
Racial/Ethnic Disparities in Food Pantry Use and Barriers in Massachusetts during the First Year of the COVID-19 Pandemic

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
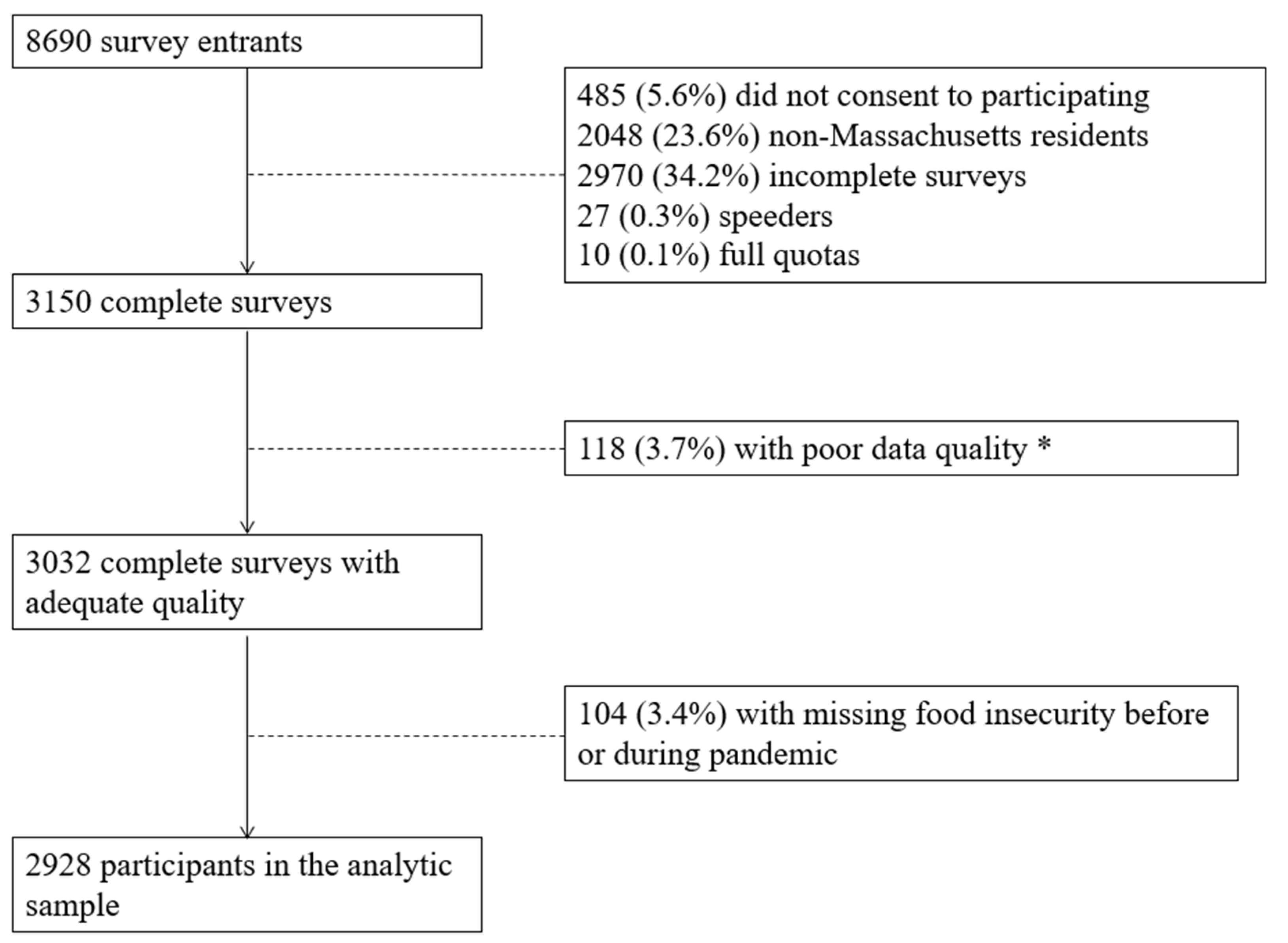
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Food Insecurity
3.2. Food Pantry Use
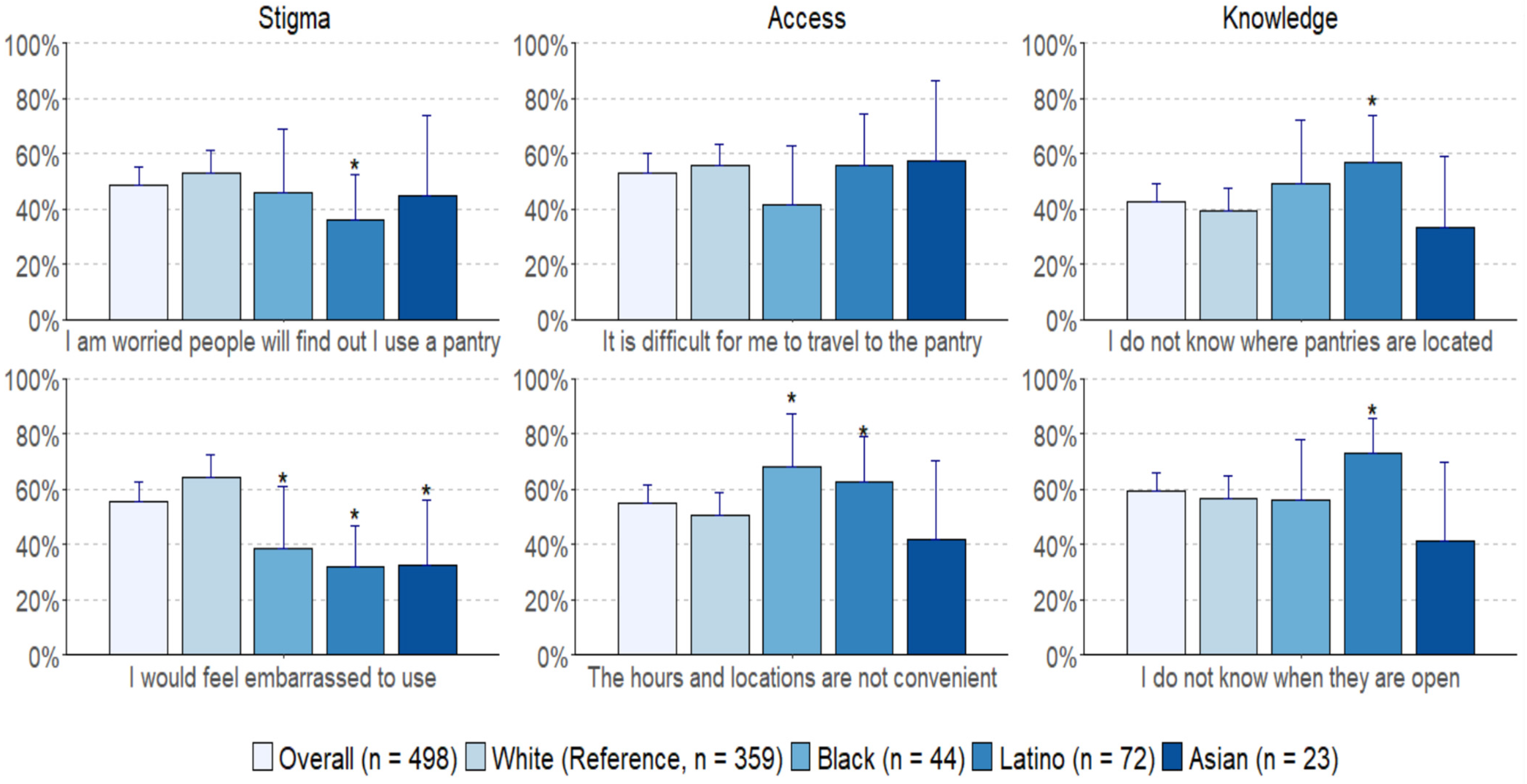
3.3. Barriers to Food Pantries
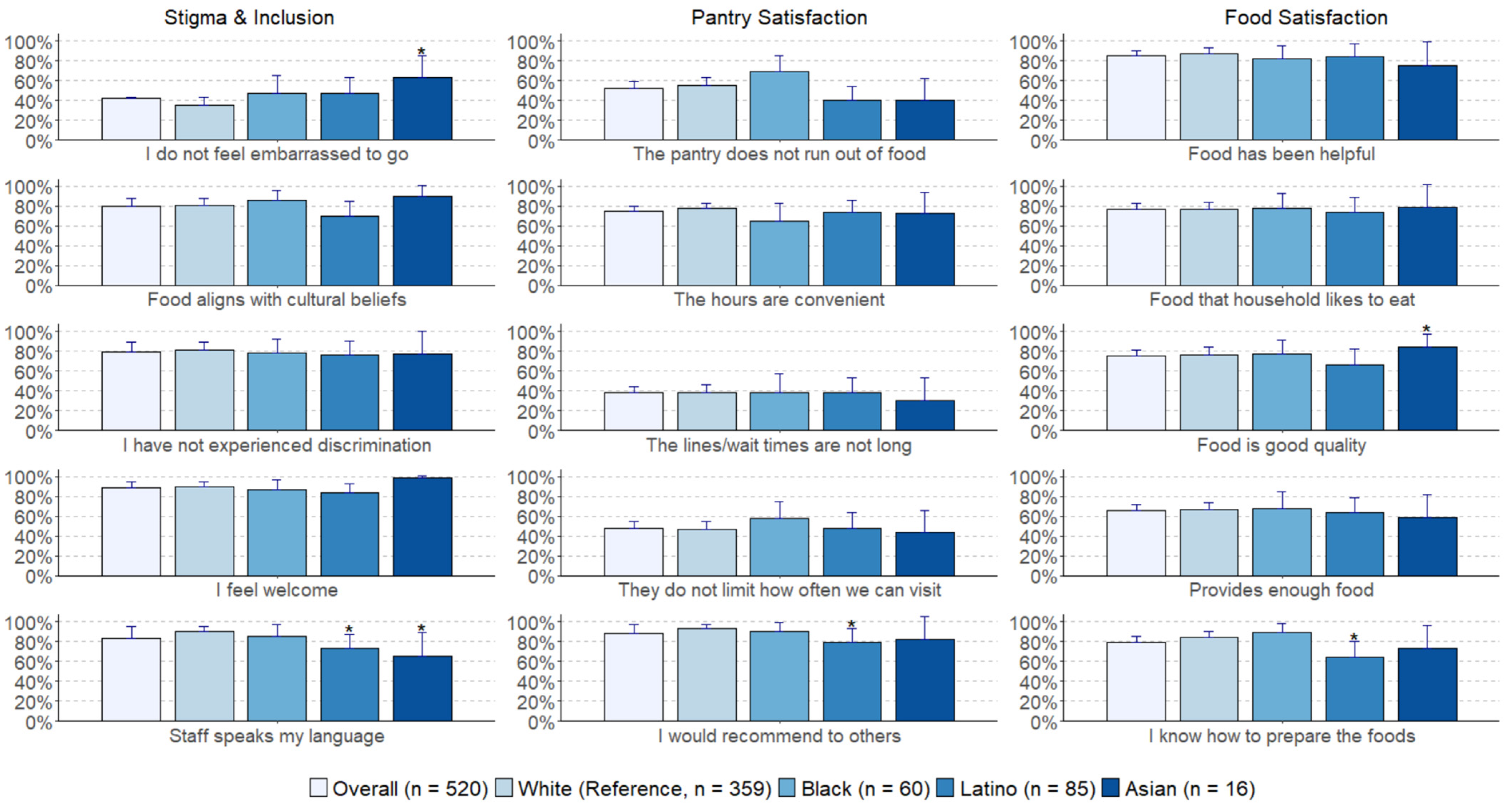
3.4. Experiences with Food Pantries
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A




{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Unweighted % | Weighted % | Massachusetts (ACS) % |
|---|---|---|---|---|
| Gender | Female | 68.8 | 52.3 | 52.1 |
| Male | 31.2 | 47.7 | 47.9 | |
| Age group, years | 18–34 | 40.3 | 29.8 | 30.5 |
| 35–54 | 34.9 | 32.4 | 32.4 | |
| 55–64 | 13.3 | 17.3 | 16.9 | |
| 65+ | 11.4 | 20.5 | 20.2 | |
| Race/ethnicity | Non-Latino White | 74.6 | 74.9 | 74.2 |
| Non-Latino Black | 6.8 | 6.5 | 6.6 | |
| Non-Latino Asian | 5.1 | 6.4 | 6.6 | |
| Latino | 10.0 | 9.9 | 10.2 | |
| Other or Multiracial | 3.5 | 2.4 | 2.4 | |
| Educational attainment | High school or less | 3.5 | 8.7 | 9.3 |
| High school graduate (including GED) | 22.2 | 24.3 | 24.6 | |
| Some college (no degree) | 21.5 | 18.8 | 18.7 | |
| Associate degree/technical school/apprenticeship | 11.3 | 7.2 | 7.1 | |
| Bachelor’s degree | 26.2 | 23.5 | 23.1 | |
| Graduate degree | 15.3 | 17.6 | 17.3 | |
| Household income | <$10,000 | 8.6 | 3.2 | 3.6 |
| $10,000 to $24,999 | 15.1 | 7.8 | 7.9 | |
| $25,000 to $49,999 | 25.4 | 13.8 | 14.0 | |
| $50,000 to $74,999 | 17.8 | 14.0 | 13.9 | |
| $75,000 to $99,999 | 12.0 | 12.9 | 12.7 | |
| $100,000 to $149,999 | 13.6 | 21.1 | 20.7 | |
| $150,000 to $199,999 | 4.4 | 12.1 | 11.7 | |
| ≥$200,000 | 3.0 | 15.2 | 15.4 | |
| Region | Western (Berkshire, Franklin, Hampshire, Hampden) | 14.9 | 12.3 | 12.2 |
| Central (Worcester) | 14.3 | 11.9 | 11.9 | |
| Boston (Suffolk, Norfolk) | 20.9 | 22.2 | 22.2 | |
| Northeast (Essex, Middlesex) | 31.2 | 34.6 | 34.6 | |
| Southeast (Bristol, Plymouth, Barnstable, Dukes, Nantucket) | 18.6 | 19.1 | 19.2 | |
| Children in household | Yes | 37.2 | 37.5 | 31.9 |
References
- Feeding America. Map the Meal Gap. Available online: https://map.feedingamerica.org/ (accessed on 5 May 2022).
- USDA. Definitions of Food Security. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security.aspx (accessed on 18 January 2022).
- Coleman-Jensen, A.; Rabbit, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2020. USDA, 2021. Available online: https://www.ers.usda.gov/webdocs/publications/102076/err-298.pdf?v=1482.7 (accessed on 18 January 2022).
- Waxman, E.; Gupta, P.; Gonzalez, D. Charitable Food Use Increased Nearly 50 Percent from 2019 to 2020; Urban Institute: Washington, DC, USA, 2021; Available online: https://www.urban.org/sites/default/files/publication/103825/charitable-food-use-increased-nearly-50-percent-from-2019-to-2020_0.pdf (accessed on 18 January 2022).
- Feeding America. The Feeding America Network. Available online: https://www.feedingamerica.org/our-work/food-bank-network (accessed on 5 May 2022).
- Zack, R.M.; Weil, R.; Babbin, M.; Lynn, C.D.; Velez, D.S.; Travis, L.; Taitelbaum, D.J.; Fiechtner, L. An Overburdened Charitable Food System: Making the Case for Increased Government Support During the COVID-19 Crisis. Am. J. Public Health 2021, 111, 804–807. [Google Scholar] [CrossRef] [PubMed]
- USDA. USDA to Invest $1 Billion to Purchase Healthy Food for Food Insecure Americans and Build Food Bank Capacity. Available online: https://www.usda.gov/media/press-releases/2021/06/04/usda-invest-1-billion-purchase-healthy-food-food-insecure-americans (accessed on 4 March 2022).
- USDA. USDA Increases SNAP Benefits 15% with Funding from American Rescue Plan. Available online: https://www.usda.gov/media/press-releases/2021/03/22/usda-increases-snap-benefits-15-funding-american-rescue-plan (accessed on 4 March 2022).
- Mabli, J.; Ohls, J. Supplemental Nutrition Assistance Program Participation Is Associated with an Increase in Household Food Security in a National Evaluation. J. Nutr. 2015, 145, 344–351. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Wang, J.; Liu, J.; Shen, J.; Loehmer, E.; McCaffrey, J. A systematic review of food pantry-based interventions in the USA. Public Health Nutr. 2019, 22, 1704–1716. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Shore-Sheppard, L.; Watson, T. The Effect of Safety-Net Programs on Food Insecurity. J. Hum. Resour. 2016, 51, 589–614. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Leung, C.W. Food Insecurity and COVID-19, Disparities in Early Effects for US Adults. Nutrients 2020, 12, 1648. [Google Scholar] [CrossRef]
- Lauren, B.N.; Silver, E.R.; Faye, A.S.; Rogers, A.M.; Woo-Baidal, J.A.; Ozanne, E.M.; Hur, C. Predictors of households at risk for food insecurity in the United States during the COVID-19 pandemic. Public Health Nutr. 2021, 3929–3936. [Google Scholar] [CrossRef]
- Flores-Lagunes, A.; Jales, H.B.; Liu, J.; Wilson, N.L. The Differential Incidence and Severity of Food Insecurity by Racial, Ethnic, and Immigrant Groups over the Great Recession in the United States. AEA Pap. Proc. 2018, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Vahabi, M.; Damba, C. Perceived Barriers in Accessing Food among Recent Latin American Immigrants in Toronto. Int. J. Equity Health. 2013, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Wilson, N.L.; Calancie, L.; Adkins, J.; Folta, S.C. Understanding Micro-pantries as an Emergency Food Source during the COVID-19 Pandemic. J. Nutr. Educ. Behav. 2022, 299–310. [Google Scholar] [CrossRef]
- Larson, N.; Alexander, T.; Slaughter-Acey, J.C.; Berge, J.; Widome, R.; Neumark-Sztainer, D. Barriers to Accessing Healthy Food and Food Assistance during the COVID-19 Pandemic and Racial Justice Uprisings: A Mixed-Methods Investigation of Emerging Adults’ Experiences. J. Acad. Nutr. Diet. 2021, 121, 1679–1694. [Google Scholar] [CrossRef] [PubMed]
- Oliver, T.L.; McKeever, A.; Shenkman, R.; Diewald, L. Barriers to Healthy Eating in a Community That Relies on an Emergency Food Pantry. J. Nutr. Educ. Behav. 2020, 52, 299–306. [Google Scholar] [CrossRef] [PubMed]
- El Zein, A.; Mathews, A.E.; House, L.; Shelnutt, K.P. Why Are Hungry College Students Not Seeking Help? Predictors of and Barriers to Using an On-Campus Food Pantry. Nutrients 2018, 10, 1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, C.B.; Byrne, A.T.; Whitaker, T. But It Came from a Food Pantry: Product Stigma and Quality Perceptions of Food Pantry Offerings. 2021. Available online: https://ssrn.com/abstract=3950670 (accessed on 5 May 2022).
- Kindle, P.; Foust-Newton, M.; Reis, M.; Gell, M. Food Pantries and Stigma: Users’ Concerns and Public Support. Contemp. Rural Soc. Work. J. 2020, 11, 2. [Google Scholar]
- Niles, M.T.; Neff, R.; Biehl, E.; Bertmann, F.; Belarmino, E.H.; Acciai, F.; Ohri-Vachaspati, P. Food Access and Food Security during COVID-19 Survey–Version 2.1; Harvard Dataverse: Cambridge, MA, USA, 2020. [Google Scholar] [CrossRef]
- Miller, C.A.; Guidry, J.P.D.; Dahman, B.; Thomson, M.D. A Tale of Two Diverse Qualtrics Samples: Information for Online Survey Researchers. Cancer Epidemiol. Biomark. Prev. 2020, 29, 731–735. [Google Scholar] [CrossRef] [Green Version]
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 18 January 2022).
- USDA ERS. U.S. Household Food Security Survey Module: Six-Item Short Form 2012. Available online: https://www.ers.usda.gov/media/8282/short2012.pdf (accessed on 15 February 2022).
- Explore Census Data. Available online: https://data.census.gov/cedsci/ (accessed on 18 January 2022).
- Massachusetts Department of Public Health. COVID-19 Community Impact Survey. Available online: https://www.mass.gov/doc/covid-19-community-impact-survey-ccis-preliminary-analysis-results-full-report/download (accessed on 15 February 2022).
- Niles, M.T.; Beavers, A.W.; A Clay, L.; Dougan, M.M.; A Pignotti, G.; Rogus, S.; Savoie-Roskos, M.R.; E Schattman, R.; Zack, R.M.; Acciai, F.; et al. A Multi-Site Analysis of the Prevalence of Food Insecurity in the United States, before and during the COVID-19 Pandemic. Curr. Dev. Nutr. 2021, 5, nzab135. [Google Scholar] [CrossRef]
- Morales, D.X.; Morales, S.A.; Beltran, T.F. Racial/Ethnic Disparities in Household Food Insecurity during the COVID-19 Pandemic: A Nationally Representative Study. J. Racial Ethn. Health Disparities 2020, 8, 1300–1314. [Google Scholar] [CrossRef]
- Conrad, F.G.; Schober, M.F.; Antoun, C.; Yan, Y.; Hupp, A.L.; Johnston, M.; Ehlen, P.; Vickers, L.; Zhang, C. Respondent mode choice in a smartphone survey. Public Opin. Q. 2017, 81, 307–337. [Google Scholar] [CrossRef] [Green Version]
- Coleman-Jensen, A.; Rabbit, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2016. 2017. Available online: https://www.ers.usda.gov/webdocs/publications/84973/err-237.pdf (accessed on 15 February 2022).
- Odoms-Young, A.M. Examining the Impact of Structural Racism on Food Insecurity: Implications for Addressing Racial/Ethnic Disparities. Fam. Community Health 2018, 41, S3–S6. [Google Scholar] [CrossRef]
- Tan, S.B.; deSouza, P.; Raifman, M. Structural Racism and COVID-19 in the USA: A County-Level Empirical Analysis. J. Racial Ethn. Health Disparities 2022, 9, 236–246. [Google Scholar] [CrossRef]
- Raskind, I.G. Hunger Does Discriminate: Addressing Structural Racism and Economic Inequality in Food Insecurity Research. Am. J. Public Health 2020, 110, 1264–1265. [Google Scholar] [CrossRef] [PubMed]
- Burke, M.P.; Jones, S.J.; Frongillo, E.A.; Fram, M.S.; Blake, C.E.; Freedman, D.A. Severity of household food insecurity and lifetime racial discrimination among African-American households in South Carolina. Ethn. Health. 2018, 23, 276–292. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.; Wright, R.A.; Wimer, C. The Cost of Free Assistance: Why Low-Income Individuals Do Not Access Food Pantries. J. Sociol Soc. Welf. 2016, 43, 71–96. [Google Scholar]
- Pak, T.Y. Welfare stigma as a risk factor for major depressive disorder: Evidence from the Supplemental Nutrition Assistance Program. J. Affect. Disord. 2020, 260, 53–60. [Google Scholar] [CrossRef]
- U.S. Census Bureau QuickFacts: Massachusetts. Available online: https://www.census.gov/quickfacts/MA (accessed on 18 January 2022).
- Pew Research Center. Internet/Broadband Fact Sheet. Available online: https://www.pewresearch.org/internet/fact-sheet/internet-broadband/ (accessed on 12 April 2022).
- Berkowitz, S.A.; Seligman, H.K.; Meigs, J.B.; Basu, S. Food Insecurity, Healthcare Utilization, and High Cost: A Longitudinal Cohort Study. Am. J. Manag. Care. 2018, 24, 399–404. [Google Scholar]
- Gundersen, C.; Ziliak, J.P. Food Insecurity And Health Outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [Green Version]
- Heflin, C.M.; Siefert, K.; Williams, D.R. Food insufficiency and women’s mental health: Findings from a 3-year panel of welfare recipients. Soc. Sci. Med. 2005, 61, 1971–1982. [Google Scholar] [CrossRef]
- Raifman, J.; Bor, J.; Venkataramani, A. Association Between Receipt of Unemployment Insurance and Food Insecurity Among People Who Lost Employment During the COVID-19 Pandemic in the United States. JAMA Netw. Open 2021, 4, e2035884. [Google Scholar] [CrossRef]
- Idzerda, L.; Gariépy, G.; Corrin, T.; Tarasuk, V.; McIntyre, L.; Neil-Sztramko, S.; Dobbins, M.; Garcia, A.J. What is known about the prevalence of household food insecurity in Canada during the COVID-19 pandemic: A systematic review. Health Promot. Chronic Dis. Prev. Can. 2022, 42, 177–187. [Google Scholar] [CrossRef]
- Emery, J.; Fleisch, V.; McIntyre, L. How a Guaranteed Annual Income Could Put Food Banks Out of Business. SPP Res. Pap. 2013, 6, 20. Available online: http://www.niagaraknowledgeexchange.com/wp-content/uploads/sites/2/2014/05/How_a_Guaranteed_Income_Could_Put_Food_Banks_Out_of_Business (accessed on 5 May 2022).
| Food Insecurity 1 | Race/Ethnicity | n 2 | Before Pandemic 3 | First Year of Pandemic 4 | Absolute Difference | ||
|---|---|---|---|---|---|---|---|
| Prevalence (95% CI) | p-Value | Prevalence (95% CI) | p-Value | ||||
| Overall | Overall | 2826 | 19% (17–21%) | 30% (27%–32%) | 11% | ||
| White | 2184 | 15% (13–17%) | Ref | 24% (22%–27%) | Ref | 9% | |
| Black | 200 | 31% (22–40%) | <0.001 | 45% (35%–55%) | <0.001 | 14% | |
| Latino | 292 | 44% (35–53%) | <0.001 | 58% (49%–67%) | <0.001 | 14% | |
| Asian | 150 | 16% (8–23%) | 0.823 | 26% (17%–36%) | 0.660 | 11% | |
| Adults with children in the household | Overall | 1052 | 27% (23–31%) | 42% (38%–47%) | 15% | ||
| White | 717 | 21% (17–25%) | Ref | 36% (31%–42%) | Ref | 15% | |
| Black | 113 | 36% (23–48%) | 0.244 | 46% (32%–60%) | 0.343 | 10% | |
| Latino | 171 | 47% (36–59%) | <0.001 | 64% (53%–75%) | 0.015 | 16% | |
| Asian | 51 | 19% (7–31%) | 0.834 | 30% (15%–45%) | 0.882 | 11% | |
| Adults without children in the household | Overall | 1774 | 14% (12–17%) | 22% (20%–25%) | 8% | ||
| White | 1467 | 12% (10–14%) | Ref | 19% (16%–22%) | Ref | 7% | |
| Black | 87 | 24% (12–36%) | <0.001 | 43% (28%–58%) | <0.001 | 19% | |
| Latino | 121 | 37% (25–50%) | <0.001 | 48% (34%–61%) | <0.001 | 10% | |
| Asian | 99 | 13% (3–23%) | 0.915 | 24% (12%–36%) | 0.733 | 11% | |
| Food Pantry Use | Race/Ethnicity | Before Pandemic 2 | First Year of Pandemic 3 | Absolute Difference | ||||
|---|---|---|---|---|---|---|---|---|
| n 1 | Prevalence (95% CI) | p-Value | n 1 | Prevalence (95% CI) | p-Value | |||
| Overall | Overall | 2826 | 9% (7–10%) | 2826 | 12% (11%–14%) | 4% | ||
| White | 2184 | 6% (5–7%) | Ref | 2184 | 9% (7%–10%) | Ref | 3% | |
| Black | 200 | 20% (13–28%) | <0.001 | 200 | 26% (17%–34%) | <0.001 | 5% | |
| Latino | 292 | 21% (14–28%) | <0.001 | 292 | 28% (20%–35%) | <0.001 | 7% | |
| Asian | 150 | 6% (2–11%) | 0.800 | 150 | 9% (3%–15%) | 0.946 | 2% | |
| Adults with food insecurity | Overall | 825 | 27% (22–32%) | 1188 | 32% (28%–36%) | 5% | ||
| White | 570 | 24% (18–29%) | Ref | 845 | 29% (24%–34%) | Ref | 5% | |
| Black | 82 | 32% (18–46%) | 0.252 | 105 | 40% (26%–54%) | 0.123 | 8% | |
| Latino | 142 | 32% (20–43%) | 0.186 | 186 | 41% (30%–52%) | 0.042 | 9% | |
| Asian | 31 | 24% (1–47%) | 0.962 | 52 | 25% (7%–43%) | 0.696 | 1% | |
| Domain | Statement | Race 1 | % Agree 2 | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Knowledge | I do not know where the pantries are located | Overall | 42% | ||||
| White | 39% | Ref | Ref | ||||
| Black | 50% | 1.55 (0.55–4.35) | 0.402 | 1.77 (0.64–3.84) | 0.274 | ||
| Latino | 56% | 2.31 (1.06–5.07) | 0.036 | 2.98 (1.25–7.10) | 0.014 | ||
| Asian | 33% | 0.80 (0.24–2.62) | 0.708 | 0.76 (0.24–2.35) | 0.629 | ||
| I do not know when they are open | Overall | 59% | |||||
| White | 57% | Ref | Ref | ||||
| Black | 63% | 1.43 (0.54–3.75) | 0.469 | 1.40 (0.52–3.81) | 0.507 | ||
| Latino | 74% | 2.24 (1.07–4.68) | 0.032 | 2.82 (1.23–6.45) | 0.014 | ||
| Asian | 42% | 0.62 (0.18–2.08) | 0.436 | 0.59 (0.19–1.81) | 0.354 | ||
| Access | The hours and locations are not convenient | Overall | 55% | ||||
| White | 51% | Ref | Ref | ||||
| Black | 76% | 3.67 (1.40–9.62) | 0.008 | 4.73 (1.68–13.30) | 0.003 | ||
| Latino | 62% | 2.17 (1.00–4.70) | 0.051 | 3.61 (1.53–8.50) | 0.003 | ||
| Asian | 42% | 0.80 (0.24–2.69) | 0.716 | 0.90 (0.32–2.56) | 0.848 | ||
| It is difficult for me to travel to the pantry | Overall | 53% | |||||
| White | 56% | Ref | Ref | ||||
| Black | 34% | 0.44 (0.17–1.10) | 0.078 | 0.50 (0.22–1.18) | 0.113 | ||
| Latino | 55% | 0.91 (0.39–2.10) | 0.826 | 0.84 (0.37–1.93) | 0.687 | ||
| Asian | 57% | 1.10 (0.32–3.72) | 0.880 | 1.26 (0.35–4.54) | 0.720 | ||
| Stigma | I am worried people will find out I use the pantry | Overall | 48% | ||||
| White | 53% | Ref | Ref | ||||
| Black | 40% | 0.62 (0.22–1.70) | 0.349 | 0.42 (0.14–1.27) | 0.124 | ||
| Latino | 36% | 0.47 (0.21–1.03) | 0.058 | 0.49 (0.21–1.11) | 0.086 | ||
| Asian | 45 | 0.78 (0.23–2.62) | 0.683 | 0.58 (0.18–1.51) | 0.233 | ||
| I would feel embarrassed to use | Overall | 56% | |||||
| White | 65% | Ref | Ref | ||||
| Black | 37% | 0.34 (0.12–0.96) | 0.041 | 0.27 (0.10–0.76) | 0.013 | ||
| Latino | 32% | 0.23 (0.11–0.48) | <0.001 | 0.28 (0.13–0.64) | 0.002 | ||
| Asian | 33% | 0.27 (0.09–0.84) | 0.024 | 0.23 (0.08–0.63) | 0.004 |
| Domain | Statement | Race 1 | % Agree 2 | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Stigma and Inclusion | Food aligns with cultural beliefs | Overall | 80% | ||||
| White | 81% | Ref | Ref | ||||
| Black | 85% | 1.35 (0.52–3.51) | 0.531 | 1.83 (0.67–5.00) | 0.241 | ||
| Latino | 69% | 0.53 (0.23–1.25) | 0.145 | 0.78 (0.32–1.91) | 0.592 | ||
| Asian | 89% | 2.34 (0.31–17.80) | 0.410 | 1.95 (0.30–12.90) | 0.488 | ||
| Staff speaks my language | Overall | 84% | |||||
| White | 90% | Ref | Ref | ||||
| Black | 85% | 0.63 (0.20–1.94) | 0.417 | 0.58 (0.20–1.71) | 0.323 | ||
| Latino | 73% | 0.30 (0.12–0.76) | 0.011 | 0.21 (0.08–0.57) | 0.002 | ||
| Asian | 65% | 0.08 (0.02–0.36) | 0.001 | 0.09 (0.02–0.57) | 0.010 | ||
| I have not experienced discrimination | Overall | 79% | |||||
| White | 81% | Ref | Ref | ||||
| Black | 78% | 0.82 (0.32–2.10) | 0.678 | 0.94 (0.30–2.95) | 0.920 | ||
| Latino | 76% | 0.73 (0.30–1.79) | 0.488 | 0.69 (0.29–1.65) | 0.405 | ||
| Asian | 77% | 0.35 (0.07–1.74) | 0.200 | 0.48 (0.10–2.31) | 0.358 | ||
| I don’t feel embarrassed to go | Overall | 42% | |||||
| White | 36% | Ref | Ref | ||||
| Black | 47% | 1.61 (0.74–3.53) | 0.232 | 1.50 (0.63–3.56) | 0.356 | ||
| Latino | 47% | 1.62 (0.81–3.27) | 0.175 | 1.70 (0.88–3.30) | 0.114 | ||
| Asian | 63% | 3.41 (0.72–16.10) | 0.121 | 4.00 (0.78–20.50) | 0.096 | ||
| I feel welcome | Overall | 89% | |||||
| White | 90% | Ref | Ref | ||||
| Black | 87% | 0.76 (0.27–2.10) | 0.590 | 1.27 (0.46–3.56) | 0.645 | ||
| Latino | 84% | 0.60 (0.26–1.39) | 0.230 | 0.88 (0.28–2.81) | 0.834 | ||
| Asian | 99% | 7.34 (0.85–63.30) | 0.070 | 22.50 (2.15–236.00) | 0.009 | ||
| Pantry Satisfaction | The pantry does not run out of food | Overall | 52% | ||||
| White | 55% | Ref | Ref | ||||
| Black | 69% | 1.85 (0.82–4.17) | 0.139 | 1.73 (0.70–4.28) | 0.232 | ||
| Latino | 40% | 0.55 (0.27–1.09) | 0.086 | 0.51 (0.25–1.04) | 0.066 | ||
| Asian | 41% | 0.31 (0.08–1.14) | 0.078 | 0.34 (0.09–1.29) | 0.112 | ||
| The hours are convenient | Overall | 74% | |||||
| White | 77% | Ref | Ref | ||||
| Black | 65% | 0.54 (0.23–1.27) | 0.156 | 0.61 (0.25–1.52) | 0.290 | ||
| Latino | 74% | 0.83 (0.41–1.69) | 0.605 | 0.86 (0.41–1.79) | 0.680 | ||
| Asian | 72% | 0.87 (0.15–5.09) | 0.878 | 1.76 (0.29–10.70) | 0.536 | ||
| The lines/wait times are not long | Overall | 38% | |||||
| White | 39% | Ref | Ref | ||||
| Black | 39% | 1.00 (0.44–2.27) | 0.999 | 1.00 (0.45–2.21) | 0.996 | ||
| Latino | 38% | 0.97 (0.48–1.98) | 0.937 | 0.79 (0.38–1.64) | 0.528 | ||
| Asian | 31% | 0.85 (0.16–4.37) | 0.841 | 1.13 (0.18–7.33) | 0.897 | ||
| They don’t limit how often we can visit | Overall | 48% | |||||
| White | 47% | Ref | Ref | ||||
| Black | 58% | 1.56 (0.71–3.40) | 0.268 | 1.33 (0.58–3.05) | 0.503 | ||
| Latino | 48% | 1.05 (0.52–2.13) | 0.894 | 0.72 (0.35–1.49) | 0.380 | ||
| Asian | 43% | 0.56 (0.14–2.20) | 0.401 | 0.86 (0.21–3.50) | 0.829 | ||
| I would recommend to others | Overall | 89% | |||||
| White | 93% | Ref | Ref | ||||
| Black | 91% | 0.71 (0.21–2.44) | 0.582 | 1.07 (0.25–4.60) | 0.923 | ||
| Latino | 79% | 0.28 (0.09–0.81) | 0.020 | 0.29 (0.10–0.88) | 0.029 | ||
| Asian | 82% | 0.23 (0.03–1.89) | 0.171 | 0.41 (0.05–3.36) | 0.406 | ||
| Food Satisfaction | Food has been helpful | Overall | 85% | ||||
| White | 87% | Ref | Ref | ||||
| Black | 82% | 0.69 (0.26–1.86) | 0.467 | 1.05 (0.34–3.25) | 0.928 | ||
| Latino | 84% | 0.80 (0.28–2.34) | 0.688 | 1.87 (0.57–6.14) | 0.299 | ||
| Asian | 75% | 0.46 (0.06–3.40) | 0.444 | 0.52 (0.06–4.73) | 0.558 | ||
| Food that household likes to eat | Overall | 77% | |||||
| White | 77% | Ref | Ref | ||||
| Black | 78% | 1.06 (0.42–2.72) | 0.898 | 1.75 (0.64–4.79) | 0.272 | ||
| Latino | 74% | 0.83 (0.35–1.98) | 0.679 | 1.45 (0.58–3.60) | 0.425 | ||
| Asian | 79% | 0.92 (0.13–6.64) | 0.932 | 0.97 (0.08–11.20) | 0.979 | ||
| Food is good quality | Overall | 75% | |||||
| White | 76% | Ref | Ref | ||||
| Black | 77% | 1.06 (0.42–2.64) | 0.906 | 1.88 (0.72–4.91) | 0.199 | ||
| Latino | 67% | 0.62 (0.27–1.42) | 0.262 | 1.07 (0.47–2.45) | 0.870 | ||
| Asian | 84% | 5.94 (1.27–27.70) | 0.024 | 8.85 (1.45–53.90) | 0.018 | ||
| Provides enough food | Overall | 66% | |||||
| White | 67% | Ref | Ref | ||||
| Black | 68% | 1.03 (0.45–2.37) | 0.947 | 0.98 (0.37–2.57) | 0.960 | ||
| Latino | 64% | 0.87 (0.42–1.82) | 0.712 | 0.85 (0.41–1.76) | 0.654 | ||
| Asian | 59% | 1.16 (0.23–6.00) | 0.857 | 1.61 (0.34–7.64) | 0.549 | ||
| I know how to prepare the foods | Overall | 79% | |||||
| White | 84% | Ref | Ref | ||||
| Black | 89% | 1.53 (0.53–4.41) | 0.426 | 2.77 (0.93–8.26) | 0.068 | ||
| Latino | 64% | 0.34 (0.15–0.81) | 0.015 | 0.83 (0.36–1.93) | 0.665 | ||
| Asian | 73% | 0.41 (0.07–2.22) | 0.298 | 0.47 (0.08–2.91) | 0.417 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marriott, J.P.; Fiechtner, L.; Birk, N.W.; Taitelbaum, D.; Odoms-Young, A.; Wilson, N.L.; Clay, L.A.; Zack, R.M. Racial/Ethnic Disparities in Food Pantry Use and Barriers in Massachusetts during the First Year of the COVID-19 Pandemic. Nutrients 2022, 14, 2531. https://doi.org/10.3390/nu14122531
Marriott JP, Fiechtner L, Birk NW, Taitelbaum D, Odoms-Young A, Wilson NL, Clay LA, Zack RM. Racial/Ethnic Disparities in Food Pantry Use and Barriers in Massachusetts during the First Year of the COVID-19 Pandemic. Nutrients. 2022; 14(12):2531. https://doi.org/10.3390/nu14122531
Chicago/Turabian StyleMarriott, James P., Lauren Fiechtner, Nick W. Birk, Daniel Taitelbaum, Angela Odoms-Young, Norbert L. Wilson, Lauren A. Clay, and Rachel M. Zack. 2022. "Racial/Ethnic Disparities in Food Pantry Use and Barriers in Massachusetts during the First Year of the COVID-19 Pandemic" Nutrients 14, no. 12: 2531. https://doi.org/10.3390/nu14122531
APA StyleMarriott, J. P., Fiechtner, L., Birk, N. W., Taitelbaum, D., Odoms-Young, A., Wilson, N. L., Clay, L. A., & Zack, R. M. (2022). Racial/Ethnic Disparities in Food Pantry Use and Barriers in Massachusetts during the First Year of the COVID-19 Pandemic. Nutrients, 14(12), 2531. https://doi.org/10.3390/nu14122531