
Celiac Disease and Thrombotic Events: Systematic Review of Published Cases

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
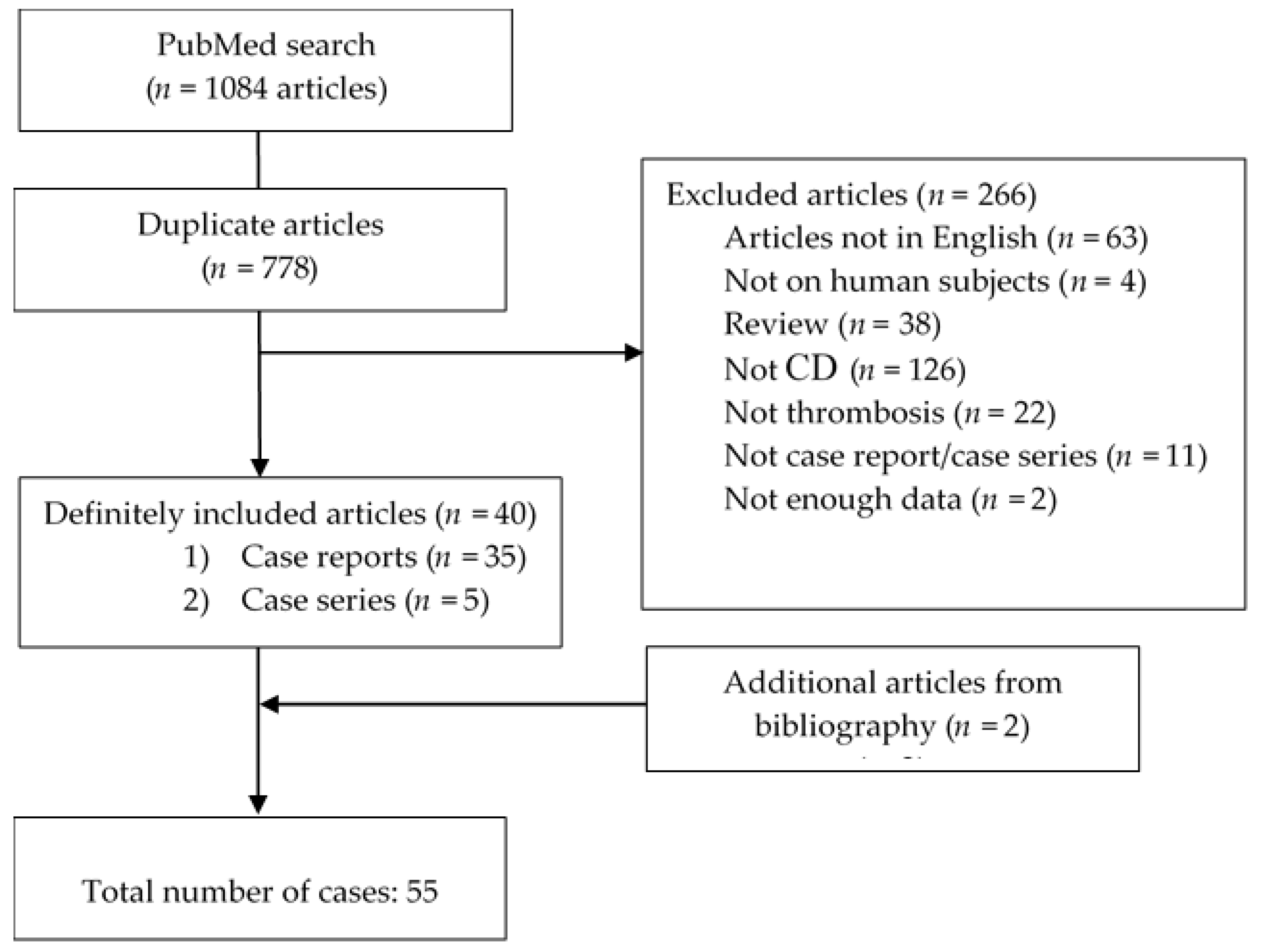
2. Materials and Methods
3. Results
3.1. Demographic Characteristics and Comorbidities
3.2. Clinical Presentation and Laboratory Parameters
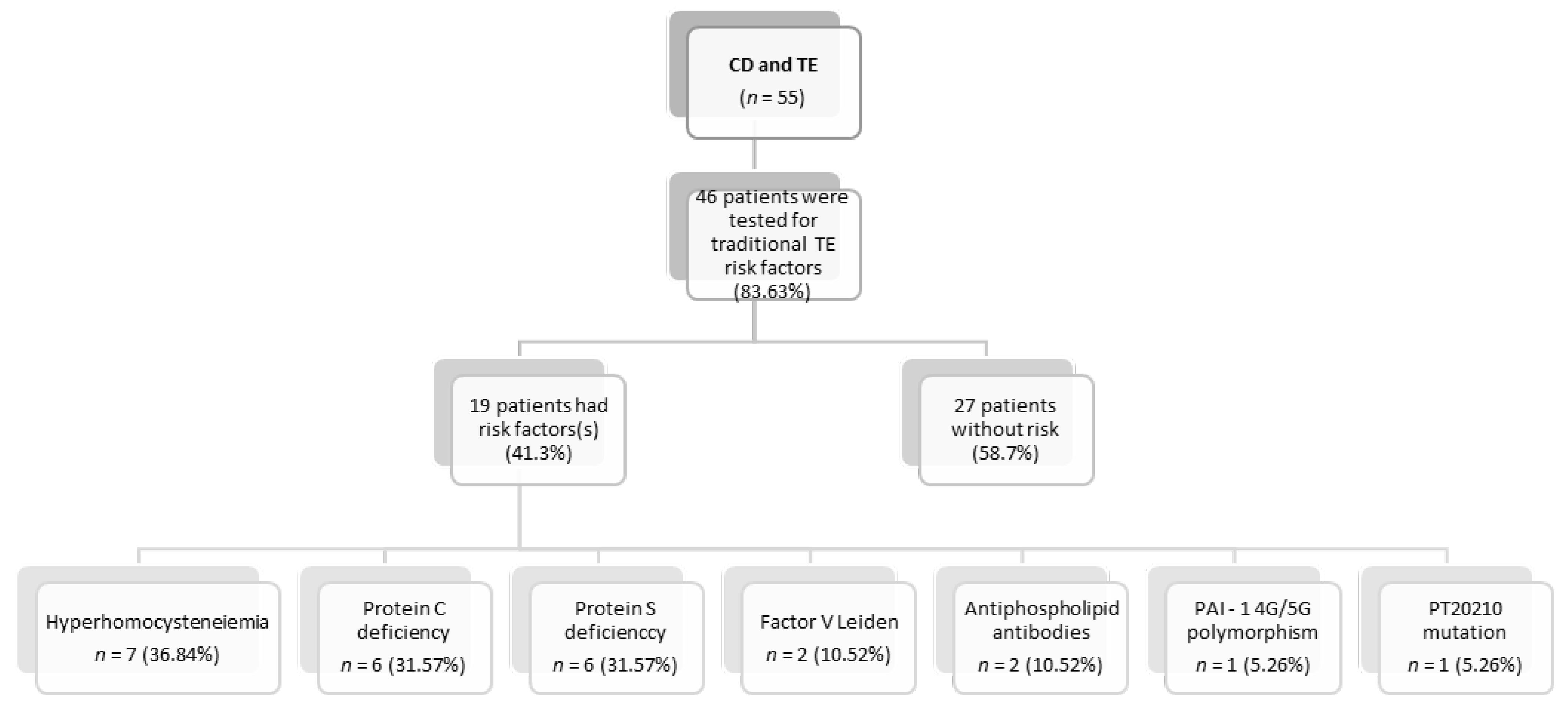
3.3. Risk Factors for Development of Thrombotic Events
3.4. Treatment Modalities and Outcome
4. Discussion
4.1. Epidemiology and Demographic Characteristics
4.2. Clinical Presentation
4.3. Thrombosis and Celiac Disease
4.4. Hypothesis Regarding Pathogenesis of Thrombosis in CD
4.5. Prevention, Treatment, and Outcome
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leffler, D.A.; Green, P.H.; Fasano, A. Extraintestinal manifestations of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Laurikka, P.; Nurminen, S.; Kivelä, L.; Kurppa, K. Extraintestinal Manifestations of Celiac Disease: Early Detection for Better Long-Term Outcomes. Nutrients 2018, 10, 1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durazzo, M.; Ferro, A.; Brascugli, I.; Mattivi, S.; Fagoonee, S.; Pellicano, R. Extra-Intestinal Manifestations of Celiac Disease: What Should We Know in 2022? J. Clin. Med. 2022, 11, 258. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Dastoli, S.; Bennardo, L.; Boccuto, L.; Passante, M.; Silvestri, M.; Proietti, I.; Potenza, C.; Luzza, F.; Nisticò, S.P. The Skin in Celiac Disease Patients: The Other Side of the Coin. Medicina 2019, 55, 578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaban, D.V.; Popp, A.; Ionita Radu, F.; Jinga, M. Hematologic Manifestations in Celiac Disease-A Practical Review. Medicina 2019, 55, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfdanarson, T.R.; Litzow, M.R.; Murray, J.A. Hematologic manifestations of celiac disease. Blood 2007, 109, 412–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baydoun, A.; Maakaron, J.E.; Halawi, H.; Abou Rahal, J.; Taher, A.T. Hematological manifestations of celiac disease. Scand. J. Gastroenterol. 2012, 47, 1401–1411. [Google Scholar] [CrossRef]
- Upadhyay, R.; Park, R.H.; Russell, R.I.; Danesh, B.J.; Lee, F.D. Acute mesenteric ischaemia: A presenting feature of coeliac disease? Br. Med. J. (Clin. Res. Ed.) 1987, 295, 958–959. [Google Scholar] [CrossRef] [Green Version]
- Marteau, P.; Cadranel, J.F.; Messing, B.; Gargot, D.; Valla, D.; Rambaud, J.C. Association of hepatic vein obstruction and coeliac disease in North African subjects. J. Hepatol. 1994, 20, 650–653. [Google Scholar] [CrossRef]
- Dumic, I.; Martin, S.; Salfiti, N.; Watson, R.; Alempijevic, T. Deep Venous Thrombosis and Bilateral Pulmonary Embolism Revealing Silent Celiac Disease: Case Report and Review of the Literature. Case Rep. Gastrointest. Med. 2017, 2017, 5236918. [Google Scholar] [CrossRef]
- Lerner, A.; Blank, M. Hypercoagulability in celiac disease-an update. Autoimmun. Rev. 2014, 13, 1138–1141. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Agmon-Levin, N.; Shapira, Y.; Gilburd, B.; Reuter, S.; Lavi, I.; Shoenfeld, Y. The thrombophilic network of autoantibodies in celiac disease. BMC Med. 2013, 11, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramagopalan, S.V.; Wotton, C.J.; Handel, A.E.; Yeates, D.; Goldacre, M.J. Risk of venous thromboembolism in people admitted to hospital with selected immune-mediated diseases: Record-linkage study. BMC Med. 2011, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zöller, B.; Li, X.; Sundquist, J.; Sundquist, K. Risk of pulmonary embolism in patients with autoimmune disorders: A nationwide follow-up study from Sweden. Lancet 2012, 379, 244–249. [Google Scholar] [CrossRef]
- Johannesdottir, S.A.; Erichsen, R.; Horváth-Puhó, E.; Schmidt, M.; Sørensen, H.T. Coeliac disease and risk of venous thromboembolism: A nationwide population-based case-control study. Br. J. Haematol. 2012, 157, 499–501. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Welander, A.; Lassila, R.; Ekbom, A.; Montgomery, S.M. Risk of thromboembolism in 14,000 individuals with coeliac disease. Br. J. Haematol. 2007, 139, 121–127. [Google Scholar] [CrossRef]
- Ungprasert, P.; Wijarnpreecha, K.; Tanratana, P. Risk of venous thromboembolism in patients with celiac disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 1240–1245. [Google Scholar] [CrossRef]
- Szakács, Z.; Csiszár, B.; Kenyeres, P.; Sarlós, P.; Erőss, B.; Hussain, A.; Nagy, Á.; Kőszegi, B.; Veczák, I.; Farkas, N.; et al. Haemorheological and haemostatic alterations in coeliac disease and inflammatory bowel disease in comparison with non-coeliac, non-IBD subjects (HERMES): A case-control study protocol. BMJ Open 2019, 9, e026315. [Google Scholar] [CrossRef] [Green Version]
- Alhosain, D.; Kouba, L. Concurrent cerebral arterial and venous sinus thrombosis revealing celiac disease—A case report and literature review. BMC Gastroenterol. 2020, 20, 327. [Google Scholar] [CrossRef]
- Hasleton, P.S.; Ironside, J.W.; Whittaker, J.S.; Kelly, W.; Ward, C.; Thompson, G.S. Pulmonary veno-occlusive disease. A report of four cases. Histopathology 1986, 10, 933–944. [Google Scholar] [CrossRef]
- Gnodi, E.; Meneveri, R.; Barisani, D. Celiac disease: From genetics to epigenetics. World J. Gastroenterol. 2022, 28, 449–463. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Sanders, D.S.; Green, P.H.R. Coeliac disease. Lancet 2018, 391, 70–81. [Google Scholar] [CrossRef]
- McAllister, B.P.; Williams, E.; Clarke, K. A Comprehensive Review of Celiac Disease/Gluten-Sensitive Enteropathies. Clin. Rev. Allergy Immunol. 2019, 57, 226–243. [Google Scholar] [CrossRef] [PubMed]
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; de Bruyn, J.; Ronksley, P.E.; Shaheen, A.A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [Green Version]
- Cataldo, F.; Montalto, G. Celiac disease in the developing countries: A new and challenging public health problem. World J. Gastroenterol. 2007, 13, 2153–2159. [Google Scholar] [CrossRef] [Green Version]
- Teresi, S.; Crapisi, M.; Vallejo, M.D.C.; Castellaneta, S.P.; Francavilla, R.; Iacono, G.; Ravelli, A.; Menegazzi, P.; Louali, M.; Catassi, C. Celiac disease seropositivity in Saharawi children: A follow-up and family study. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 506–509. [Google Scholar] [CrossRef]
- Catassi, C.; Ratsch, I.M.; Gandolfi, L.; Pratesi, R.; Fabiani, E.; El Asmar, R.; Frijia, M.; Bearzi, I.; Vizzoni, L. Why is coeliac disease endemic in the people of the Sahara? Lancet 1999, 354, 647–648. [Google Scholar] [CrossRef]
- Lohi, S.; Mustalahti, K.; Kaukinen, K.; Laurila, K.; Collin, P.; Rissanen, H.; Lohi, O.; Bravi, E.; Gasparin, M.; Reunanen, A.; et al. Increasing prevalence of coeliac disease over time. Aliment. Pharmacol. Ther. 2007, 26, 1217–1225. [Google Scholar] [CrossRef]
- Vivas, S.; Vaquero, L.; Rodríguez-Martín, L.; Caminero, A. Age-related differences in celiac disease: Specific characteristics of adult presentation. World J. Gastrointest. Pharmacol. Ther. 2015, 6, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Miehsler, W.; Reinisch, W.; Valic, E.; Osterode, W.; Tillinger, W.; Feichtenschlager, T.; Grisar, J.; Machold, K.; Scholz, S.; Vogelsang, H.; et al. Is inflammatory bowel disease an independent and disease specific risk factor for thromboembolism? Gut 2004, 53, 542–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poddar, B.; Shava, U.; Srivastava, A.; Kapoor, A. Severe heart failure, dilated cardiomyopathy and pulmonary haemosiderosis in coeliac disease: Report of two cases. Paediatr. Int. Child Health 2014, 34, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Afredj, N.; Metatla, S.; Faraoun, S.A.; Nani, A.; Guessab, N.; Benhalima, M.; Bendib, S.E.; Debzi, N.; Layaida, K.; Gamar, L.; et al. Association of Budd-Chiari syndrome and celiac disease. Gastroenterol. Clin. Biol. 2010, 34, 621–624. [Google Scholar] [CrossRef]
- Kochhar, R.; Masoodi, I.; Dutta, U.; Singhal, M.; Miglani, A.; Singh, P.; Singh, K. Celiac disease and Budd Chiari syndrome: Report of a case with review of literature. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1092–1094. [Google Scholar] [CrossRef]
- Grigg, A.P. Deep venous thrombosis as the presenting feature in a patient with coeliac disease and homocysteinaemia. Aust. N. Z. J. Med. 1999, 29, 566–567. [Google Scholar] [CrossRef]
- Gabrielli, M.; Santoliquido, A.; Gasbarrini, G.; Pola, P.; Gasbarrini, A. Latent coeliac disease, hyperhomocysteinemia and pulmonary thromboembolism: A close link? Thromb. Haemost. 2003, 89, 203–204. [Google Scholar] [CrossRef]
- Hallert, C.; Grant, C.; Grehn, S.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef]
- Lai, Y.; Masatoshi, H.; Ma, Y.; Guo, Y.; Zhang, B. Role of Vitamin K in Intestinal Health. Front. Immunol. 2022, 12, 791565. [Google Scholar] [CrossRef]
- Esmon, C.T. The protein C pathway. Chest 2003, 124 (Suppl. 3), 26S–32S. [Google Scholar] [CrossRef] [Green Version]
- Saibeni, S.; Lecchi, A.; Meucci, G.; Cattaneo, M.; Tagliabue, L.; Rondonotti, E.; Formenti, S.; De Franchis, R.; Vecchi, M. Prevalence of hyperhomocysteinemia in adult gluten-sensiti.ive enteropathy at diagnosis: Role of B12, folate, and genetics. Clin. Gastroenterol. Hepatol. 2005, 3, 574–580. [Google Scholar] [CrossRef]
- Kaye, A.D.; Jeha, G.M.; Pham, A.D.; Fuller, M.C.; Lerner, Z.I.; Sibley, G.T.; Cornett, E.M.; Urits, I.; Viswanath, O.; Kevil, C.G. Folic Acid Supplementation in Patients with Elevated Homocysteine Levels. Adv. Ther. 2020, 37, 4149–4164. [Google Scholar] [CrossRef] [PubMed]
- Coppola, A.; Davi, G.; De Stefano, V.; Mancini, F.P.; Cerbone, A.M.; Di Minno, G. Homocysteine, coagulation, platelet function, and thrombosis. Semin. Thromb. Hemost. 2000, 26, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, H.; Khasnis, A. Venous thromboembolism in systemic autoimmune diseases: A narrative review with emphasis on primary systemic vasculitides. Vasc. Med. 2015, 20, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, E.; Scalera, A.; Emmi, G.; Squatrito, D.; Ciucciarelli, L.; Cenci, C.; Tamburini, C.; Emmi, L.; Di Minno, G.; Prisco, D. Thrombosis in Autoimmune Diseases: A Role for Immunosuppressive Treatments? Semin. Thromb. Hemost. 2016, 42, 650–661. [Google Scholar] [PubMed]
- Ciaccio, E.J.; Lewis, S.K.; Biviano, A.B.; Iyer, V.; Garan, H.; Green, P.H. Cardiovascular involvement in celiac disease. World J. Cardiol. 2017, 9, 652–666. [Google Scholar] [CrossRef]
- Leeds, J.S.; Höroldt, B.S.; Sidhu, R.; Hopper, A.D.; Robinson, K.; Toulson, B.; Dixon, L.; Lobo, A.J.; McAlindon, M.E.; Hurlstone, D.P.; et al. Is there an association between coeliac disease and inflammatory bowel diseases? A study of relative prevalence in comparison with population controls. Scand. J. Gastroenterol. 2007, 42, 1214–1220. [Google Scholar] [CrossRef]
- Shah, A.; Walker, M.; Burger, D.; Martin, N.; Von Wulffen, M.; Koloski, N.; Jones, M.; Talley, N.J.; Holtmann, G.J. Link between Celiac Disease and Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2019, 53, 514–522. [Google Scholar] [CrossRef]
- Festen, E.A.; Goyette, P.; Green, T.; Boucher, G.; Beauchamp, C.; Trynka, G.; Dubois, P.C.; Lagace, C.; Stokkers, P.C.; Hommes, D.W.; et al. A meta-analysis of genome-wide association scans identifies IL18RAP, PTPN2, TAGAP, and PUS10 as shared risk loci for Crohn’s disease and celiac disease. PLoS Genet. 2011, 7, e1001283. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, M.C.; Bistritz, L.; Meddings, J.B. Alterations in intestinal permeability. Gut 2006, 55, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Söderholm, J.D.; Olaison, G.; Peterson, K.H.; Franzen, L.E.; Lindmark, T.; Wirén, M.; Tagesson, C.; Sjödahl, R. Augmented increase in tight junction permeability by luminal stimuli in the non-inflamed ileum of Crohn’s disease. Gut 2002, 50, 307–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schürmann, G.; Brüwer, M.; Klotz, A.; Schmid, K.W.; Senninger, N.; Zimmer, K.P. Transepithelial transport processes at the intestinal mucosa in inflammatory bowel disease. Int. J. Colorectal Dis. 1999, 14, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Alkim, H.; Koksal, A.R.; Boga, S.; Sen, I.; Alkim, C. Etiopathogenesis, Prevention, and Treatment of Thromboembolism in Inflammatory Bowel Disease. Clin. Appl. Thromb. Hemost. 2017, 23, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Wajda, A.; Blanchard, J.F. The incidenc.ce of arterial thromboembolic diseases in inflammatory bowel disease: A population-based study. Clin. Gastroenterol. Hepatol. 2008, 6, 41–45. [Google Scholar] [CrossRef]
- Laine, O.; Pitkänen, K.; Lindfors, K.; Huhtala, H.; Niemelä, O.; Collin, P.; Kurppa, K.; Kaukinen, K. Elevated serum antiphospholipid antibodies in adults with celiac disease. Dig. Liver Dis. 2018, 50, 457–461. [Google Scholar] [CrossRef]
- Rokkam, V.R.; Kotagiri, R. Secondary Thrombocytosis. [Updated 1 August 2021]; In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560810/ (accessed on 27 March 2022).
- Maryala, S.; Vaddiparti, A. Reactive Thrombocytosis Related Cerebral Venous Thrombosis: A Rare Complication of Untreated Iron Deficiency Anemia. Cureus 2021, 13, e19064. [Google Scholar] [CrossRef]
- VenugopalanPathiyil, D.; Henry, R.A.; Joseph, J.; Oomen, A.T.; Kakkra, J.J. Severe Iron Deficiency Anemia Leading to Thrombocytosis with Arterial and Venous Thrombosis. Cureus 2021, 13, e17893. [Google Scholar]
- Tang, X.; Zhang, Z.; Fang, M.; Han, Y.; Wang, G.; Wang, S.; Xue, M.; Li, Y.; Zhang, L.; Wu, J.; et al. Transferrin plays a central role in coagulation balance by interacting with clotting factors. Cell Res. 2020, 30, 119–132. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Fang, M.; Cheng, R.; Zhang, Z.; Wang, Y.; Shen, C.; Han, Y.; Lu, Q.; Du, Y.; Liu, Y.; et al. Iron-Deficiency and Estrogen Are Associated with Ischemic Stroke by Up-Regulating Transferrin to Induce Hypercoagulability. Circ. Res. 2020, 127, 651–663. [Google Scholar] [CrossRef]
- Karunakaran, P.; Kochhar, R.; Lal, S.; Nampoothiri, R.V.; Varma, N.; Varma, S.; Malhotra, P. High Prevalence of Celiac Disease in Patients with Immune Thrombocytopenia. Indian J. Hematol. Blood Transfus. 2019, 35, 722–725. [Google Scholar] [CrossRef]
- Swan, D.; Newland, A.; Rodeghiero, F.; Thachil, J. Thrombosis in immune thrombocytopenia–current status and future perspectives. Br. J. Haematol. 2021, 194, 822–834. [Google Scholar] [CrossRef] [PubMed]
- Arca, K.N.; Halker Singh, R.B. Dehydration and Headache. Curr. Pain Headache Rep. 2021, 25, 56. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; West, J.; Card, T.; Appelros, P. Risk of stroke in 28,000 patients with celiac disease: A nationwide cohort study in Sweden. J. Stroke Cerebrovasc. Dis. 2012, 21, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; James, S.; Askling, J.; Stenestrand, U.; Ingelsson, E. Nationwide cohort study of risk of ischemic heart disease in patients with celiac disease. Circulation 2011, 123, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fousekis, F.S.; Beka, E.T.; Mitselos, I.V.; Milionis, H.; Christodoulou, D.K. Thromboembolic complications and cardiovascular events associated with celiac disease. Ir. J. Med. Sci. 2021, 190, 133–141. [Google Scholar] [CrossRef]
- Bouziane, M.; Arous, S.; Habbal, R. Cerebral venous thrombosis as a rare thromboembolic complication of celiac disease: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–5. [Google Scholar] [CrossRef]
- Meena, D.S.; Sonwal, V.S.; Bohra, G.K.; Balesa, J.; Rohila, A.K. Celiac disease with Budd-Chiari syndrome: A rare association. SAGE Open Med. Case Rep. 2019, 7, 2050313X19842697. [Google Scholar] [CrossRef]
- McNeill, A.; Duthie, F.; Galloway, D.J. Small bowel infarction in a patient with coeliac disease. J. Clin. Pathol. 2006, 59, 216–218. [Google Scholar] [CrossRef] [Green Version]
- Thorburn, D.; Stanley, A.J.; Foulis, A.; Campbell Tait, R. Coeliac disease presenting as variceal haemorrhage. Gut 2003, 52, 758. [Google Scholar] [CrossRef]
- Makhdoom, Z.A.; Randall, N.W. Dilated cardiomyopathy due to anticardiolipin syndrome in association with celiac sprue. J. Clin. Gastroenterol. 2000, 31, 91–92. [Google Scholar] [CrossRef]
- Beyrouti, R.; Mansour, M.; Kacem, A.; Derbali, H.; Mrissa, R. Recurrent cerebral venous thrombosis revealing celiac disease: An exceptional case report. Acta Neurol. Belg. 2017, 117, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Florholmen, J.; Waldum, H.; Nordøy, A. Cerebral thrombosis in two patients with malabsorption syndrome treated with vitamin K. Br. Med. J. 1980, 281, 541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebwohl, B.; Green, P.H.R.; Söderling, J.; Roelstraete, B.; Ludvigsson, J.F. Association between Celiac Disease and Mortality Risk in a Swedish Population. JAMA 2020, 323, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Posner, E.B.; Haseeb, M. Celiac Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Holmes, G.K.T.; Muirhead, A. Mortality in coeliac disease: A population-based cohort study from a single centre in Southern Derbyshire, UK. BMJ Open Gastroenterol. 2018, 5, e000201. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Characteristics | |||
|---|---|---|---|
| Gender | Median age (years) | Age range (years) | |
| Female | 34 (61.82%) | 29.5 | 8–59 |
| Male | 21 (38.18%) | 34 | 15–66 |
| Total | 55 (100%) | 32 | 8–66 |
| Geographical distribution | |||
| Africa | 18 (32.73%) | ||
| Asia | 15 (27.27%) | ||
| Australia | 2 (3.64%) | ||
| Europe | 17 (30.91%) | ||
| North America | 3 (5.45%) | ||
| Order of diagnosis | |||
| CD first | 17 (30.91%) | ||
| Thrombosis first | 19 (34.54%) | ||
| At the same time | 19 (34.54%) | ||
| Presenting signs and symptoms | |||
| Abdominal symptoms (distension, pain, diarrhea, vomiting, etc.) | 26/55 (47.27%) | ||
| Neurological symptoms and/or altered vision | 12/55 (21.81%) | ||
| Generalized weakness and fatigue | 9/55 (16.36%) | ||
| Lower extremities swelling | 8/55 (14.54%) | ||
| Weight loss/growth restriction | 6/55 (10.91%) | ||
| Anemia | 4/55 (7.27%) | ||
| Bleeding (hematochezia, hemoptysis) | 2/55 (3.63%) | ||
| Other | 7/55 (12.72%) | ||
| Not reported | 6/55 (10.91%) | ||
| Comorbidities | |||
| Yes | 19 (34.54%) | ||
| No | 36 (65.45%) | ||
| Laboratory parameters | |||
| Anemia | |||
| Yes | 29 (52.72%) | ||
| No | 8 (14.54%) | ||
| Not reported | 18 (32.72%) | ||
| Platelet count | |||
| Increased | 6 (10.91%) | ||
| Decreased | 4 (7.27%) | ||
| Within normal range | 19 (34.54%) | ||
| Not reported | 26 (47.27%) | ||
| Thrombosis risk factors | |||
| Inflammation | 7/55 (12.72%) | ||
| Oral contraceptives | 5/55 (9.09%) | ||
| Immobilization | 3/55 (5.45%) | ||
| Dehydration | 3/55 (5.45%) | ||
| Malignancy | 3/55 (5.45%) | ||
| Pregnancy | 2/55 (3.63%) | ||
| Surgery | 2/55 (3.63%) | ||
| No risk factors | 12/55 (21.81%) | ||
| Not reported | 24/55 (43.63%) | ||
| Thrombophilia | |||
| Yes | 19 (34.54%) | ||
| Hyperhomocysteinemia | 7/19 (36.84%) | ||
| Protein S deficiency | 6/19 (31.57%) | ||
| Protein C deficiency | 6/19 (31.57%) | ||
| Antiphospholipid antibodies | 2/19 (10.52%) | ||
| APCR | 1/19 (5.26%) | ||
| Factor V Leiden | 2/19 (10.52%) | ||
| PAI–1 4G/5G polymorphism | 1/19 (5.26%) | ||
| PT20210 mutation | 1/19 (5.26%) | ||
| No | 27 (49.09%) | ||
| Not specified | 9 (16.36%) | ||
| Type of Thrombosis | |
|---|---|
| Venous | 44 (80%) |
| Arterial | 9 (16.36%) |
| Both | 2 (3.64%) |
| Number of sites involved | |
| 1 | 43 (78.18%) |
| 2 | 10 (18.18%) |
| 3 or more | 2 (3.64%) |
| Site of thrombosis | |
| Hepatic veins | 17/55 (30.91%) |
| Deep venous thrombosis of lower extremities | 10/55 (18.18%) |
| Cerebral blood vessels | 10/55 (18.18%) |
| Pulmonary thromboembolism | 9/55 (16.36%) |
| Portal system vessels | 8/55 (14.54%) |
| Central retinal vein | 4/55 (7.27%) |
| Abdominal arteries | 3/55 (5.45%) |
| Other | 5/55 (9.09%) |
| Therapy | |
| Yes | 38 (69.09%) |
| Vitamin K antagonists | 19/38 (50%) |
| Heparin/LMWH | 15/38 (39.47%) |
| Antiplatelet medications | 5/38 (13.15%) |
| Direct-acting anticoagulants | 1/38 (2.63%) |
| Oral anticoagulants (not specified) | 8/38 (21.05%) |
| No | 17 (30.91%) |
| Outcome | |
| Recovered | 29 (52.72%) |
| Partially recovered | 14 (25.45%) |
| Death | 8 (14.54%) |
| Thrombosis extension | 2 (3.64%) |
| Unknown | 2 (3.64%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantic, N.; Pantic, I.; Jevtic, D.; Mogulla, V.; Oluic, S.; Durdevic, M.; Nordin, T.; Jecmenica, M.; Milovanovic, T.; Gavrancic, T.; et al. Celiac Disease and Thrombotic Events: Systematic Review of Published Cases. Nutrients 2022, 14, 2162. https://doi.org/10.3390/nu14102162
Pantic N, Pantic I, Jevtic D, Mogulla V, Oluic S, Durdevic M, Nordin T, Jecmenica M, Milovanovic T, Gavrancic T, et al. Celiac Disease and Thrombotic Events: Systematic Review of Published Cases. Nutrients. 2022; 14(10):2162. https://doi.org/10.3390/nu14102162
Chicago/Turabian StylePantic, Nikola, Ivana Pantic, Dorde Jevtic, Vanajakshi Mogulla, Stevan Oluic, Momcilo Durdevic, Terri Nordin, Mladen Jecmenica, Tamara Milovanovic, Tatjana Gavrancic, and et al. 2022. "Celiac Disease and Thrombotic Events: Systematic Review of Published Cases" Nutrients 14, no. 10: 2162. https://doi.org/10.3390/nu14102162
APA StylePantic, N., Pantic, I., Jevtic, D., Mogulla, V., Oluic, S., Durdevic, M., Nordin, T., Jecmenica, M., Milovanovic, T., Gavrancic, T., & Dumic, I. (2022). Celiac Disease and Thrombotic Events: Systematic Review of Published Cases. Nutrients, 14(10), 2162. https://doi.org/10.3390/nu14102162