
Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
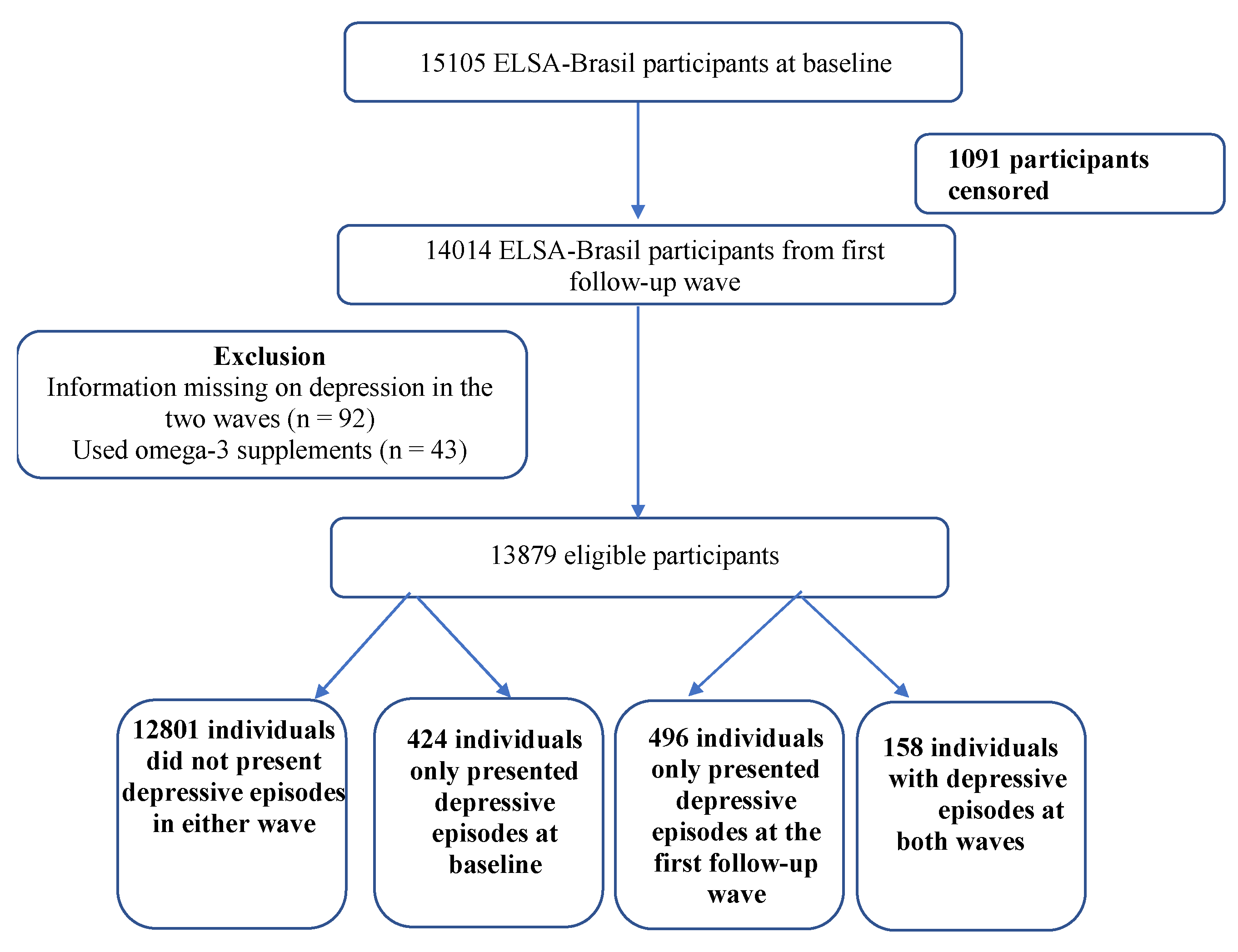
2.1. Study Design, Data Collection, and Study Population
2.2. Study Variables
2.2.1. Outcomes
2.2.2. Target Exposure
2.2.3. Covariables
2.2.4. Ethical Aspects
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD. Disease and Injury Incidence and Prevalence Collaborators (2016). Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2015, 388, 1545–1602. [Google Scholar]
- Kiadaliri, A.A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar]
- World Health Organization (WHO/OMS). Depression: And Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization (WHO/OMS). Sixty-Sixth World Assembly. Resolutions and Decisions. Annexes; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization (OMS/WHO). Time to Deliver: Report of the WHO Independent High-Level Commission on Noncommunicable Diseases; OMS/WHO: Genebra, Switzerland, 2018; p. 43. [Google Scholar]
- Barbosa, B.P. Terapia nutricional na depressão–como nutrir a saúde mental: Uma revisão bibliográfica. Braz. J. Develop. 2020, 6, 100617–100632. [Google Scholar] [CrossRef]
- Gabriel, F.C.; de Melo, D.O.; Fráguas, R.; Leite-Santos, N.C.; da Silva, R.A.M.; Ribeiro, E. Pharmacological treatment of depression: A systematic review comparing clinical practice guideline recommendations. PLoS ONE 2020, 15, e0231700. [Google Scholar] [CrossRef] [Green Version]
- De Souza, B.O.; de Vargas, V.M.K.; Rezende Pereira, E.; Buchli, G.; Ferreira Crispim, L.; da Silva Freitas, L.; de Sousa, M.F. A importância da abordagem nutricional no tratamento da depressão. Braz. J. of Develop. 2021, 7, 75964–75983. [Google Scholar] [CrossRef]
- Willett, W.C. Dietary fats and coronary heart disease. J. Intern. Med. 2012, 272, 13–24. [Google Scholar] [CrossRef]
- Natacci, L.; Marchioni, D.M.; Goulart, A.C.; Nunes, M.A.; Moreno, A.B.; Cardoso, L.O.; Giatti, L.; Molina, M.D.C.B.; Santos, I.S.; Brunoni, A.R.; et al. Omega 3 Consumption and Anxiety Disorders: A Cross-Sectional Analysis of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutrients 2018, 10, 663. [Google Scholar] [CrossRef] [Green Version]
- Quirk, S.E.; Williams, L.J.; O’Neil, A.; Pasco, J.A.; Jacka, F.N.; Housden, S.; Berk, M.; Brennan, S.L. The association between diet quality, dietary patterns and depression in adults: A systematic review. BMC Psychiatry 2013, 13, 175. [Google Scholar] [CrossRef] [Green Version]
- Molendijk, M.; Molero, P.; Sánchez-Pedreño, F.O.; Van der Does, W.; Martínez-González, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, M.B.A.; Lima, M.G.; de Azevedo, R.C.S.; de Paula Medina, L.B.; de Souza Lopes, C.; Rossi Menezes, P.; Carvalho Malta, D. Depressão e comportamentos de saúde em adultos brasileiros–PNS 2013. Rev. Saúde Públ. 2017, 51, 1s–8s. Available online: https://www.scielo.br/scielo.php?pid=S0034-89102017000200307&script=sci_arttext&tlng=pt (accessed on 6 July 2018).
- Wu, D.; Feng, L.; Gao, Q.; Li, J.L.; Rajendran, K.S.; Wong, J.C.M.; Kua, E.H.; Ng, T.-P. Association between fish intake and depressive symptoms among community-living older Chinese adults in Singapore: A cross-sectional study. J. Nutr. Health Aging 2016, 20, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Álvarez-Pérez, J.; Toledo, E.; Salas-Salvadó, J.; Ortega-Azorín, C.; Zomeño, M.D.; Vioque, J.; Martínez, J.A.; Romaguera, D.; Pérez-López, J.; et al. Seafood consumption, omega-3 fatty acids intake, and life-time prevalence of depression in the PREDIMED-plus trial. Nutrients 2018, 10, 2000. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Micek, A.; Marventano, S.; Castellano, S.; Mistretta, A.; Pajak, A.; Galvano, F. Dietary n-3 PUFA, fish consumption and depression: A systematic review and meta-analysis of observational studies. J. Affect. Disord. 2016, 205, 269–281. [Google Scholar] [CrossRef]
- Simopoulos, A.P. Evolutionary aspects of diet: The omega-6/omega-3 ratio and the brain. Mol. Neurobiol. 2011, 44, 203–215. [Google Scholar] [CrossRef]
- Ibrahim, K.S.; El-Sayed, E.M. Proposed remedies for some developmental disorders. Toxicol. Ind. Health 2013, 29, 367–384. [Google Scholar] [CrossRef] [PubMed]
- Crupi, R.; Marino, A.; Cuzzocrea, S. n-3 fatty acids: Role in neurogenesis and neu-roplasticity. Curr. Med. Chem. 2013, 20, 2953–2963. [Google Scholar] [CrossRef] [PubMed]
- Logan, A.C. Neurobehavioral aspects of ómega-3 fatty acids: Possible mechanism and therapeutic value in major depression. Omega -3/Depression. Altern. Med. Rev. 2003, 8, 410–425. [Google Scholar] [PubMed]
- Pawels, E.K.; Voterrani, D. Fatty acids facts, Part, I. Essential fatty acids as treatment for depression, or food for mood? Drug News Perspect. 2008, 21, 446–451. [Google Scholar]
- Mcnamara, R.K. Role of Omega-3 Fatty Acids in the Etiology, Treatment, and Prevention of Depression: Current Status and Future Directions. J. Nutr. Intermed. Metab. 2017, 5, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Shakya, P.R.; Melaku, Y.A.; Page, A.; Gill, T.K. Association between dietary patterns and adult depression symptoms based on principal component analysis, reduced-rank regression and partial least-squares. Clin. Nutr. 2019, 19, 33180–33182. [Google Scholar] [CrossRef]
- O’Neil, A.; Berk, M.; Itsiopoulos, C.; Castle, D.; Opie, R.; Pizzzinga, J.; Brazionis, L.; Hodge, A.; Mihalopopulos, C.; Chatterton, M.L.; et al. A randomised, controlled trial of a dietary intervention for adults with major depression (the “SMILES” trial): Study protocol. BMC Psychiatry 2013, 13, 114. [Google Scholar] [CrossRef] [Green Version]
- Ansari, F.; Pourjafar, H.; Tabrizi, A.; Homayouni, A. The Effects of Probiotics and Prebiotics on Mental Disorders: A Review on Depression, Anxiety, Alzheimer, and Autism Spectrum Disorders. Curr. Pharm. Biotechnol. 2020, 21. Available online: https://pubmed.ncbi.nlm.nih.gov/31914909/ (accessed on 6 May 2019). [CrossRef]
- Głąbska, D.; Guzek, D.; Groele, B.; Gutkowska, K. Fruit and Vegetable Intake and Mental Health in Adults: A Systematic Review. Nutrients 2020, 12, 115. [Google Scholar] [CrossRef] [Green Version]
- Wani, A.L.; Bhat, S.A.; Ara, A. Omega-3 fatty acids and the treatment of depression: A review of scientific evidence. Integr. Med. Res. 2015, 4, 132–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souto, E.P. Percepção da Disponibilidade do Capital Social e Sua Associação com Os Transtornos Mentais Comuns e Depressão: Resultados do ELSA-Brasil. Ph.D. Thesis, Escola Nacional de Saúde Pública Sérgio Arouca, Rio de Janeiro, Brazil, 2018. [Google Scholar]
- Aquino, E.M.L.; Barreto, S.; Bensenor, I.M.; Carvalho, M.; Chor, D.; Duncan, B.B.; Lotufo, P.; Mill, J.G.; Molina, M.D.C.; Mota, E.L.A.; et al. Brazilian longitudinal study of adult health (ELSA-Brasil): Objectives and design. Am. J. Epidemiol. 2012, 175, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.I.; Griep, R.H.; Passos, V.M.; Luft, V.C.; Goulart, A.C.; Menezes, G.M.D.S.; Molina, M.D.C.B.; Vigo, A.; Nunes, M.A. Estratégias e desenvolvimento de garantia e controle de qualidade no ELSA-Brasil. Rev. Saúde Públ. 2013, 47, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chor, D.; de Mello Alves, M.G.; Giatti, L.; Cade, N.V.; Nunes, M.A.; Bisi Molina, M.d.C.; Bensenor, I.M.; Aquino, E.M.L.; Pasos, V.; Santos, S.M.; et al. Questionário do Elsa-Brasil: Desafios na elaboração de instrumento multidimensional. Rev. Saúde Públ. 2013, 47, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, G.; Pelosi, A.J.; Araya, R.; Dunn, G. Measuring psychiatric disorder in the community: A standardized assessment for use by lay interviewers. Psychol. Med. 1992, 22, 465–486. [Google Scholar] [CrossRef]
- Nunes, M.A.A.; de Mello Alves, M.; Chos, D.; Schmidt, M.I.; Duncan, B.B. Adaptação Transcultural do CIS-R (Clinical Interview Schedule—Revised Version) para o Português no Estudo Longitudinal de Saúde do Adulto (ELSA). Arch. Clin. Biomed. Res. 2011, 31, 487–490. [Google Scholar]
- Molina, M.C.B.; Bensenor, I.M.; de Oliveira Cardoso, L.; Velasquez-Melendez, G.; Drehmer, M.; Silva Pereira, T.S.; de Faria, C.P.; Melere, C.; Manato, L.; Costa Gomez, A.L.; et al. Reprodutibilidade e validade relativa do Questionário de Frequência Alimentar do Elsa-Brasil. Cad. Saúde Publica 2013, 29, 379–389. [Google Scholar] [CrossRef]
- Food and Nutrition Board/Institute of Medicine. Dietary References Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; The National Academy Press: Washington, DC, USA, 2005; p. 1332. [Google Scholar]
- International Society for the Study of Fatty Acids and Lipids (ISSFAL). 3. Intake of PUFA in Healthy Adults. Available online: https://www.issfal.org/statement-3 (accessed on 1 December 2021).
- World Health Organization (WHO). Obesity. Preventing and Managing the Global Epidemic. Report of WHO Consultation on Obesity; WHO: Geneva, Switzerland, 1998; p. 252. [Google Scholar]
- Da Silva, R.C.; de Fátima Haueisen Sander Diniz, M.; Alvim, S.; Vidigal, P.G.; Fedeli, L.M.G.; Barreto, S.M. Physical activity and lipid profile in the ELSA-Brasil study. Arq. Bras. Cardiol. 2016, 107, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.I.; Duncan, B.B.; Mill, J.G.; A Lotufo, P.; Chor, D.; Barreto, S.M.; Aquino, E.M.; Passos, V.M.A.; Matos, S.M.; Molina, M.D.C.B.; et al. Cohort Profile: Longitudinal Study of Adult Health (ELSA-Brasil). Int. J. Epidemiol. 2015, 44, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.R.-project.org/ (accessed on 1 December 2018).
- Silva, S.M.C.; Mura, J.D.P. Tratado de Nutrição, Alimentação & Dietoterapia, 3rd ed.; Editora Roca: São Paulo, Brazil, 2016; p. 1338. [Google Scholar]
- Horikawa, C.; Otsuka, R.; Kato, Y.; Nishita, Y.; Tange, C.; Rogi, T.; Kawashima, H.; Shibata, H.; Ando, F.; Shimokata, H. Longitudinal association between n-3 long-chain polyunsaturated fatty acid intake and depressive symptoms: A Population-Based Cohort Study in Japan. Nutrients 2018, 10, 1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.; D’Arcy, C. The projected effect of risk factor reduction on major depression incidence: A 16-year longitudinal Canadian cohort of the National Population Health Survey. J. Affect. Disord. 2014, 158, 56–61. [Google Scholar] [CrossRef]
- Meng, X.; Brunet, A.; Turecki, G.; Liu, A.; D’Arcy, C.; Caron, J. Risk factor modifications and depression incidence: A 4-year longitudinal Canadian cohort of the Montreal Catchment Area Study. BMJ Open 2017, 7, 6. [Google Scholar] [CrossRef] [Green Version]
- Bogren, M.; Brådvik, L.; Holmstrand, C.; Nöbbelin, L.; Mattisson, C. Gender differences in subtypes of depression by first incidence and age of onset: A follow-up of the Lundby population. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Kim, Y.; Je, Y. Fish consumption and risk of depression: Epidemiological evidence from prospective studies. Asia Pac. Psychiatry 2018, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Araújo, A.D.S.F.; Veira, I.N.U.; Da Silva, J.N.F.; de Faria, S.P.; Nunes, G.L.; Khouri, A.G.; Souza, A.P.S.; de Morais, M.C.; de Silveira, A.A. Avaliação do consumo alimentar em pacientes com diagnóstico de depressão e/ou ansiedade. Ref. Saúde Fac. Estácio Sá Goiás-RRS-FESGO 2020, 3, 18–26. [Google Scholar]
- Jacka, F. Brain Changer: The Good Mental Health Diet; Macmillan: Sydney, Australia, 2019; p. 297. [Google Scholar]
- Mischoulon, D.; Freeman, M.P. Omega-3 Fatty Acids in Psychiatry. Psychiatr. Clin. N. Am. 2013, 36, 15–23. [Google Scholar] [CrossRef]
- Avancini, V.S. O papel da inflamação e a influência da dieta e do ômega 3 na prevenção e no tratamento dos quadros depressivos. Rev. AMRIGS 2021, 65, 355–364. [Google Scholar]
- Zhang, R.; Sun, J.; Li, Y.; Zhang, D. Associations of n-3, n-6 Fatty Acids Intakes and n-6:n-3 Ratio with the Risk of Depressive Symptoms: NHANES 2009–2016. Nutrients 2020, 12, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.S.; Oldmeadow, C.; Hure, A.J. Inflammation mediates the association between fatty acid intake and depression in older men and women. Nutr. Res. 2016, 36, 234–245. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Maintenance Depressive Episodes n (%) | Non- Maintenance of Depressive Episodes n (%) | p-Value a | Incidence of Depressive Episodes n (%) | Non- Incidence of Depressive Episodes n (%) | p-Value a |
|---|---|---|---|---|---|---|
| Total | 158 (27.1) | 424 (72.9) | <0.001 * | 496 (3.7) | 12,801 (96.3) | <0.001 * |
| Sex | ||||||
| Male | 27 (18.6) | 118 (81.4) | 0.004 * | 147 (2.4) | 6021 (97.6) | <0.001 * |
| Female | 131 (29.9) | 306 (70.1) | 349 (4.9) | 6780(95.1) | ||
| Age group | ||||||
| 39–44 | 13 (24.5) | 40 (75.5) | 0.65 | 62 (4.5) | 1309 (95.5) | <0.001 * |
| 45–64 | 121 (26.7) | 332 (73.3) | 378 (4.0) | 9179 (96.0) | ||
| >65 years | 24 (31.6) | 52 (68.4) | 56 (2.4) | 2313 (97.6) | ||
| Schooling | ||||||
| Complete primary | 28 (32.2) | 59 (67.8) | 0.03 * | 64 (4.3) | 1433 (95.7) | 0.01 * |
| Complete secondary | 76 (30.8) | 171 (69.2) | 183 (4.4) | 3939 (95.6) | ||
| Complete university | 54 (21.8) | 194 (78.2) | 249 (3.2) | 7429 (96.8) | ||
| Marital status | ||||||
| Married/stable union | 77 (25.4) | 226 (74.6) | 0.60 | 266 (3.1) | 8364 (96.9) | <0.001 * |
| Single | 26 (25.7) | 75 (74.3) | 82 (4.3) | 1818 (95.7) | ||
| Widow(er)/Divorced | 55 (30.9) | 123 (69.1) | 148 (5.3) | 2619 (94.7) | ||
| Race/Color | ||||||
| White | 62 (23.7) | 200 (76.3) | 0.04 * | 225 (3.2) | 6710 (96.8) | 0.02 * |
| Brown | 50 (26.9) | 136 (73.1) | 148 (4.1) | 3499 (95.9) | ||
| Black | 40 (35.4) | 71 (64.6) | 94 (4.5) | 1997 (95.5) | ||
| Other b | 6 (26.1) | 17 (73.9) | 29 (4.6) | 595 (95.4) | ||
| Monthly per capita family income | ||||||
| 1st tertile | 45 (25.6) | 131 (74.4) | 0,6 | 150 (3.6) | 3995 (96.4) | 0.06 |
| 2nd tertile | 60 (29.9) | 141 (70.1) | 158 (3.6) | 4191 (96.4) | ||
| 3rd tertile | 53 (25.9) | 152 (74.1) | 170 (3.8) | 4283 (96.2) | ||
| Missing | - | - | 18 (5.1) | 332 (94.9) | ||
| Nutritional status | ||||||
| Normal weight | 52 (34.0) | 101 (66.0) | 0.14 | 140 (3.2) | 4205 (96.8) | <0.001 * |
| Overweight | 49 (22.8) | 166 (77.2) | 184 (3.3) | 5317 (96.7) | ||
| Obesity | 57 (26.6) | 157 (73.4) | 172 (5.0) | 3279 (95.0) | ||
| Smoking | ||||||
| Smoker | 31 (31.3) | 68 (68.7) | 0.59 | 79 (5.6) | 1328 (94.4) | 0.01 * |
| Former smoker | 43 (25.0) | 129 (75.0) | 141 (3.5) | 3932 (96.5) | ||
| Nonsmoker | 84 (27.0) | 227 (73.0) | 276 (3.5) | 7541 (96.5) | ||
| Alcohol consumption | ||||||
| None | 85 (67.5) | 41 (32.5) | 0.27 | 63 (3.7) | 1643 (96.3) | 0.02 * |
| Light | 55 (24.3) | 171 (75.7) | 204 (3.4) | 5838 (96.6) | ||
| Moderate | 11 (5.4) | 194(94.6) | 201 (4.4) | 4372 (95.6) | ||
| Excessive | 7 (28.0) | 18 (72.0) | 28 (2.9) | 948 (97.1) | ||
| Physical activity | ||||||
| Light | 143 (29.1) | 348 (70.9) | 0.08 | 420 (4.3) | 9391 (95.7) | <0.001 * |
| Moderate | 8 (11.8) | 60 (88.2) | 56 (2.3) | 2334 (97.7) | ||
| Vigorous | 7 (30.4) | 16 (69.6) | 20 (1.8) | 1076 (98.2) |
| Indicator | Maintenance Depressive Episodes n = 158 | Non-Maintenance of Depressive Episodes n = 424 | p-value b | Incidence of Depressive Episodes n = 496 | Non-Incidence of Depressive Episodes n = 12,801 | p-Value b |
|---|---|---|---|---|---|---|
| Mean (Standard Deviation) | Mean (Standard Deviation) | |||||
| Total energy value (kcal) | 2665.2 (1171.8) | 2800.1 (1109.0) | 0.09 | 2834.7 (1266.5) | 2658.5 (1049.2) | 0.004 |
| Omega-3 (g) a | 2.7 (1.1) | 2.9 (1.2) | 0.09 | 2.7 (1.2) | 2.9 (1.2) | 0.001 * |
| Alpha-linolenic acid (g) a | 1.9 (0.5) | 2.0 (0.5) | 0.6 | 1.9 (0.5) | 2.0 (0.4) | 0.004 * |
| Polyunsaturated fat (PUFA) (g) a | 16.2 (4.1) | 16.5 (3.7) | 0.38 | 16.3 (3.9) | 16.6 (3.6) | 0.06 |
| Eicosapentaenoic acid (EPA) (g) a | 0.13 (0.2) | 0.16 (0.2) | <0.001 * | 0.16 (0.2) | 0.17 (0.2) | 0.002 * |
| Docosahexaenoic acid (DHA) (g) a | 0.44 (0.5) | 0.54 (0.6) | 0.05 * | 0.52 (0.6) | 0.60 (0.6) | 0.002 * |
| Docosapentaenoic acid (DPA) (g) a | 0.12 (0.1) | 0.15 (0.2) | 0.06 | 0.13 (0.2) | 0.15 (0.2) | 0.003 * |
| Maintenance of Depressive Episodes | Crude OR (95% CI) | Model 1 OR (95% CI) | Model 2 OR (95% CI) |
|---|---|---|---|
| Omega-3 | 0.88 (0.73–1.03) | 0.87 (0.73–1.02) | 0.87 (0.70–1.03) ** |
| Alpha-linolenic acid | 0.91 (0.61–1.35) | 0.91 (0.61–1.37) | 0.93 (0.62–1.39) |
| EPA | 0.36 (0.10–1.11) | 0.35 (0.10–1.07) | 0.35 (0.10–1.09) |
| DHA | 0.73 (0.50–1.02) | 0.71 (0.49–1.05) | 0.72 (0.49–1.01) ** |
| DPA | 0.32 (0.10–1.17) | 0.29 (0.07–1.10) | 0.31 (0.10–1.13) |
| PUFA | 0.98 (0.93–1.02) | 0.98 (0.94–1.03) | 0.98 (0.94–1.04) ** |
| Incidence of Depressive Episodes | Crude OR (95% CI) | Model 1 1 OR (95% CI) | Model 2 1 OR (95% CI) |
| Omega-3 | 0.90 (0.82–0.98 )* | 0.91 (0.82–0.98) * | 0.91 (0.84–0.98) * |
| Alpha-linolenic acid | 0.72 (0.59–0.89) * | 0.73 (0.59–0.90) * | 0.71 (0.59–0.91) * |
| EPA | 0.62 (0.34–1.09) | 0.67 (0.37–1.15) | 0.69 (0.39–1.20) |
| DHA | 0.87 (0.73 -1.02) ** | 0.88 (0.74 -1.04) ** | 0.89 (0.75 -1.05) ** |
| DPA | 0.59 (0.29–1.12) | 0.62 (0.32–1.18) | 0.66 (0.33–1.25) |
| PUFA | 0.97 (0.95–1.00) ** | 0.98 (0.95–1.00) ** | 0.98 (0.95–1.00) ** |
| Maintenance of Depressive Episodes a OR (95% CI) | Incidence of Depressive Episodes b OR (95% CI) | |
|---|---|---|
| Omega-3 | 0.87 (0.73–1.03) | 0.91 (0.83–0.99) |
| alpha-linolenic acid | 0.93 (0.62–1.38) | 0.74 (0.60–0.91) |
| EPA | 0.35 (0.10–1.08) | 0.69 (0.38–1.20) |
| DHA | 0.72 (0.49–1.00) | 0.89 (0.75–1.05) |
| DPA | 0.30 (0.07–1.11) | 0.65 (0.33–1.23) |
| PUFA | 0.99 (0.94–1.04) | 0.97 (0.95–0.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaves, R.d.C.S.; Aguiar, O.B.; Moreno, A.B.; Brunoni, A.R.; Molina, M.d.C.B.; Viana, M.C.; Bensoñor, I.; Griep, R.H.; da Fonseca, M.d.J.M. Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study. Nutrients 2022, 14, 3227. https://doi.org/10.3390/nu14153227
Chaves RdCS, Aguiar OB, Moreno AB, Brunoni AR, Molina MdCB, Viana MC, Bensoñor I, Griep RH, da Fonseca MdJM. Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study. Nutrients. 2022; 14(15):3227. https://doi.org/10.3390/nu14153227
Chicago/Turabian StyleChaves, Renata da Conceição Silva, Odaleia Barbosa Aguiar, Arlinda B. Moreno, André R. Brunoni, Maria del Carmem B. Molina, Maria Carmen Viana, Isabela Bensoñor, Rosane H. Griep, and Maria de Jesus Mendes da Fonseca. 2022. "Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study" Nutrients 14, no. 15: 3227. https://doi.org/10.3390/nu14153227
APA StyleChaves, R. d. C. S., Aguiar, O. B., Moreno, A. B., Brunoni, A. R., Molina, M. d. C. B., Viana, M. C., Bensoñor, I., Griep, R. H., & da Fonseca, M. d. J. M. (2022). Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study. Nutrients, 14(15), 3227. https://doi.org/10.3390/nu14153227