
Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population


Abstract
:1. Introduction
2. Materials and Methods
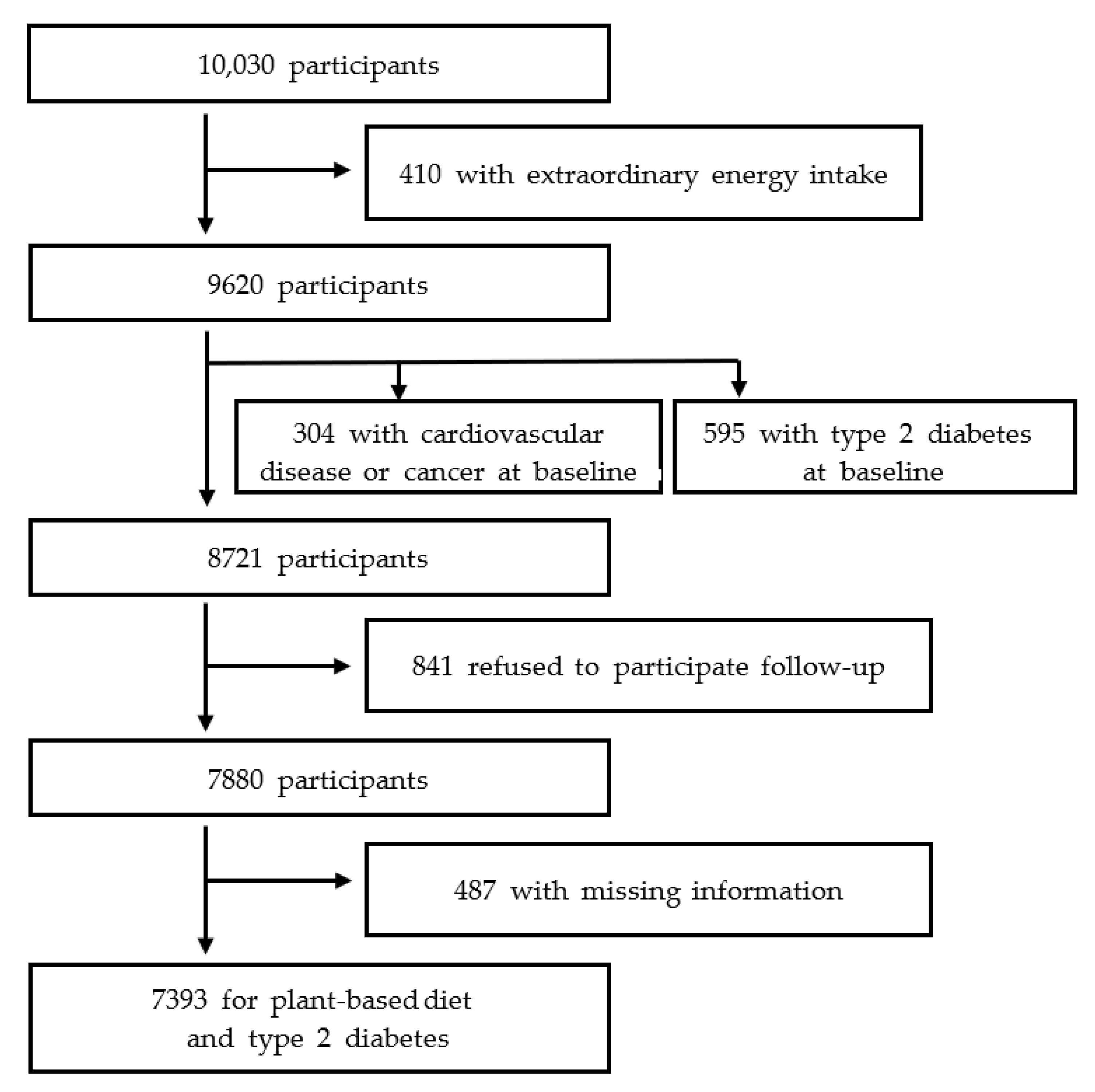
2.1. Study Population
2.2. Assessment of Plant-Based Diet Index Score
2.3. Ascertainment of Type 2 Diabetes
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kos, K. Cardiometabolic morbidity and mortality with smoking cessation, review of recommendations for people with diabetes and obesity. Curr. Diab. Rep. 2020, 20, 82. [Google Scholar] [CrossRef]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Zuurmond, M.G.; van der Schaft, N.; Nano, J.; Wijnhoven, H.A.H.; Ikram, M.A.; Franco, O.H.; Voortman, T. Plant versus animal based diets and insulin resistance, prediabetes and type 2 diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2018, 33, 883–893. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Norat, T.; Romundstad, P.; Vatten, L.J. Whole grain and refined grain consumption and the risk of type 2 diabetes: A systematic review and dose–response meta-analysis of cohort studies. Eur. J. Epidemiol. 2013, 28, 845–858. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.J.; Forouhi, N.G.; Ye, Z.; Buijsse, B.; Arriola, L.; Balkau, B.; Barricarte, A.; Beulens, J.W.; Boeing, H.; Büchner, F.L. Fruit and vegetable intake and type 2 diabetes: EPIC-InterAct prospective study and meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 1082–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraki, I.; Imamura, F.; Manson, J.E.; Hu, F.B.; Willett, W.C.; van Dam, R.M.; Sun, Q. Fruit consumption and risk of type 2 diabetes: Results from three prospective longitudinal cohort studies. BMJ 2013, 347, f5001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B. Potato and french fry consumption and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2006, 83, 284–290. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [Green Version]
- Soriguer, F.; Colomo, N.; Olveira, G.; García-Fuentes, E.; Esteva, I.; de Adana, M.S.R.; Morcillo, S.; Porras, N.; Valdés, S.; Rojo-Martínez, G. White rice consumption and risk of type 2 diabetes. Clin. Nutr. 2013, 32, 481–484. [Google Scholar] [CrossRef]
- Gijsbers, L.; Ding, E.L.; Malik, V.S.; De Goede, J.; Geleijnse, J.M.; Soedamah-Muthu, S.S. Consumption of dairy foods and diabetes incidence: A dose-response meta-analysis of observational studies. Am. J. Clin. Nutr. 2016, 103, 1111–1124. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: A comprehensive review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Picard-Deland, E.; Marette, A. Fish and marine omega-3 polyunsatured fatty acid consumption and incidence of type 2 diabetes: A systematic review and meta-analysis. Int. J. Endocrinol. 2013, 2013, 501015. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture, US Department of Health and Human Services. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture. Washington (District of Columbia). 2015. Available online: https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines/previous-dietary-guidelines/2015/advisory-report (accessed on 20 July 2022).
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-based dietary patterns and incidence of type 2 diabetes in US men and women: Results from three prospective cohort studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in US adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.-C.; Koh, W.-P.; Neelakantan, N.; Yuan, J.-M.; Qin, L.-Q.; van Dam, R.M. Diet quality indices and risk of type 2 diabetes mellitus: The Singapore Chinese Health Study. Am. J. Epidemiol. 2018, 187, 2651–2661. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, H.; Giovannucci, E.L. Quality of plant-based diets and risk of hypertension: A Korean genome and examination study. Eur. J. Nutr. 2021, 60, 3841–3851. [Google Scholar] [CrossRef]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Plant-based diets and incident metabolic syndrome: Results from a South Korean prospective cohort study. PLoS Med. 2020, 17, e1003371. [Google Scholar] [CrossRef]
- Lee, K.; Kim, H.; Rebholz, C.M.; Kim, J. Association between different types of plant-based diets and risk of dyslipidemia: A prospective cohort study. Nutrients 2021, 13, 220. [Google Scholar] [CrossRef]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Singh, G.; Yakoob, M.Y.; Abdollahi, M.; Al-Hooti, S.; et al. Global Burden of Diseases I, Risk Factors Study N, Chronic Diseases Expert G, Metabolic Risk Factors of Chronic Diseases Collaborating Group. The impact of dietary habits and metabolic risk factors on cardiovascular and diabetes mortality in countries of the Middle East and North Africa in 2010: A comparative risk assessment analysis. BMJ Open 2015, 5, e006385. [Google Scholar] [PubMed] [Green Version]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D. Global Burden of Diseases N, Chronic Diseases Expert G. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5, e008705. [Google Scholar] [CrossRef] [Green Version]
- Hopping, B.N.; Erber, E.; Grandinetti, A.; Verheus, M.; Kolonel, L.N.; Maskarinec, G. Dietary fiber, magnesium, and glycemic load alter risk of type 2 diabetes in a multiethnic cohort in Hawaii. J. Nutr. 2010, 140, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolonel, L.N.; Henderson, B.E.; Hankin, J.H.; Nomura, A.M.; Wilkens, L.R.; Pike, M.C.; Stram, D.O.; Monroe, K.R.; Earle, M.E.; Nagamine, F.S. A multiethnic cohort in Hawaii and Los Angeles: Baseline characteristics. Am. J. Epidemiol. 2000, 151, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Harmon, B.E.; Boushey, C.J.; Morimoto, Y.; Wilkens, L.R.; Le Marchand, L.; Kröger, J.; Schulze, M.B.; Kolonel, L.N.; Maskarinec, G. A priori-defined diet quality indexes and risk of type 2 diabetes: The Multiethnic Cohort. Diabetologia 2015, 58, 98–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liese, A.D.; Nichols, M.; Sun, X.; D’Agostino, R.B.; Haffner, S.M. Adherence to the DASH diet is inversely associated with incidence of type 2 diabetes: The insulin resistance atherosclerosis study. Diabetes Care 2009, 32, 1434–1436. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.-G. KoGES Group. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency (KDCA). Manual of Korean Genome and Epidemiology Study. Osong: KDCA, National Institute of Health, Center for Genomics. 2011. Available online: https://nih.go.kr/contents.es?mid=a50401010300#1 (accessed on 20 July 2022).
- American Diabetes Association. Standards of medical care in diabetes—2010. Diabetes Care 2010, 33 (Suppl. S1), S11–S61. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.J.; Yang, J.H.; Kim, J.; Cho, L.Y.; Park, B.; Ma, S.H.; Song, S.H.; Min, W.-K.; Kim, S.S.; Park, M.S. Reliability of quadruplicated serological parameters in the Korean genome and epidemiology study. Epidemiol. Health 2011, 33, e2011004. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; OBrien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32 (Suppl. S1), S498–S504. [Google Scholar] [CrossRef] [Green Version]
- The Korean Nutrition Society. Food Composition Table. In Recommended Dietary Allowances for Koreans, 7th ed; The Korean Nutrition Society: Seoul, Korea, 2000. [Google Scholar]
- Schoenfeld, D. Partial residuals for the proportional hazards regression model. Biometrika 1982, 69, 239–241. [Google Scholar] [CrossRef]
- SAS [Computer Program]; Version 9.4; SAS Institue Inc.: Cary, NC, USA, 2020.
- Li, W.; Ruan, W.; Peng, Y.; Wang, D. Soy and the risk of type 2 diabetes mellitus: A systematic review and meta-analysis of observational studies. Diabetes Res. Clin. Pract. 2018, 137, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.-M.; Knüppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Hébert, J.R.; Li, W.; Bertone-Johnson, E.R.; Olendzki, B.; Pagoto, S.L.; Tinker, L.; Rosal, M.C.; Ockene, I.S.; Ockene, J.K. Association between dietary fiber and markers of systemic inflammation in the Women’s Health Initiative Observational Study. Nutrition 2008, 24, 941–949. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Gou, L.; Peng, M.; Zheng, J.; Chen, L. Effects of soluble fiber supplementation on glycemic control in adults with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2020, 40, 1800–1810. [Google Scholar] [CrossRef]
- Cao, H.; Ou, J.; Chen, L.; Zhang, Y.; Szkudelski, T.; Delmas, D.; Daglia, M.; Xiao, J. Dietary polyphenols and type 2 diabetes: Human study and clinical trial. Crit. Rev. Food Sci. Nutr. 2019, 59, 3371–3379. [Google Scholar] [CrossRef] [PubMed]
- Poreba, M.; Rostoff, P.; Siniarski, A.; Mostowik, M.; Golebiowska-Wiatrak, R.; Nessler, J.; Undas, A.; Gajos, G. Relationship between polyunsaturated fatty acid composition in serum phospholipids, systemic low-grade inflammation, and glycemic control in patients with type 2 diabetes and atherosclerotic cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Lopetuso, L.R.; Scaldaferri, F.; Pulcini, G.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Food components and dietary habits: Keys for a healthy gut microbiota composition. Nutrients 2019, 11, 2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomova, A.; Bukovsky, I.; Rembert, E.; Yonas, W.; Alwarith, J.; Barnard, N.D.; Kahleova, H. The effects of vegetarian and vegan diets on gut microbiota. Front. Nutr. 2019, 6, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.; Choi, J.-Y.; Lee, S.-A.; Lee, K.-M.; Shin, A.; Oh, J.; Park, J.; Song, M.; Yang, J.J.; Lee, J.-k. Association between family history of diabetes and clusters of adherence to healthy behaviors: Cross-sectional results from the Health Examinees-Gem (HEXA-G) study. BMJ Open 2019, 9, e025477. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, D.; Yoshida, T.; Yoshimura, E.; Nanri, H.; Goto, C.; Ishikawa-Takata, K.; Ebine, N.; Fujita, H.; Kimura, M.; Yamada, Y. Doubly labelled water–calibration approach attenuates the underestimation of energy intake calculated from self-reported dietary assessment data in Japanese older adults. Public Health Nutr. 2021, 25, 1893–1903. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PDI | hPDI | uPDI | ||||
|---|---|---|---|---|---|---|
| Quintile 1 | Quintile 5 | Quintile 1 | Quintile 5 | Quintile 1 | Quintile 5 | |
| Sample size, n | 1451 | 1438 | 1506 | 1452 | 1586 | 1186 |
| Median score (range) | 44 (31–46) | 58 (56–69) | 43 (28–45) | 59 (57–74) | 43 (29–46) | 62 (60–76) |
| Female, n (%) | 673 (46.4) | 875 (60.9) | 542 (36.0) | 1033 (71.1) | 1014 (63.9) | 581 (49.0) |
| Age, years | 49.7 (8.4) | 53.8 (8.9) | 49.2 (8.2) | 54.2 (8.7) | 49.1 (7.8) | 55.4 (8.9) |
| Residential location, n (%) | ||||||
| Rural, Ansung | 618 (42.6) | 830 (57.7) | 496 (32.9) | 834 (57.4) | 394 (24.8) | 939 (79.2) |
| Urban, Ansan | 833 (57.4) | 608 (42.3) | 1010 (67.1) | 618 (42.6) | 1192 (75.2) | 247 (20.8) |
| Education level, n (%) | ||||||
| ≤6 years | 334 (23.0) | 607 (42.2) | 315 (20.9) | 616 (42.4) | 233 (14.7) | 627 (52.9) |
| 7–12 years | 842 (58.0) | 709 (49.3) | 886 (58.8) | 716 (49.3) | 1009 (63.6) | 499 (42.1) |
| >12 years | 275 (19.0) | 122 (8.5) | 305 (20.3) | 120 (8.3) | 344 (21.7) | 60 (5.0) |
| Cigarette smoking (pack-year) | 9.5 (14.9) | 8.4 (15.6) * | 12.6 (16.4) | 5.7 (13.1) | 6.3 (13.1) | 11.0 (17.1) |
| Alcohol intake (g/day) | 11.8 (23.1) | 7.1 (20.1) | 13.7 (26.3) | 5.7 (17.8) | 8.7 (20.7) | 8.4 (19.0) |
| Body Mass Index (kg/m2) | 24.4 (3.0) | 24.8 (3.2) | 24.5 (3.1) | 24.8 (3.3) | 24.7 (3.0) | 24.3 (3.2) |
| Physical activity (MET/day) | 21.7 (14.3) | 25.9 (15.6) | 21.7 (14.0) | 24.8 (15.5) | 20.2 (12.0) | 27.2 (16.8) |
| Family history of diabetes, n (%) | 179 (12.3) | 140 (9.7) * | 160 (10.6) | 143 (9.9) * | 223 (14.1) | 91 (7.7) |
| History of hypertension, n (%) | 151 (10.4) | 227 (15.8) | 160 (10.6) | 282 (19.4) | 200 (12.6) | 203 (17.1) |
| PDI | hPDI | uPDI | ||||
|---|---|---|---|---|---|---|
| Quintile 1 | Quintile 5 | Quintile 1 | Quintile 5 | Quintile 1 | Quintile 5 | |
| Total energy intake, kcal/day | 2048 (676) | 1836 (584) | 2016 (594) | 1850 (617) | 2064 (584) | 1717 (584) |
| Food group intake (servings/1000 kcal/week) | ||||||
| Whole grain | 4.6 (4.4) | 7.0 (4.5) | 2.5 (3.2) | 9.9 (3.7) | 7.5 (3.5) | 3.6 (4.5) |
| Fruits | 8.2 (7.0) | 13.2 (8.3) | 7.4 (5.3) | 13.7 (9.2) | 14.0 (7.7) | 7.0 (6.7) |
| Vegetables | 11.9 (6.7) | 18.2 (8.4) | 13.5 (6.4) | 16.1 (9.3) | 18.5 (8.0) | 10.6 (6.4) |
| Nuts | 0.1 (0.3) | 0.3 (0.5) | 0.1 (0.4) | 0.3 (0.6) | 0.4 (0.7) | 0.0 (0.2) |
| Legumes | 1.7 (1.5) | 3.8 (3.0) | 1.9 (1.6) | 3.7 (3.0) | 3.3 (2.0) | 1.7 (2.2) |
| Tea and coffee | 4.3 (3.8) | 6.5 (4.9) | 6.2 (4.7) | 4.6 (4.4) | 6.4 (4.4) | 3.9 (4.8) |
| Refined grains | 3.3 (4.6) | 1.8 (2.9) | 4.7 (5.0) | 0.9 (1.6) | 1.0 (1.7) | 4.6 (5.4) |
| Potatoes | 0.6 (0.6) | 1.3 (1.2) | 1.0 (0.9) | 0.8 (1.0) | 0.9 (0.9) | 0.9 (1.5) * |
| Sugar-sweetened beverages | 0.6 (1.0) | 0.7 (1.0) | 1.1 (1.1) | 0.3 (0.6) | 0.6 (0.8) | 0.6 (1.0) * |
| Sweets and desserts | 3.4 (3.0) | 4.8 (3.8) | 5.6 (3.5) | 2.6 (2.9) | 3.9 (2.9) | 3.8 (4.2) * |
| Salty foods | 11.6 (6.2) | 19.6 (8.2) | 16.0 (7.5) | 15.2 (8.3) | 13.3 (6.2) | 18.8 (9.3) |
| Animal fat | 3.5 (3.8) | 3.5 (4.4) * | 5.3 (4.3) | 1.9 (3.2) | 4.1 (3.9) | 2.8 (4.3) |
| Dairy | 3.4 (2.7) | 1.8 (2.1) | 3.0 (2.3) | 2.1 (2.5) | 3.8 (2.6) | 1.3 (1.9) |
| Eggs | 1.1 (1.0) | 0.6 (0.8) | 1.1 (0.9) | 0.6 (0.8) | 1.2 (0.9) | 0.4 (0.7) |
| Fish | 4.7 (2.7) | 3.7 (2.9) | 5.0 (2.7) | 3.5 (3.1) | 5.9 (2.9) | 2.0 (1.7) |
| Meat | 0.9 (1.1) | 0.4 (0.5) | 1.2 (1.3) | 0.3 (0.5) | 0.6 (0.7) | 0.5 (0.8) |
| Miscellaneous animal foods | 0.2 (0.3) | 0.1 (0.2) | 0.2 (0.3) | 0.1 (0.1) | 0.2 (0.2) | 0.1 (0.2) |
| Healthy plant foods | 30.8 (12.0) | 48.9 (13.6) | 31.7 (10.8) | 48.3 (14.7) | 50.2 (12.5) | 26.8 (10.7) |
| Less healthy plant foods | 19.5 (8.4) | 28.2 (9.7) | 28.3 (9.9) | 19.7 (8.8) | 19.7 (6.9) | 28.8 (11.9) |
| Animal foods | 13.8 (5.7) | 10.1 (5.7) | 15.8 (5.5) | 8.5 (5.3) | 15.8 (5.0) | 7.0 (4.9) |
| Model | PDI | hPDI | uPDI |
|---|---|---|---|
| Median (SD) | 51 (5.2) | 51 (6.4) | 52 (7.0) |
| Model 1 | 1.04 (0.92–1.18) | 0.92 (0.83–1.02) | 1.06 (0.97–1.16) |
| Model 2 | 0.99 (0.88–1.12) | 0.86 (0.77–0.95) | 1.06 (0.96–1.18) |
| Healthful Plant-Based Diet Index | p Interaction | |
|---|---|---|
| Sex | ||
| Men | 0.89 (0.77–1.04) * | 0.85 |
| Women | 0.84 (0.72–0.97) | |
| Baseline body mass index | ||
| ≥25 kg/m2 | 0.84 (0.73–0.96) | 0.19 |
| <25 kg/m2 | 0.90 (0.76–1.07) | |
| Family history of T2D | ||
| Yes | 0.58 (0.44–0.76) | 0.01 |
| No | 0.92 (0.82–1.03) | |
| History of hypertension | ||
| Yes | 0.73 (0.60–0.89) | 0.04 |
| No | 0.92 (0.81–1.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Giovannucci, E. Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population. Nutrients 2022, 14, 3078. https://doi.org/10.3390/nu14153078
Kim J, Giovannucci E. Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population. Nutrients. 2022; 14(15):3078. https://doi.org/10.3390/nu14153078
Chicago/Turabian StyleKim, Jihye, and Edward Giovannucci. 2022. "Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population" Nutrients 14, no. 15: 3078. https://doi.org/10.3390/nu14153078
APA StyleKim, J., & Giovannucci, E. (2022). Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population. Nutrients, 14(15), 3078. https://doi.org/10.3390/nu14153078