
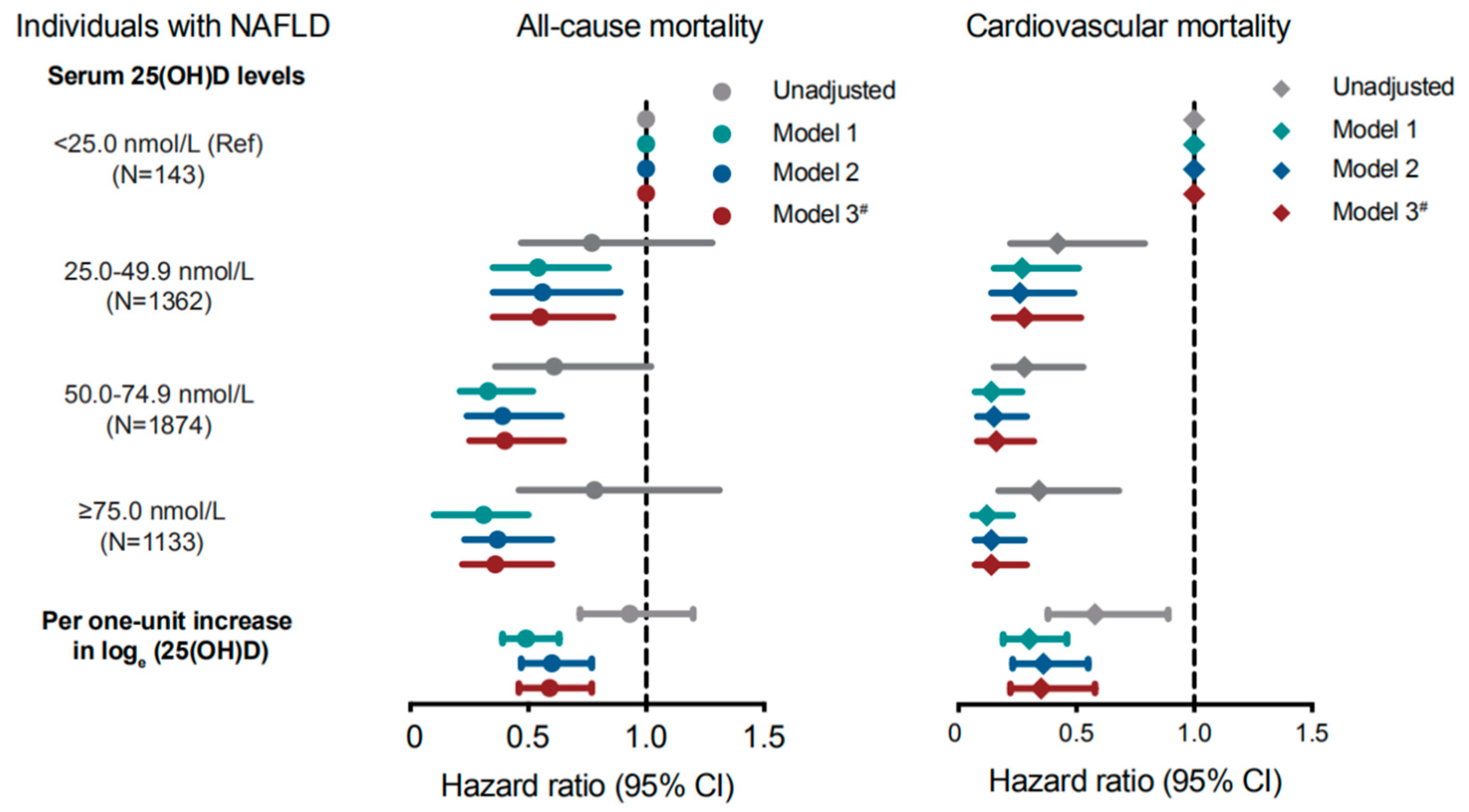
Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease


Abstract
:1. Introduction
2. Material and Methods
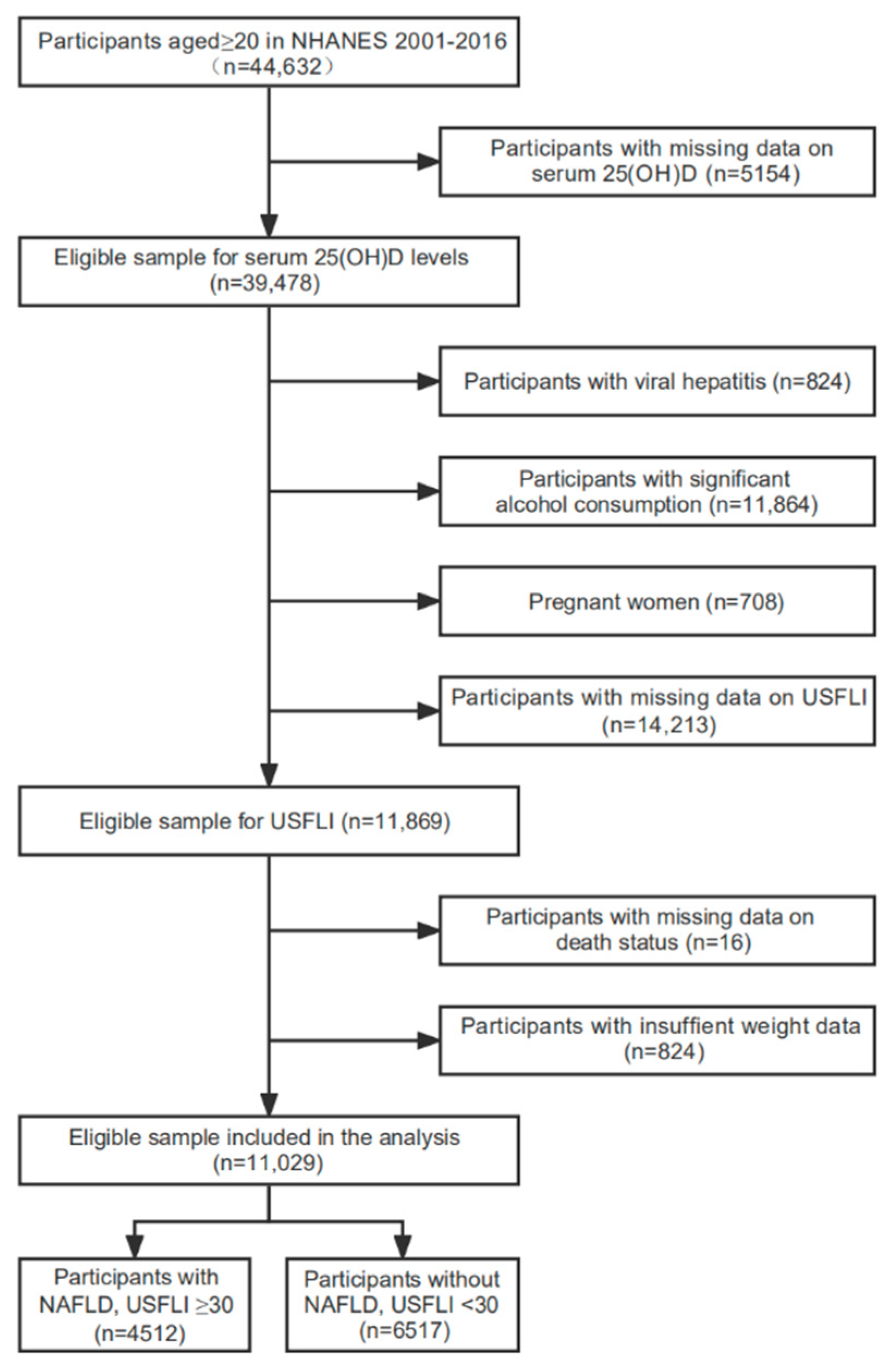
2.1. Study Participants
2.2. Definition of NAFLD
2.3. Serum 25(OH)D Measurement
2.4. Ascertainment of Mortality
2.5. Study Covariates
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Golabi, P.; Paik, J.M.; Herring, M.; Younossi, E.; Kabbara, K.; Younossi, Z.M. Prevalence of High and Moderate Risk Nonalcoholic Fatty Liver Disease among Adults in the United States, 1999–2016. Clin. Gastroenterol. Hepatol. 2021, in press. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef]
- Alvarez, C.S.; Graubard, B.I.; Thistle, J.E.; Petrick, J.L.; McGlynn, K.A. Attributable Fractions of Nonalcoholic Fatty Liver Disease for Mortality in the United States: Results From the Third National Health and Nutrition Examination Survey with 27 Years of Follow-up. Hepatology 2019, 72, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and Chronic Diseases. Aging Dis. 2017, 8, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Barchetta, I.; Cimini, F.A.; Cavallo, M.G. Vitamin D and Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): An Update. Nutrients 2020, 12, 3302. [Google Scholar] [CrossRef] [PubMed]
- Eliades, M.; Spyrou, E. Vitamin D: A new player in non-alcoholic fatty liver disease? World J. Gastroenterol. 2015, 21, 1718–1727. [Google Scholar] [CrossRef]
- Sofianopoulou, E.; Kaptoge, S.K.; Afzal, S.; Jiang, T.; Gill, D.; Gundersen, T.E.; Bolton, T.R.; Allara, E.; Arnold, M.G.; Mason, A.M.; et al. Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: Observational and Mendelian randomisation analyses. Lancet Diabetes Endocrinol. 2021, 9, 837–846. [Google Scholar] [CrossRef]
- Zhang, P.; Guo, D.; Xu, B.; Huang, C.; Yang, S.; Wang, W.; Liu, W.; Deng, Y.; Li, K.; Liu, D.; et al. Association of Serum 25-Hydroxyvitamin D With Cardiovascular Outcomes and All-Cause Mortality in Individuals With Prediabetes and Diabetes: Results From the UK Biobank Prospective Cohort Study. Diabetes Care 2022, 45, 1219–1229. [Google Scholar] [CrossRef]
- Zhao, G.; Ford, E.S.; Li, C.; Croft, J.B. Serum 25-hydroxyvitamin D levels and all-cause and cardiovascular disease mortality among US adults with hypertension: The NHANES linked mortality study. J. Hypertens. 2012, 30, 284–289. [Google Scholar] [CrossRef]
- Thomas, G.N.; ó Hartaigh, B.; Bosch, J.A.; Pilz, S.; Loerbroks, A.; Kleber, M.E.; Fischer, J.E.; Grammer, T.B.; Böhm, B.O.; März, W. Vitamin D levels predict all-cause and cardiovascular disease mortality in subjects with the metabolic syndrome: The Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Diabetes Care 2012, 35, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Liu, M.; Chen, L. Association of Serum 25-Hydroxyvitamin D Concentrations with All-Cause and Cause-Specific Mortality among Adult Patients with Existing Cardiovascular Disease. Front. Nutr. 2021, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, C.E.; Everhart, J.E. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment. Pharmacol. Ther. 2014, 41, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Analytical Note for 25-Hydroxyvitamin D Data Analysis Using NHANES III (1988–1994), NHANES 2001–2006, and NHANES 2007–2010 (October 2015). Available online: https://wwwn.cdc.gov/nchs/nhanes/vitamind/analyticalnote.aspx (accessed on 4 August 2020).
- Tucker, L.A. Physical activity and telomere length in U.S. men and women: An NHANES investigation. Prev. Med. 2017, 100, 145–151. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A. Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S14–S31. [Google Scholar] [CrossRef]
- Skversky, A.L.; Kumar, J.; Abramowitz, M.K.; Kaskel, F.J.; Melamed, M.L. Association of Glucocorticoid Use and Low 25-Hydroxyvitamin D Levels: Results from the National Health and Nutrition Examination Survey (NHANES): 2001–2006. J. Clin. Endocrinol. Metab. 2011, 96, 3838–3845. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Efird, J.T.; Nielsen, S.S. A Method to Compute Multiplicity Corrected Confidence Intervals for Odds Ratios and Other Relative Effect Estimates. Int. J. Environ. Res. Public Health 2008, 5, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Wan, Z.; Guo, J.; Pan, A.; Chen, C.; Liu, L.; Liu, G. Association of Serum 25-Hydroxyvitamin D Concentrations With All-Cause and Cause-Specific Mortality Among Individuals With Diabetes. Diabetes Care 2020, 44, 350–357. [Google Scholar] [CrossRef]
- Yoo, E.R.; Kim, D.; Vazquez-Montesino, L.M.; Escober, J.A.; Li, A.A.; Tighe, S.P.; Fernandes, C.T.; Cholankeril, G.; Ahmed, A. Diet quality and its association with nonalcoholic fatty liver disease and all-cause and cause-specific mortality. Liver Int. 2020, 40, 815–824. [Google Scholar] [CrossRef]
- Liu, X.; Baylin, A.; Levy, P.D. Vitamin D deficiency and insufficiency among US adults: Prevalence, predictors and clinical implications. Br. J. Nutr. 2018, 119, 928–936. [Google Scholar] [CrossRef]
- Liu, T.; Xu, L.; Chen, F.-H.; Zhou, Y.-B. Association of serum vitamin D level and nonalcoholic fatty liver disease: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, W.; Zhang, Y.; Yang, Y.; Qin, G. Association between vitamin D and non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: Results from a meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 17221–17234. [Google Scholar]
- Eliades, M.; Spyrou, E.; Agrawal, N.; Lazo, M.; Brancati, F.L.; Potter, J.J.; Koteish, A.A.; Clark, J.M.; Guallar, E.; Hernaez, R. Meta-analysis: Vitamin D and non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2013, 38, 246–254. [Google Scholar] [CrossRef]
- Kim, H.-S.; Rotundo, L.; Kothari, N.; Kim, S.-H.; Pyrsopoulos, N. Vitamin D Is Associated with Severity and Mortality of Non-alcoholic Fatty Liver Disease: A US Population-based Study. J. Clin. Transl. Hepatol. 2017, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Chang, Y.; Ryu, S.; Cho, I.Y.; Kwon, M.J.; Sohn, W.; Kim, M.K.; Wild, S.H.; Byrne, C.D. Resolution of, and risk of incident non-alcoholic fatty liver disease with changes in serum 25-hydroxy vitamin D status. J. Clin. Endocrinol. Metab. 2022, 107, e3437–e3447. [Google Scholar] [CrossRef]
- Dasarathy, J.; Periyalwar, P.; Allampati, S.; Bhinder, V.; Hawkins, C.; Brandt, P.; Khiyami, A.; McCullough, A.J.; Dasarathy, S. Hypovitaminosis D is associated with increased whole body fat mass and greater severity of non-alcoholic fatty liver disease. Liver Int. 2013, 34, e118–e127. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Tabrizi, R.; Nowrouzi-Sohrabi, P.; Jalali, M.; Shabani-Borujeni, M.; Modaresi, S.; Gholamalizadeh, M.; Doaei, S. The Effects of Vitamin D Supplementation on Anthropometric and Biochemical Indices in Patients With Non-alcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis. Front. Pharmacol. 2021, 12, 2918. [Google Scholar] [CrossRef] [PubMed]
- Lukenda Zanko, V.; Domislovic, V.; Trkulja, V.; Krznaric-Zrnic, I.; Turk-Wensveen, T.; Krznaric, Z.; Filipec Kanizaj, T.; Radic-Kristo, D.; Bilic-Zulle, L.; Orlic, L.; et al. Vitamin D for treatment of non-alcoholic fatty liver disease detected by transient elastography: A randomized, double-blind, placebo-controlled trial. Diabetes Obes. Metab. 2020, 22, 2097–2106. [Google Scholar] [CrossRef] [PubMed]
- Sindhughosa, D.A.; Wibawa, I.D.N.; Mariadi, I.K.; Somayana, G. Additional treatment of vitamin D for improvement of insulin resistance in non-alcoholic fatty liver disease patients: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 7716. [Google Scholar] [CrossRef]
- Guo, X.-F.; Wang, C.; Yang, T.; Li, S.; Li, K.-L.; Li, D. Vitamin D and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 7389–7399. [Google Scholar] [CrossRef]
- Jaruvongvanich, V.; Ahuja, W.; Sanguankeo, A.; Wijarnpreecha, K.; Upala, S. Vitamin D and histologic severity of nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 618–622. [Google Scholar] [CrossRef]
- Fan, X.; Wang, J.; Song, M.; Giovannucci, E.L.; Ma, H.; Jin, G.; Hu, Z.; Shen, H.; Hang, D. Vitamin D Status and Risk of All-Cause and Cause-Specific Mortality in a Large Cohort: Results From the UK Biobank. J. Clin. Endocrinol. Metab. 2020, 105, e3606–e3619. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Wan, Z.; Guo, J.; Liu, L.; Pan, A.; Liu, G. Association Between Serum 25-hydroxyvitamin D Concentrations and Mortality among Adults with Prediabetes. J. Clin. Endocrinol. Metab. 2021, 106, e4039–e4048. [Google Scholar] [CrossRef]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: Systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.L.; Elfers, C.T.; Figlewicz, D.P.; Melhorn, S.J.; Morton, G.J.; Hoofnagle, A.; Yeh, M.M.; Nelson, J.E.; Kowdley, K.V. Vitamin D deficiency in obese rats exacerbates nonalcoholic fatty liver disease and increases hepatic resistin and toll-like receptor activation. Hepatology 2011, 55, 1103–1111. [Google Scholar] [CrossRef]
- Ma, M.; Long, Q.; Chen, F.; Zhang, T.; Wang, W. Active vitamin D impedes the progression of non-alcoholic fatty liver disease by inhibiting cell senescence in a rat model. Clin. Res. Hepatol. Gastroenterol. 2019, 44, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.-G.; Liu, Y.-X.; Wang, H.; Wang, B.-P.; Qu, H.-Q.; Zhu, M. Active form of vitamin D ameliorates non-alcoholic fatty liver disease by alleviating oxidative stress in a high-fat diet rat model. Endocr. J. 2017, 64, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Ding, N.; Yu, R.T.; Subramaniam, N.; Sherman, M.H.; Wilson, C.; Rao, R.; Leblanc, M.; Coulter, S.; He, M.; Scott, C.; et al. A Vitamin D Receptor/SMAD Genomic Circuit Gates Hepatic Fibrotic Response. Cell 2013, 153, 601–613. [Google Scholar] [CrossRef]
- Abramovitch, S.; Sharvit, E.; Weisman, Y.; Bentov, A.; Brazowski, E.; Cohen, G.; Volovelsky, O.; Reif, S. Vitamin D inhibits development of liver fibrosis in an animal model but cannot ameliorate established cirrhosis. Am. J. Physiol. Liver Physiol. 2015, 308, G112–G120. [Google Scholar]
- Bozic, M.; Guzmán, C.; Benet, M.; Sánchez-Campos, S.; García-Monzón, C.; Gari, E.; Gatius, S.; Valdivielso, J.M.; Jover, R. Hepatocyte Vitamin D Receptor Regulates Lipid Metabolism and Mediates Experimental Diet-Induced Steatosis. J. Hepatol. 2016, 65, 748–757. [Google Scholar]
- Zhang, H.; Shen, Z.; Lin, Y.; Zhang, J.; Zhang, Y.; Liu, P.; Zeng, H.; Yu, M.; Chen, X.; Ning, L.; et al. Vitamin D receptor targets hepatocyte nuclear factor 4α and mediates protective effects of vitamin D in nonalcoholic fatty liver disease. J. Biol. Chem. 2020, 295, 3891–3905. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Luo, M.; Pan, L.; Chen, Y.; Guo, S.; Luo, D.; Zhu, L.; Liu, Y.; Pan, L.; Xu, S.; et al. Vitamin D signaling maintains intestinal innate immunity and gut microbiota: Potential intervention for metabolic syndrome and NAFLD. Am. J. Physiol. Liver Physiol. 2020, 318, G542–G553. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.C.; Maeng, H.J.; Liu, S.; Khan, A.A.; Groothuis, G.M.; Pang, K.S. 1alpha,25-Dihydroxyvitamin D(3) triggered vitamin D receptor and farnesoid X receptor-like effects in rat intestine and liver in vivo. Biopharm. Drug Dispos. 2009, 30, 457–475. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Serum 25(OH)D Levels (nmol/L) | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Total (N = 4512) | <25.0 (N = 143) | 25.0–49.9 (N = 1362) | 50.0–74.9 (N = 1874) | ≥75.0 (N = 1133) | p Value |
| Age (years) | 54.12 ± 0.29 | 47.52 ± 1.70 | 50.22 ± 0.60 | 53.23 ± 0.47 | 59.37 ± 0.57 | <0.001 |
| Sex, n (%) | <0.001 | |||||
| Male | 2452 (56.77) | 55 (35.06) | 652 (48.99) | 1112 (62.42) | 633 (57.09) | |
| Female | 2060 (43.23) | 88 (64.94) | 710 (51.01) | 762 (37.58) | 500 (42.91) | |
| Race/ethnicity, n (%) | <0.001 | |||||
| Non-Hispanic White | 2189 (72.03) | 23 (27.87) | 435 (55.68) | 972 (75.19) | 759 (85.32) | |
| Non-Hispanic Black | 508 (6.55) | 65 (38.56) | 254 (13.62) | 127 (3.49) | 62 (2.27) | |
| Mexican American | 1042 (10.21) | 34 (20.91) | 418 (15.67) | 470 (10.91) | 120 (3.54) | |
| Others | 773 (11.20) | 21 (12.66) | 255 (15.04) | 305 (10.41) | 192 (8.87) | |
| Smoking status, n (%) | <0.001 | |||||
| Never | 2495 (55.06) | 87 (59.26) | 792 (59.22) | 1025 (55.18) | 591 (51.03) | |
| Former | 1428 (31.40) | 26 (18.89) | 359 (23.44) | 625 (32.77) | 418 (37.46) | |
| Current | 585 (13.47) | 30 (21.85) | 210 (17.34) | 222 (12.05) | 123 (11.51) | |
| Education level, n (%) | 0.02 | |||||
| Less than high school | 1466 (21.53) | 46 (30.19) | 497 (23.70) | 630 (21.65) | 293 (18.79) | |
| High school or equivalent | 1023 (24.19) | 31 (20.31) | 298 (26.30) | 410 (22.93) | 284 (24.53) | |
| College or above | 2019 (54.23) | 66 (49.50) | 565 (50.00) | 833 (55.42) | 555 (56.68) | |
| Family poverty income ratio, n (%) | <0.001 | |||||
| <1.0 | 865 (12.62) | 35 (23.72) | 295 (16.67) | 363 (12.06) | 172 (9.00) | |
| ≥1.0 and <3.0 | 1825 (35.72) | 67 (47.21) | 583 (39.17) | 735 (34.65) | 440 (33.34) | |
| ≥3.0 | 1453 (44.97) | 29 (20.93) | 364 (36.83) | 628 (47.05) | 432 (51.01) | |
| Unknown | 369 (6.68) | 12 (8.14) | 120 (7.33) | 148 (6.24) | 89 (6.65) | |
| Physical activity, n (%) | <0.001 | |||||
| Sedentary | 1479 (28.28) | 59 (43.41) | 523 (35.33) | 546 (25.08) | 351 (25.55) | |
| Insufficient | 913 (21.07) | 19 (12.06) | 272 (21.01) | 426 (23.46) | 196 (18.35) | |
| Moderate | 527 (12.68) | 13 (9.34) | 134 (10.82) | 240 (13.78) | 140 (12.96) | |
| High | 1593 (37.97) | 52 (35.19) | 433 (32.83) | 662 (37.68) | 446 (43.15) | |
| BMI (kg/m2), n (%) | <0.001 | |||||
| <25.0 | 291 (5.06) | 6 (6.66) | 73 (3.44) | 114 (4.69) | 98 (6.99) | |
| 25.0–29.9 | 1346 (28.18) | 20 (14.38) | 325 (20.92) | 603 (29.04) | 398 (34.94) | |
| ≥30.0 | 2839 (66.22) | 117 (78.97) | 954 (75.64) | 1141 (66.27) | 627 (58.07) | |
| Diabetes, n (%) | 1526 (28.31) | 50 (30.60) | 506 (32.22) | 594 (26.11) | 376 (27.91) | 0.05 |
| Hypertension, n (%) | 2745 (58.58) | 85 (56.77) | 782 (54.51) | 1084 (55.49) | 794 (66.81) | <0.001 |
| Hyperlipidemia, n (%) | 3970 (88.12) | 121 (81.51) | 1169 (87.00) | 1664 (88.73) | 1016 (88.72) | 0.21 |
| CVD, n (%) | 815 (16.18) | 28 (19.79) | 233 (15.32) | 305 (14.63) | 249 (18.92) | 0.03 |
| Steroid use, n (%) | 84 (1.57) | 3 (2.31) | 24 (1.51) | 32 (1.52) | 25 (1.63) | 0.93 |
| eGFR (mL/min/1.73 m2) | 88.32 ± 0.42 | 97.75 ± 2.92 | 94.83 ± 0.81 | 89.44 ± 0.61 | 80.20 ± 0.62 | <0.001 |
| Waist circumference (cm) | 112.12 ± 0.32 | 115.67 ± 1.97 | 114.70 ± 0.50 | 111.85 ± 0.52 | 109.97 ± 0.55 | <0.001 |
| Total cholesterol (mg/dL) | 195.48 ± 0.89 | 187.47 ± 3.45 | 196.97 ± 1.74 | 195.59 ± 1.22 | 194.63 ± 1.56 | 0.12 |
| Low-density lipoprotein cholesterol (mg/dL) | 115.43 ± 0.74 | 113.31 ± 2.96 | 117.26 ± 1.55 | 115.82 ± 1.08 | 113.45 ± 1.19 | 0.18 |
| High-density lipoprotein cholesterol (mg/dL) | 46.52 ± 0.21 | 46.94 ± 0.92 | 45.47 ± 0.42 | 45.53 ± 0.29 | 48.84 ± 0.49 | <0.001 |
| Fasting triglyceride (mg/dL) | 173.24 ± 2.91 | 137.76 ± 8.70 | 177.16 ± 6.82 | 177.85 ± 3.73 | 165.88 ± 4.43 | <0.001 |
| Fasting glucose (mg/dL) | 118.74 ± 0.77 | 126.71 ± 5.93 | 123.00 ± 1.79 | 117.48 ± 1.01 | 116.19 ± 1.08 | 0.01 |
| Fasting insulin (pmol/L) | 20.87 ± 0.35 | 24.83 ± 1.25 | 23.00 ± 0.56 | 20.88 ± 0.63 | 18.65 ± 0.50 | <0.001 |
| Glycosylated hemoglobin, Type A1C (%) | 5.99 ± 0.02 | 6.22 ± 0.14 | 6.13 ± 0.05 | 5.93 ± 0.03 | 5.95 ± 0.04 | 0.001 |
| Gamma-glutamyltransferase (U/L) | 36.98 ± 0.61 | 41.16 ± 5.47 | 36.37 ± 1.10 | 36.02 ± 0.83 | 38.59 ± 1.39 | 0.31 |
| Serum 25(OH)D Levels (nmol/L) | ||||||
|---|---|---|---|---|---|---|
| Subgroup | No. Deaths/Total | <25.0 | 25.0–49.9 | 50.0–74.9 | ≥75.0 | p for Interaction |
| Age, years | 0.014 | |||||
| <60 | 126/2266 | 1.00 | 0.87 (0.43, 1.78) | 0.42 (0.18, 0.99) | 0.34 (0.13, 0.90) | |
| ≥60 | 772/2246 | 1.00 | 0.47 (0.28, 0.79) | 0.39 (0.22, 0.68) | 0.35 (0.20, 0.62) | |
| Sex | 0.568 | |||||
| Male | 554/2452 | 1.00 | 0.78 (0.31, 1.93) | 0.50 (0.20, 1.23) | 0.50 (0.20, 1.27) | |
| Female | 344/2060 | 1.00 | 0.46 (0.25, 0.86) | 0.40 (0.21, 0.75) | 0.31 (0.16, 0.60) | |
| Race/ethnicity | 0.186 | |||||
| White | 604/2189 | 1.00 | 0.51 (0.27, 0.95) | 0.36 (0.19, 0.69) | 0.31 (0.16, 0.58) | |
| Non-White | 294/2323 | 1.00 | 0.59 (0.31, 1.12) | 0.41 (0.22, 0.75) | 0.53 (0.27, 1.04) | |
| Smoking status | 0.770 | |||||
| Never | 367/2495 | 1.00 | 0.58 (0.34, 1.00) | 0.38 (0.22, 0.64) | 0.35 (0.21, 0.60) | |
| Former/Current | 528/2013 | 1.00 | 0.48 (0.21, 1.09) | 0.35 (0.16, 0.78) | 0.32 (0.14, 0.73) | |
| BMI, kg/m2 | 0.300 | |||||
| <30 | 396/1637 | 1.00 | 2.53 (0.50, 12.68) | 1.76 (0.35, 8.73) | 1.49 (0.29, 7.55) | |
| ≥30 | 475/2839 | 1.00 | 0.41 (0.24, 0.71) | 0.30 (0.17, 0.52) | 0.28 (0.17, 0.47) | |
| Physical activity | 0.723 | |||||
| Sedentary/Insufficient | 608/2329 | 1.00 | 0.50 (0.31, 0.81) | 0.37 (0.22, 0.61) | 0.34 (0.20, 0.56) | |
| Moderate/High | 290/2120 | 1.00 | 0.58 (0.20, 1.69) | 0.33 (0.11, 0.98) | 0.34 (0.12, 0.98) | |
| eGFR, mL/min/1.73 m2 | 0.222 | |||||
| ≤90 | 742/2358 | 1.00 | 0.41 (0.24, 0.69) | 0.35 (0.20, 0.59) | 0.31 (0.19, 0.51) | |
| >90 | 156/2154 | 1.00 | 1.05 (0.37, 2.99) | 0.62 (0.22, 1.77) | 0.71 (0.24, 2.14) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Feng, S.; Chang, Z.; Zhao, Y.; Liu, Y.; Fu, J.; Liu, Y.; Tang, S.; Han, Y.; Zhang, S.; et al. Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease. Nutrients 2022, 14, 4013. https://doi.org/10.3390/nu14194013
Chen Y, Feng S, Chang Z, Zhao Y, Liu Y, Fu J, Liu Y, Tang S, Han Y, Zhang S, et al. Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease. Nutrients. 2022; 14(19):4013. https://doi.org/10.3390/nu14194013
Chicago/Turabian StyleChen, Yuxiong, Siqin Feng, Zhen’ge Chang, Yakun Zhao, Yanbo Liu, Jia Fu, Yijie Liu, Siqi Tang, Yitao Han, Shuyang Zhang, and et al. 2022. "Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease" Nutrients 14, no. 19: 4013. https://doi.org/10.3390/nu14194013
APA StyleChen, Y., Feng, S., Chang, Z., Zhao, Y., Liu, Y., Fu, J., Liu, Y., Tang, S., Han, Y., Zhang, S., & Fan, Z. (2022). Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease. Nutrients, 14(19), 4013. https://doi.org/10.3390/nu14194013