78. [Google Scholar] [CrossRef]
- Vaquero-Cristóbal, R.; Alacid, F.; Esparza-Ros, F.; López-Plaza, D.; Muyor, J.M.; López-Miñarro, P.A. The effects of a reformer Pilates program on body composition and morphological characteristics in active women after a detraining period. Women Health 2016, 56, 784–806. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.L.; Weeks, B.K.; Weis, L.J.; Harding, A.T.; Horan, S.A.; Beck, B.R. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: The liftmor randomized controlled trial. J. Bone Miner. Res. 2018, 33, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Villareal, D.T.; Aguirre, L.; Gurney, A.B. Aerobic or resistance exercise, or both, in dieting obese older adults. N. Engl. J. Med. 2017, 376, 1943–1955. [Google Scholar] [CrossRef] [Green Version]
- Correa-de-Araujo, R.; Hadley, E. Skeletal muscle function deficit: A new terminology to embrace the evolving concepts of sarcopenia and age-related muscle dysfunction. J. Gerontol. A. Biol. Sci. Med. Sci. 2014, 69, 591–594. [Google Scholar] [CrossRef] [Green Version]
- Baasch-Skytte, T.; Lemgart, C.T.; Oehlenschläger, M.H.; Petersen, P.E.; Hostrup, M.; Bangsbo, J.; Gunnarsson, T.P. Efficacy of 10-20-30 training versus moderate-intensity continuous training on HbA1c, body composition and maximum oxygen uptake in male patients with type 2 diabetes: A randomized controlled trial. Diabetes Obes. Metab. 2020, 22, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Boukabous, I.; Marcotte-Chénard, A.; Amamou, T.; Boulay, P.; Brochu, M.; Tessier, D.; Dionne, I.; Riesco, E. Low-volume high-intensity interval training versus moderate-intensity continuous training on body composition, cardiometabolic profile, and physical capacity in older women. J. Aging Phys. Act. 2019, 27, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Tong, T.K.; Qiu, W.; Zhang, X.; Zhou, S.; Liu, Y.; He, Y. Comparable effects of high-intensity interval training and prolonged continuous exercise training on abdominal visceral fat reduction in obese young women. J. Diabetes Res. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Keating, S.E.; Johnson, N.A.; Mielke, G.I.; Coombes, J.S. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes. Rev. 2017, 18, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, C.G.; Seo, T.B.; Kim, H.G.; Yoon, S.J. Effects of 8-week combined training on body composition, isokinetic strength, and cardiovascular disease risk factors in older women. Aging Clin. Exp. Res. 2015, 27, 179–186. [Google Scholar] [CrossRef]
- Perry, C.A.; Van Guilder, G.P.; Kauffman, A.; Hossain, M. A calorie-restricted DASH diet reduces body fat and maintains muscle strength in obese older adults. Nutrients 2020, 12, 102. [Google Scholar] [CrossRef] [Green Version]
- Boldsen, J.L.; Carter, J.E.L.; Honeyman, B. Lindsay carter, barbara honeyman heath. In Somatotyping: Development and Applications; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Li, S.; Xue, J.; Hong, P. Relationships between serum omentin-1 concentration, body composition and physical activity levels in older women. Medicine 2021, 100, e25020. [Google Scholar] [CrossRef] [PubMed]
- Cobo, C.M.S. Body image in older. Descriptive studie. Gerokomos 2012, 23, 15–18. [Google Scholar]
- Allaz, A.F.; Bernstein, M.; Rouget, P.; Archinard, M.; Morabia, A. Body weight preoccupation in middle-age and ageing women: A general population survey. Int. J. Eat. Disord. 1998, 23, 287–294. [Google Scholar] [CrossRef]
- Webster, J.; Tiggemann, M. The relationship between women’s body satisfaction and self-image across the life span: The role of cognitive control. J. Genet. Psychol. 2003, 164, 241–252. [Google Scholar] [CrossRef]
- Bouzas, C.; Bibiloni, M.D.M.; Tur, J.A. Relationship between body image and body weight control in overweight ≥55-year-old adults: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1622. [Google Scholar] [CrossRef] [Green Version]
- Fougner, M.; Bergland, A.; Lund, A.; Debesay, J. Aging and exercise: Perceptions of the active lived-body. Physiother. Theory Pract. 2019, 35, 651–662. [Google Scholar] [CrossRef]
- Dean, E.; Haywood, C.; Hunter, P.; Austin, N.; Prendergast, L. Body image in older, inpatient women and the relationship to BMI, anxiety, depression, and other sociodemographic factors. Int. J. Geriatr. Psychiatry 2020, 35, 182–187. [Google Scholar] [CrossRef]
- Latorre Román, P.A.; García-Pinillos, F.; Huertas Herrador, J.A.; Cózar Barba, M.; Muñoz Jiménez, M. Relacion entre sexo, Composicion corporal, Velocidad de la marcha y satisfaccion corporal en ancianos. Nutr. Hosp. 2014, 30, 851–857. [Google Scholar]
- Pedersen, M.T.; Vorup, J.; Nistrup, A.; Wikman, J.M.; Alstrøm, J.M.; Melcher, P.S.; Pfister, G.U.; Bangsbo, J. Effect of team sports and resistance training on physical function, quality of life, and motivation in older adults. Scand. J. Med. Sci. Sport. 2017, 27, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Tramontano, G.; De Luca, V.; Illario, M.; Colao, A.; Savastano, S. Association between Mediterranean diet and hand grip strength in older adult women. Clin. Nutr. 2019, 38, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Cano-Ibáñez, N.; Gea, A.; Martínez-González, M.A.; Salas-Salvadó, J.; Corella, D.; Zomeño, M.D.; Romaguera, D.; Vioque, J.; Aros, F.; Wärnberg, J.; et al. Dietary diversity and nutritional adequacy among an older Spanish population with metabolic syndrome in the predimed-plus study: A cross-sectional analysis. Nutrients 2019, 11, 958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martí, A.Z.; Martínez, M.J.C.; Sánchez, J.A.H.; Pérez, A.L. Adherencia a la dieta mediterránea y su relación con el estado nutricional en personas mayores. Nutr. Hosp. 2015, 31, 1667–1674. [Google Scholar]


{kind=link}
| Variables | Intervention Group (n = 17) | Control Group (n = 17) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Baseline | Baseline Differences | |||||||
| Mean | SD | Mean | SD | t | p | ES | |||
| Age (Years) | 69.6 | ± | 5.0 | 67.7 | ± | 3.6 | 1.257 | 0.218 | 0.431 |
| Height (cm) | 162.0 | ± | 7.9 | 154.0 | ± | 5.4 | 3.347 | 0.002 | 1.148 |
| Weight (kg) | 75.3 | ± | 12.8 | 66.9 | ± | 10.2 | 2.122 | 0.042 | 0.728 |
| BMI (kg/m2) | 28.8 | ± | 4.7 | 28.2 | ± | 4.2 | 0.385 | 0.703 | 0.132 |
| Variables | Intervention Group (n = 17) | Control Group (n = 17) | Effect Time | Effect Time × Group | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | ||||||||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |||||
| Body Composition | ||||||||||||||||||
| Weight (kg) | 75.3 | ± | 12.8 | 75.3 | ± | 13.2 | 66.9 | ± | 10.2 | 67.4 | ± | 10.3 | 1.065 | 0.310 | 0.033 | 0.329 | 0.570 | 0.011 |
| % fat mass | 32.3 | ± | 4.5 * | 29.5 | ± | 3.9 * | 34.2 | ± | 4.1 * | 36.5 | ± | 3.9 * | 0.205 | 0.654 | 0.007 | 58.649 | <0.001 | 0.654 |
| % residual mass | 11.8 | ± | 2.5 | 12.1 | ± | 2.4 | 10.6 | ± | 1.4 | 10.3 | ± | 1.2 | 0.319 | 0.577 | 0.010 | 0.434 | 0.515 | 0.014 |
| % muscle mass | 40.5 | ± | 3.4 * | 43.0 | ± | 2.4 * | 41.6 | ± | 2.8 * | 39.6 | ± | 2.7 * | 1.160 | 0.291 | 0.036 | 50.09 | <0.001 | 0.618 |
| % bone mass | 10.2 | ± | 1.5 | 10.2 | ± | 1.5 | 8.5 | ± | 0.9 | 8.5 | ± | 0.9 | 2.164 | 0.151 | 0.065 | 0.194 | 0.662 | 0.006 |
| % skin | 5.1 | ± | 0.7 # | 5.15 | ± | 0.8 # | 5.0 | ± | 0.4 # | 5.1 | ± | 0.5 # | 4.526 | 0.041 | 0.127 | 3.827 | 0.060 | 0.110 |
| kg fat mass | 24.5 | ± | 6.2 * | 22.4 | ± | 5.3 * | 22.9 | ± | 4.3 * | 24.7 | ± | 4.7 * | 1.110 | 0.300 | 0.035 | 59.27 | <0.001 | 0.657 |
| kg muscle mass | 30.5 | ± | 5.6 * | 32.5 | ± | 6.1 * | 27.8 | ± | 4.7 | 26.6 | ± | 4.5 | 0.140 | 0.710 | 0.005 | 22.118 | <0.001 | 0.416 |
| kg residual mass | 8.9 | ± | 2.3 | 9.1 | ± | 2.1 | 7.2 | ± | 1.8 | 6.9 | ± | 1.6 | 1.330 | 0.258 | 0.041 | 2.56 | 0.120 | 0.076 |
| kg bone mass | 7.6 | ± | 1.2 | 7.7 | ± | 1.2 | 5.7 | ± | 0.9 | 5.7 | ± | 0.9 | 3.218 | 0.083 | 0.094 | 0.441 | 0.511 | 0.014 |
| kg skin | 3.8 | ± | 0.6 | 3.8 | ± | 0.6 | 3.3 | ± | 0.3 | 3.4 | ± | 0.3 | 4.120 | 0.051 | 0.117 | 0.202 | 0.656 | 0.006 |
| WHR | 0.9 | ± | 0.1 | 0.9 | ± | 0.1 | 0.9 | ± | 0.1 | 0.9 | ± | 0.1 | 0.297 | 0.590 | 0.009 | 4.377 | 0.055 | 0.124 |
| Endomorph | 5.79 | ± | 1.72 * | 5.45 | ± | 1.67 * | 6.57 | ± | 1.22 | 6.90 | ± | 1.50 | 0.000815 | 0.977 | 0.000 | 15.0 | <0.001 | 0.011 |
| Mesomorph | 4.87 | ± | 1.26 * | 5.41 | ± | 1.41 * | 5.28 | ± | 1.56 * | 5.03 | ± | 1.40 * | 5.65 | 0.023 | 0.003 | 43.01 | <0.001 | 0.021 |
| Ectomorph | 0.59 | ± | 0.69 | 0.56 | ± | 0.60 | 0.46 | ± | 0.47 | 0.45 | ± | 0.47 | 0.580 | 0.451 | 0.017 | 0.183 | 0.672 | 0.005 |
| Body Image | ||||||||||||||||||
| BSQ | 52.4 | ± | 17.1 | 45.9 | ± | 12.7 | 57.4 | ± | 20.4 | 53.6 | ± | 20.9 | 2.050 | 0.162 | 0.062 | 0.482 | 0.493 | 0.015 |
| Mediterranean Diet | ||||||||||||||||||
| Predimed | 5.7 | ± | 2.0 | 5.9 | ± | 2.36 | 6.1 | ± | 2.1 | 5.5 | ± | 2.3 | 0.198 | 0.659 | 0.006 | 3.128 | 0.087 | 0.092 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rodríguez, A.; Cuestas-Calero, B.J.; Martínez-Olcina, M.; Marcos-Pardo, P.J. Benefits of Adding an Aquatic Resistance Interval Training to a Nutritional Education on Body Composition, Body Image Perception and Adherence to the Mediterranean Diet in Older Women. Nutrients 2021, 13, 2712. https://doi.org/10.3390/nu13082712
Martínez-Rodríguez A, Cuestas-Calero BJ, Martínez-Olcina M, Marcos-Pardo PJ. Benefits of Adding an Aquatic Resistance Interval Training to a Nutritional Education on Body Composition, Body Image Perception and Adherence to the Mediterranean Diet in Older Women. Nutrients. 2021; 13(8):2712. https://doi.org/10.3390/nu13082712
Chicago/Turabian StyleMartínez-Rodríguez, Alejandro, Bernardo J. Cuestas-Calero, María Martínez-Olcina, and Pablo Jorge Marcos-Pardo. 2021. "Benefits of Adding an Aquatic Resistance Interval Training to a Nutritional Education on Body Composition, Body Image Perception and Adherence to the Mediterranean Diet in Older Women" Nutrients 13, no. 8: 2712. https://doi.org/10.3390/nu13082712
APA StyleMartínez-Rodríguez, A., Cuestas-Calero, B. J., Martínez-Olcina, M., & Marcos-Pardo, P. J. (2021). Benefits of Adding an Aquatic Resistance Interval Training to a Nutritional Education on Body Composition, Body Image Perception and Adherence to the Mediterranean Diet in Older Women. Nutrients, 13(8), 2712. https://doi.org/10.3390/nu13082712