
Food Security Challenges and Resilience during the COVID-19 Pandemic: Corner Store Communities in Washington, D.C.

 , and
, and
Abstract
:1. Introduction
COVID-19 Pandemic and Food Security
2. Materials and Methods
2.1. DC Central Kitchen Healthy Corners Program
2.2. Humanities Truck
2.3. Data Collection
2.4. Data Analysis
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berkowitz, S.A.; Seligman, H.K.; Meigs, J.B.; Basu, S. Food insecurity, healthcare utilization, and high cost: A longitudinal cohort study. Am. J. Manag. Care 2018, 24, 399–404. [Google Scholar]
- Gundersen, C.; Ziliak, J.P. Food insecurity and health outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [Green Version]
- United States Department of Agriculture. Definitions of Food Security. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security.aspx (accessed on 8 June 2022).
- Althoff, R.R.; Ametti, M.; Bertmann, F. The role of food insecurity in developmental psychopathology. Prev. Med. 2016, 92, 106–109. [Google Scholar] [CrossRef] [Green Version]
- Holben, D.H.; Marshall, M.B. Position of the Academy of Nutrition and Dietetics: Food insecurity in the United States. J Acad. Nutr. Diet. 2017, 117, 1991–2002. [Google Scholar] [CrossRef] [Green Version]
- Seligman, H.K.; Bindman, A.B.; Vittinghoff, E. Food insecurity is associated with diabetes mellitus: Results from the National Health Examination and Nutrition Examination Survey (NHANES) 1999–2002. J. Gen. Intern. Med. 2007, 22, 1018–1023. [Google Scholar] [CrossRef] [Green Version]
- Seligman, H.K.; Laraia, B.A.; Kushel, M.B. Food insecurity is associated with chronic disease among low-income NHANES participants. J. Nutr. 2010, 140, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, B.; Rong, S. Food insecurity is associated with cardiovascular and all-cause mortality among adults in the United States. J. Am. Heart Assoc. 2020, 9, e014629. [Google Scholar] [CrossRef]
- Whitaker, R.C.; Phillips, S.M.; Orzol, S.M. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics 2006, 118, e859–e868. [Google Scholar] [CrossRef]
- Garcia, S.P.; Haddix, A.; Barnett, K. Incremental health care costs associated with food insecurity and chronic conditions among older adults. Prev. Chronic. Dis. 2018, 15, E108. [Google Scholar] [CrossRef] [Green Version]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2020, ERR-298. U.S. Dep. Agric. Econ. Res. Serv. 2021, 47, 1–55. [Google Scholar]
- Huang, J.; Kim, Y.; Birkenmaier, J. Unemployment and household food hardship in the economic recession. Public Health Nutr. 2016, 19, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Nord, M.; Coleman-Jensen, A.; Gregory, C. Prevalence of US Food Insecurity Is Related to Changes in Unemployment, Inflation, and the Price of Food; United States Department of Agriculture: Washington, DC, USA, 2014.
- Ralston, K.; Treen, K.; Coleman-Jensen, A. Children’s Food Security and USDA Child Nutrition Programs. Available online: https://www.ers.usda.gov/webdocs/publications/84003/eib-174.pdf?v=720.6 (accessed on 9 June 2022).
- Gundersen, C.; Kaiser, B.; Pepper, J. The impact of the National School Lunch Program on Child Health: A nonparametric bounds analysis. J. Econom. 2011, 66, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Kenney, E.L.; Barrett, J.L.; Bleich, S.N.; Ward, Z.J.; Cradock, A.L.; Gortmaker, S.L. Impact of The Healthy, Hunger-Free Kids Act On Obesity Trends. Health Aff. 2020, 39, 1122–1129. [Google Scholar] [CrossRef]
- Schwartz, A.E.; Rothbart, M.W. Let them eat lunch: The impact of universal free meals on student performance. J. Policy Anal. Manag. 2020, 39, 376–410. [Google Scholar] [CrossRef]
- Dunn, C.G.; Kenney, E.; Fleischhacker, S.E. Feeding low-income children during the COVID-19 pandemic. N. Engl. J. Med. 2020, 382, e40. [Google Scholar] [CrossRef]
- Kinsey, E.W.; Hecht, A.A.; Dunn, C.G. School closures during COVID-19: Opportunities for innovation in meal service. Am. J. Public Health 2020, 110, 1635–1643. [Google Scholar] [CrossRef]
- Food Resource and Action Center. School Meals: The Impact of the Pandemic on 54 Large School Districts. Available online: https://frac.org/research/resource-library/largedistrictsreport2021 (accessed on 24 June 2022).
- School Nutrition Association (2021) New USDA Data: Fewer Meals Served, $2B Loss for School Meal Programs. Available online: https://schoolnutrition.org/news-publications/press-releases/2021/new-usda-data-fewer-meals-served-2B-loss-for-school-meal-programs/ (accessed on 14 June 2022).
- McKenzie, S. COVID-19 Forces Recalibration of Priorities as World Embraces New Habits; Nielsen: New York, NY, USA, 2020. [Google Scholar]
- Johns Hopkins Center for a Livable Future. Baltimore City’s Food Environment. Available online: https://clf.jhsph.edu/sites/default/files/2019-01/baltimore-city-food-environment-2018-report.pdf.2018 (accessed on 21 June 2022).
- Hawkins, M.; Panzera, A. Food insecurity: A key determinant of health. Arch. Psychiatr. Nurs. 2020, 35, 113–117. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Leung, C.W. Food Insecurity and COVID-19: Disparities in Early Effects for US Adults. Nutrients 2020, 12, 1648. [Google Scholar] [CrossRef]
- Niles, M.T.; Bertmann, F.; Belarmino, E.H.; Wentworth, T.; Biehl, E.; Neff, R. The Early Food Insecurity Impacts of COVID-19. Nutrients 2020, 12, 2096. [Google Scholar] [CrossRef]
- Almohamad, M.; Mofleh, D.; Sharma, S. The impact of the COVID-19 pandemic on food insecurity. J. Agric. Food Syst. Community Dev. 2020, 10, 261–264. [Google Scholar] [CrossRef]
- Arndt, C.; Davies, R.; Gabriel, S.; Harris, L.; Makrelov, K.; Robinson, S.; Levy, S.; Simbanegavi, W.; Van Seventer, D.; Anderson, L. COVID-19 lockdowns, income distribution, and food security: An analysis for South Africa. Glob. Food Secur. 2020, 26, 100410. [Google Scholar] [CrossRef] [PubMed]
- Buheji, M.; Costa Cunha, K.; Beka, G.; Mavric, B.; Souza, Y.; Costa Silva, S.S.; Hanafi, M.; Yein, T.C. The extent of COVID-19 pandemic socio-economic impact on global poverty. A global integrative multidisciplinary review. Am. J. Econ. 2020, 10, 213–224. [Google Scholar] [CrossRef]
- Chirisa, I.; Mutambisi, T.; Chivenge, M.; Mabaso, E.; Matamanda, A.R.; Ncube, R. The urban penalty of COVID-19 lockdowns across the globe: Manifestations and lessons for Anglophone sub-Saharan Africa. GeoJournal 2020, 87, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, S.M.; Koya, S.F.; Jamieson, M.; Verma, M.; Haldane, V.; Jung, A.-S.; Singh, S.; Nordström, A.; Obaid, T.; Legido-Quigley, H. Investing in trust and community resilience: Lessons from the early months of the first digital pandemic. Br. Manag. J. 2021, 375, 067487. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, A.; Hawkins, M.; Cotter, E.W.; Snelling, A. Interest in receiving nutrition information through social media among food security program participants in Washington DC. Prev. Chronic Dis. 2021, 18, E50. [Google Scholar] [CrossRef]
- Hawkins, M.; Belson, S.I.; McClave, R.; Kohls, L.; Little, S.; Snelling, A. Healthy Schoolhouse 2.0 health promotion intervention to reduce childhood obesity in Washington, DC: A feasibility study. Nutrients 2021, 13, 2935. [Google Scholar] [CrossRef]
- Hawkins, M.; Fuchs, H.; Watts, E.; Belson, S.I.; Snelling, A. Development of a nutrition literacy survey for use among elementary school students in communities with high rates of food insecurity. J. Hunger. Environ. Nutr. 2021, 16, 108. [Google Scholar] [CrossRef]
- Hawkins, M.; Watts, E.; Belson, S.I.; Albershardt, R.; Snelling, A. Design and implementation of a 5-year school-based nutrition education intervention. J. Nutr. Educ. Behav. 2019, 52, 421–428. [Google Scholar] [CrossRef]
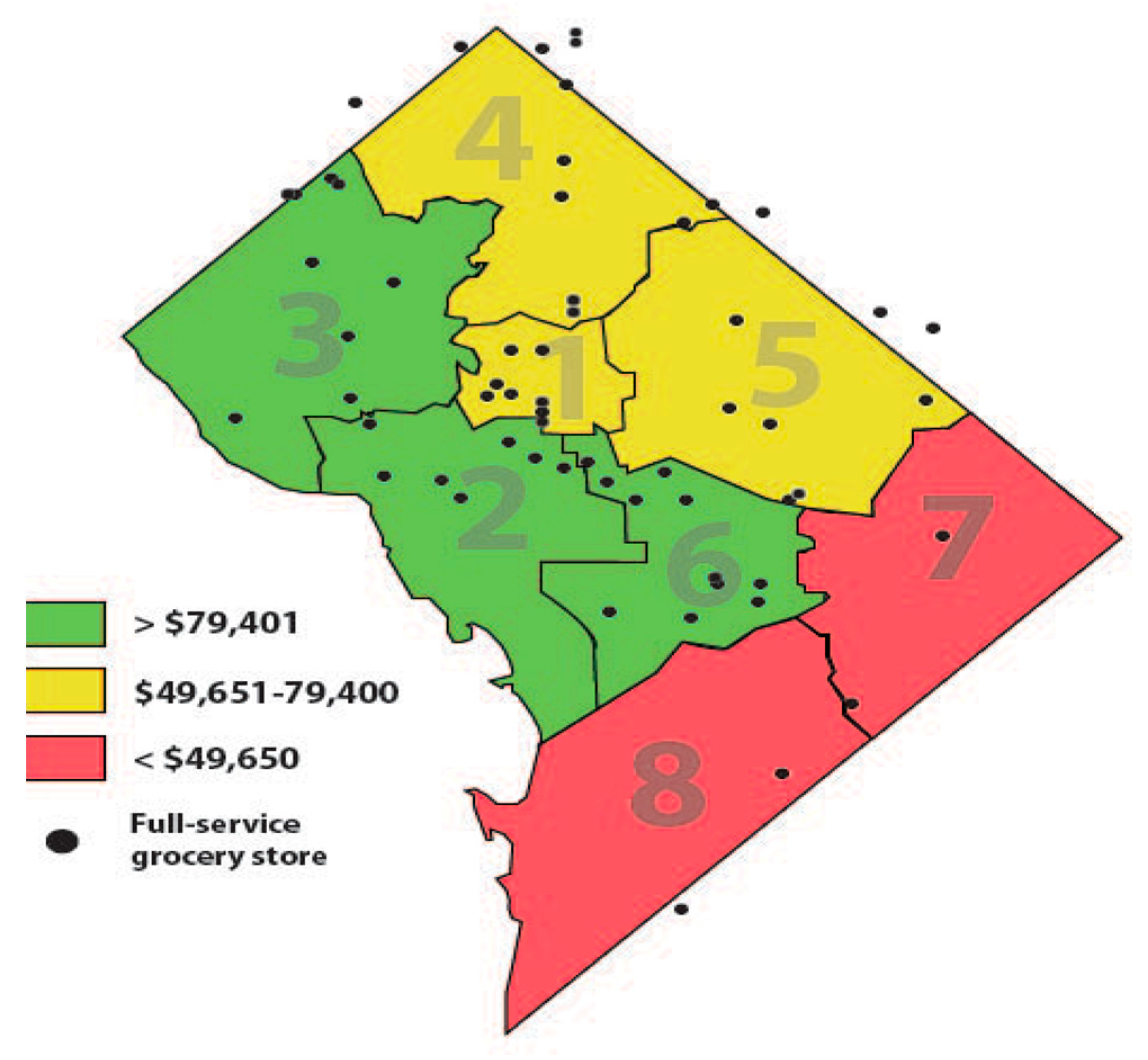
- U.S. Census Bureau. QuickFacts District of Columbia. 2021. Available online: https://www.census.gov/quickfacts/DC (accessed on 12 July 2022).
- Virginia Commonwealth University Center on Society, Health for the Metropolitan Washington Council of Governments, Health Officials Committee (2018) Uneven Opportunities: How Conditions for Wellness Vary Across the Metropolitan Washington Region. Available online: https://www.mwcog.org/documents/2020/10/26/uneven-opportunities-how-conditions-for-wellness-vary-across-the-metropolitan-washington-region-health-health-data/ (accessed on 19 June 2022).
- Arias, E.; Xu, J.Q.; Tejada-Vera, B.; Bastian, B.U.S. State Life Tables, 2019. In National Vital Statistics Reports; Hyattsville, M.D., Ed.; National Center for Health Statistics: Hyattsville, MD, USA, 2022; Volume 70. [Google Scholar] [CrossRef]
- DC Hunger Solutions. Still Minding the Grocery Gap in DC. Available online: https://www.dchunger.org/wp-content/uploads/2021/01/StillMindingGroceryGap.pdf (accessed on 12 July 2022).
- Kijakazi, K.; Brooks, R.M.; Atkins, M.R.; Price, A.E.; Hamilton, D.; Darity, W.A. The Color of Wealth in the Nation’s Capital; Duke University: Durham, NC, USA; Urban Institute: Washington, DC, USA; The New School: New York, NY, USA; Insight Center for Community Economic Development: Oakland, CA, USA, 2016. [Google Scholar]
- Stuff, J.E.; Casey, P.H.; Szeto, K.L.; Gossett, J.M.; Robbins, J.M.; Simpson, P.M.; Connell, C.; Bogle, M.L. Household food insecurity is associated with adult health status. J. Nutr. 2004, 134, 2330–2335. [Google Scholar] [CrossRef]
- Vozoris, N.T.; Tarasuk, V.S. Household food insufficiency is associated with poorer health. J. Nutr. 2003, 133, 120–126. [Google Scholar] [CrossRef]
- United States Department of Agriculture. Making Corner Stores Healthier Places to Shop; United States Department of Agriculture: Washington, DC, USA, 2016.
- Snelling, A.; McClave, R.; Van Dyke, H.; Wells, A.; Joseph, L. Healthy Corners: Balancing Store Performance & Customer Needs to Promote Fresh Produce Access & Consumption, 2017–2020 Evaluation. September 2020. Available online: https://www.american.edu/cas/healthyschools/publications.cfm.
- Let’s Move! Healthy Communities. Available online: http://www.letsmove.gov/healthy-communities (accessed on 11 July 2022).
- Resilient Washington DC. Available online: https://resilient.dc.gov/ (accessed on 13 July 2022).
- Kumanyika, S. Getting to Equity in Obesity Prevention: A New Framework. 2017. National Academy of Medicine. Available online: https://nam.edu/getting-to-equity-in-obesity-prevention-a-new-framework (accessed on 10 June 2022).
- McClave, R.; Snelling, A.; Hawkins, M.; Belson, S.I. Healthy Schoolhouse 2.0 strides toward equity in obesity prevention. Child. Obes. 2022. [Google Scholar] [CrossRef] [PubMed]
- Jumarali, S.N.; Nnawulezi, N.; Royson, S.; Lippy, C.; Rivera, A.N.; Toopet, T. Participatory Research Engagement of Vulnerable Populations: Employing Survivor-Centered, Trauma-Informed Approaches. J. Particip. Res. Methods 2021, 2, 1–21. [Google Scholar] [CrossRef]
- DC Central Kitchen. Healthy Corner Store Program. Available online: https://dccentralkitchen.org/healthy-corners/ (accessed on 13 June 2022).
- Snelling, A.M.; Yamamoto, J.J.; Belazis, L.B.; Selzter, G.R.; McClave, R.L.; Watts, E. Incentivizing Supplemental Nutrition Assistance Program Purchases with Fresh Produce in Corner Stores to Reduce Food Inequity in Underserved Areas of Washington DC. Health Equity 2020, 4, 386–393. [Google Scholar] [CrossRef]
- Drahota, A.; Meza, R.D.; Brikho, B. Community-academic partnerships: A systematic review of the state of the literature and recommendations for future research. Milbank Q. 2016, 94, 163–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, H. Navigating the waves: The usefulness of a pilot in qualitative research. Qual. Res. 2004, 4, 383–402. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo (Released in March 2020). 2020. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 15 June 2022).
- Campbell, J.L.; Quincy, C.; Osserman, J. Coding in-depth semi structured interviews problems of unitization and intercoder reliability and agreement. Soc. Methods Res. 2013, 42, 294–320. [Google Scholar] [CrossRef]
- Burla, L.; Knierim, B.; Barth, J. From text to codings: Intercoder reliability assessment in qualitative content analysis. Nurs. Res. 2008, 5, 113–117. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Aldrich, D.P.; Meyer, M.A. Social capital and community resilience. Am. Behav. Sci. 2015, 59, 254–269. [Google Scholar] [CrossRef]
- Dawes, S.S.; Cresswell, A.M.; Cahan, B.B. Learning from crisis: Lessons in human and information infrastructure from the world trade center response. Soc. Sci. Comput. Rev. 2004, 22, 52–66. [Google Scholar] [CrossRef]
- Sippel, L.M.; Pietrzak, R.H.; Charney, D.S.; Mayes, L.C.; Southwick, S.M. How does social support enhance resilience in the trauma-exposed individual? Ecol. Soc. 2015, 20, 10. [Google Scholar] [CrossRef]
- Vieselmeyer, J.; Holguin, J.; Mezulis, A. The role of resilience and gratitude in posttraumatic stress and growth following a campus shooting. Psychol. Trauma Theory Res. Pract. Policy 2017, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Coles, E.; Buckle, P. Developing community resilience as a foundation for effective disaster recovery. Aust. J. Emerg. Management 2004, 19, 6. [Google Scholar]
- Patel, S.S.; Rogers, M.B.; Amlôt, R.; Rubin, G.J. What Do We Mean by ‘Community Resilience’? A Systematic Literature Review of How It Is Defined in the Literature. PLoS Curr. 2017, 9. [Google Scholar] [CrossRef]
- Shanks, C.B.; Hingle, M.D.; Parks, C.A. The COVID-19 pandemic: A watershed moment to strengthen food security across the US food system. Am. J. Public Health 2020, 110, 1133–1134. [Google Scholar] [CrossRef]
- Katigbak, C.; Van Devanter, N.; Islam, N.; Trinh-Shevrin, C. Partners in health: A conceptual framework for the role of community health workers in facilitating patients’ adoption of healthy behaviors. Am. J. Public Health 2015, 105, 872–880. [Google Scholar] [CrossRef]
- Ballard, M.; Bancroft, E.; Nesbit, J. Prioritising the role of community health workers in the COVID-19 response. BMJ Glob. Health 2020, 5, e002550. [Google Scholar] [CrossRef]
- Johnson, S.L.; Gunn, V.L. Community health workers as a component of the health care team. J. Community Health 2012, 37, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Kangovi, S.; Mitra, N.; Turr, L.; Huo, H.; Grande, D.; Long, J.A. A randomized controlled trial of a community health worker intervention in a population of patients with multiple chronic diseases: Study design and protocol. Contemp. Clin. Trials 2017, 53, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.F.W.; Hecht, A.A.; McLoughlin, G.M.; Turner, L.; Schwartz, M.B. Universal School Meals and Associations with Student Participation, Attendance, Academic Performance, Diet Quality, Food Security, and Body Mass Index: A Systematic Review. Nutrients 2021, 13, 911. [Google Scholar] [CrossRef]
- Ryu, J.-H.; Bartfeld, J.S. Household food insecurity during childhood and subsequent health status: The early childhood longitudinal study—Kindergarten cohort. Am. J. Public Health 2012, 102, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, C.; Engelhard, E.; Crumbaug, A.; Seligman, H. Brief assessment of food insecurity accurately identifies high-risk US adults. Public Health Nutr. 2017, 20, 1367–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Category | Questions |
|---|---|
| Demographic | First name, age, neighborhood |
| Challenges | What has been biggest challenge to you/family during the pandemic? Is there anything that has been good for you/family during the pandemic? |
| Food Access | How are you navigating food access for you/family? How well do your current grocery store options fit your needs? How often do you shop at corner stores? |
| Information/Resources | Where or from who to do you get information you can trust? |
| Feelings/expectations | What do you expect from your family/community/politicians/institutions during this Covid pandemic? |
| Fears/hopes/lessons | What is your biggest fear about Covid going forward? What is your biggest hope for you/DC/US/world after the pandemic? What gives you strength right now? What is something you hope will be different for you/DC/US/world after pandemic? |
| Public Health | How would you describe public health? What does public health mean to you? |
| Specific: DC Programs, Vaccination, Schools | What do you think of the way DC has managed Covid response? |
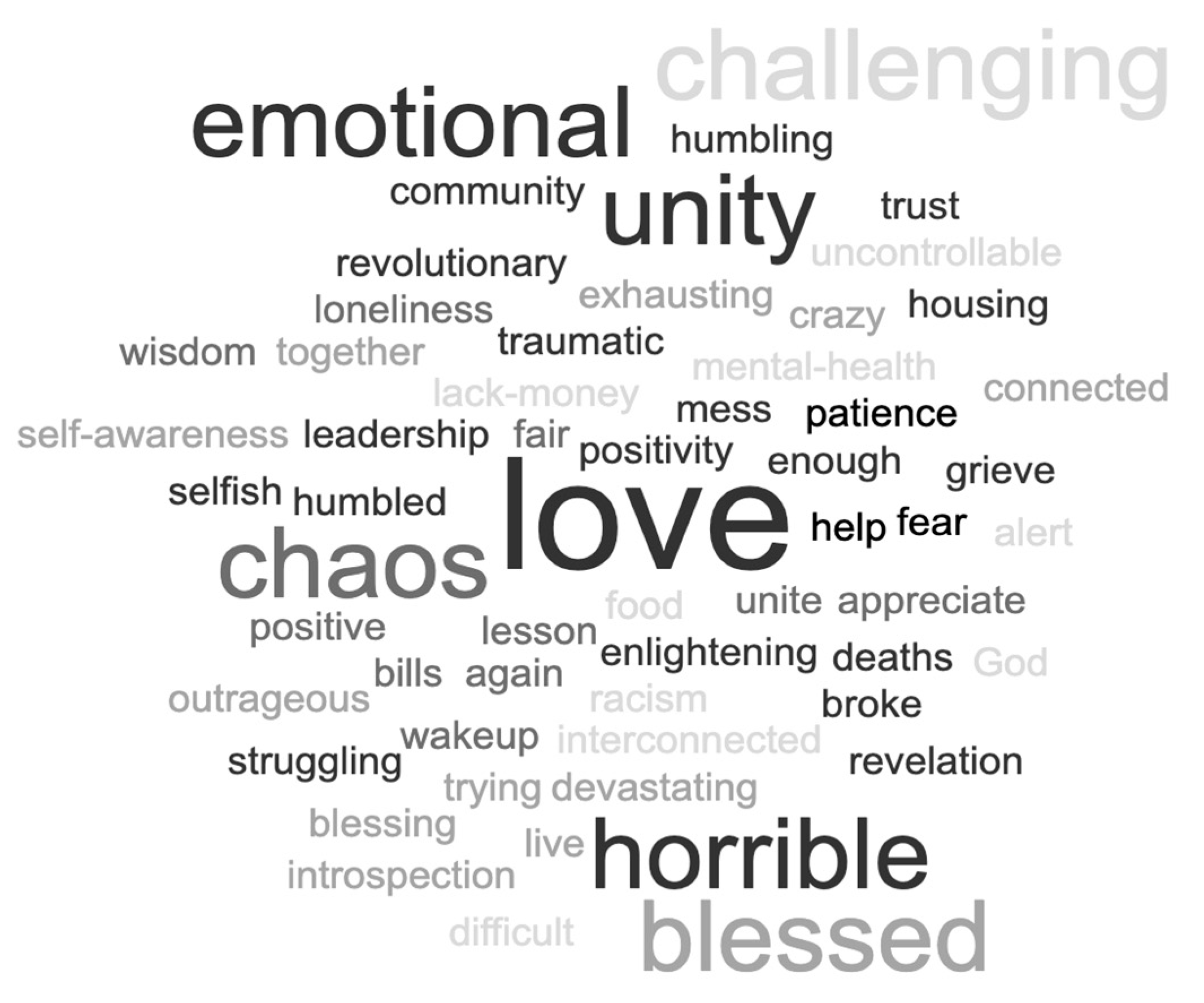
| One word | What is one word to describe this time for you? |
| Final remarks | Is there anything that we have not covered? Would you like to share anything else? |
| n (%) | |
|---|---|
| Gender | |
| male | 31 (39%) |
| female | 48 (61%) |
| Age | Mean = 42.4 (20–73 years) |
| Corner Store/Grocery Location | |
| (21 truck visits) | |
| Ward 5 | 6 (25%) |
| Ward 7 | 6 (25%) |
| Ward 8 | 9 (43%) |
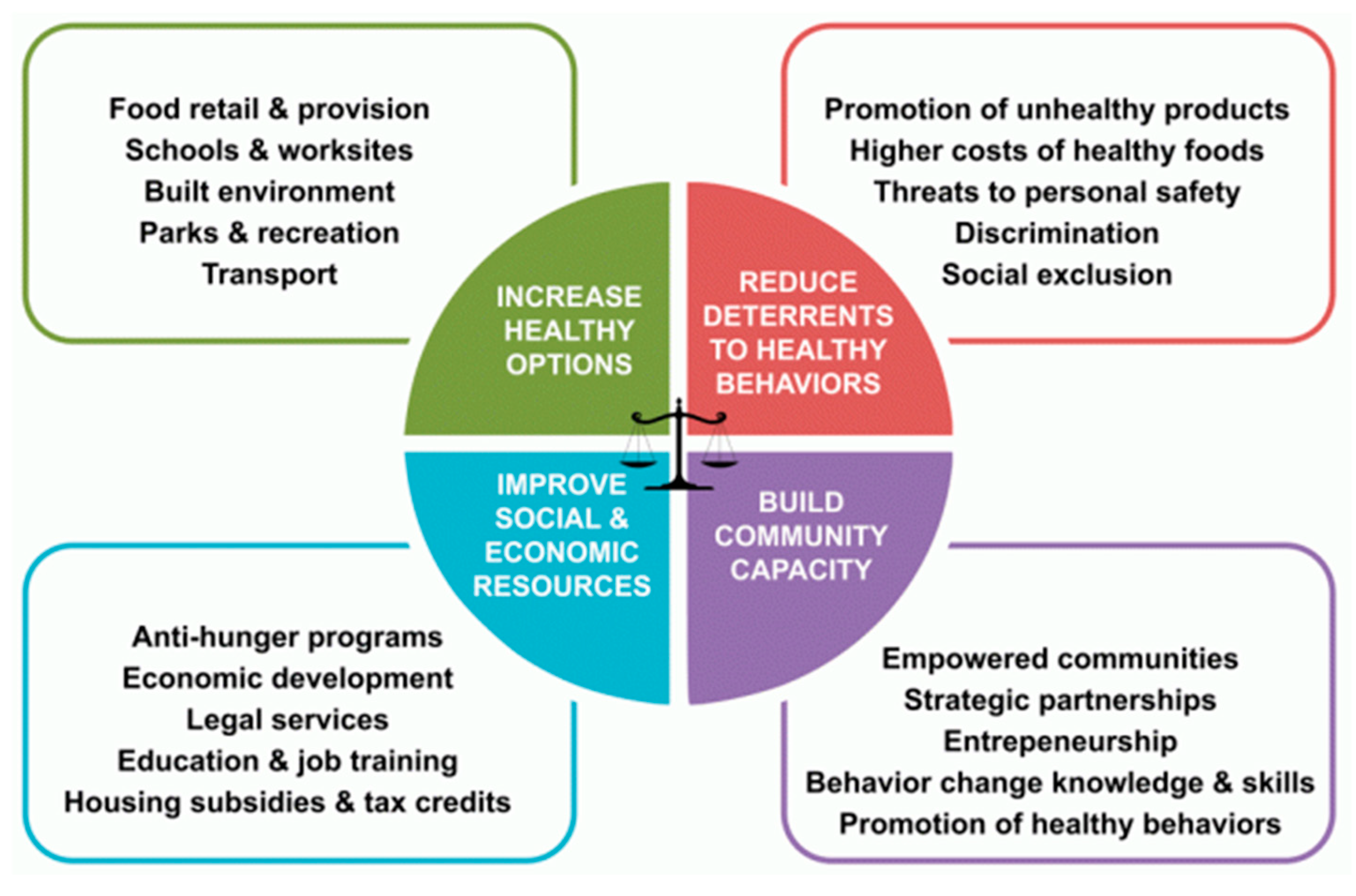
| GTE Framework Quadrant | Key Themes | Exemplary Quotes |
|---|---|---|
| Increase Healthy Options |
| “DC told us where to get the food. Transportation was free. Food was free. I was eating healthier through this. I didn’t expect that.” “The biggest challenge is high price of food and getting around to get it. There has been a lot of help in the neighborhood with people giving out food. They’ve been handing out vegetables and produce and that’s been a big help.” “I get food stamps so that’s a big help. They’ve increased them and I wish that it could go longer before it goes back. It’s helped my pantry tremendously. To be able to get organic fresh produce is so good.” |
| Reduce Deterrents to Healthy Behaviors |
| “At my grocery store you can tell they know what neighborhood they are in. The meat is spoiled, I have brought management attention to multiple expired items on entire shelves, molded cucumbers. You expect them to treat you like they treat you.” “It’s a class thing. They don’t give us the freshest produce. They give us soft apples…or food that expires in a matter of days. You get tired of traveling outside of your community going all the way uptown to get the freshest produce. It’s just sad.” “I have a problem with proliferation of liquor stores in the middle of a food desert. There are 7 liquor stores in one block, but no grocery stores. You have to throw a search party to find fruit in this neighborhood.” |
| Improve Social and Economic Resources |
| “The majority of people who are food insecure in DC are working class people, not homeless. The system shames you if you are poor. I’m hoping we see a change in our value system.” “DC and the Mayor have been doing an amazing job, getting support whether you are resident or not from providing food to basic sanitation items. They made sure everyone had a meal or place to pick up healthy food. I helped pass out too, so I saw firsthand what a difference getting help with food made. We made it ok for people to be comfortable asking for help.” “We dabbled in universal access to health care in this pandemic and we saw it’s important and effective.” |
| Build Community Capacity |
| “It’s been a reminder to me how interconnected everything is.” “I can’t rely on grocery stores to have food, so had to rely on kindness of neighbors, kindness of government. We saw the best and worst in society coming out during the pandemic.” “The corner stores are selling more healthy food now. I can get grapes for their snacks now. I love that they did that now. That tells me they do care about the community and our children. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawkins, M.; Clermont, M.; Wells, D.; Alston, M.; McClave, R.; Snelling, A. Food Security Challenges and Resilience during the COVID-19 Pandemic: Corner Store Communities in Washington, D.C. Nutrients 2022, 14, 3028. https://doi.org/10.3390/nu14153028
Hawkins M, Clermont M, Wells D, Alston M, McClave R, Snelling A. Food Security Challenges and Resilience during the COVID-19 Pandemic: Corner Store Communities in Washington, D.C. Nutrients. 2022; 14(15):3028. https://doi.org/10.3390/nu14153028
Chicago/Turabian StyleHawkins, Melissa, Maulie Clermont, Deborah Wells, Marvena Alston, Robin McClave, and Anastasia Snelling. 2022. "Food Security Challenges and Resilience during the COVID-19 Pandemic: Corner Store Communities in Washington, D.C." Nutrients 14, no. 15: 3028. https://doi.org/10.3390/nu14153028
APA StyleHawkins, M., Clermont, M., Wells, D., Alston, M., McClave, R., & Snelling, A. (2022). Food Security Challenges and Resilience during the COVID-19 Pandemic: Corner Store Communities in Washington, D.C. Nutrients, 14(15), 3028. https://doi.org/10.3390/nu14153028