
Association between Dietary Intake of Flavonoids and Cancer Recurrence among Breast Cancer Survivors


Abstract
:1. Introduction
2. Materials and Methods
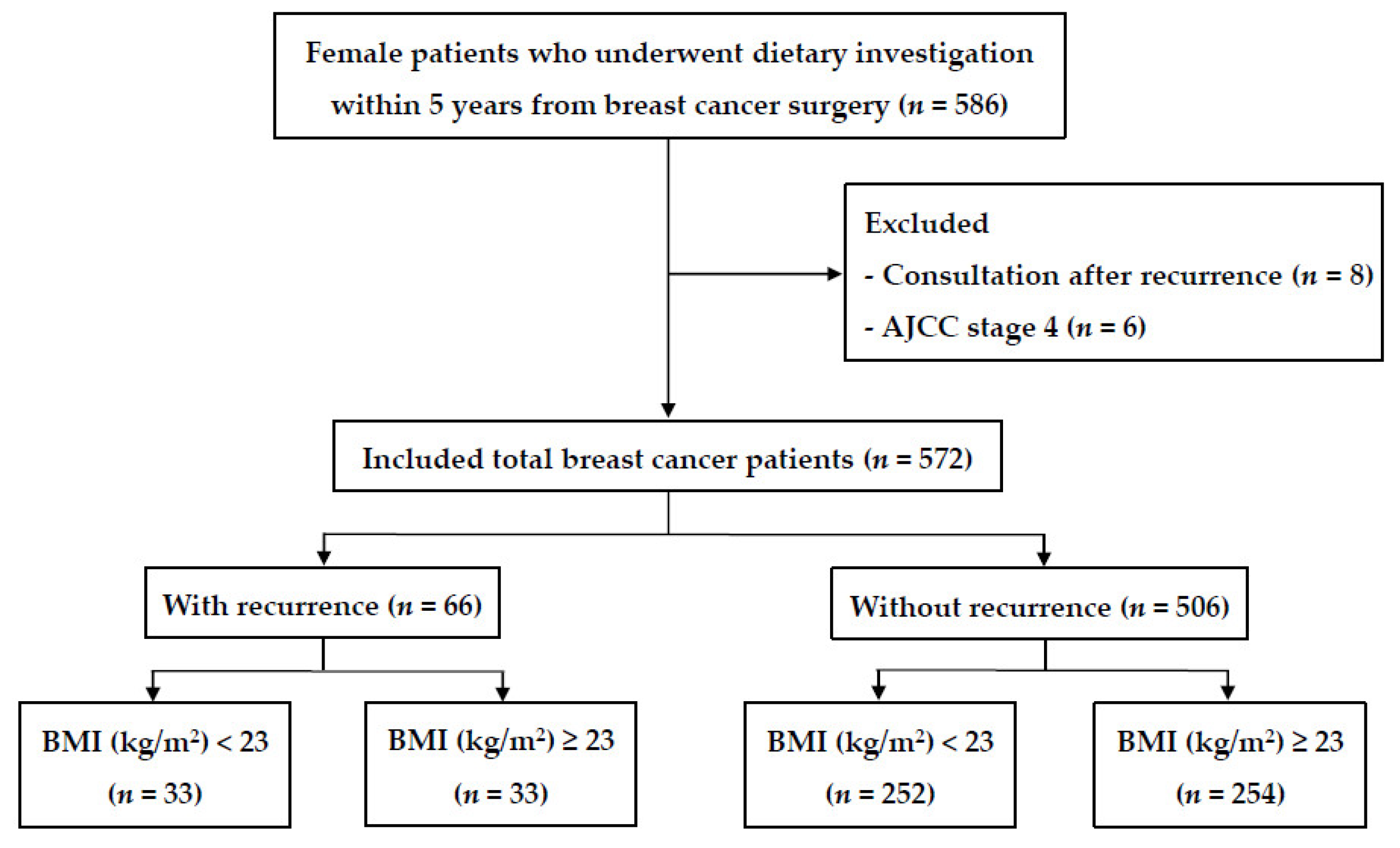
2.1. Patients
2.2. Data Collection
2.3. Intake of Dietary Flavonoids
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Patients with Breast Cancer
3.2. Association between Intake of Flavonoids/Flavonoid-Rich Foods and Cancer Recurrence
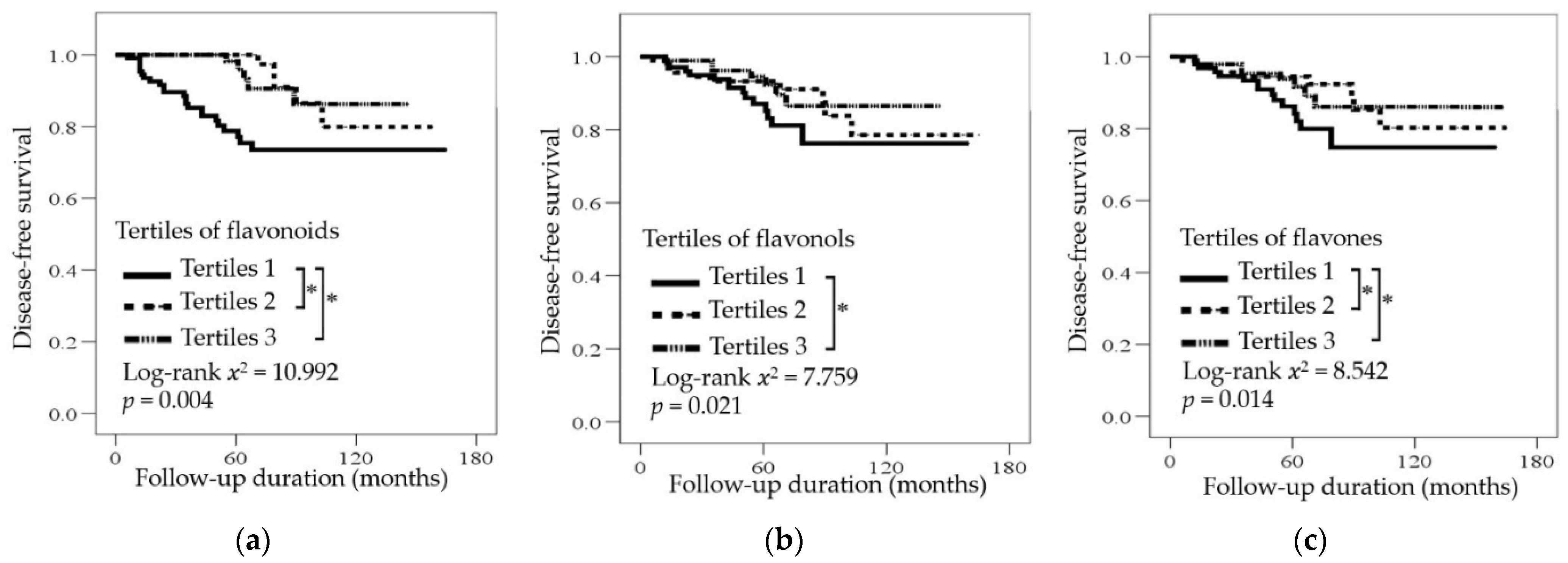
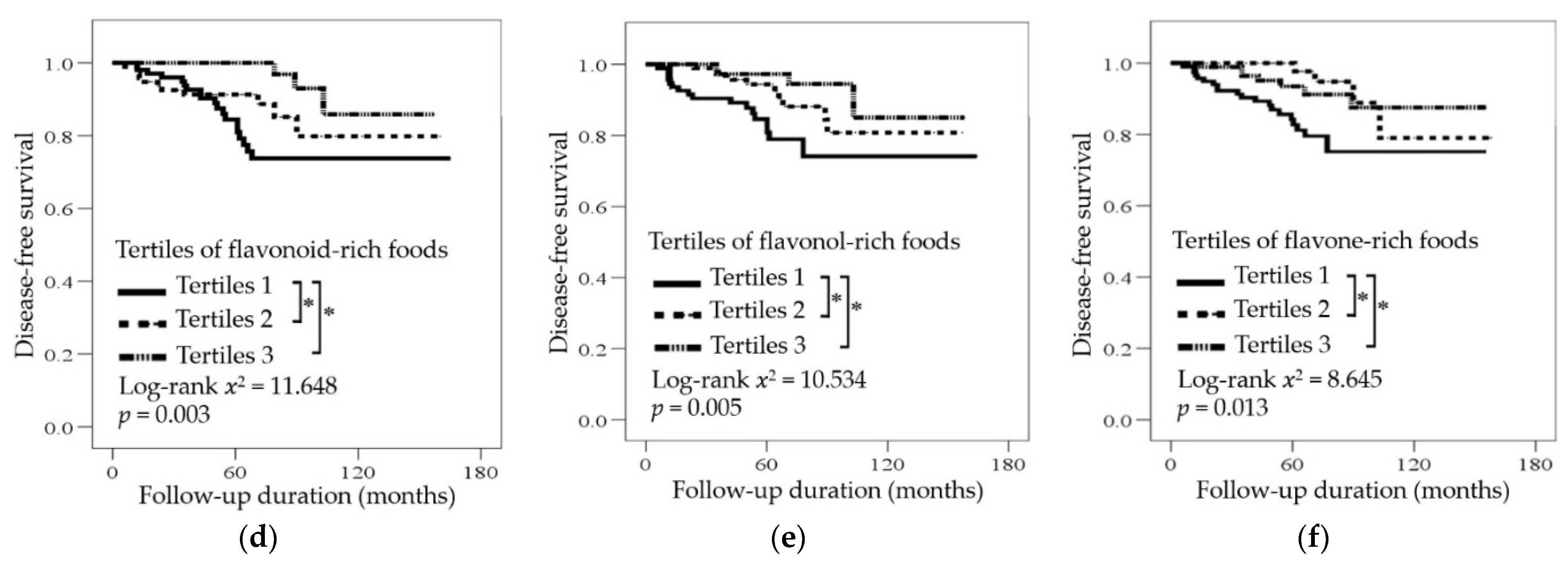
3.3. Association between Intake of Flavonoids/Flavonoid-Rich Foods and Disease-Free Survival
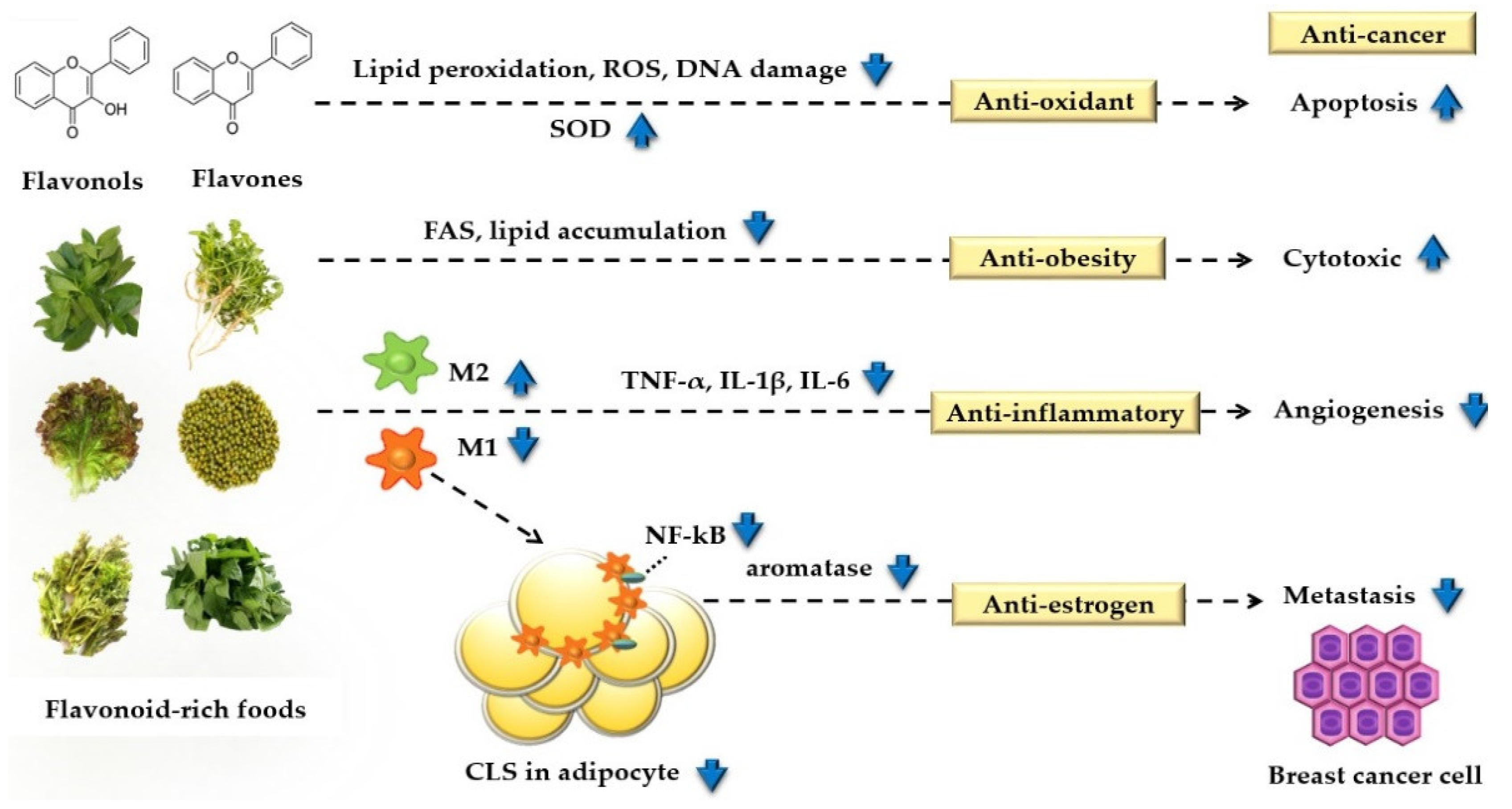
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Report on Cancer: Setting Priorities, Investing Wisely and Providing Care for All; World Health Organization: Geneva, Switzerland, 2020; Available online: http://apps.who.int/iris/handle/10665/330745 (accessed on 27 March 2020).
- Hamer, J.; Warner, E. Lifestyle modifications for patients with breast cancer to improve prognosis and optimize overall health. CMAJ 2017, 189, E268–e274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, H.; Chung, M.S.; Kang, S.S.; Park, Y. Association between the dietary inflammatory index and risk for cancer recurrence and mortality among patients with breast cancer. Nutrients 2018, 10, 1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandini, S.; Merzenich, H.; Robertson, C.; Boyle, P. Meta-analysis of studies on breast cancer risk and diet: The role of fruit and vegetable consumption and the intake of associated micronutrients. Eur. J. Cancer 2000, 36, 636–646. [Google Scholar] [CrossRef]
- Martinez-Perez, C.; Ward, C.; Cook, G.; Mullen, P.; McPhail, D.; Harrison, D.J.; Langdon, S.P. Novel flavonoids as anti-cancer agents: Mechanisms of action and promise for their potential application in breast cancer. Biochem. Soc. Trans. 2014, 42, 1017–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosetti, C.; Spertini, L.; Parpinel, M.; Gnagnarella, P.; Lagiou, P.; Negri, E.; Franceschi, S.; Montella, M.; Peterson, J.; Dwyer, J.; et al. Flavonoids and breast cancer risk in Italy. Cancer Epidemiol. Biomark. Prev. 2005, 14, 805–808. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.L.; Ho, S.C.; Mo, X.F.; Lin, F.Y.; Zhang, N.Q.; Luo, H.; Zhang, X.; Zhang, C.X. Association between flavonoids, flavonoid subclasses intake and breast cancer risk: A case-control study in China. Eur. J. Cancer Prev. 2020, 29, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Hui, C.; Qi, X.; Qianyong, Z.; Xiaoli, P.; Jundong, Z.; Mantian, M. Flavonoids, flavonoid subclasses and breast cancer risk: A meta-analysis of epidemiologic studies. PLoS ONE 2013, 8, 54318. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Bosetti, C.; Negri, E.; Lagiou, P.; La Vecchia, C. Flavonoids, proanthocyanidins, and cancer risk: A network of case-control studies from Italy. Nutr. Cancer 2010, 62, 871–877. [Google Scholar] [CrossRef]
- Fink, B.N.; Steck, S.E.; Wolff, M.S.; Britton, J.A.; Kabat, G.C.; Gaudet, M.M.; Abrahamson, P.E.; Bell, P.; Schroeder, J.C.; Teitelbaum, S.L.; et al. Dietary flavonoid intake and breast cancer survival among women on Long Island. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2285–2292. [Google Scholar] [CrossRef] [Green Version]
- Kyrø, C.; Zamora-Ros, R.; Scalbert, A.; Tjønneland, A.; Dossus, L.; Johansen, C.; Bidstrup, P.E.; Weiderpass, E.; Christensen, J.; Ward, H.; et al. Pre-diagnostic polyphenol intake and breast cancer survival: The European prospective investigation into cancer and nutrition (EPIC) cohort. Breast Cancer Res. Treat. 2015, 154, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Bertoia, M.L.; Rimm, E.B.; Mukamal, K.J.; Hu, F.B.; Willett, W.C.; Cassidy, A. Dietary flavonoid intake and weight maintenance: Three prospective cohorts of 124,086 US men and women followed for up to 24 years. BMJ 2016, 352, i17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernarelli, J.A.; Lambert, J.D. Flavonoid intake is inversely associated with obesity and C-reactive protein, a marker for inflammation, in US adults. Nutr. Diabetes 2017, 7, e276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.H.; Yang, M.Y.; Chan, K.C.; Chung, P.J.; Ou, T.T.; Wang, C.J. Improvement in high-fat diet-induced obesity and body fat accumulation by a nelumbo nucifera leaf flavonoid-rich extract in mice. J. Agric. Food Chem. 2010, 58, 7075–7081. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Mi Hae, S.; Won-Young, L.; Sung Soo, K.; Jae-Heon, K.; Jee-Hyun, K.; Kyoung Kon, K.; Bo-Yeon, K.; Yang-Hyun, K.; Won-Jun, K.; Eun Mi, K.; et al. 2018 Korean society for the study of obesity guideline for the management of obesity in Korea. J. Obes. Metab. Syndr. 2019, 28, 40–45. [Google Scholar] [CrossRef]
- Korea National Institute of Agricultural Sciences. Food and Nutrition Functional Information Flavonoid Ingredient Search. Available online: http://koreanfood.rda.go.kr/kfi/fct/fctCompSrch/list (accessed on 31 March 2020).
- Perez-Jimenez, J.; Neveu, V.; Vos, F.; Scalbert, A. Systematic analysis of the content of 502 polyphenols in 452 foods and beverages: An application of the phenol-explorer database. J. Agric. Food Chem. 2010, 58, 4959–4969. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S. Modeling and variable selection in epidemiologic analysis. Am. J. Public Health 1989, 79, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Farvid, M.S.; Chen, W.Y.; Rosner, B.A.; Tamimi, R.M.; Willett, W.C.; Eliassen, A.H. Fruit and vegetable consumption and breast cancer incidence: Repeated measures over 30 years of follow-up. Int. J. Cancer 2019, 144, 1496–1510. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Shao, F.; Zhang, F.; Miao, Q. Association between dietary carrot intake and breast cancer: A meta-analysis. Medicine 2018, 97, e12164. [Google Scholar] [CrossRef] [PubMed]
- Do, M.H.; Lee, S.S.; Jung, P.J.; Lee, M.H. Intake of fruits, vegetables, and soy foods in relation to breast cancer risk in Korean women: A case-control study. Nutr. Cancer 2017, 57, 20–27. [Google Scholar] [CrossRef]
- Challier, B.; Perarnau, J.M.; Viel, J.F. Garlic, onion and cereal fibre as protective factors for breast cancer: A French case-control study. Eur. J. Epidemiol. 1998, 14, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Adebamowo, C.A.; Cho, E.; Sampson, L.; Katan, M.B.; Spiegelman, D.; Willett, W.C.; Holmes, M.D. Dietary flavonols and flavonol-rich foods intake and the risk of breast cancer. Int. J. Cancer 2005, 114, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.A.; Rock, C.L.; Thompson, P.A.; Caan, B.J.; Cussler, E.; Flatt, S.W.; Pierce, J.P. Vegetable intake is associated with reduced breast cancer recurrence in tamoxifen users: A secondary analysis from the women’s healthy eating and living study. Breast Cancer Res. Treat. 2011, 125, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Chi, F.; Wu, R.; Zeng, Y.C.; Xing, R.; Liu, Y.; Xu, Z.G. Post-diagnosis soy food intake and breast cancer survival: A meta-analysis of cohort studies. Asian Pac. J. Cancer Prev. 2013, 14, 2407–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincenza, G.; Daniele, N.; Angela, A.; Mattia, A.; Milena, V.; Massimo, M.; Stefano, R. Green tea consumption and risk of breast cancer and recurrence—a systematic review and meta-analysis of observational studies. Nutrients 2018, 10, 1886. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Lu, C.K.; Tu, M.C.; Chang, J.H.; Chen, Y.J.; Tu, Y.H.; Huang, H.C. Polyphenol-rich Avicennia marina leaf extracts induce apoptosis in human breast and liver cancer cells and in a nude mouse xenograft model. Oncotarget 2019, 7, 35874–35893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, B.N.; Steck, S.E.; Wolff, M.S.; Britton, J.A.; Kabat, G.C.; Schroeder, J.C.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Dietary flavonoid intake and breast cancer risk among women on Long Island. Am. J. Epidemiol. 2007, 165, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.S.; Kim, H.; Vijayakumar, A.; Kwon, O.; Kim, Y.; Chang, N. Association of dietary flavonoid intake with prevalence of type 2 diabetes mellitus and cardiovascular disease risk factors in Korean women aged ≥30 years. J. Nutr. Sci. Vitaminol. 2017, 63, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.-L.; Zhan, X.-X.; Zuo, L.-S.-Y.; Mo, X.-F.; Zhang, X.; Liu, K.-Y.; Li, L.; Zhang, C.-X. Associations between serum concentration of flavonoids and breast cancer risk among Chinese women. Eur. J. Nutr. 2021, 60, 1347–1362. [Google Scholar] [CrossRef] [PubMed]
- Jodynis-Liebert, J.; Kujawska, M. Biphasic dose-response induced by phytochemicals: Experimental evidence. J. Clin. Med. 2020, 9, 718. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Sanchez, K.; Leyva, M.J.; Wu, M.; Betts, N.M.; Aston, C.E.; Lyons, T.J.; Basu, A.; Sanchez, K.; Leyva, M.J.; et al. Green tea supplementation affects body weight, lipids, and lipid peroxidation in obese subjects with metabolic syndrome. J. Am. Coll. Nutr. 2010, 29, 31–40. [Google Scholar] [CrossRef]
- Caimi, G.; Canino, B.; Montana, M.; Urso, C.; Calandrino, V.; Presti, R.L.; Hopps, E. Lipid peroxidation, protein oxidation, gelatinases, and their inhibitors in a group of adults with obesity. Horm. Metab. Res. 2019, 51, 389–395. [Google Scholar] [CrossRef]
- Blüher, M.; Klöting, N.; Wueest, S.; Schoenle, E.J.; Schön, M.R.; Dietrich, A.; Fasshauer, M.; Stumvoll, M.; Konrad, D. Fas and FasL expression in human adipose tissue is related to obesity, insulin resistance, and type 2 diabetes. J. Clin. Endocrinol. Metab. 2014, 99, E36–E44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, A.C.; Victorino, V.J.; Campos, F.C.; Verenitach, B.D.; Lemos, L.T.; Aranome, A.M.; Oliveira, S.R.; Cecchini, A.L.; Simão, A.N.; Abdelhay, E.; et al. Impact of tumor removal on the systemic oxidative profile of patients with breast cancer discloses lipid peroxidation at diagnosis as a putative marker of disease recurrence. Clin. Breast Cancer 2014, 14, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Alo, P.L.; Visca, P.; Marci, A.; Mangoni, A.; Botti, C.; Di Tondo, U. Expression of fatty acid synthase (FAS) as a predictor of recurrence in stage I breast carcinoma patients. Cancer 1996, 77, 474–482. [Google Scholar] [CrossRef]
- Padmavathi, R.; Senthilnathan, P.; Chodon, D.; Sakthisekaran, D. Therapeutic effect of paclitaxel and propolis on lipid peroxidation and antioxidant system in 7,12 dimethyl benz(a)anthracene-induced breast cancer in female sprague dawley rats. Life Sci. 2006, 78, 2820–2825. [Google Scholar] [CrossRef]
- Brusselmans, K.; Vrolix, R.; Verhoeven, G.; Swinnen, J.V. Induction of cancer cell apoptosis by flavonoids is associated with their ability to inhibit fatty acid synthase activity. J. Biol. Chem. 2005, 280, 5636–5645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saqib, U.; Sarkar, S.; Suk, K.; Mohammad, O.; Baig, M.S.; Savai, R. Phytochemicals as modulators of M1-M2 macrophages in inflammation. Oncotarget 2018, 9, 17937–17950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aryappalli, P.; Al-Qubaisi, S.S.; Attoub, S.; George, J.A.; Arafat, K.; Ramadi, K.B.; Mohamed, Y.A.; Al-Dhaheri, M.M.; Al-Sbiei, A.; Fernandez-Cabezudo, M.J.; et al. The IL-6/STAT3 signaling pathway is an early target of manuka honey-induced suppression of human breast cancer cells. Front Oncol. 2017, 7, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.J.; Choo, W.H.; Kim, H.R.; Chung, K.H.; Oh, S.M. Inhibitory aromatase effects of flavonoids from ginkgo biloba extracts on estrogen biosynthesis. Asian Pac. J. Cancer Prev. 2015, 16, 6317–6325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, S.; Shin, S.; Joung, H. Estimation of dietary flavonoid intake and major food sources of Korean adults. Br. J. Nutr. 2016, 115, 480–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Q.; Kroon, P.A.; Shao, H.; Needs, P.W.; Yang, X. Differential effects of quercetin and two of its derivatives, isorhamnetin and isorhamnetin-3-glucuronide, in inhibiting the proliferation of human breast-cancer MCF-7 cells. J. Agric. Food Chem. 2018, 66, 7181–7189. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, M.; Nieminen, R.; Vuorela, P.; Heinonen, M.; Moilanen, E. Anti-inflammatory effects of flavonoids: Genistein, kaempferol, quercetin, and daidzein inhibit STAT-1 and NF-kappaB activations, whereas flavone, isorhamnetin, naringenin, and pelargonidin inhibit only NF-kappaB activation along with their inhibitory effect on iNOS expression and NO production in activated macrophages. Mediators Inflamm. 2007, 2007, 45673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondonno, N.P.; Dalgaard, F.; Kyrø, C.; Murray, K.; Bondonno, C.P.; Lewis, J.R.; Croft, K.D.; Gislason, G.; Scalbert, A.; Cassidy, A.; et al. Flavonoid intake is associated with lower mortality in the danish diet cancer and health cohort. Nat. Commun. 2019, 10, 3651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyinlola, O.; Vanessa, G.-D.; Alice, W.; Jennifer S, M. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of health survey for england data. J. Epidemiol. Community Health 2014, 68, 856–862. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, H.; Zhu, Z.; Zhang, Q.; Ma, X.; Cui, Z.; Yao, T. Effects and mechanism of flavonoids from astragalus complanatus on breast cancer growth. Naunyn Schmiedebergs Arch. Pharmacol. 2015, 388, 965–972. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Gu, Y.; Zhang, S. Consumption of vegetables and fruits and breast cancer survival: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 599. [Google Scholar] [CrossRef]
- Rodríguez-García, C.; Sánchez-Quesada, C.; J, J.G. Dietary flavonoids as cancer chemopreventive agents: An updated review of human studies. Antioxidants 2019, 8, 137. [Google Scholar] [CrossRef] [Green Version]
- Ambrosone, C.B.; Zirpoli, G.R.; Hutson, A.D.; McCann, W.E.; McCann, S.E.; Barlow, W.E.; Kelly, K.M.; Cannioto, R.; Sucheston-Campbell, L.E.; Hershman, D.L.; et al. Dietary supplement use during chemotherapy and survival outcomes of patients with breast cancer enrolled in a cooperative group clinical trial (SWOG S0221). J. Clin. Oncol. 2019, 38, 804–814. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | With Recurrence (n = 66) | Without Recurrence (n = 506) | p-Value 2 | ||
|---|---|---|---|---|---|
| BMI < 23 (n = 33) | BMI ≥ 23 (n = 33) | BMI < 23 (n = 252) | BMI ≥ 23 (n = 254) | ||
| BMI (kg/m2) | 21.1 ± 1.3 a3 | 26.5 ± 2.3 c | 20.7 ± 1.5 a | 25.7 ± 2.4 b | <0.001 |
| Age (years) | 49.0 ± 9.5 a | 51.5 ± 11.5 a | 50.3 ± 9.7 a | 53.8 ± 10.9 b | <0.001 |
| WC (cm) | 70.5 ± 3.5 a | 81.1 ± 6.6 c | 70.1 ± 5.7 a | 77.9 ± 6.5 b | <0.001 |
| FH, n (%) | 4 (14.8) | 4 (18.2) | 31 (13.9) | 32 (13.8) | 0.952 |
| Drinking, n (%) | 0.002 | ||||
| Never | 16 (48.5) | 25 (75.8) | 156 (61.9) | 155 (61.3) | |
| Former | 8 (24.2) | 3 (9.1) | 77 (30.6) | 77 (30.4) | |
| Current | 9 (27.3) | 5 (15.2) | 19 (7.5) | 21 (8.3) | |
| Smoking, n (%) | 0.934 | ||||
| Never | 31 (93.9) | 32 (97.0) | 235 (93.3) | 237 (93.7) | |
| Former | 2 (6.1) | 1 (3.0) | 13 (5.2) | 11 (4.3) | |
| Current | 0 (0.0) | 0 (0.0) | 4 (1.6) | 5 (2.0) | |
| Tumor, n (%) | 0.003 | ||||
| <2 cm | 19 (57.6) | 9 (27.3) | 155 (61.5) | 139 (54.9) | |
| ≥2 cm | 14 (42.4) | 24 (72.7) | 97 (38.5) | 114 (45.1) | |
| Lymph node metastasis, n (%) | 0.012 | ||||
| Absence | 24 (72.7) | 19 (57.6) | 197 (78.2) | 171 (67.3) | |
| Presence | 9 (27.3) | 14 (42.4) | 55 (21.8) | 83 (32.7) | |
| AJCC, n (%) | 0.075 | ||||
| Stages 0–2 | 28 (84.4) | 25 (75.8) | 226 (90.8) | 220 (87.3) | |
| Stage 3 | 5 (15.2) | 8 (24.2) | 23 (9.2) | 32 (12.7) | |
| Treatment, n (%) | |||||
| Chemotherapy | 22 (66.7) | 22 (68.8) | 124 (56.6) | 126 (55.0) | 0.331 |
| Hormonal therapy | 24 (72.7) | 21 (65.6) | 169 (77.2) | 165 (72.1) | 0.427 |
| Radiotherapy | 11 (33.3) | 15 (46.9) | 121 (55.3) | 128 (55.9) | 0.080 |
| Histologic grade, n (%) | 0.405 | ||||
| Grade 1 | 8 (24.2) | 4 (12.5) | 62 (26.1) | 67 (27.3) | |
| Grade 2 | 11 (33.3) | 15 (46.9) | 103 (43.3) | 108 (44.1) | |
| Grade 3 | 14 (42.4) | 13 (40.6) | 73 (30.7) | 70 (28.6) | |
| ER-negative, n (%) | 11 (33.3) | 14 (42.4) | 71 (28.4) | 77 (30.4) | 0.413 |
| PR-negative, n (%) | 12 (36.4) | 17 (51.5) | 78 (31.2) | 86 (34.0) | 0.140 |
| HER2, n (%) | 0.705 | ||||
| Not amplified | 23 (69.7) | 21 (63.6) | 183 (73.2) | 181 (71.5) | |
| Amplification | 10 (30.3) | 12 (36.4) | 67 (26.8) | 72 (28.5) | |
| Subtype, n (%) | 0.901 | ||||
| HR+/HER2− | 20 (60.6) | 15 (45.5) | 151 (60.4) | 145 (57.3) | |
| HR+/HER2+ | 6 (18.2) | 8 (24.2) | 42 (16.8) | 41 (16.2) | |
| HR+/HER2+ | 4 (12.1) | 4 (12.1) | 25 (10.0) | 31 (12.3) | |
| HR−/HER2− | 3 (9.1) | 6 (18.1) | 32 (12.8) | 36 (14.2) | |
| With Recurrence (n = 66) | Without Recurrence (n = 506) | p-Value 2 | p-Value for Flavonoids × BMI Interaction 4 | |||
|---|---|---|---|---|---|---|
| BMI < 23 (n = 33) | BMI ≥ 23 (n = 33) | BMI < 23 (n = 252) | BMI ≥ 23 (n = 254) | |||
| Flavonoids (mg/d) | 60.84 ± 34.03 b3 | 30.62 ± 20.99 a | 63.23 ± 45.81 b | 57.11 ± 41.08 b | 0.001 | 0.002 |
| Flavonols (mg/d) | 37.97 ± 29.21 b | 18.32 ± 14.07 a | 40.73 ± 41.12 b | 38.76 ± 36.09 b | 0.007 | 0.041 |
| Quercetin (mg/d) | 26.78 ± 17.99 ab | 11.67 ± 13.43 a | 29.36 ± 27.83 b | 27.15 ± 22.68 b | 0.018 | 0.008 |
| Kaempferol (mg/d) | 8.09 ± 6.83 ab | 4.17 ± 3.35 a | 7.85 ± 7.17 b | 8.09 ± 9.47 b | 0.011 | 0.030 |
| Isorhamnetin (mg/d) | 3.10 ± 3.50 | 2.48 ± 2.22 | 3.53 ± 4.11 | 3.52 ± 3.54 | 0.691 | 0.584 |
| Flavone (mg/d) | 22.24 ± 12.51 b | 12.29 ± 11.33 a | 22.51 ± 15.65 b | 18.35 ± 15.38 b | 0.007 | 0.003 |
| Apigenin (mg/d) | 9.09 ± 4.50 ab | 4.61 ± 3.71 a | 9.08 ± 7.89 b | 9.44 ± 11.55 b | 0.004 | 0.005 |
| Luteolin (mg/d) | 8.91 ± 6.43 ab | 7.68 ± 8.40 a | 13.42 ± 9.69 b | 13.15 ± 9.02 b | 0.010 | 0.020 |
| Flavonoid-rich foods (g/d) | 101.33 ± 63.99 b | 61.77 ± 53.44 a | 109.76 ± 79.90 b | 111.59 ± 80.60 b | 0.005 | <0.001 |
| Flavonol-rich foods (g/d) | 65.63 ± 44.03 ab | 41.04 ± 42.30 a | 64.93 ± 56.89 b | 72.11 ± 63.64 b | 0.025 | 0.009 |
| Flavone-rich foods (g/d) | 35.70 ± 31.48 ab | 20.73 ± 24.23 a | 44.83 ± 42.55 b | 39.48 ± 37.77 b | 0.045 | 0.030 |
| Tertiles of Flavonoid Intake | p for Trend 1 | Continuous | |||
|---|---|---|---|---|---|
| T1 | T2 | T3 | |||
| Flavonoids | |||||
| Cutoff (range), 10 mg/d | 2.14 (≤3.15) | 4.27 (3.15 < to ≤ 5.78) | 8.51 (>5.78) | ||
| No. with/without recurrence | 19/76 | 8/88 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.426 (0.18–0.97) | 0.299 (0.11–0.74) | 0.011 | 0.967 (0.95−0.98) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.208 (0.08–0.52) | 0.249 (0.09–0.64) | 0.008 | 0.959 (0.93−0.98) |
| Flavonols | |||||
| Cutoff (range), 10 mg/d | 0.91 (≤1.45) | 2.45 (1.45 < to ≤ 3.56) | 6.80 (>3.56) | ||
| No. with/without recurrence | 18/78 | 9/86 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.479 (0.21–1.06) | 0.325 (0.12–0.82) | 0.026 | 0.945 (0.91−0.97) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.299 (0.12–0.70) | 0.274 (0.99–0.76) | 0.024 | 0.943 (0.90−0.97) |
| Quercetin | |||||
| Cutoff (range), 10 mg/d | 0.36 (≤0.64) | 1.06 (0.64 < to ≤ 2.52) | 5.00 (>2.52) | ||
| No. with/without recurrence | 19/77 | 8/87 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.441 (0.19–1.00) | 0.325 (0.13–0.81) | 0.041 | 0.972 (0.95−0.99) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.353 (0.14–0.84) | 0.301 (0.11–0.82) | 0.047 | 0.966 (0.93−0.99) |
| Kaempferol | |||||
| Cutoff (range), 10 mg/d | 0.21 (≤0.33) | 0.46 (0.33 < to ≤ 0.75) | 1.25 (>0.75) | ||
| No. with/without recurrence | 19/76 | 8/89 | 6/89 | ||
| Crude HR (95% CI) | 1.0 | 0.389 (0.17–0.88) | 0.275 (0.11–0.69) | 0.013 | 0.865 (0.77−0.96) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.427 (0.17–1.04) | 0.268 (0.10–0.69) | 0.014 | 0.868 (0.78−0.96) |
| Isorhamnetin | |||||
| Cutoff (range), 10 mg/d | 0.09 (≤0.16) | 0.23 (0.16 < to ≤ 0.34) | 0.53 (>0.34) | ||
| No. with/without recurrence | 16/79 | 9/87 | 8/88 | ||
| Crude HR (95% CI) | 1.0 | 0.533 (0.23–1.20) | 0.523 (0.22–1.22) | 0.167 | 0.899 (0.77−1.04) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.523 (0.21–1.25) | 0.428 (0.17–1.03) | 0.080 | 0.901 (0.77−1.04) |
| Flavones | |||||
| Cutoff (range), 10 mg/d | 0.59 (≤1.01) | 1.50 (1.01 < to ≤ 2.04) | 2.62 (>2.04) | ||
| No. with/without recurrence | 19/76 | 8/88 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.391 (0.17–0.89) | 0.290 (0.11–0.72) | 0.005 | 0.946 (0.91−0.98) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.403 (0.16–0.98) | 0.337 (0.13–0.86) | 0.015 | 0.948 (0.91−0.98) |
| Apigenin | |||||
| Cutoff (range), 10 mg/d | 0.23 (≤0.45) | 0.67 (0.45 < to ≤ 0.89) | 1.30 (>0.89) | ||
| No. with/without recurrence | 20/76 | 7/88 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.332 (0.14–0.78) | 0.266 (0.10–0.66) | 0.003 | 0.838 (0.73−0.95) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.464 (0.18–1.14) | 0.317 (0.12–0.81) | 0.015 | 0.835 (0.71−0.95) |
| Luteolin | |||||
| Cutoff (range), 10 mg/d | 0.13 (≤0.45) | 0.86 (0.45 < to ≤ 1.30) | 1.35 (>1.30) | ||
| No. with/without recurrence | 17/79 | 10/85 | 6/90 | ||
| Crude HR (95% CI) | 1.0 | 0.588 (0.26–1.28) | 0.315 (0.12–0.80) | 0.011 | 0.974 (0.95−0.99) |
| Adjusted HR (95% CI) 2 | 1.0 | 0.409 (0.17–0.93) | 0.315 (0.11–0.83) | 0.007 | 0.971 (0.94−0.99) |
| Tertiles of Flavonoid-Rich Food Intake | p for Trend 1 | Continuous | |||
|---|---|---|---|---|---|
| T1 | T2 | T3 | |||
| Flavonoid-rich food | |||||
| Cutoff (range), 10 g/d | 3.52 (≤5.99) | 9.25 (5.99 < to ≤ 12.54) | 16.75 (>12.54) | ||
| No. with/without recurrence | 19/75 | 8/88 | 6/91 | ||
| Crude HR (95% CI) | 1.0 | 0.356 (0.15–0.81) | 0.285 (0.11–0.71) | 0.005 | 0.986 (0.97−0.99) |
| Adjusted HR (95% CI)2 | 1.0 | 0.294 (0.11–0.72) | 0.244 (0.09–0.66) | 0.006 | 0.985 (0.97−0.99) |
| Flavonol-rich food | |||||
| Cutoff (range), 10 g/d | 0.85 (≤3.74) | 5.95 (3.74 < to ≤ 8.24) | 11.95 (> 8.24) | ||
| No. with/without recurrence | 17/75 | 9/87 | 7/92 | ||
| Crude HR (95% CI) | 1.0 | 0.416 (0.18–0.93) | 0.339 (0.14–0.81) | 0.012 | 0.979 (0.96−0.99) |
| Adjusted HR (95% CI)2 | 1.0 | 0.384 (0.16–0.88) | 0.321 (0.14–0.81) | 0.014 | 0.979 (0.95−0.99) |
| Flavone-rich food | |||||
| Cutoff (range), 10 g/d | 0.00 (≤1.79) | 2.80 (1.79 < to ≤ 4.49) | 6.80 (> 4.49) | ||
| No. with/without recurrence | 19/72 | 9/91 | 5/91 | ||
| Crude HR (95% CI) | 1.0 | 0.418 (0.18–0.92) | 0.260 (0.09–0.69) | 0.005 | 0.986 (0.97−0.99) |
| Adjusted HR (95% CI)2 | 1.0 | 0.421 (0.18–0.97) | 0.284 (0.10–0.79) | 0.012 | 0.985 (0.97−0.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheon, M.; Chung, M.; Park, Y. Association between Dietary Intake of Flavonoids and Cancer Recurrence among Breast Cancer Survivors. Nutrients 2021, 13, 3049. https://doi.org/10.3390/nu13093049
Cheon M, Chung M, Park Y. Association between Dietary Intake of Flavonoids and Cancer Recurrence among Breast Cancer Survivors. Nutrients. 2021; 13(9):3049. https://doi.org/10.3390/nu13093049
Chicago/Turabian StyleCheon, Minjung, Minsung Chung, and Yongsoon Park. 2021. "Association between Dietary Intake of Flavonoids and Cancer Recurrence among Breast Cancer Survivors" Nutrients 13, no. 9: 3049. https://doi.org/10.3390/nu13093049
APA StyleCheon, M., Chung, M., & Park, Y. (2021). Association between Dietary Intake of Flavonoids and Cancer Recurrence among Breast Cancer Survivors. Nutrients, 13(9), 3049. https://doi.org/10.3390/nu13093049