
Diet Quality and Bone Density in Youth with Healthy Weight, Obesity, and Type 2 Diabetes

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anthropometrics
2.2. Dual-Energy X-ray Absorptiometry
2.3. Diet Intake
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weaver, C.M.; Gordon, C.M.; Janz, K.F.; Kalkwarf, H.J.; Lappe, J.M.; Lewis, R.; O’Karma, M.; Wallace, T.C.; Zemel, B.S. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos Int. 2016, 27, 1281–1386. [Google Scholar] [CrossRef] [Green Version]
- Committee, D.G.A. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2020.
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M.; Reeve, B.B. Evaluation of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1854–1864. [Google Scholar] [CrossRef]
- Baxter-Jones, A.D.G.; A Faulkner, R.; Forwood, M.R.; Mirwald, R.L.; A Bailey, D. Bone mineral accrual from 8 to 30 years of age: An estimation of peak bone mass. J. Bone Miner. Res. 2011, 26, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Movassagh, E.Z.; Vatanparast, H. Current Evidence on the Association of Dietary Patterns and Bone Health: A Scoping Review. Adv. Nutr. 2017, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Coheley, L.M.; Lewis, R.D. Dietary Patterns and Pediatric Bone. Curr. Osteoporos. Rep. 2021, 19, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Wosje, K.S.; Khoury, P.R.; Claytor, R.P.; Copeland, K.A.; Hornung, R.W.; Daniels, S.R.; Kalkwarf, H.J. Dietary patterns associated with fat and bone mass in young children. Am. J. Clin. Nutr. 2010, 92, 294–303. [Google Scholar] [CrossRef] [Green Version]
- Kessler, J.; Koebnick, C.; Smith, N.; Adams, A. Childhood Obesity Is Associated With Increased Risk of Most Lower Extremity Fractures. Clin. Orthop. Relat. Res. 2013, 471, 1199–1207. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, A.V. Association of BMD and FRAX Score with Risk of Fracture in Older Adults with Type 2 Diabetes. JAMA 2011, 305, 2184–2192. [Google Scholar] [CrossRef]
- Kindler, J.M.; Kelly, A.; Khoury, P.R.; Katz, L.E.L.; Urbina, E.M.; Zemel, B.S. Bone Mass and Density in Youth with Type 2 Diabetes, Obesity, and Healthy Weight. Diabetes Care 2020, 43, 2544–2552. [Google Scholar] [CrossRef] [PubMed]
- de Koning, L.; Chiuve, S.E.; Fung, T.T.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Diet-Quality Scores and the Risk of Type 2 Diabetes in Men. Diabetes Care 2011, 34, 1150–1156. [Google Scholar] [CrossRef] [Green Version]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef] [PubMed]
- Seiquer, I.; Mesías, M.; Hoyos, A.M.; Galdó, G.; Navarro, M.P. A Mediterranean dietary style improves calcium utilization in healthy male adolescents. J. Am. Coll. Nutr. 2008, 27, 454–462. [Google Scholar] [CrossRef]
- Zeng, F.; Xue, W.; Cao, W.; Wu, B.; Xie, H.; Fan, F.; Zhu, H.; Chen, Y. Diet-quality scores and risk of hip fractures in elderly urban Chinese in Guangdong, China: A case–control study. Osteoporos. Int. 2014, 25, 2131–2141. [Google Scholar] [CrossRef]
- Shams-White, M.M.; Chung, M.; Du, M.; Fu, Z.; Insogna, K.L.; Karlsen, M.C.; LeBoff, M.S.; Shapses, S.A.; Sackey, J.; Wallace, T.C.; et al. Dietary protein and bone health: A systematic review and meta-analysis from the National Osteoporosis Foundation. Am. J. Clin. Nutr. 2017, 105, 1528–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shams-White, M.M.; Chung, M.; Fu, Z.; Insogna, K.L.; Karlsen, M.C.; LeBoff, M.S.; Shapses, S.A.; Sackey, J.; Shi, J.; Wallace, T.C.; et al. Animal versus plant protein and adult bone health: A systematic review and meta-analysis from the National Osteoporosis Foundation. PLoS ONE 2018, 13, e0192459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, T.C.; Marzorati, M.; Spence, L.; Weaver, C.M.; Williamson, P.S. New Frontiers in Fibers: Innovative and Emerging Research on the Gut Microbiome and Bone Health. J. Am. Coll. Nutr. 2017, 36, 218–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whisner, C.M.; Martin, B.R.; Nakatsu, C.H.; A Story, J.; Macdonald-Clarke, C.J.; McCabe, L.D.; McCabe, G.P.; Weaver, C.M. Soluble Corn Fiber Increases Calcium Absorption Associated with Shifts in the Gut Microbiome: A Randomized Dose-Response Trial in Free-Living Pubertal Females. J. Nutr. 2016, 146, 1298–1306. [Google Scholar] [CrossRef] [Green Version]
- Whisner, C.M.; Martin, B.R.; Nakatsu, C.H.; McCabe, G.P.; McCabe, L.D.; Peacock, M.; Weaver, C.M. Soluble maize fibre affects short-term calcium absorption in adolescent boys and girls: A randomised controlled trial using dual stable isotopic tracers. Br. J. Nutr. 2014, 112, 446–456. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Ding, M.; Sampson, L.; Willett, W.C.; E Manson, J.; Wang, M.; Rosner, B.; Hu, F.B.; Sun, Q. Intake of whole grain foods and risk of type 2 diabetes: Results from three prospective cohort studies. BMJ 2020, 370, m2206. [Google Scholar] [CrossRef]
- Gower, B.A.; Bergman, R.; Stefanovski, D.; Darnell, B.; Ovalle, F.; Fisher, G.; Sweatt, S.K.; Resuehr, H.S.; Pelkman, C. Baseline insulin sensitivity affects response to high-amylose maize resistant starch in women: A randomized, controlled trial. Nutr. Metab. (Lond.) 2016, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer-Davis, E.J.; Lawrence, J.M.; Dabelea, D.; Divers, J.; Isom, S.; Dolan, L.; Imperatore, G.; Linder, B.; Marcovina, S.; Pettitt, D.J.; et al. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002–2012. N. Engl. J. Med. 2017, 376, 1419–1429. [Google Scholar] [CrossRef] [Green Version]
- Gordon, C.M.; Leonard, M.B.; Zemel, B.S. 2013 Pediatric Position Development Conference: Executive summary and reflections. J. Clin. Densitom 2014, 17, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Gunnes, M.; Lehmann, E.H. Dietary calcium, saturated fat, fiber and vitamin C as predictors of forearm cortical and trabecular bone mineral density in healthy children and adolescents. Acta Paediatr. 1995, 84, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Vogel, K.A.; Martin, B.R.; McCabe, L.D.; Peacock, M.; Warden, S.J.; McCabe, G.P.; Weaver, C.M. The effect of dairy intake on bone mass and body composition in early pubertal girls and boys: A randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 1214–1229. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Healthy Weight | Obesity | Type 2 Diabetes | p | |
|---|---|---|---|---|
| n = 197 | n = 128 | n = 90 | ||
| Age (years) | 17.8 (3.6) | 18.5 (3.4) | 18.5 (3.0) | 0.089 |
| Sex (% female) | 65.6% | 76.4% | 71.0% | 0.087 |
| Ancestry (% African American) | 50.0% | 66.2% | 51.4% | 0.006 |
| Height Z-score | 0.15 (0.99) | 0.20 (1.10) | 0.24 (1.17) | 0.767 |
| BMI Z-score | 0.14 (−0.43 to 0.52) | 2.33 (1.73 to 2.90) a | 1.89 (1.47 to 2.84) a | <0.001 |
| aBMD Z-score | 0.53 (0.85) | 0.84 (0.93) a | 0.92 (0.88) a | <0.001 |
| Energy (kcal/day) | 2305 (802) | 2351 (717) | 2263 (798) | 0.702 |
| HbA1c (%) | 5.3 (5.1 to 5.5) | 5.5 (5.2 to 5.7) a | 6.9 (5.7 to 10.2) a,b | <0.001 |
| Maximum Score | Healthy Weight | Obesity | T2D | p | |
|---|---|---|---|---|---|
| Total HEI | 100 | 49.7 (41.6 to 56.4) | 46.6 (39.9 to 52.3) | 51.1 (44.1 to 55.6) b | 0.024 |
| HEI Sub-Components | |||||
| Adequacy Sub-Components | |||||
| Meats and beans | 10 | 9.9 (6.4 to 10) | 10.0 (7.09 to 10) | 10.0 (9.3 to 10) a,b | 0.001 |
| Total vegetables | 5 | 2.3 (1.4) | 2.1 (1.2) | 2.7 (1.4) a,b | 0.004 |
| Dark green and orange vegetables | 5 | 1.1 (1.6) | 1.0 (1.5) | 1.2 (1.7) | 0.563 |
| Total fruit | 5 | 1.1 (0.0 to 2.5) | 0.7 (0.0 to 2.2) | 0.6 (0.0 to 2.2) | 0.166 |
| Whole fruit | 5 | 0.1 (0.0 to 2.2) | 0.0 (0.0 to 1.1) | 0.0 (0.0 to 0.9) a | 0.080 |
| Total grains | 5 | 4.7 (0.6) | 4.7 (0.6) | 4.7 (0.6) | 0.844 |
| Whole grains | 5 | 1.1 (0.0 to 2.5) | 0.6 (0.0 to 2.0) | 0.8 (0.0 to 1.5) | 0.120 |
| Milk | 10 | 6.2 (2.8) | 5.1 (2.8) a | 5.3 (2.6) | 0.002 |
| Oils | 10 | 7.2 (2.7) | 7.3 (2.8) | 8.3 (2.3) a,b | 0.003 |
| Moderation Sub-Components | |||||
| Saturated fat | 10 | 4.9 (3.1) | 5.0 (3.0) | 3.8 (3.1) a,b | 0.008 |
| Sodium | 10 | 2.6 (2.3) | 2.8 (2.4) | 1.3 (1.9) a,b | <0.001 |
| Empty calories | 20 | 8.4 (5.3) | 7.5 (5.5) | 11.0 (5.3) a,b | <0.001 |
| b | SE | Beta | p | |
|---|---|---|---|---|
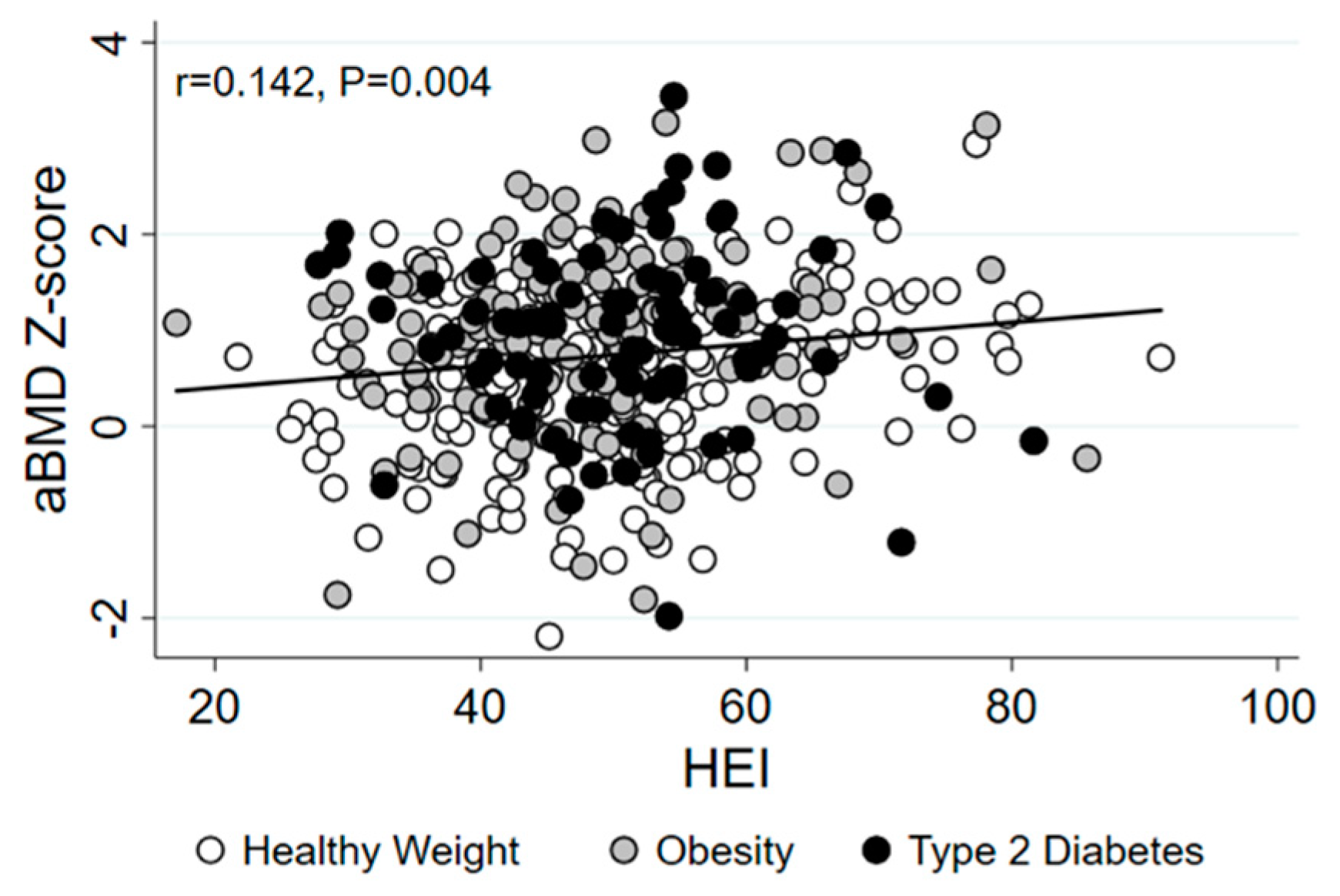
| Total HEI | 0.009 | 0.004 | 0.114 | 0.025 |
| HEI Sub-Components | ||||
| Adequacy | ||||
| Meats and beans | 0.138 | 0.092 | 0.074 | 0.133 |
| Total vegetables | 0.022 | 0.034 | 0.032 | 0.520 |
| Dark green and orange vegetables | 0.022 | 0.028 | 0.038 | 0.438 |
| Total fruit | 0.018 | 0.029 | 0.031 | 0.528 |
| Whole fruit | 0.021 | 0.030 | 0.036 | 0.487 |
| Total grains | −0.022 | 0.095 | 0.011 | 0.817 |
| Whole grains | 0.059 | 0.030 | 0.098 | 0.052 |
| Milk | 0.013 | 0.017 | 0.040 | 0.439 |
| Oils | 0.007 | 0.017 | 0.021 | 0.666 |
| Moderation | ||||
| Saturated fat | 0.004 | 0.014 | 0.012 | 0.806 |
| Sodium | −0.032 | 0.020 | −0.081 | 0.103 |
| Empty calories | 0.022 | 0.008 | 0.131 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kindler, J.M.; Gallo, S.; Khoury, P.R.; Urbina, E.M.; Zemel, B.S. Diet Quality and Bone Density in Youth with Healthy Weight, Obesity, and Type 2 Diabetes. Nutrients 2021, 13, 3288. https://doi.org/10.3390/nu13093288
Kindler JM, Gallo S, Khoury PR, Urbina EM, Zemel BS. Diet Quality and Bone Density in Youth with Healthy Weight, Obesity, and Type 2 Diabetes. Nutrients. 2021; 13(9):3288. https://doi.org/10.3390/nu13093288
Chicago/Turabian StyleKindler, Joseph M., Sina Gallo, Philip R. Khoury, Elaine M. Urbina, and Babette S. Zemel. 2021. "Diet Quality and Bone Density in Youth with Healthy Weight, Obesity, and Type 2 Diabetes" Nutrients 13, no. 9: 3288. https://doi.org/10.3390/nu13093288
APA StyleKindler, J. M., Gallo, S., Khoury, P. R., Urbina, E. M., & Zemel, B. S. (2021). Diet Quality and Bone Density in Youth with Healthy Weight, Obesity, and Type 2 Diabetes. Nutrients, 13(9), 3288. https://doi.org/10.3390/nu13093288