
The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
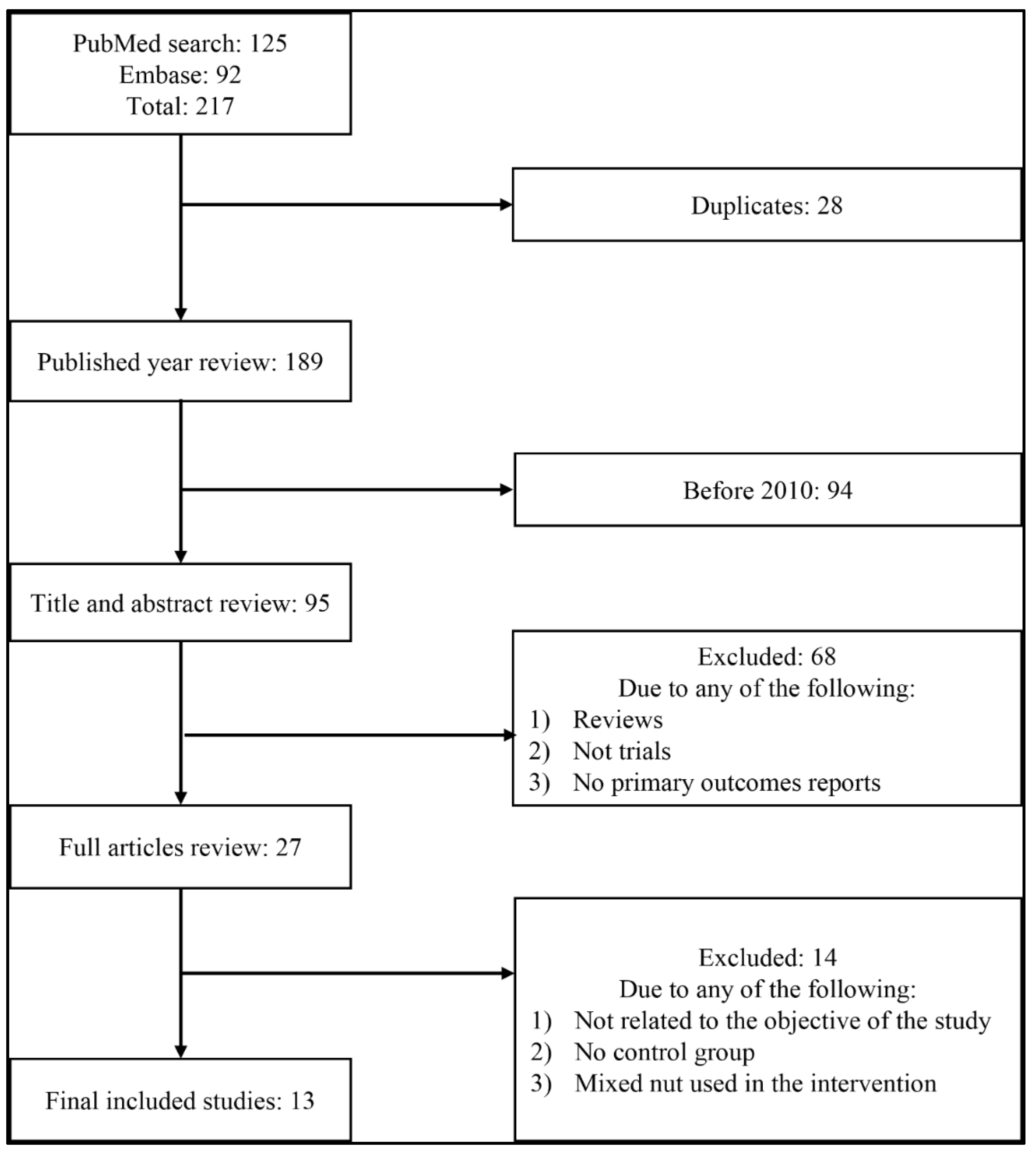
3.1. Study Selection
3.2. Characteristics of the Included Studies
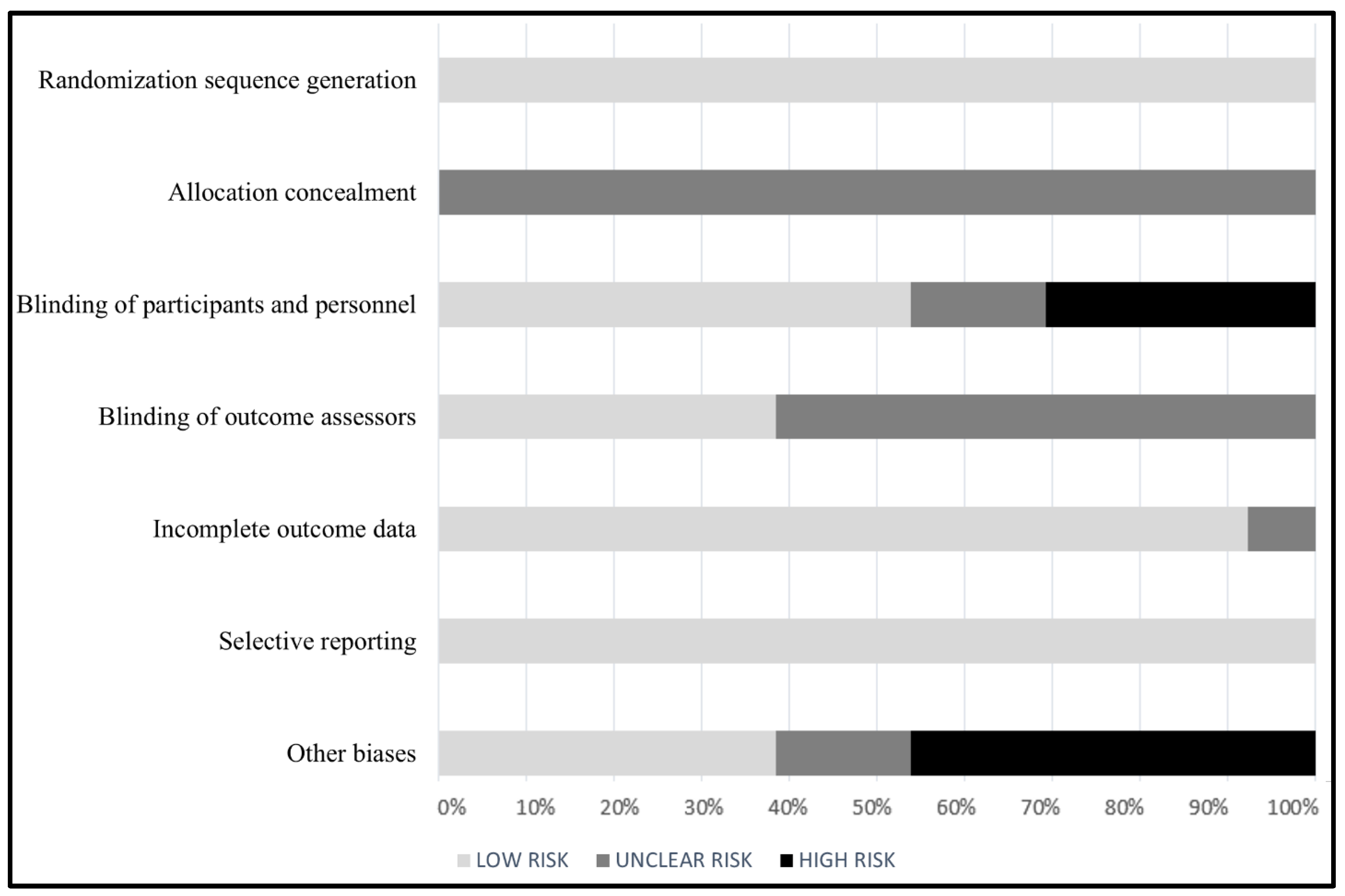
3.3. Quality Assessment
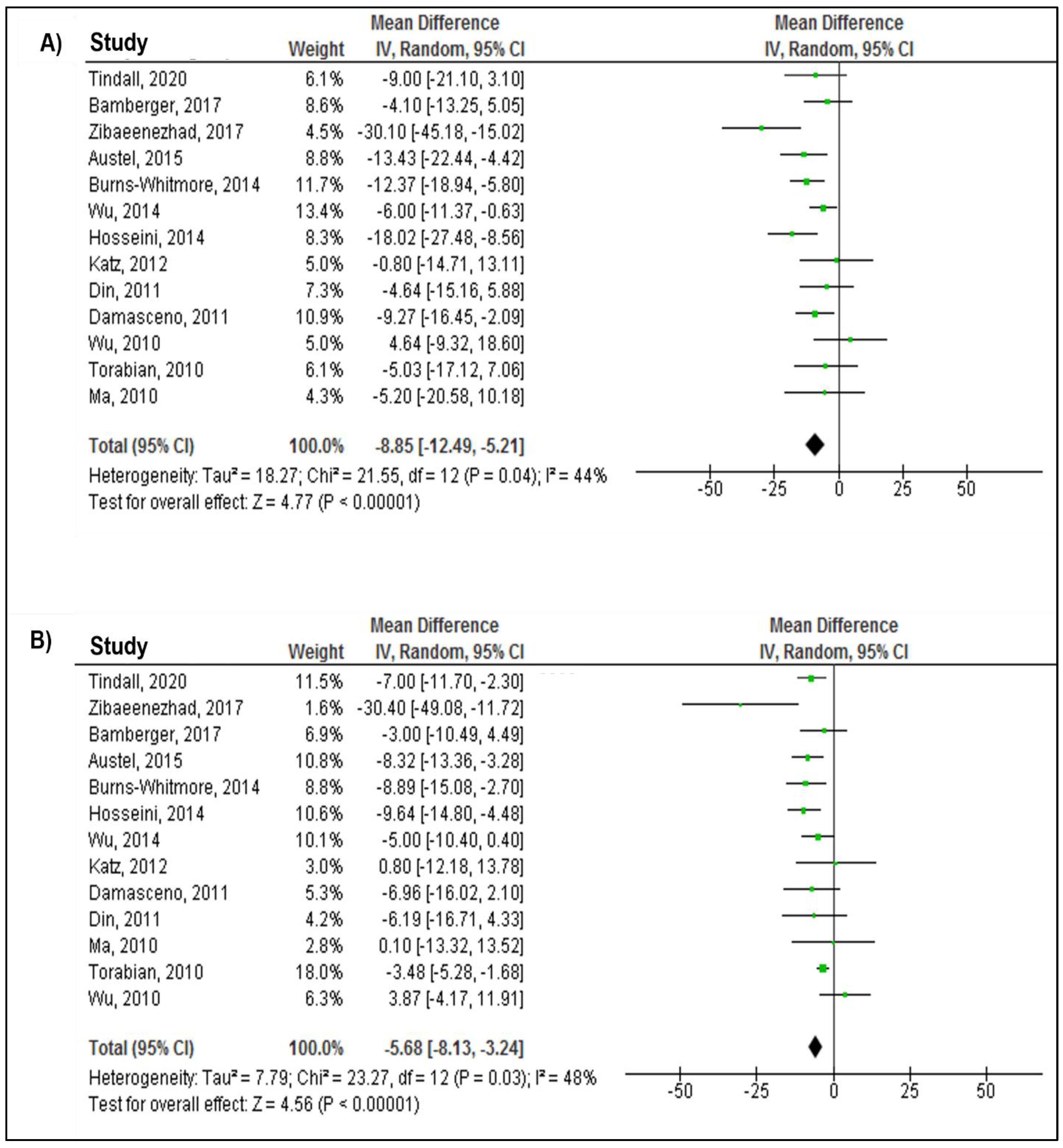
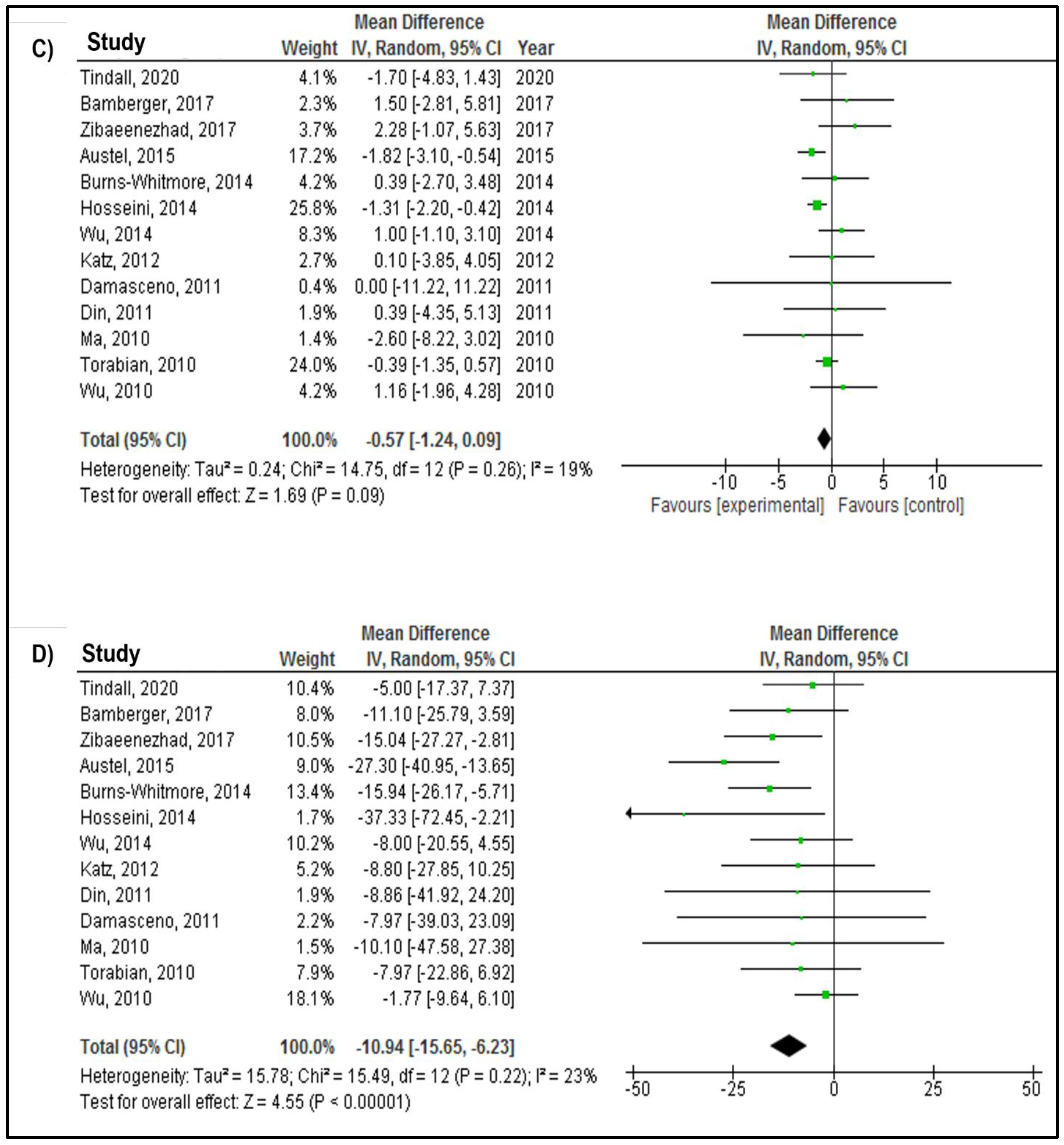
3.4. Meta-Analysis Results
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
3.7. Publication Bias
4. Discussion
Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finegold, J.A.; Asaria, P.; Francis, D.P. Mortality from ischaemic heart disease by country, region, and age: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2013, 168, 934–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlöf, B. Cardiovascular disease risk factors: Epidemiology and risk assessment. Am. J. Cardiol. 2010, 105, 3A–9A. [Google Scholar] [CrossRef]
- Cannon, C.P. Cardiovascular disease and modifiable cardiometabolic risk factors. Clin. Cornerstone 2007, 8, 11–28. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; Zhang, Y.-L.; Hernandez-Ono, A. Metabolic syndrome: Focus on dyslipidemia. Obesity 2006, 14, 41S. [Google Scholar] [CrossRef]
- Ponce, O.J.; Larrea-Mantilla, L.; Hemmingsen, B.; Serrano, V.; Rodriguez-Gutierrez, R.; Spencer-Bonilla, G.; Alvarez-Villalobos, N.; Benkhadra, K.; Haddad, A.; Gionfriddo, M.R. Lipid-lowering agents in older individuals: A systematic review and meta-analysis of randomized clinical trials. J. Clin. Endocrinol. Metab. 2019, 104, 1585–1594. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-B.; Kim, K.; Kim, C.; Kang, S.-J.; Kim, H.J.; Yoon, S.; Shin, Y.-A. Effects of exercise on the body composition and lipid profile of individuals with obesity: A systematic review and meta-analysis. J. Obes. Metab. Syndr. 2019, 28, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, H.; Zhu, L.; Kord-Varkaneh, H.; Santos, H.O.; Tinsley, G.M.; Fu, P. Effects of intermittent fasting and energy-restricted diets on lipid profile: A systematic review and meta-analysis. Nutrition 2020, 77, 110801. [Google Scholar] [CrossRef] [PubMed]
- Enriquez Guerrero, A.; San Mauro Martin, I.; Garicano Vilar, E.; Camina Martin, M.A. Effectiveness of an intermittent fasting diet versus continuous energy restriction on anthropometric measurements, body composition and lipid profile in overweight and obese adults: A meta-analysis. Eur. J. Clin. Nutr. 2021, 75, 1024–1039. [Google Scholar] [CrossRef]
- Zhan, S.; Ho, S.C. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am. J. Clin. Nutr. 2005, 81, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Riccardi, G.; Giacco, R.; Rivellese, A. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin. Nutr. 2004, 23, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Basciano, H.; Federico, L.; Adeli, K. Fructose, insulin resistance, and metabolic dyslipidemia. Nutr. Metab. 2005, 2, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Song, S.J.; Lee, J.E.; Paik, H.-Y.; Park, M.S.; Song, Y.J. Dietary patterns based on carbohydrate nutrition are associated with the risk for diabetes and dyslipidemia. Nutr. Res. Pract. 2012, 6, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magriplis, E.; Marakis, G.; Kotopoulou, S.; Naska, A.; Michas, G.; Micha, R.; Panagiotakos, D.; Zampelas, A. Trans fatty acid intake increases likelihood of dyslipidemia especially among individuals with higher saturated fat consumption. Rev. Cardiovasc. Med. 2022, 23, 130. [Google Scholar] [CrossRef]
- Ghobadi, S.; Hassanzadeh-Rostami, Z.; Mohammadian, F.; Zare, M.; Faghih, S. Effects of canola oil consumption on lipid profile: A systematic review and meta-analysis of randomized controlled clinical trials. J. Am. Coll. Nutr. 2019, 38, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Peou, S.; Milliard-Hasting, B.; Shah, S.A. Impact of avocado-enriched diets on plasma lipoproteins: A meta-analysis. J. Clin. Lipidol. 2016, 10, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, Y.; Levin, S.M.; Barnard, N.D. Association between plant-based diets and plasma lipids: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 683–698. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Zheng, J.; Yang, B.; Jiang, J.; Fu, Y.; Li, D. Effects of vegetarian diets on blood lipids: A systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2015, 4, e002408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemler, E.C.; Hu, F.B. Plant-based diets for cardiovascular disease prevention: All plant foods are not created equal. Curr. Atheroscler. Rep. 2019, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalam, M.; Sathe, S.K. Chemical composition of selected edible nut seeds. J. Agric. Food Chem. 2006, 54, 4705–4714. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Estruch, R. Nut consumption and age-related disease. Maturitas 2016, 84, 11–16. [Google Scholar] [CrossRef]
- Fischer, S.; Glei, M. Potential health benefits of nuts. Ernaehrungs Umsch. Int. 2013, 60, 206–215. [Google Scholar]
- Del Gobbo, L.C.; Falk, M.C.; Feldman, R.; Lewis, K.; Mozaffarian, D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: Systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am. J. Clin. Nutr. 2015, 102, 1347–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cupino, A.; Fraser, G.; Knutsen, S.; Knutsen, R.; Heskey, C.; Sabaté, J.; Shavlik, D. Are total omega-3 and omega-6 polyunsaturated fatty acids predictors of fatal stroke in the Adventist Health Study 2 prospective cohort? PLoS ONE 2022, 17, e0274109. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.; Angove, M.J.; Tucci, J.; Dennis, C. Walnuts (Juglans regia) chemical composition and research in human health. Crit. Rev. Food Sci. Nutr. 2016, 56, 1231–1241. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.A.; Oliveira, I.; Sousa, A.; Valentão, P.; Andrade, P.B.; Ferreira, I.C.; Ferreres, F.; Bento, A.; Seabra, R.; Estevinho, L. Walnut (Juglans regia L.) leaves: Phenolic compounds, antibacterial activity and antioxidant potential of different cultivars. Food Chem. Toxicol. 2007, 45, 2287–2295. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M. Walnuts decrease risk of cardiovascular disease: A summary of efficacy and biologic mechanisms. J. Nutr. 2014, 144, 547S–554S. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Hernández-Alonso, P.; Drouin-Chartier, J.-P.; Ruiz-Canela, M.; Razquin, C.; Toledo, E.; Li, J.; Dennis, C.; Wittenbecher, C.; Corella, D. Walnut consumption, plasma metabolomics, and risk of type 2 diabetes and cardiovascular disease. J. Nutr. 2021, 151, 303–311. [Google Scholar] [CrossRef]
- Banel, D.K.; Hu, F.B. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: A meta-analysis and systematic review. Am. J. Clin. Nutr. 2009, 90, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Li, J.; Hu, F.B.; Salas-Salvadó, J.; Tobias, D.K. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: An updated meta-analysis and systematic review of controlled trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Din, J.N.; Aftab, S.M.; Jubb, A.W.; Carnegy, F.H.; Lyall, K.; Sarma, J.; Newby, D.E.; Flapan, A.D. Effect of moderate walnut consumption on lipid profile, arterial stiffness and platelet activation in humans. Eur. J. Clin. Nutr. 2011, 65, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Davidhi, A.; Ma, Y.; Kavak, Y.; Bifulco, L.; Njike, V.Y. Effects of walnuts on endothelial function in overweight adults with visceral obesity: A randomized, controlled, crossover trial. J. Am. Coll. Nutr. 2012, 31, 415–423. [Google Scholar] [CrossRef]
- Burns-Whitmore, B.; Haddad, E.; Sabaté, J.; Rajaram, S. Effects of supplementing n-3 fatty acid enriched eggs and walnuts on cardiovascular disease risk markers in healthy free-living lacto-ovo-vegetarians: A randomized, crossover, free-living intervention study. Nutr. J. 2014, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.; Jamshidi, L.; Mehrzadi, S.; Mohammad, K.; Najmizadeh, A.R.; Alimoradi, H.; Huseini, H.F. Effects of Juglans regia L. leaf extract on hyperglycemia and lipid profiles in type two diabetic patients: A randomized double-blind, placebo-controlled clinical trial. J. Ethnopharmacol. 2014, 152, 451–456. [Google Scholar] [CrossRef]
- Wu, L.; Piotrowski, K.; Rau, T.; Waldmann, E.; Broedl, U.C.; Demmelmair, H.; Koletzko, B.; Stark, R.G.; Nagel, J.M.; Mantzoros, C.S. Walnut-enriched diet reduces fasting non-HDL-cholesterol and apolipoprotein B in healthy Caucasian subjects: A randomized controlled cross-over clinical trial. Metabolism 2014, 63, 382–391. [Google Scholar] [CrossRef]
- Austel, A.; Ranke, C.; Wagner, N.; Görge, J.; Ellrott, T. Weight loss with a modified Mediterranean-type diet using fat modification: A randomized controlled trial. Eur. J. Clin. Nutr. 2015, 69, 878–884. [Google Scholar] [CrossRef]
- Zibaeenezhad, M.J.; Farhadi, P.; Attar, A.; Mosleh, A.; Amirmoezi, F.; Azimi, A. Effects of walnut oil on lipid profiles in hyperlipidemic type 2 diabetic patients: A randomized, double-blind, placebo-controlled trial. Nutr. Diabetes 2017, 7, e259. [Google Scholar] [CrossRef] [Green Version]
- Bamberger, C.; Rossmeier, A.; Lechner, K.; Wu, L.; Waldmann, E.; Stark, R.G.; Altenhofer, J.; Henze, K.; Parhofer, K.G. A walnut-enriched diet reduces lipids in healthy Caucasian subjects, independent of recommended macronutrient replacement and time point of consumption: A prospective, randomized, controlled trial. Nutrients 2017, 9, 1097. [Google Scholar] [CrossRef]
- Tindall, A.M.; Kris-Etherton, P.M.; Petersen, K.S. Replacing saturated fats with unsaturated fats from walnuts or vegetable oils lowers atherogenic lipoprotein classes without increasing lipoprotein (a). J. Nutr. 2020, 150, 818–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torabian, S.; Haddad, E.; Cordero-MacIntyre, Z.; Tanzman, J.; Fernandez, M.; Sabate, J. Long-term walnut supplementation without dietary advice induces favorable serum lipid changes in free-living individuals. Eur. J. Clin. Nutr. 2010, 64, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Pan, A.; Yu, Z.; Qi, Q.; Lu, L.; Zhang, G.; Yu, D.; Zong, G.; Zhou, Y.; Chen, X. Lifestyle counseling and supplementation with flaxseed or walnuts influence the management of metabolic syndrome. J. Nutr. 2010, 140, 1937–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Njike, V.Y.; Millet, J.; Dutta, S.; Doughty, K.; Treu, J.A.; Katz, D.L. Effects of walnut consumption on endothelial function in type 2 diabetic subjects: A randomized controlled crossover trial. Diabetes Care 2010, 33, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Damasceno, N.R.T.; Pérez-Heras, A.; Serra, M.; Cofán, M.; Sala-Vila, A.; Salas-Salvadó, J.; Ros, E. Crossover study of diets enriched with virgin olive oil, walnuts or almonds. Effects on lipids and other cardiovascular risk markers. Nutr. Metab. Cardiovasc. Dis. 2011, 21, S14–S20. [Google Scholar] [CrossRef]
- Almario, R.U.; Vonghavaravat, V.; Wong, R.; Kasim-Karakas, S.E. Effects of walnut consumption on plasma fatty acids and lipoproteins in combined hyperlipidemia. Am. J. Clin. Nutr. 2001, 74, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapsell, L.C.; Batterham, M.; Teuss, G.; Tan, S.Y.; Dalton, S.; Quick, C.J.; Gillen, L.J.; Charlton, K.E. Long-term effects of increased dietary polyunsaturated fat from walnuts on metabolic parameters in type II diabetes. Eur. J. Clin. Nutr. 2009, 63, 1008–1015. [Google Scholar] [CrossRef] [Green Version]
- Mukuddem-Petersen, J.; Stonehouse, W.; Jerling, J.C.; Hanekom, S.M.; White, Z. Effects of a high walnut and high cashew nut diet on selected markers of the metabolic syndrome: A controlled feeding trial. Br. J. Nutr. 2007, 97, 1144–1153. [Google Scholar] [CrossRef]
- Schutte, A.E.; Van Rooyen, J.M.; Huisman, H.W.; Mukuddem-Petersen, J.; Oosthuizen, W.; Hanekom, S.M.; Jerling, J.C. Modulation of baroreflex sensitivity by walnuts versus cashew nuts in subjects with metabolic syndrome. Am. J. Hypertens. 2006, 19, 629–636. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Gillen, L.J.; Patch, C.S.; Batterham, M.; Owen, A.; Baré, M.; Kennedy, M. Including walnuts in a low-fat/modified-fat diet improves HDL cholesterol-to-total cholesterol ratios in patients with type 2 diabetes. Diabetes Care 2004, 27, 2777–2783. [Google Scholar] [CrossRef] [Green Version]
- Aronis, K.N.; Vamvini, M.T.; Chamberland, J.P.; Sweeney, L.L.; Brennan, A.M.; Magkos, F.; Mantzoros, C.S. Short-term walnut consumption increases circulating total adiponectin and apolipoprotein A concentrations, but does not affect markers of inflammation or vascular injury in obese humans with the metabolic syndrome: Data from a double-blinded, randomized, placebo-controlled study. Metabolism 2012, 61, 577–582. [Google Scholar]
- Binici, H.İ.; Şat, İ.G.; Aoudeh, E. Nutritional Composition and Health Benefits of Walnut and its Products. Atatürk Üniversitesi Ziraat Fakültesi Derg. 2021, 52, 224–230. [Google Scholar] [CrossRef]
- Muñoz, S.; Merlos, M.; Zambón, D.; Rodríguez, C.; Sabaté, J.; Ros, E.; Laguna, J.C. Walnut-enriched diet increases the association of LDL from hypercholesterolemic men with human HepG2 cells. J. Lipid Res. 2001, 42, 2069–2076. [Google Scholar] [CrossRef]
- Hadi, A.; Asbaghi, O.; Kazemi, M.; Haghighian, H.K.; Pantovic, A.; Ghaedi, E.; Abolhasani Zadeh, F. Consumption of pistachio nuts positively affects lipid profiles: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Asbaghi, O.; Moodi, V.; Hadi, A.; Eslampour, E.; Shirinbakhshmasoleh, M.; Ghaedi, E.; Miraghajani, M. The effect of almond intake on lipid profile: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2021, 12, 1882–1896. [Google Scholar] [CrossRef]
- Perna, S.; Giacosa, A.; Bonitta, G.; Bologna, C.; Isu, A.; Guido, D.; Rondanelli, M. Effects of hazelnut consumption on blood lipids and body weight: A systematic review and Bayesian meta-analysis. Nutrients 2016, 8, 747. [Google Scholar] [CrossRef]
- Ogah, A.O.; Ezeani, O.E.; Nwobi, S.C.; Ikelle, I.I. Physical and Mechanical Properties of Agro-Waste Filled Recycled High Density Polyethylene Biocomposites. South Asian Res. J. Eng. Tech. 2022, 4, 55–62. [Google Scholar] [CrossRef]
- Brennan, A.M.; Sweeney, L.L.; Liu, X.; Mantzoros, C.S. Walnut consumption increases satiation but has no effect on insulin resistance or the metabolic profile over a 4-day period. Obesity 2010, 18, 1176–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamberger, C.; Rossmeier, A.; Lechner, K.; Wu, L.; Waldmann, E.; Fischer, S.; Stark, R.G.; Altenhofer, J.; Henze, K.; Parhofer, K.G. A walnut-enriched diet affects gut microbiome in healthy caucasian subjects: A randomized, controlled trial. Nutrients 2018, 10, 244. [Google Scholar] [CrossRef] [Green Version]
- Holscher, H.D.; Guetterman, H.M.; Swanson, K.S.; An, R.; Matthan, N.R.; Lichtenstein, A.H.; Novotny, J.A.; Baer, D.J. Walnut consumption alters the gastrointestinal microbiota, microbially derived secondary bile acids, and health markers in healthy adults: A randomized controlled trial. J. Nutr. 2018, 148, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8. [Google Scholar] [CrossRef]
- Afshin, A.; Babalola, D.; Mclean, M.; Yu, Z.; Ma, W.; Chen, C.Y.; Arabi, M.; Mozaffarian, D. Information technology and lifestyle: A systematic evaluation of internet and mobile interventions for improving diet, physical activity, obesity, tobacco, and alcohol use. J. Am. Heart Assoc. 2016, 5, e003058. [Google Scholar] [CrossRef]
- Costa, J.; Carrapatoso, I.; Oliveira, M.; Mafra, I. Walnut allergens: Molecular characterization, detection and clinical relevance. Clin. Exp. Allergy 2014, 44, 319–341. [Google Scholar] [CrossRef]
- Mateș, L.; Popa, D.-S.; Rusu, M.E.; Fizeșan, I.; Leucuța, D. Walnut intake interventions targeting biomarkers of metabolic syndrome and inflammation in middle-aged and older adults: A systematic review and meta-analysis of randomized controlled trials. Antioxidants 2022, 11, 1412. [Google Scholar] [CrossRef]
- Domènech, M.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.; Valls-Pedret, C.; Cofán, M.; López, A.; Sala-Vila, A.; Calvo, C.; Rajaram, S. Effect of a walnut diet on office and 24-hour ambulatory blood pressure in elderly individuals: Findings from the WAHA randomized trial. Hypertension 2019, 73, 1049–1057. [Google Scholar] [CrossRef]
- Zibaeenezhad, M.; Aghasadeghi, K.; Hakimi, H.; Yarmohammadi, H.; Nikaein, F. The effect of walnut oil consumption on blood sugar in patients with diabetes mellitus type 2. Int. J. Endocrinol. Metab. 2016, 14, e34889. [Google Scholar] [PubMed] [Green Version]
- Cahoon, D.; Shertukde, S.P.; Avendano, E.E.; Tanprasertsuk, J.; Scott, T.M.; Johnson, E.J.; Chung, M.; Nirmala, N. Walnut intake, cognitive outcomes and risk factors: A systematic review and meta-analysis. Ann. Med. 2021, 53, 972–998. [Google Scholar] [CrossRef]
- Liu, X.; Guasch-Ferré, M.; Tobias, D.K.; Li, Y. Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in US Adults. Nutrients 2021, 13, 2699. [Google Scholar] [CrossRef]
- Ros, E. Health benefits of nut consumption. Nutrients 2010, 2, 652–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitok, E.; Rajaram, S.; Jaceldo-Siegl, K.; Oda, K.; Sala-Vila, A.; Serra-Mir, M.; Ros, E.; Sabaté, J. Effects of long-term walnut supplementation on body weight in free-living elderly: Results of a randomized controlled trial. Nutrients 2018, 10, 1317. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Sample Size (n) | Participants | Mean Age (yrs) | Mean BMI (kg/m2) | Gender (M%, F %) | Mean Baseline Lipids (mg/dL) | Trial Duration (wks) | Intervention | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | Dose | Control | ||||||||||
| Tindall, 2020 [42] | USA | Crossover | 34 | Cardiovascular disease patients | 44 | 30 | 62, 38 | TC: 182 LDL-C: 115 HDL-C: 45 TG: 111 | 18 | Walnut diet | 57–99 g/d | walnut fatty acid–matched diet that did not contain walnut |
| Bamberger, 2017 [41] | Germany | Crossover | 194 | Healthy | 63 | 25 | 31, 69 | TC: 232 LDL-C: 146 HDL-C: 69 TG: 101 | 16 | Walnut-enriched diet (shelled walnut) | 43 g/d | Nut-free control diet |
| Zibaeenezhad, 2017 [40] | Iran | Parallel | 100 | Type II diabetic patients | 56 | 27 | 59, 41 | TC: 234 LDL-C: 144 HDL-C: 48 TG: 194 | 12 | 4 walnut oil capsules containing Persian walnut (Juglans Regia L.) oil | 15 cc/d | 4 placebo capsules containing distilled water |
| Austel, 2015 [39] | Germany | Crossover | 212 | Overweight/Obese | 52 | 30 | 18, 82 | TC: 206 LDL-C: 134 HDL-C: 62 TG: 125 | 12 | Walnuts and walnut oil | Two portions | A modified Mediterranean-type diet |
| Wu, 2014 [38] | Germany | Crossover | 40 | Healthy | 60 | 25 | 25, 75 | TC: 222 LDL-C: 135 HDL-C: 72 TG: 89 | 16 | walnut-enriched diet (shelled walnuts) | 43 g/d | Western diet |
| Hosseini, 2014 [37] | Iran | Parallel | 61 | Type II diabetic patients | 55 | 27 | 46, 54 | TC: 192 LDL-C: 105 HDL-C: 40 TG: 162 | 12 | Persian Juglans regia leaves extract powder capsule before meal | 100 mg twice a day | Placebo capsule |
| Burns-Whitmore, 2014 [36] | USA | Crossover | 20 | Healthy | 38 | 23 | 20, 80 | TC: 185 LDL-C: 109 HDL-C: 49 TG: 100 | 16 | Walnuts eaten raw or used on salads, muffins, etc. | 28 g/d | Standard egg diet |
| Katz, 2012 [35] | USA | Crossover | 46 | Overweight/Obese | 57 | 33 | 39, 61 | TC: 205 LDL-C: 121 HDL-C: 53 TG: 157 | 16 | Walnut-enriched ad libitum diet (shelled, unroasted English walnuts) | 56 g/d | Ad libitum diet without walnuts |
| Din, 2011 [34] | UK | Crossover | 30 | Healthy | 23 | 25 | Males | TC: 178 LDL-C: 104 HDL-C: 51 TG: 108 | 8 | Walnut supplements | 15 g/d | No walnuts |
| Damasceno, 2011 [46] | Spain | Crossover | 18 | Hypercholesteremic | 56 | 26 | 50, 50 | TC: 272 LDL-C: 196 HDL-C: 63 TG: 120 | 12 | Spanish grown walnuts (Serr/Chandler variety) | 40–65 g/d | Virgin olive oil-based diet |
| Wu, 2010 [44] | China | Parallel | 189 | Metabolic syndrome patients | 48 | 25 | 56, 44 | TC: 224 LDL-C: 166 HDL-C: 50 TG: 176 | 12 | Walnuts supplementation | 30 g/d | Healthy lifestyle counseling diet |
| Torabian, 2010 [43] | USA | Crossover | 87 | Healthy | 54 | 27 | 44, 56 | TC: 220 LDL-C: 131 HDL-C: 59 TG: 123 | 52 | Walnut-supplemented diet | 28–64 g/d | Habitual (control) diet |
| Ma, 2010 [45] | USA | Crossover | 24 | Type II diabetic patients | 58 | 33 | 42, 58 | TC: 183 LDL-C: 103 HDL-C: 56 TG: 124 | 8 | Walnut-enriched ad libitum (shelled, unroasted English walnuts) | 56 g/d | Ad libitum diet without walnuts |
| WMD (95% CI) | p for Effect | p for Heterogeneity | I2 | ||
|---|---|---|---|---|---|
| Subgroups for TC | |||||
| Overall effect | −8.85 (−12.49, −5.21) | <0.00001 | 0.04 | 44% | |
| Health status | Healthy | −7.24 (−10.65, −3.82) | <0.0001 | 0.50 | 0% |
| With comorbidities | −10.45 (−16.58, −4.32) | 0.0008 | 0.02 | 57% | |
| Mean age | ≥55 | −9.80 (−15.57, −4.04) | 0.0009 | 0.02 | 60% |
| <55 | −8.32 (−13.09, −3.55) | 0.0006 | 0.25 | 25% | |
| Mean BMI | >25 | −12.98 (−19.19, −6.77) | <0.0001 | 0.06 | 52% |
| ≤25 | −6.50 (−9.75, −3.25) | <0.0001 | 0.42 | 0% | |
| Gender distribution | Majority females | −8.03 (−11.58, −4.48) | <0.00001 | 0.36 | 9% |
| Majority males or almost equal gender distribution | −10.01 (−16.70, −3.31) | 0.003 | 0.02 | 61% | |
| Baseline TC | ≥200 | −7.74 (−12.84, −2.63) | 0.003 | 0.03 | 54% |
| <200 | −11.17 (−15.71, −6.64) | <0.00001 | 0.36 | 7% | |
| Trial duration | >12 weeks | −7.26 (−10.62, −3.90) | <0.0001 | 0.55 | 0% |
| 12 weeks or less | −10.88 (−17, 48, −4.28) | 0.001 | 0.02 | 61% | |
| Subgroups for LDL-C | |||||
| Overall effect | −5.68 (−8.13, −3.24) | <0.00001 | 0.03 | 48% | |
| Health status | Healthy | −4.01 (−5.60, −2.42) | <0.00001 | 0.54 | 0% |
| With comorbidities | −6.19 (−10.49, −1.90) | 0.005 | 0.02 | 58% | |
| Mean age | ≥55 | −6.32 (−10.75, −1.90) | 0.005 | 0.09 | 45% |
| <55 | −5.24 (−8.28, −2.20) | 0.0007 | 0.06 | 53% | |
| Mean BMI | >25 | −8.28 (−11.94, −4.63) | <0.00001 | 0.16 | 37% |
| ≤25 | −3.76 (−5.91, −1.60) | 0.0006 | 0.33 | 14% | |
| Gender distribution | Majority females | −6.04 (−8.82, −3.26) | <0.0001 | 0.51 | 0% |
| Majority males or almost equal gender distribution | −6.04 (−10.03, −2.05) | 0.003 | 0.006 | 67% | |
| Baseline LDL-C | ≥130 | −4.94 (−8.52, −1.35) | 0.007 | 0.02 | 60% |
| <130 | −7.43 (−10.21, −4.65) | <0.00001 | 0.58 | 0% | |
| Trial duration | >12 weeks | −4.21 (−5.72, −2.70) | <0.00001 | 0.42 | 0% |
| 12 weeks or less | −6.69 (−11.83, −1.54) | 0.01 | 0.02 | 61% | |
| Subgroups for HDL-C | |||||
| Overall effect | −0.57 (−1.24, 0.09) | 0.09 | 0.26 | 19% | |
| Health status | Healthy | −0.04 (-.85, 0.77) | 0.92 | 0.73 | 0% |
| With comorbidities | −1.07 (-.1.91, −0.23) | 0.01 | 0.32 | 14% | |
| Mean age | ≥55 | −0.02 (−1.39, −1.34) | 0.97 | 0.17 | 33% |
| <55 | −0.74 (−1.57, 0.09) | 0.08 | 0.33 | 13% | |
| Mean BMI | >25 | −1.22 (−2.04, −0.40) | 0.004 | 0.34 | 11% |
| ≤25 | −0.01 (−0.79, 0.76) | 0.97 | 0.76 | 0% | |
| Gender distribution | Majority females | −0.37 (−1.77, 1.02) | 0.60 | 0.19 | 33% |
| Majority males or almost equal gender distribution | −0.59 (−1.39, 0.21) | 0.15 | 0.30 | 17% | |
| Baseline HDL-C | >50 | −0.58 (−1.36, 0.21) | 0.15 | 0.37 | 8% |
| ≤50 | −0.26 (−1.70, 1.19) | 0.73 | 0.14 | 42% | |
| Trial duration | >12 weeks | −0.15 (−0.93, 0.63) | 0.71 | 0.70 | 0% |
| 12 weeks or less | −0.91 (−1.39, 0.11) | 0.08 | 0.24 | 25% | |
| Subgroups for TG | |||||
| Overall effect | −10.94 (−15.65, −6.23) | <0.00001 | 0.22 | 23% | |
| Health status | Healthy | −11.50 (−17.71, −5.29) | 0.0003 | 0.87 | 0% |
| With comorbidities | −11.92 (−20.11, −3.73) | 0.004 | 0.05 | 50% | |
| Mean age | ≥55 | −11.87 (18.46, −5.27) | 0.0004 | 0.83 | 0% |
| <55 | −10.87 (−19.14, −2.61) | 0.010 | 0.03 | 59% | |
| Mean BMI | >25 | −15.12 (−23.91, −6.33) | 0.0007 | 0.17 | 36% |
| ≤25 | −7.81 (−12.64, −2.97) | 0.002 | 0.56 | 0% | |
| Gender distribution | Majority females | −14.72 (−20.62, −8.81) | <0.00001 | 0.41 | 2% |
| Majority males or almost equal gender distribution | −6.96 (−12.50, −1.42) | 0.01 | 0.39 | 5% | |
| Baseline TG | ≥150 | −10.17 (−20.98, 0.64) | 0.07 | 0.10 | 52% |
| <150 | −12.45 (−17.48, −7.43) | <0.00001 | 0.49 | 0% | |
| Trial duration | >12 weeks | −10.12 (−15.51, −4.72) | 0.0002 | 0.83 | 0% |
| 12 weeks or less | −14.17 (−24.74, −3.60) | 0.009 | 0.04 | 55% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshahrani, S.M.; Mashat, R.M.; Almutairi, D.; Mathkour, A.; Alqahtani, S.S.; Alasmari, A.; Alzahrani, A.H.; Ayed, R.; Asiri, M.Y.; Elsherif, A.; et al. The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 4460. https://doi.org/10.3390/nu14214460
Alshahrani SM, Mashat RM, Almutairi D, Mathkour A, Alqahtani SS, Alasmari A, Alzahrani AH, Ayed R, Asiri MY, Elsherif A, et al. The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2022; 14(21):4460. https://doi.org/10.3390/nu14214460
Chicago/Turabian StyleAlshahrani, Saeed Mastour, Reham M. Mashat, Diaa Almutairi, Alaa Mathkour, Sahar Saad Alqahtani, Amirah Alasmari, Abdullah Hassan Alzahrani, Reem Ayed, Mohammed Yahya Asiri, Alsanussi Elsherif, and et al. 2022. "The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 14, no. 21: 4460. https://doi.org/10.3390/nu14214460
APA StyleAlshahrani, S. M., Mashat, R. M., Almutairi, D., Mathkour, A., Alqahtani, S. S., Alasmari, A., Alzahrani, A. H., Ayed, R., Asiri, M. Y., Elsherif, A., & Alsabaani, A. (2022). The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 14(21), 4460. https://doi.org/10.3390/nu14214460