
Effect of Spirulina Supplementation on Systolic and Diastolic Blood Pressure: Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Design and Search Strategy
2.2. Study Selection
2.3. Extraction and Qualification of the Data
2.4. Statistical Methods
3. Results
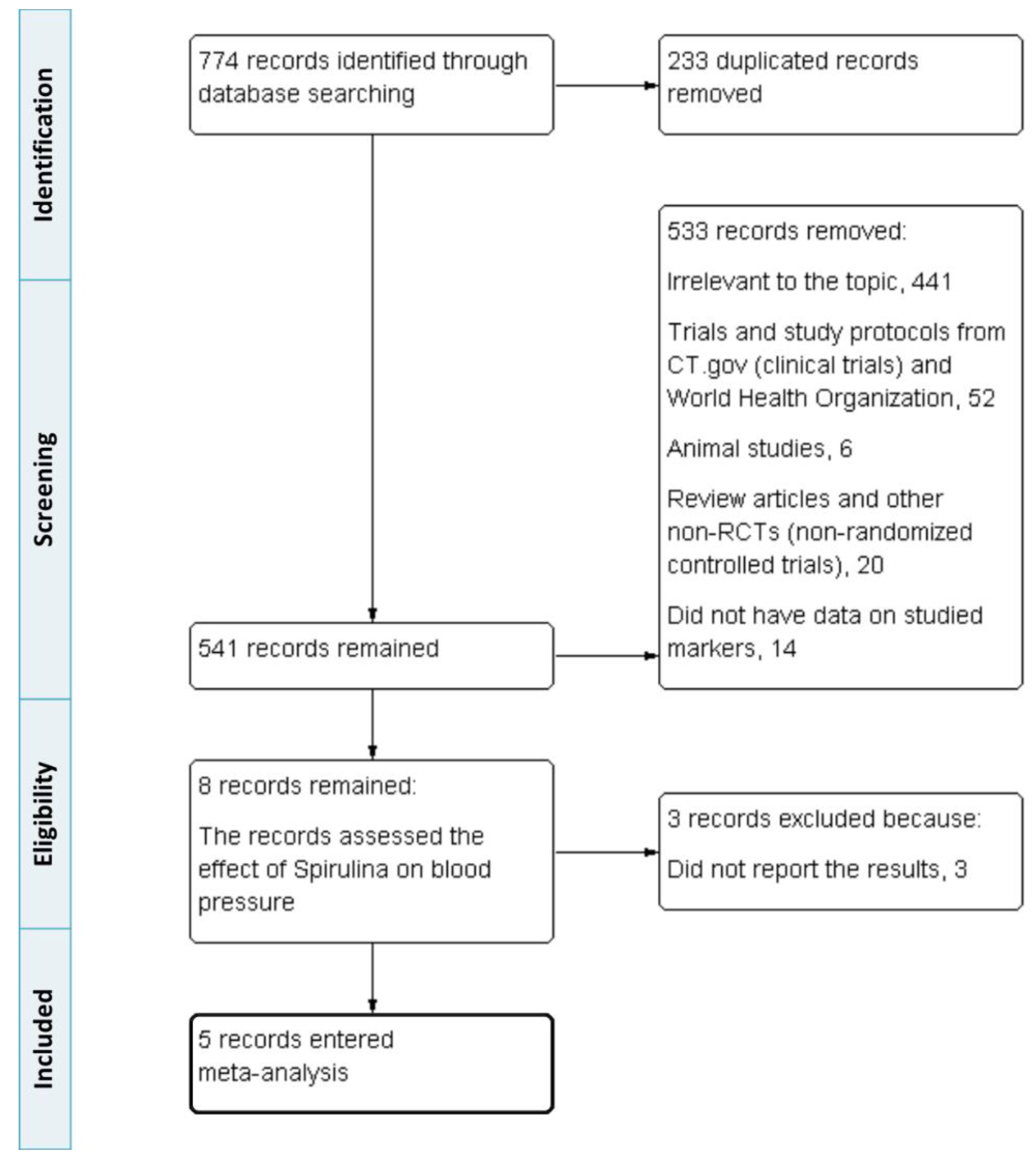
3.1. Selection and Identification of Studies
3.2. Characteristics of Studies
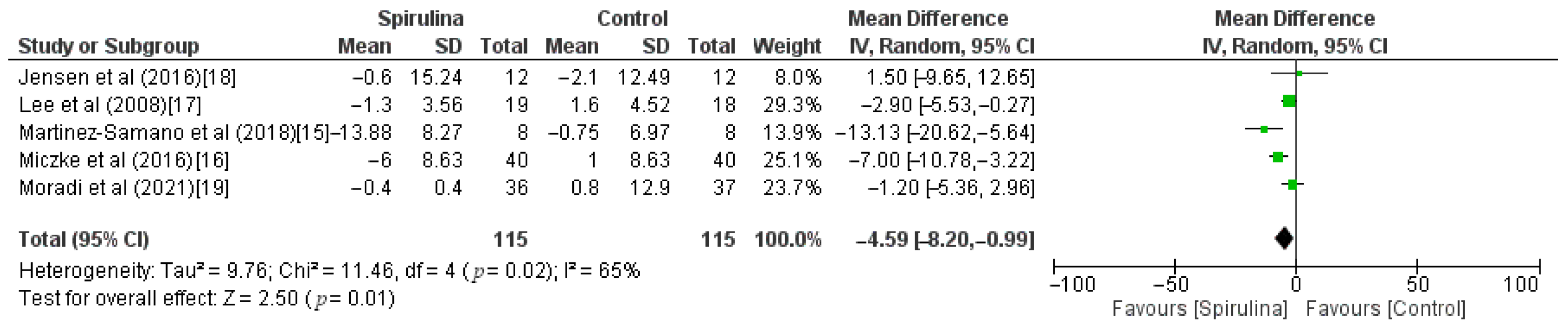
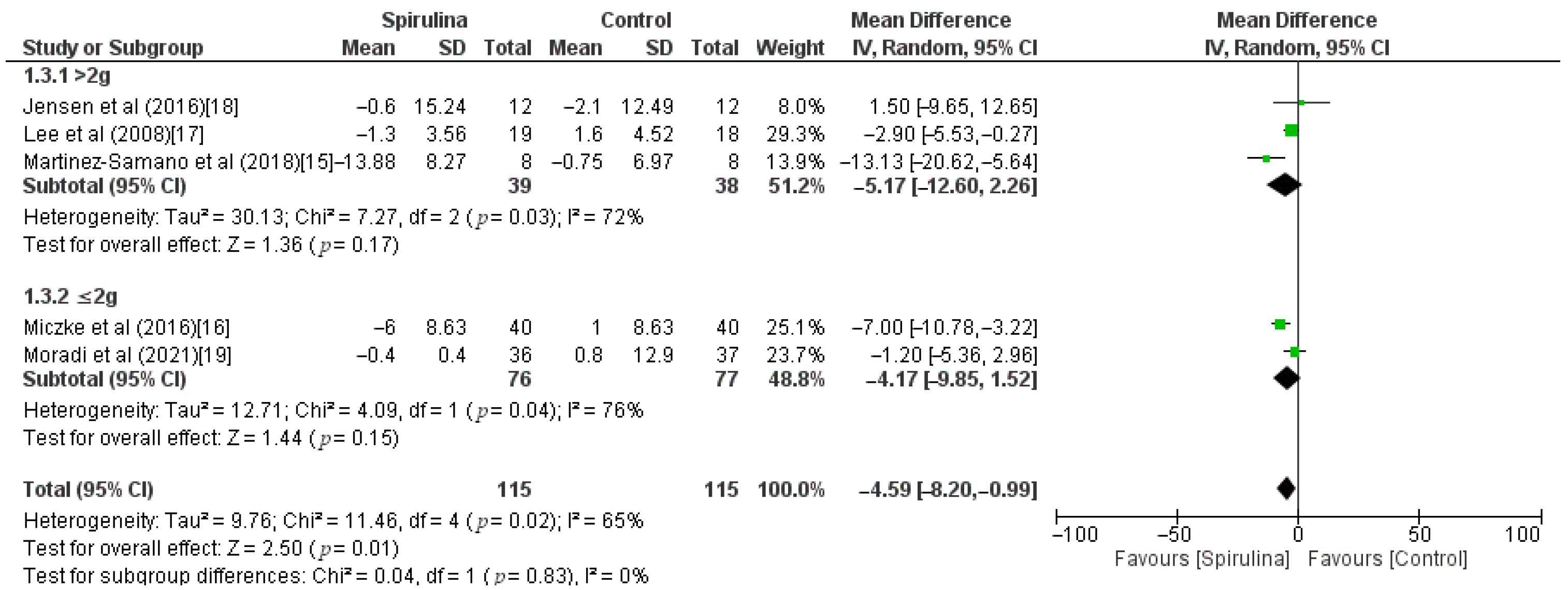
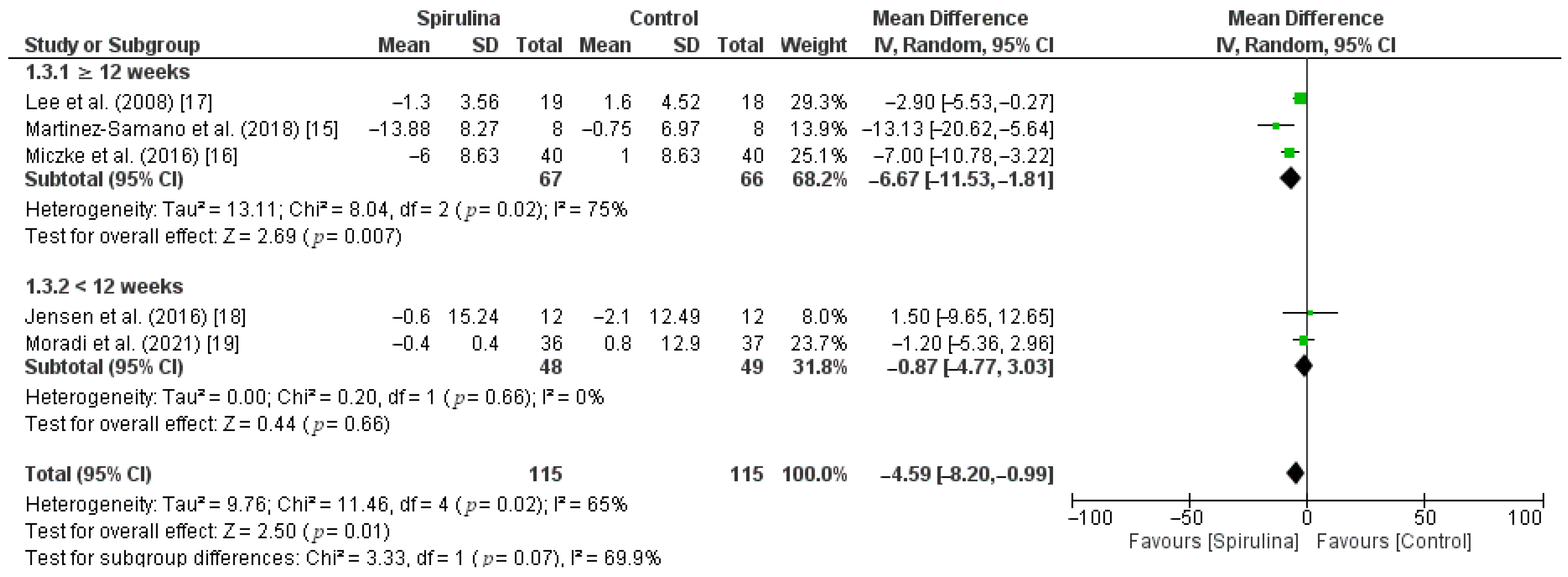
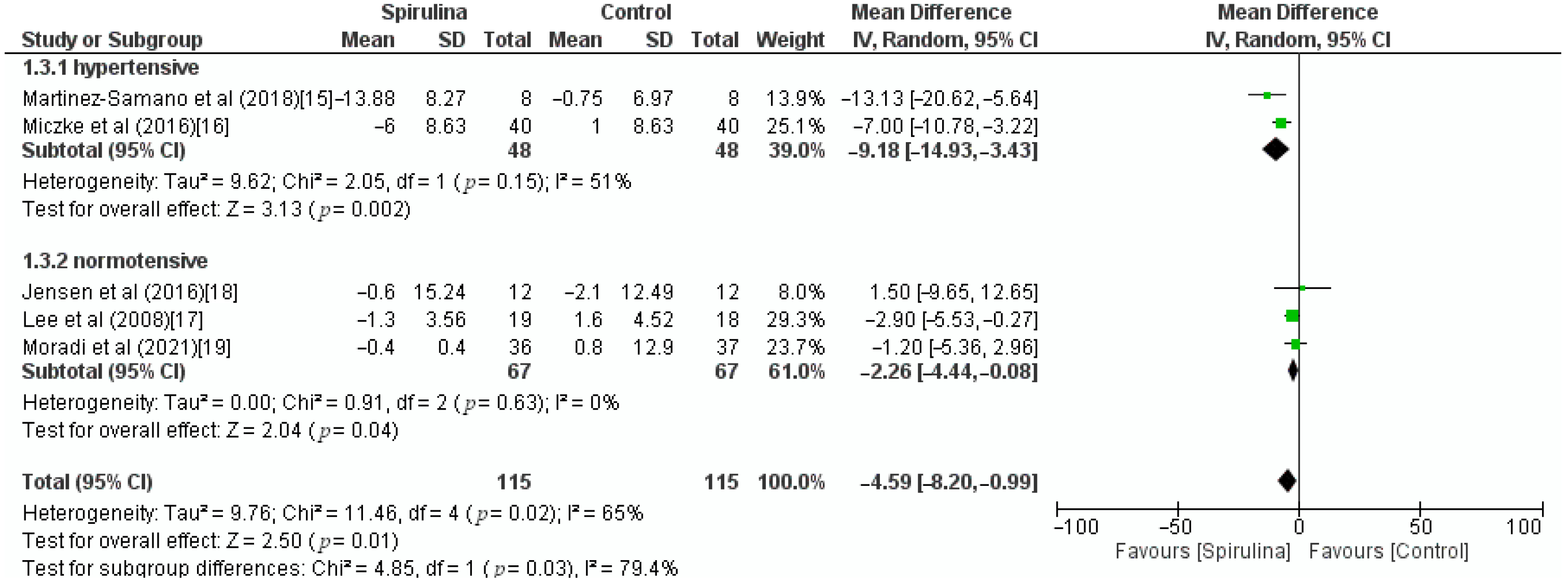
3.3. Effect of Spirulina on Systolic Blood Pressure
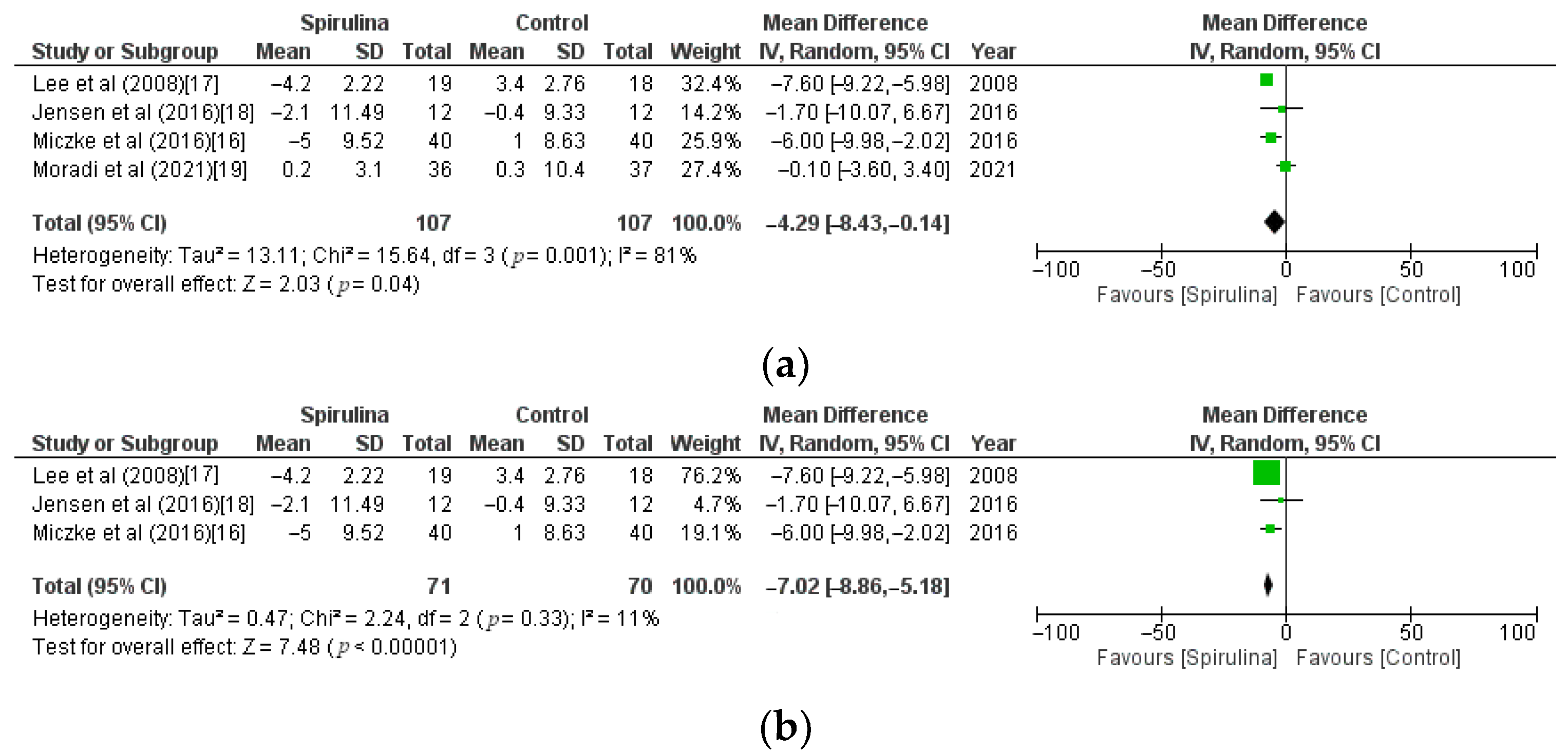
3.4. Effect of Spirulina on Diastolic Blood Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salkic, S.; Ljuca, F.; Batic-Mujanovic, O.; Brkic, S.; Mesic, D.; Mustafic, S. The Frequency of Hypertension Crises in the Emergency Medical Service Department in Tuzla. Med. Arch. 2013, 67, 393–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wermelt, J.A.; Schunkert, H. Management der arteriellen Hypertonie. Herz 2017, 42, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Sood, N.; Reinhart, K.M.; Baker, W.L. Combination therapy for the management of hypertension: A review of the evidence. Am. J. Health Pharm. 2010, 67, 885–894. [Google Scholar] [CrossRef]
- Riva, N.; Lip, G.Y. Which is the Optimal Antihypertensive Combination in Different Diseases, a Renin- Angiotensin-aldosterone System Inhibitor with a Diuretic or with a Calcium Channel Blocker? Curr. Pharm. Des. 2013, 19, 3753–3765. [Google Scholar] [CrossRef]
- Ardalani, H.; Moghadam, M.H.; Rahimi, R.; Soltani, J.; Mozayanimonfared, A.; Moradi, M.; Azizi, A. Sumac as a novel adjunctive treatment in hypertension: A randomized, double-blind, placebo-controlled clinical trial. RSC Adv. 2016, 6, 11507–11512. [Google Scholar] [CrossRef]
- Buono, S.; Langellotti, A.L.; Martello, A.; Rinna, F.; Fogliano, V. Functional ingredients from microalgae. Food Funct. 2014, 5, 1669–1685. [Google Scholar] [CrossRef]
- Christaki, E.; Florou-Paneri, P.; Bonos, E. Microalgae: A novel ingredient in nutrition. Int. J. Food Sci. Nutr. 2011, 62, 794–799. [Google Scholar] [CrossRef]
- Finamore, A.; Palmery, M.; Bensehaila, S.; Peluso, I. Antioxidant, Immunomodulating, and Microbial-Modulating Activities of the Sustainable and EcofriendlySpirulina. Oxidative Med. Cell. Longev. 2017, 2017, 3247528. [Google Scholar] [CrossRef] [Green Version]
- Deng, R.; Chow, T.-J. Hypolipidemic, Antioxidant, and Antiinflammatory Activities of Microalgae Spirulina. Cardiovasc. Ther. 2010, 28, e33–e45. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Liu, L.; Miron, A.; Klímová, B.; Wan, D.; Kuča, K. The antioxidant, immunomodulatory, and anti-inflammatory activities of Spirulina: An overview. Arch. Toxicol. 2016, 90, 1817–1840. [Google Scholar] [CrossRef]
- Gunes, S.; Tamburaci, S.; Dalay, M.C.; Gurhan, I.D. In vitro evaluation of Spirulina platensis extract incorporated skin cream with its wound healing and antioxidant activities. Pharm. Biol. 2017, 55, 1824–1832. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.A.; Baek, S.Y.; Cheong, S.H.; Kim, M.R. Spirulina Enhances Bone Modeling in Growing Male Rats by Regulating Growth-Related Hormones. Nutrients 2020, 12, 1187. [Google Scholar] [CrossRef]
- Serban, M.-C.; Sahebkar, A.; Dragan, S.; Stoichescu-Hogea, G.; Ursoniu, S.; Andrica, F.; Banach, M. A systematic review and meta-analysis of the impact of Spirulina supplementation on plasma lipid concentrations. Clin. Nutr. 2016, 35, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Masuda, K.; Chitundu, M. Multiple micronutrient supplementation using Spirulina platensis and infant growth, morbidity, and motor development: Evidence from a randomized trial in Zambia. PLoS ONE 2019, 14, e0211693. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sámano, J.; De Oca, A.T.-M.; Luqueño-Bocardo, O.I.; Torres-Durán, P.V.; Juárez-Oropeza, M.A. Spirulina maxima Decreases Endothelial Damage and Oxidative Stress Indicators in Patients with Systemic Arterial Hypertension: Results from Exploratory Controlled Clinical Trial. Mar. Drugs 2018, 16, 496. [Google Scholar] [CrossRef] [Green Version]
- Miczke, A.; Szulinska, M.; Hansdorfer-Korzon, R.; Kręgielska-Narożna, M.; Suliburska, J.; Walkowiak, J.; Bogdański, P. Effects of spirulina consumption on body weight, blood pressure, and endothelial function in overweight hypertensive Caucasians: A double-blind, placebo-controlled, randomized trial. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 150–156. [Google Scholar]
- Lee, E.H.; Park, J.-E.; Choi, Y.-J.; Huh, K.-B.; Kim, W.-Y. A randomized study to establish the effects of spirulina in type 2 diabetes mellitus patients. Nutr. Res. Pract. 2008, 2, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, G.S.; Drapeau, C.; Lenninger, M.; Benson, K.F. Clinical Safety of a High Dose of Phycocyanin-Enriched Aqueous Extract from Arthrospira (Spirulina) platensis: Results from a Randomized, Double-Blind, Placebo-Controlled Study with a Focus on Anticoagulant Activity and Platelet Activation. J. Med. Food 2016, 19, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Moradi, S.; Zobeiri, M.; Feizi, A.; Clark, C.C.T.; Entezari, M.H. The effects of spirulina (Arthrospira platensis) supplementation on anthropometric indices, blood pressure, sleep quality, mental health, fatigue status and quality of life in patients with ulcerative colitis: A randomised, double-blinded, placebo-controlled trial. Int. J. Clin. Pract. 2021, e14472. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Moher, D.; Cook, D.J.; Jadad, A.R.; Tugwell, P.; Jones, A.; Pham, B.; Klassen, T.P. Assessing the quality of reports of randomised trials: Implications for the conduct of meta-analyses. Health Technol. Assess 1999, 3, 98. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Jafari, T.; Fallah, A.A.; Barani, A. Effects of vitamin D on serum lipid profile in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Clin. Nutr. 2016, 35, 1259–1268. [Google Scholar] [CrossRef]
- Jafari, T.; Feizi, A.; Askari, G.; Fallah, A.A. Parenteral immunonutrition in patients with acute pancreatitis: A systematic review and meta-analysis. Clin. Nutr. 2015, 34, 35–43. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Deeks, J.; Altman, D. Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Green, S., Eds.; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 10 July 2021).
- Rattanavipanon, W.; Nithiphongwarakul, C.; Sirisuwansith, P.; Chaiyasothi, T.; Thakkinstian, A.; Nathisuwan, S.; Pathomwichaiwat, T. Effect of tomato, lycopene and related products on blood pressure: A systematic review and network meta-analysis. Phytomedicine 2021, 88, 153512. [Google Scholar] [CrossRef]
- Fantin, F.; Macchi, F.; Giani, A.; Bissoli, L. The Importance of Nutrition in Hypertension. Nutrients 2019, 11, 2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Duran, P.V.; Ferreira-Hermosillo, A.; Juarez-Oropeza, M.A. Antihyperlipemic and antihypertensive effects of Spirulina maxima in an open sample of mexican population: A preliminary report. Lipids Health Dis. 2007, 6, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Mazokopakis, E.E.; Papadomanolaki, M.G.; Fousteris, A.A.; Kotsiris, D.A.; Lampadakis, I.M.; Ganotakis, E. The hepatoprotective and hypolipidemic effects of Spirulina (Arthrospira platensis) supplementation in a Cretan population with non-alcoholic fatty liver disease: A prospective pilot study. Ann. Gastroenterol. 2014, 27, 387–394. [Google Scholar]
- Mazokopakis, E.; Starakis, I.K.; Papadomanolaki, M.G.; Mavroeidi, N.G.; Ganotakis, E. The hypolipidaemic effects of Spirulina (Arthrospira platensis) supplementation in a Cretan population: A prospective study. J. Sci. Food Agric. 2014, 94, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Bobescu, E.; Bălan, A.; Moga, M.A.; Teodorescu, A.; Mitrică, M.; Dima, L. Are There Any Beneficial Effects of Spirulina Supplementation for Metabolic Syndrome Components in Postmenopausal Women? Mar. Drugs 2020, 18, 651. [Google Scholar] [CrossRef]
- Carrizzo, A.; Conte, G.M.; Sommella, E.; Damato, A.; Ambrosio, M.; Sala, M.; Scala, M.C.; Aquino, R.P.; De Lucia, M.; Madonna, M.; et al. Novel Potent Decameric Peptide of Spirulina platensis Reduces Blood Pressure Levels Through a PI3K/AKT/eNOS-Dependent Mechanism. Hypertension 2019, 73, 449–457. [Google Scholar] [CrossRef]
- Szulinska, M.; Gibas-Dorna, M.; Miller-Kasprzak, E.; Suliburska, J.; Miczke, A.; Walczak-Gałezewska, M.; Stelmach-Mardas, M.; Walkowiak, J.; Bogdanski, P. Spirulina maxima improves insulin sensitivity, lipid profile, and total antioxidant status in obese patients with well-treated hypertension: A randomized double-blind placebo-controlled study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2473–2481. [Google Scholar] [PubMed]
- Anekthanakul, K.; Senachak, J.; Hongsthong, A.; Charoonratana, T.; Ruengjitchatchawalya, M. Natural ACE inhibitory peptides discovery from Spirulina (Arthrospira platensis) strain C1. Peptides 2019, 118, 170107. [Google Scholar] [CrossRef]
- Wang, K.; Luo, Q.; Hong, H.; Liu, H.; Luo, Y. Novel antioxidant and ACE inhibitory peptide identified from Arthrospira platensis protein and stability against thermal/pH treatments and simulated gastrointestinal digestion. Food Res. Int. 2021, 139, 109908. [Google Scholar] [CrossRef]
- Grosshagauer, S.; Kraemer, K.; Somoza, V. The True Value of Spirulina. J. Agric. Food Chem. 2020, 68, 4109–4115. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, T.; Kormas, K.; Vardaka, E. Cyanotoxin contamination in commercial Spirulina food supplements. J. Consum. Prot. Food Saf. 2021, 16, 227–235. [Google Scholar] [CrossRef]
- Huang, H.; Liao, D.; Pu, R.; Cui, Y. Quantifying the effects of spirulina supplementation on plasma lipid and glucose concentrations, body weight, and blood pressure. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 729–742. [Google Scholar] [CrossRef] [Green Version]
- Yousefi, R.; Saidpour, A.; Mottaghi, A. The effects of Spirulina supplementation on metabolic syndrome components, its liver manifestation and related inflammatory markers: A systematic review. Complement. Ther. Med. 2019, 42, 137–144. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Formulae |
|---|---|
| Formula for combining groups—mean | Mean = N1M1 + N2M2/N1 + N2 |
| Formula for combining groups—SD | SD = square root [(N1 − 1)SD12 + (N2 − 1)SD22 + (N1N2/N1 + N2) × (M12 + M22 − 2M1M2)]/ (N1 + N2 − 1) |
| Formula for imputing correlation coefficient | Corr = (SDE2 + SDC2 − SDdiff2)/(2 × SDE × SDC) |
| Parameter | Description |
|---|---|
| Participants | Adults with arterial hypertension, diabetes mellitus type 2, Body Mass Index (BMI) < 35 and chronic joint pain, or ulcerative colitis |
| Interventions | Oral daily supplementation of Spirulina (1 g, 2 g, 2.3 g, 4.5 g, 8 g) for 2, 8, or 12 weeks |
| Comparison | Oral daily placebo (pure microcrystalline cellulose or not specified) or no intervention |
| Outcomes | Decrease of SBP and DBP |
| Study design | Parallel RCTs were included in the meta-analysis |
| Reference | No. of Subjects | Outcomes Studied before and after Supplementation | Spirulina Group | Placebo/Non-Spirulina Group |
|---|---|---|---|---|
| Martínez-Sámano et al., 2018 [15] | n = 8 Spirulina, n = 8 placebo | SBP (mmHg) before | 140.38 ± 9.04 | 140.75 ± 7.03 |
| SBP (mmHg) after | 126.50 ± 5.53 | 140.00 ± 6.05 | ||
| DBP (mmHg) before | 83.75 ± 5.31 | 84.25 ± 5.28 | ||
| DBP (mmHg) after | - | - | ||
| Miczke et al., 2016 [16] | n = 40 Spirulina, n = 40 placebo | SBP (mmHg) before | 149 ± 7 | 150 ± 7 |
| SBP (mmHg) after | 143 ± 9 | 151 ± 9 | ||
| DBP (mmHg) before | 84 ± 9 | 85 ± 9 | ||
| DBP (mmHg) after | 79 ± 9 | 86 ± 7 | ||
| Lee et al., 2008 [17] | n = 19 Spirulina, n = 18 non-Spirulina | SBP (mmHg) before | 130.7 ± 3.8 | 131.8 ± 4.0 |
| SBP (mmHg) after | 129.4 ± 2.7 | 133.4 ± 4.5 | ||
| DBP (mmHg) before | 84.0 ± 2.1 | 80.1 ± 2.5 | ||
| DBP (mmHg) after | 79.8 ± 2.1 | 83.5 ± 2.7 | ||
| Jensen et al., 2016 [18] | n = 12 Spirulina (female F = 10, male M = 2), n = 12 placebo (F = 9, M = 3) | SBP (mmHg) before | F 120.8 ± 15.3 M 113.5 ± 6.4 | F 112.7 ± 8.9 M 131.7 ± 5.5 |
| SBP (mmHg) after | F 120 ± 15.8 M 114 ± 2.8 | F 111.3 ± 9.9 M 127.7 ± 9.0 | ||
| DBP (mmHg) before | F 75.5 ± 12 M 75 ± 5.7 | F 70.8 ± 9.1 M 75 ± 7 | ||
| DBP (mmHg) after | F 73.3 ± 11.6 M 73.5 ± 6.4 | F 70.2 ± 9.6 M 75.3 ± 7.6 | ||
| Moradi et al., 2021 [19] | n = 36 Spirulina, n = 37 placebo | SBP (mmHg) before | 118.7 ± 9.0 | 117.8 ± 16.6 |
| SBP (mmHg) after | 118.3 ± 6.6 | 118.6 ± 4.8 | ||
| DBP (mmHg) before | 80.4 ± 5.6 | 79.7 ± 11.6 | ||
| DBP (mmHg) after | 80.6 ± 5.3 | 80.0 ± 4.7 |
| Reference | Location | Quality Score | Study Design | No. of Subjects | Health Status | Intervention Duration | Spirulina Group | Control Group | Outcomes Studied |
|---|---|---|---|---|---|---|---|---|---|
| Martinez-Samano et al., 2018 [15] | Mexico | 2 | Parallel | 16 | Systemic arterial hypertension | 12 weeks | 4.5 g per day of Spirulina maxima | Placebo | SBP, DBP |
| Miczke et al., 2016 [16] | Poland | 4 | Parallel | 80 | Systemic arterial hypertension | 12 weeks | 2 g per day of Hawaiian Spirulina maxima | Placebo consisted of pure microcrystalline cellulose | SBP, DBP |
| Lee et al., 2008 [17] | South Korea | 3 | Parallel | 37 | Diabetes mellitus type 2 | 12 weeks | 8 g per day of of freeze-dried Spirulina | Received nothing (control group was instructed not to take any functional foods or supplements) | SBP, DBP |
| Jensen et al., 2016 [18] | USA | 3 | Parallel | 24 | Adults 25–65 years of age with BMI < 35 and chronic pain related to specific joint(s) for >6 months | 2 weeks | 2.3 g per day of of phycocyanin-enriched aqueous extract from Arthrospira (Spirulina) platensis | Placebo | SBP, DBP |
| Moradi et al., 2021 [19] | Iran | 5 | Parallel | 73 | Ulcerative colitis | 8 weeks | 1 g per day of Spirulina | Placebo | SBP, DBP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machowiec, P.; Ręka, G.; Maksymowicz, M.; Piecewicz-Szczęsna, H.; Smoleń, A. Effect of Spirulina Supplementation on Systolic and Diastolic Blood Pressure: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 3054. https://doi.org/10.3390/nu13093054
Machowiec P, Ręka G, Maksymowicz M, Piecewicz-Szczęsna H, Smoleń A. Effect of Spirulina Supplementation on Systolic and Diastolic Blood Pressure: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2021; 13(9):3054. https://doi.org/10.3390/nu13093054
Chicago/Turabian StyleMachowiec, Piotr, Gabriela Ręka, Marcela Maksymowicz, Halina Piecewicz-Szczęsna, and Agata Smoleń. 2021. "Effect of Spirulina Supplementation on Systolic and Diastolic Blood Pressure: Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 13, no. 9: 3054. https://doi.org/10.3390/nu13093054
APA StyleMachowiec, P., Ręka, G., Maksymowicz, M., Piecewicz-Szczęsna, H., & Smoleń, A. (2021). Effect of Spirulina Supplementation on Systolic and Diastolic Blood Pressure: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 13(9), 3054. https://doi.org/10.3390/nu13093054