
Gastroprotective Effect of Enteral Nutrition Formula in Mice Injected Subcutaneously with Indomethacin

Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Animals
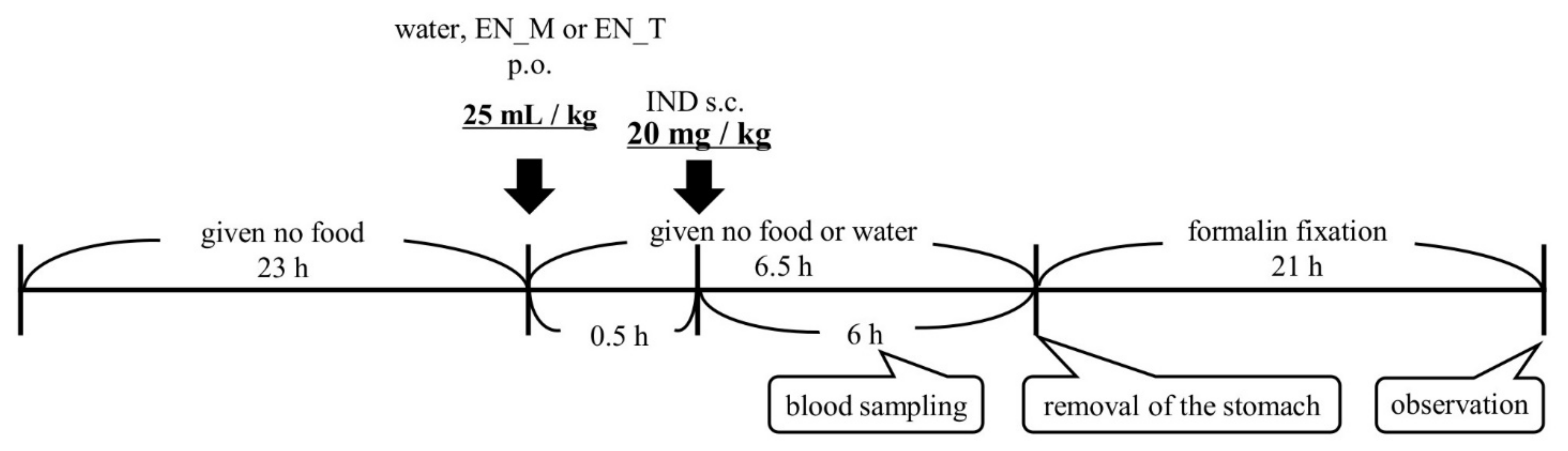
2.3. Dosing and Blood Sampling Schedule
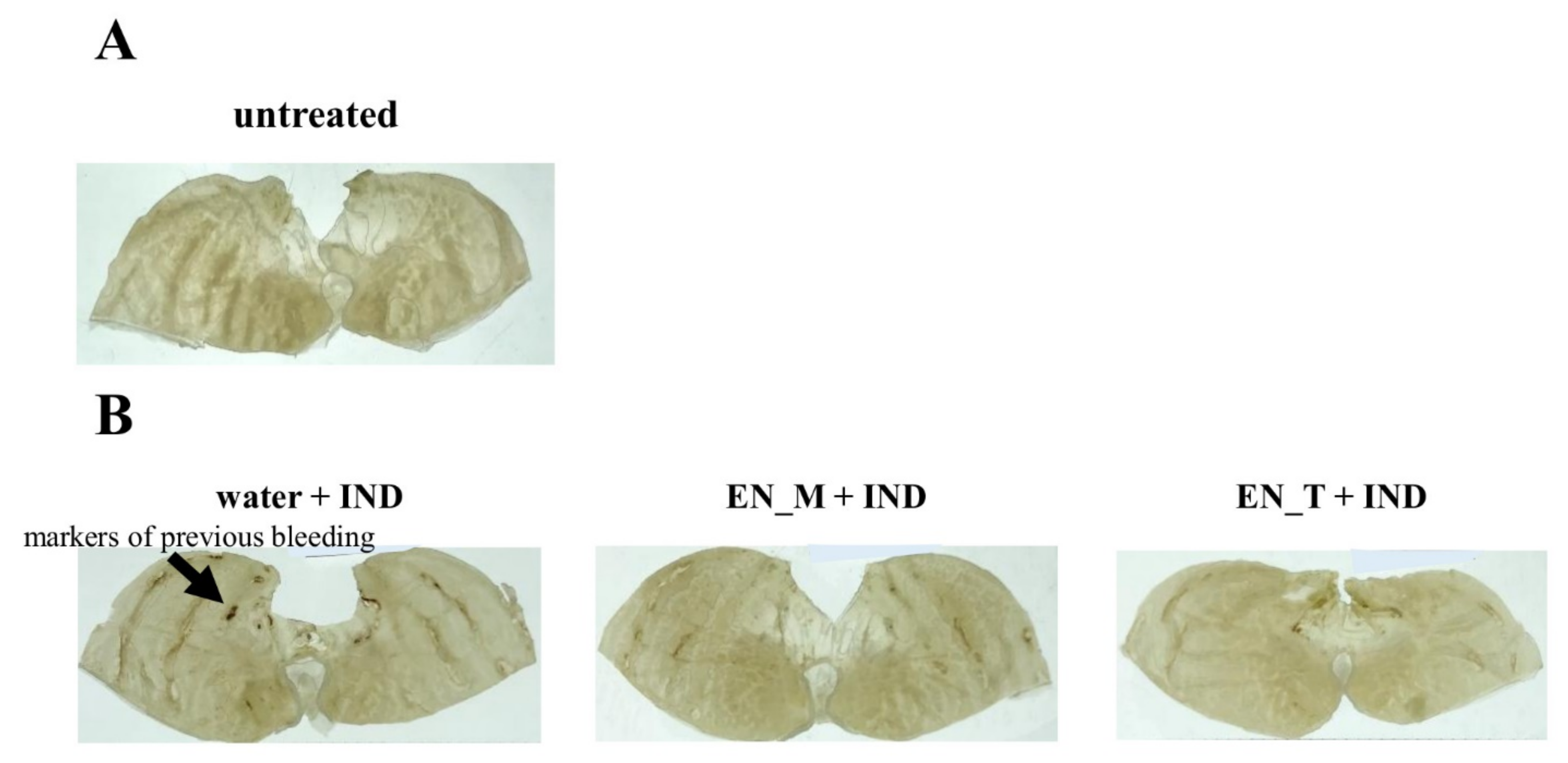
2.4. Observation of Gastric Lesions Induced by IND
2.5. Analysis of Plasma IND Concentrations
2.6. Calculation of Pharmacokinetic Parameters
2.7. Statistical Analysis
3. Results
3.1. Effect of Enteral Nutrition Formulas on Gastric Lesions Induced by Subcutaneous IND Injection
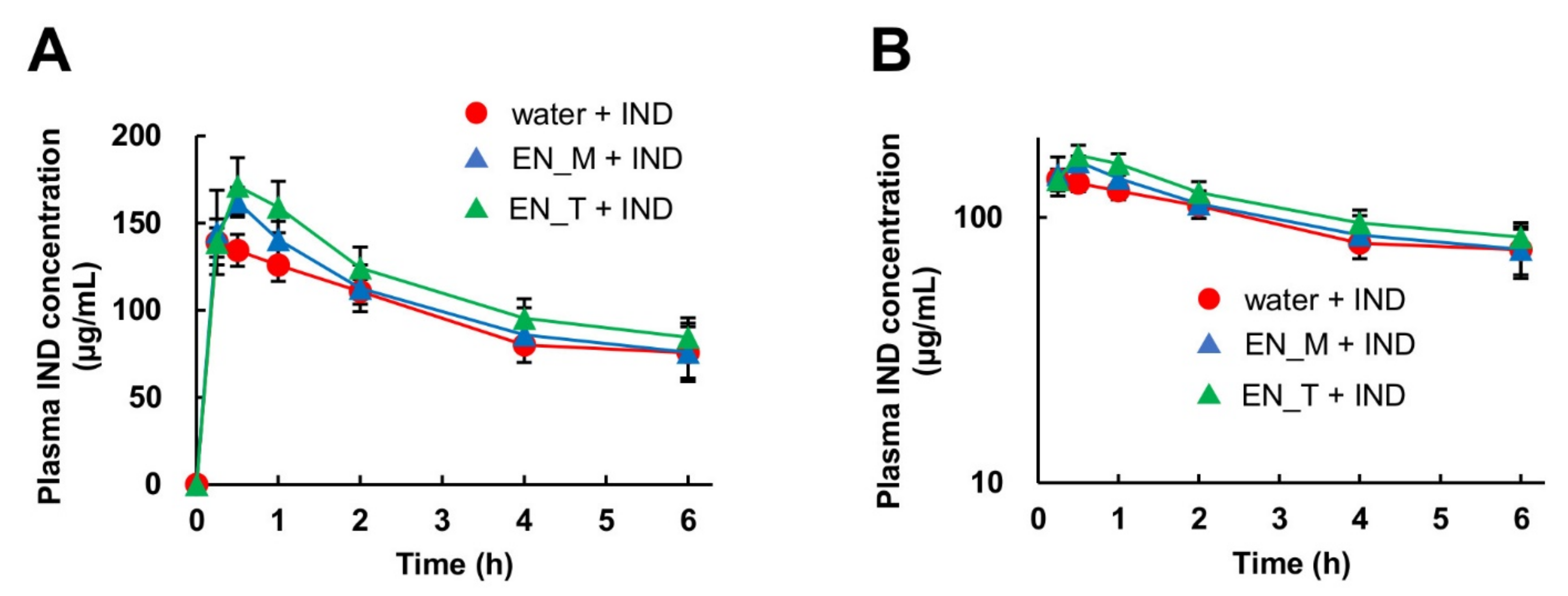
3.2. Effect of Enteral Nutrition Formulas on Plasma IND Concentration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Auriel, E.; Regev, K.; Korczyn, A.D. Nonsteroidal anti-inflammatory drugs exposure and the central nervous system. Handb. Clin. Neurol. 2014, 119, 577–584. [Google Scholar]
- Desborough, M.J.R.; Keeling, D.M. The aspirin story-from willow to wonder drug. Br. J. Haematol. 2017, 177, 674–683. [Google Scholar] [CrossRef] [Green Version]
- Satoh, K.; Yoshino, J.; Akamatsu, T.; Itoh, T.; Kato, M.; Kamada, T.; Takagi, A.; Chiba, T.; Nomura, S.; Mizokami, Y.; et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2015. J. Gastroenterol. 2016, 51, 177–194. [Google Scholar] [CrossRef] [Green Version]
- Hawkey, C.J.; Karrasch, J.A.; Szczepañski, L.; Walker, D.G.; Barkun, A.; Swannell, A.J.; Yeomans, N.D. Omeprazole compared with misoprostol for ulcers associated with nonsteroidal antiinflammatory drugs. Omeprazole versus Misoprostol for NSAID-induced Ulcer Management (OMNIUM) Study Group. N. Engl. J. Med. 1998, 338, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Williams, C. Occurrence and significance of gastric colonization during acid inhibitory therapy. Best Pract. Res. Clin. Gastroenterol. 2001, 15, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Cadle, R.M.; Mansouri, M.D.; Logan, N.; Kudva, D.R.; Musher, D.M. Association of proton-pump inhibitors with outcomes in Clostridium difficile colitis. Am. J. Health Syst. Pharm. 2007, 64, 2359–2363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ianiro, G.; Cammarota, G.; Valerio, L.; Annicchiarico, E.B.; Milani, A.; Siciliano, M.; Gasbarrini, A. Microscopic colitis. World J. Gastroenterol. 2012, 18, 6206–6215. [Google Scholar] [CrossRef]
- Mori, S.; Kadochi, Y.; Luo, Y.; Fujiwara-Tani, R.; Nishiguchi, Y.; Kishi, S.; Fujii, K.; Ohmori, H.; Kuniyasu, H. Proton pump inhibitor induced collagen expression in colonocytes is associated with collagenous colitis. World J. Gastroenterol. 2017, 23, 1586–1593. [Google Scholar] [CrossRef]
- Takeda, T.; Asaoka, D.; Tajima, Y.; Matsumoto, K.; Takeda, N.; Hiromoto, T.; Okubo, S.; Saito, H.; Aoyama, T.; Shibuya, T.; et al. Hemorrhagic polyps formed like fundic gland polyps during long term proton pump inhibitor administration. Clin. J. Gastroenterol. 2017, 10, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Kendall, M.J.; Gibson, R.; Walt, R.P. Co-administration of misoprostol or ranitidine with indomethacin: Effects on pharmacokinetics, abdominal symptoms and bowel habit. Aliment. Pharmacol. Ther. 1992, 6, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Soons, P.A.; van den Berg, G.; Danhof, M.; van Brummelen, P.; Jansen, J.B.; Lamers, C.B.; Breimer, D.D. Influence of single- and multiple-dose omeprazole treatment on nifedipine pharmacokinetics and effects in healthy subjects. Eur. J. Clin. Pharmacol. 1992, 42, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Dammann, H.G.; Simon-Schultz, J.; Steinhoff, I.; Damaschke, A.; Schmoldt, A.; Sallowsky, E. Differential effects of misoprostol and ranitidine on the pharmacokinetics of diclofenac and gastrointestinal symptoms. Br. J. Clin. Pharmacol. 1993, 36, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Serbin, M.A.; Guzauskas, G.F.; Veenstra, D.L. Clopidogrel-proton pump inhibitor drug-drug interaction and risk of adverse clinical outcomes among PCI-treated ACS patients: A meta-analysis. J. Manag. Care Spec. Pharm. 2016, 22, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Le Merdy, M.; Tan, M.L.; Sun, D.; Ni, Z.; Lee, S.C.; Babiskin, A.; Zhao, L. Physiologically based pharmacokinetic modeling approach to identify the drug-drug interaction mechanism of nifedipine and a proton pump inhibitor, omeprazole. Eur. J. Drug Metab. Pharmacokinet. 2021, 46, 41–51. [Google Scholar] [CrossRef]
- Yoshimi, T.; Yamagishi, Y.; Kanegawa, I.; Suda, M.; Saiki, R.; Tanaka, K.I.; Goda, H.; Kudo, T.; Ito, K. Study of the inhibitory effects of enteral nutrition formula on indomethacin-induced gastric lesions in mice. Nutrients 2019, 11, 3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varghese, D.; Ishida, C.; Koya, H.H. Polypharmacy, 2nd ed.; StatPearls Publishing, LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Nobelpharma. Indacin IV 1 mg (Indomethacin), 14th Revision; [package insert]; Nobelpharma Co., Ltd.: Tokyo, Japan, 2019. [Google Scholar]
- Senju Pharmaceutical. IBULIEF® I.V. 20 mg (Ibuprofen) 1st Revision; [package insert]; Senju Pharmaceutical Co., Ltd.: Osaka, Japan, 2018. [Google Scholar]
- Kaken Pharmaceutical. ROPION® (Flurbiprofen) 16th Revision; [package insert]; Kaken Pharmaceutical Co., Ltd: Tokyo, Japan, 2021. [Google Scholar]
- Nissin Pharmaceutical. Ketoprofen IM Inj. 50 mg “NISSIN” (Ketoprofen) 12th Revision; [package insert]; Nissin Pharmaceutical Co., Ltd.: Yamagata, Japan, 2021. [Google Scholar]
- Nipro Corporation. Indomethacin Suppositories (Indomethacin) 2nd Revision; [package insert]; Nipro Corporation: Osaka, Japan, 2021. [Google Scholar]
- Nichi-Iko Pharmaceutical. Diclofenac Sodium (Diclofenac Sodium) 4th Revision; [package insert]; Nichi-Iko Pharmaceutical Co., Ltd.: Toyama, Japan, 2021. [Google Scholar]
- Mizokami, Y.; Shiraishi, T.; Otsubo, T.; Narushima, K.; Matsuoka, T. Clinical studies of gastric ulcer in rheumatoid arthritis patients receiving long-term NSAIDs therapy. Clin. Rheumatol. 1998, 10, 130–141. [Google Scholar]
- Langenbach, R.; Morham, S.G.; Tiano, H.F.; Loftin, C.D.; Ghanayem, B.I.; Chulada, P.C.; Mahler, J.F.; Lee, C.A.; Goulding, E.H.; Kluckman, K.D.; et al. Prostaglandin synthase 1 gene disruption in mice reduces arachidonic acid-induced inflammation and indomethacin-induced gastric ulceration. Cell 1995, 83, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, K. Pathogenesis of NSAID-induced gastric damage: Importance of cyclooxygenase inhibition and gastric hypermotility. World J. Gastroenterol. 2012, 18, 2147–2160. [Google Scholar] [CrossRef]
- Yamamoto, A.; Itoh, T.; Nasu, R.; Nishida, R. Sodium alginate ameliorates indomethacin-induced gastrointestinal mucosal injury via inhibiting translocation in rats. World J. Gastroenterol. 2014, 20, 2641–2652. [Google Scholar] [CrossRef]
- Horibe, S.; Tanahashi, T.; Kawauchi, S.; Mizuno, S.; Rikitake, Y. Preventative effects of sodium alginate on indomethacin-induced small-intestinal injury in mice. Int. J. Med. Sci. 2016, 13, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Piper, J.M.; Ray, W.A.; Daugherty, J.R.; Griffin, M.R. Corticosteroid use and peptic ulcer disease: Role of nonsteroidal anti-inflammatory drugs. Ann. Intern. Med. 1991, 114, 735–740. [Google Scholar] [CrossRef]
- Tsujimoto, S.; Mokuda, S.; Matoba, K.; Yamada, A.; Jouyama, K.; Murata, Y.; Ozaki, Y.; Ito, T.; Nomura, S.; Okuda, Y. The prevalence of endoscopic gastric mucosal damage in patients with rheumatoid arthritis. PLoS ONE 2018, 13, e0200023. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.; Trevisani, L.; Nielsen, I.; Tassinari, D.; Panzini, I.; Abbasciano, V. Randomized trial of omeprazole or ranitidine versus placebo in the prevention of chemotherapy-induced gastroduodenal injury. J. Clin. Oncol. 2000, 18, 463–467. [Google Scholar] [CrossRef]
- Lanza, F.L.; Hunt, R.H.; Thomson, A.B.; Provenza, J.M.; Blank, M.A. Endoscopic comparison of esophageal and gastroduodenal effects of risedronate and alendronate in postmenopausal women. Gastroenterology 2000, 119, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, L.; Vidal, X.; Vendrell, L.; Moretti, U.; Laporte, J.R. Spanish-italian collaborative group for the epidemiology of gastrointestinal bleeding. Upper gastrointestinal bleeding associated with antiplatelet drugs. Aliment. Pharmacol. Ther. 2006, 23, 235–242. [Google Scholar] [CrossRef]
- Hallas, J.; Dall, M.; Andries, A.; Andersen, B.S.; Aalykke, C.; Hansen, J.M.; Andersen, M.; Lassen, A.T. Use of single and combined antithrombotic therapy and risk of serious upper gastrointestinal bleeding: Population based case-control study. BMJ 2006, 333, 726. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Sanaka, M.; Nagasawa, K.; Abe, K.; Fukami, M.; Nakayama, S.; Tsuchiya, A.; Ishii, T.; Kuyama, Y. Gastroduodenal mucosal injury in patients on antiplatelet therapy. Thromb. Res. 2007, 120, 465–469. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Water + IND | EN_M + IND | EN_T + IND | |
|---|---|---|---|
| Tmax (h) | 0.45 ± 0.29 | 0.45 ± 0.10 | 0.50 ± 0.00 |
| Cmax (µg/mL) | 142 ± 12 | 163 ± 8 * | 171 ± 16 * |
| AUC0-6 (µg·h/mL) | 581 ± 23 | 614 ± 85 | 746 ± 19 * |
| MRT (h) | 2.66 ± 0.09 | 2.61 ± 0.20 | 2.67 ± 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamagishi, Y.; Saiki, R.; Yoshimi, T.; Kudo, T.; Ito, K. Gastroprotective Effect of Enteral Nutrition Formula in Mice Injected Subcutaneously with Indomethacin. Nutrients 2021, 13, 3297. https://doi.org/10.3390/nu13093297
Yamagishi Y, Saiki R, Yoshimi T, Kudo T, Ito K. Gastroprotective Effect of Enteral Nutrition Formula in Mice Injected Subcutaneously with Indomethacin. Nutrients. 2021; 13(9):3297. https://doi.org/10.3390/nu13093297
Chicago/Turabian StyleYamagishi, Yoshiaki, Rei Saiki, Takeshi Yoshimi, Toshiyuki Kudo, and Kiyomi Ito. 2021. "Gastroprotective Effect of Enteral Nutrition Formula in Mice Injected Subcutaneously with Indomethacin" Nutrients 13, no. 9: 3297. https://doi.org/10.3390/nu13093297
APA StyleYamagishi, Y., Saiki, R., Yoshimi, T., Kudo, T., & Ito, K. (2021). Gastroprotective Effect of Enteral Nutrition Formula in Mice Injected Subcutaneously with Indomethacin. Nutrients, 13(9), 3297. https://doi.org/10.3390/nu13093297