
Quality Appraisal of Nutritional Guidelines to Prevent, Diagnose, and Treat Malnutrition in All Its Forms during Pregnancy

 , , , , ,
, , , , ,  , ,
, ,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
2.2. Search Strategy and Studies Selection
2.3. Quality Assessment
2.4. Data Analysis
3. Results
3.1. Quality of Guidelines According to the AGREE II Domains
3.1.1. Scope and Purpose Domain
3.1.2. Stakeholder Involvement
3.1.3. Rigor of Development
3.1.4. Clarity of Presentation
3.1.5. Applicability
3.1.6. Editorial Independence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of Lifetime Health Around the Time of Conception: Causes and Consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG Int. J. Obs. Gynaecol. 2019, 126, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; Von Kries, R. Gestational weight gain and long-term postpartum weight retention. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Singh, S.H.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; West, K.P.; Black, R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015, 66, 22–33. [Google Scholar] [CrossRef]
- International Weight Management in Pregnancy (i-WIP) Collaborative Group. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. BMJ 2017, 358, j3119. [Google Scholar]
- Yamamoto, J.M.; Kellett, J.E.; Balsells, M.; García-Patterson, A.; Hadar, E.; Solà, I.; Gich, I.; van der Beek, E.M.; Castañeda-Gutiérrez, E.; Heinonen, S. Gestational diabetes mellitus and diet: A systematic review and meta-analysis of randomized controlled trials examining the impact of modified dietary interventions on maternal glucose control and neonatal birth weight. Diabetes Care 2018, 41, 1346–1361. [Google Scholar] [CrossRef] [Green Version]
- Ancira-Moreno, M.; O’Neill, M.S.; Rivera-Dommarco, J.Á.; Batis, C.; Rodríguez-Ramírez, S.; Sánchez, B.N.; Castillo-Castrejón, M.; Vadillo-Ortega, F. Dietary patterns and diet quality during pregnancy and low birthweight: The PRINCESA cohort. Matern. Child Nutr. 2020, 16, e12972. [Google Scholar] [CrossRef] [Green Version]
- Gete, D.G.; Waller, M.; Mishra, G.D. Effects of maternal diets on preterm birth and low birth weight: A systematic review. Br. J. Nutr. 2020, 123, 446–461. [Google Scholar] [CrossRef]
- Li, M.; Grewal, J.; Hinkle, S.N.; Yisahak, S.F.; Grobman, W.A.; Newman, R.B.; Skupski, D.W.; Chien, E.K.; Wing, D.A.; Grantz, K.L.; et al. Healthy dietary patterns and common pregnancy complications: A prospective and longitudinal study. Am. J. Clin. Nutr. 2021, 114, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Caut, C.; Leach, M.; Steel, A. Dietary guideline adherence during preconception and pregnancy: A systematic review. Matern. Child Nutr. 2020, 16, e12916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joanna Briggs Institute. Joana Briggs Institute Revewer’s Manual: 2015 Edition/Supplement; The Johanna Briggs Institute: Adelaide, Australia, 2015; pp. 6–23. [Google Scholar]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in healthcare. Prev. Med. 2010, 51, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press US: Washington, DC, USA, 2009. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- ACOG Practice Bulletin No 156: Obesity in Pregnancy. Obs. Gynecol. 2015, 126, e112–e126. [CrossRef]
- American Diabetes Association. 12. Management of diabetes in pregnancy. Diabetes Care. 2015, 38, S77–S79. [Google Scholar] [CrossRef] [Green Version]
- Siega-Riz, A.M.; King, J.C. Position of the American Dietetic Association and American Society for Nutrition: Obesity, reproduction, and pregnancy outcomes. J. Am. Diet. Assoc. 2009, 109, 918–927. [Google Scholar]
- Department of Health. Clinical Practice Guidelines: Pregnancy Care; Australian Government Department of Health: Canberra, Australia, 2018; pp. 9–302.
- Bomba, O.D.; Hirnle, L.; Kalinka, J.; Seremak, M.A. Folate supplementation during the preconception period, pregnancy and puerperium. Polish Society of Gynecologists and Obstetricians Guidelines. Ginekol. Polska. 2017, 88, 633–636. [Google Scholar] [CrossRef] [Green Version]
- Cetin, I.; Assandro, P.; Massari, M.; Sagone, A.; Gennaretti, R.; Donzelli, G.; Knowles, A.; Monasta, L.; Davanzo, R.; Working Group on Breastfeeding; et al. Breastfeeding during pregnancy: Position paper of the Italian Society of Perinatal Medicine and the Task Force on Breastfeeding, Ministry of Health, Italy. J. Hum. Lact. 2014, 30, 20–27. [Google Scholar] [CrossRef]
- Charzewska, J.; Chlebna-Sokół, D.; Chybicka, A.; Czech-Kowalska, J.; Dobrzańska, A.; Helwich, E.; Imiela, J.R.; Karczmarewicz, E.; Ksiazyk, J.B.; Lewiński, A.; et al. Recommendations of prophylaxis of vitamin D deficiency in Poland (2009). Med. Wieku Rozw. 2010, 14, 218–223. [Google Scholar]
- Modder, J.; Fitzsimons, K. Management of women with obesity in pregnancy. In CMACE/RCOG Joint Guideline; Public Health Agency: Ottawa, ON, Canada, 2010; pp. 1–29. [Google Scholar]
- Davies, G.A.L.; Maxwell, C.; McLeod, L.; Gagnon, R.; Basso, M.; Bos, H.; Delisle, M.F.; Farine, D.; Hudon, L.; Menticoglou, S.; et al. SOGC Clinical Practice Guidelines: Obesity in pregnancy. No. 239, February 2010. Int. J. Gynaecol. Obstet. 2010, 110, 167–173. [Google Scholar] [CrossRef]
- Davies, G.A.L.; Maxwell, C.; McLeod, L. No. 239-Obesity in Pregnancy. J. Obstet. Gynaecol. Can. 2018, 40, e630–e639. [Google Scholar] [CrossRef] [PubMed]
- Denison, F.C.; Aedla, N.R.; Keag, O.; Hor, K.; Reynolds, R.M.; Milne, A.; Diamond, A.; the Royal College of Obstetricians and Gynaecologists. Care of Women with Obesity in Pregnancy. BJOG 2018, 126, e62–e106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnay, S.; Arena, J.; Lucas, A.; Velasco, I.; Ares, S.; Working Group on Disorders Related to Iodine Deficiency and Thyroid Dysfunction of the Spanish Society of Endocrinology and Nutrition. Iodine supplementation during pregnancy and lactation. Position statement of the working group on disorders related to iodine deficiency and thyroid dysfunction of the Spanish Society of Endocrinology and Nutrition. Endocrinol. Nutr. 2014, 61, 27–34. [Google Scholar] [CrossRef]
- Fitzsimons, K.J.; Modder, J.; Centre for Maternal and Child Enquires. Setting maternity care standards for women with obesity in pregnancy. Semin. Fetal Neonatal Med. 2010, 15, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Fleming, N.; O’Driscoll, T.; Becker, G.; Spitzer, R.F.; Canpago Committee. Adolescent Pregnancy Guidelines. J. Obstet. Gynaecol. Can. 2015, 37, 740–756. [Google Scholar] [CrossRef] [Green Version]
- Haq, A.; Wimalawansa, S.J.; Pludowski, P.; Anouti, F.A. Clinical practice guidelines for vitamin D in the United Arab Emirates. J. Steroid Biochem Mol. Biol. 2018, 175, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Harden, C.L.; Pennell, P.B.; Koppel, B.S.; Hovinga, C.A.; Gidal, B.; Meador, K.J.; Hopp, J.; Ting, T.Y.; Hauser, W.A.; Thurman, D.; et al. American Epilepsy Society. Practice parameter update: Management issues for women with epilepsy--focus on pregnancy (an evidence-based review): Vitamin K, folic acid, blood levels, and breastfeeding: Report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology 2009, 73, 142–149. [Google Scholar]
- Homer, C.S.; Oats, J.; Middleton, P.; Ramson, J.; Diplock, S. Updated clinical practice guidelines on pregnancy care. Med. J. Aust. 2018, 209, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Jacob, C.M.; Killeen, S.L.; McAuliffe, F.M.; Stephenson, J.; Hod, M.; Diaz-Yamal, I.; Malhotra, J.; Mocanu, E.; McIntyre, H.D.; Kihara, A.B.; et al. Prevention of noncommunicable diseases by interventions in the preconception period: A FIGO position paper for action by healthcare practitioners. Int. J. Gynecol. Obstet. 2020, 151, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Koren, G.; Carey, N.; Gagnon, R.; Maxwell, C.; Nulman, I.; Senikas, V. Cancer chemotherapy and pregnancy. J. Obstet. Gynaecol. Can. 2013, 35, 263–278. [Google Scholar] [CrossRef]
- Lausman, A.; Kingdom, J.; Maternal Fetal Medicine Committee. Intrauterine growth restriction: Screening, diagnosis, and management. J. Obstet. Gynaecol. Can. 2013, 35, 741–748. [Google Scholar] [CrossRef]
- Marsh, J.C.W.; Ball, S.E.; Cavenagh, J.; Darbyshire, P.; Dokal, I.; Gordon-Smith, E.C.; Keidan, J.; Laurie, A.; Martin, A.; Mercieca, J.; et al. Guidelines for the diagnosis and management of aplastic anaemia. Br. J. Haematol. 2009, 147, 43–70. [Google Scholar] [CrossRef]
- Maxwell, C.; Gaudet, L.; Cassir, G.; Nowik, C.; Lynne, M.L.; Jacob, C.E.; Walker, M. Guideline No. 391-Pregnancy and Maternal Obesity Part 1: Pre-conception and Prenatal Care. J. Obstet. Gynaecol. Can. 2019, 41, 1623–1640. [Google Scholar] [CrossRef]
- Maxwell, C.; Gaudet, L.; Cassir, G.; Nowik, C.; Lynne, M.L.; Jacob, C.E.; Walker, M. Guideline No. 392-Pregnancy and Maternal Obesity Part 2: Team Planning for Delivery and Postpartum Care. J. Obstet. Gynaecol. Can. 2019, 41, 1660–1675. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo-Garcia, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Muraro, A.; Halken, S.; Arshad, S.H.; Beyer, K.; Dubois, A.E.J.; Du-Toit, G.; Eigenmann, P.A.; Grimshaw, K.E.C.; Hoest, A.; Lack, G.; et al. EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy 2014, 69, 590–601. [Google Scholar] [CrossRef]
- NICE (National Institute for Health and Care Excellence). Antenatal Care for Uncomplicated Pregnancies; NICE: London, UK, 2019; pp. 4–60. [Google Scholar]
- NICE (National Institute of Health and Care Excellence). Diabetes in Pregnancy: Management from Preconception to the Postnatal Period; NICE: London, UK, 2020; pp. 4–39. [Google Scholar]
- NICE (National Institute of Health and Care Excellence). Weight Management before, during and after Pregnancy; NICE: London, UK, 2010; pp. 5–52. [Google Scholar]
- Pavord, S.; Myers, B.; Robinson, S.; Allard, S.; Strong, J.; Oppenheimer, C.; on behalf of the British Committee for Standards in Haematology. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2012, 156, 588–600. [Google Scholar] [CrossRef]
- Piccinini, V.H.; Adamo, K.; Bell, R.; Pereira, L.; Nerenberg, K. Canadian Adult Obesity Clinical Practice Guidelines: Weight Management Over the Reproductive Years for Adult Women Living with Obesity; CMAJ: Kingston, ON, Canada, 2020; pp. 1–12. [Google Scholar]
- Ryan, K.; Bain, B.J.; Worthington, D.; James, J.; Plews, D.; Mason, A.; Roper, D.; Rees, D.C.; De la Salle, B.; Streetly, A.; et al. Significant haemoglobinopathies: Guidelines for screening and diagnosis. Br. J. Haematol. 2010, 149, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Sénat, M.V.; Boulogne, A.I.; Deneux-Tharaux, C.; Fuchs, F.; Legendre, G.; Le Ray, C.; Lopez, E.; Schmitz, T.; Lejeune-Saada, V. Shoulder dystocia: Guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.L.; U.S. Preventive Services Task Force. Screening for Iron Deficiency Anemia and Iron Supplementation in Pregnant Women to Improve Maternal Health and Birth Outcomes: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Society for Maternal-Fetal Medicine (SMFM); Lauder, J.; Sciscione, A.; Biggio, J.; Osmundson, S. Society for Maternal-Fetal Medicine Consult Series #50: The role of activity restriction in obstetric management: (Replaces Consult Number 33, August 2014). Am. J. Obstet Gynecol. 2020, 223, B2–B10. [Google Scholar] [PubMed]
- Meija, L.; Rezeberga, D. Proper Maternal Nutrition during Pregnancy Planning and Pregnancy: A Healthy Start in Life; WHO: Copenhague, Dinamarca, 2017; pp. 4–31. [Google Scholar]
- World Health Organization. Guideline: Daily Iron Supplementation in Adult Women and Adolescent Girls; World Health Organization: Geneva, Switzerland, 2016; pp. 1–25. [Google Scholar]
- World Health Organization. Guideline: Intermittent Iron and Folic Acid Supplementation in Menstruating Women; World Health Organization: Geneva, Switzerland, 2011; pp. 5–25. [Google Scholar]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012; pp. 1–42. [Google Scholar]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015; pp. 1–45. [Google Scholar]
- World Health Organization. Guideline: Vitamin A Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2011; pp. 1–25. [Google Scholar]
- World Health Organization. WHO Antenatal Care Recommendations for a Positive Pregnancy Experience: Nutritional Interventions Update: Multiple Micronutrient Supplements during Pregnancy; World Health Organization: Geneva, Switzerland, 2020; pp. 1–122. [Google Scholar]
- World Health Organization. WHO Antenatal Care Recommendations for a Positive Pregnancy Experience: Nutritional Interventions Update: Vitamin D Supplements during Pregnancy; World Health Organization: Geneva, Switzerland, 2020; pp. 1–34. [Google Scholar]
- World Health Organization. WHO Recommendations on Antenatal Care for A Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016; pp. 1–152. [Google Scholar]
- Grammatikopoulou, M.G.; Theodoridis, X.; Gkiouras, K.; Lampropoulou, M.; Petalidou, A.; Patelida, M.; Tsirou, E.; Papoutsakis, C.; Goulis, D.G. Methodological quality of clinical practice guidelines for nutrition and weight gain during pregnancy: A systematic review. Nutr. Rev. 2020, 78, 546–562. [Google Scholar] [CrossRef]
- Simon, A.; Pratt, M.; Hutton, B.; Skidmore, B.; Fakhraei, R.; Rybak, N.; Corsi, D.J.; Walker, M.; Velez, M.P.; Smith, G.N.; et al. Guidelines for the management of pregnant women with obesity: A systematic review. Obes. Rev. 2020, 21, e12972. [Google Scholar] [CrossRef] [Green Version]
- Harrison, C.L.; Teede, H.; Khan, N.; Lim, S.; Chauhan, A.; Drakeley, S.; Moran, L.; Boyle, J. Weight management across preconception, pregnancy, and postpartum: A systematic review and quality appraisal of international clinical practice guidelines. Obes. Rev. 2021, 22, e13310. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Hanna, S.E.; Makarski, J.; et al. Development of the AGREE II, part 1: Performance, usefulness and areas for improvement. CMAJ 2010, 182, 1045–1052. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, C.; Ruel, M.T.; Salm, L.; Sinclair, B.; Branca, F. Double-duty actions: Seizing programme and policy opportunities to address malnutrition in all its forms. Lancet 2020, 395, 142–155. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (“Pregnancy”[Mesh] OR “Pregnancy Trimester, First”[Mesh] OR “Pregnancy Trimester, Second”[Mesh] OR “Pregnancy Trimester, Third”[Mesh]) AND (“Prenatal Care”[Mesh] OR “Nutrition Assessment”[Mesh] OR “Nutrition Therapy”[Mesh] OR “prevention and control” [Subheading] OR “Health Promotion”[Mesh]) AND (“Malnutrition”[Mesh] OR “Body Weight”[Mesh] OR “Anemia”[Mesh] OR “Deficiency Diseases”[Mesh] OR “Nutrition Disorders”[Mesh] OR “Gestational Weight Gain”[Mesh] OR “Fetal Growth Retardation”[Mesh] OR “Nutritional Physiological Phenomena”[Mesh]) |
| Reference | Clinical Guideline | Supporting Organization | Year of Publication | Region or Country | Number of References | Target Audience | Type of Recommendations |
|---|---|---|---|---|---|---|---|
| American College of Obstetricians and Gynecologists [19] | ACOG Practice Bulletin No 156: Obesity in Pregnancy | The American College of Obstetricians and Gynecologists | 2015 | USA | 112 | Obstetric care provider or healthcare professionals | P, D |
| American Diabetes Association [20] | Management of diabetes in pregnancy | American Diabetes Association. | 2015 | USA | 23 | Healthcare providers | P, D, T |
| ADA, ASN, Siega-Riz, A.M., King, J.C. [21] | Position of the American Dietetic Association and American Society for Nutrition: obesity, reproduction, and pregnancy outcomes | American Society for Nutrition | 2009 | USA | 97 | Registered dietitians, registered dietetic technicians, and other healthcare professionals | P, D, T |
| Australian Government Department of Health [22] | Clinical Practice Guidelines: Pregnancy Care | Australian Government Department of Health | 2019 | Australia | Not specified | Health professionals | P |
| Bomba-Opoń [23] | Folate supplementation during the preconception period, pregnancy, and puerperium. Polish Society of Gynecologists and Obstetricians Guidelines | Polish Society of Gynecologists and Obstetricians (PTGP): | 2017 | Poland | 30 | Not specified | P, T |
| Cetin, I. [24] | Breastfeeding during pregnancy: position paper of the Italian Society of Perinatal Medicine and the Task Force on Breastfeeding, Ministry of Health, Italy | Italian Society of Perinatal Medicine and Task Force on Breastfeeding | 2014 | Italy | 66 | Not specified | P, T |
| Charzewska. J. [25] | Prophylaxis of vitamin D deficiency, Polish Recommendations 2009 | Not specified | 2010 | Poland | Not specified | Not specified | P, D, T |
| CMACE [26] | Management of Women with Obesity in Pregnancy | Royal College of Obstetricians and Gynecologists | 2010 | UK | 77 | Health professionals | P, D, T |
| Davies. G.A. [27] | SOGC Clinical Practice Guidelines: Obesity in pregnancy. No. 239, February 2010 | Society of Obstetricians and Gynecologists of Canada | 2010 | Canada | 79 | Obstetrical care team | P, D, T |
| Davies. G.A.L. [28] | No. 239, Obesity in Pregnancy | The Society of Obstetricians and Gynecologists of Canada. | 2018 | Canada | 78 | Obstetrical care team | P, D, T |
| Denison, F.C. [29] | Care of Women with Obesity in Pregnancy: Green-Top Guideline No. 72 | Royal College of Obstetricians and Gynecologists | 2019 | UK | 202 | Healthcare providers | P, D, T |
| Donnay, S. [30] | Iodine supplementation during pregnancy and lactation. Position statement of the working group on disorders related to iodine deficiency and thyroid dysfunction of the Spanish Society of Endocrinology and Nutrition | Spanish Society of Endocrinology and Nutrition | 2014 | Spain | 73 | Not specified | D |
| Fitzsimons, K.J. [31] | Setting maternity care standards for women with obesity in pregnancy | Centre for Maternal and Child Enquiries(CMACE) | 2010 | UK | 55 | Not specified | P, D, T |
| Fleming, N. [32] | Adolescent Pregnancy Guidelines | Canadian Pediatric and Adolescent Gynecology andObstetricians (CANPAGO) | 2015 | Canada | 119 | Healthcare providers | P, D |
| Haq, A. [33] | Clinical practice guidelines for vitamin D in the United Arab Emirates | Not specified | 2018 | United Arab Emirates | 32 | Physicians | D, T |
| Harden, C.L. [34] | Practice parameter update: management issues for women with epilepsy--focus on pregnancy (an evidence-based review): vitamin K, folic acid, blood levels, and breastfeeding: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society | American Academy of Neurology | 2009 | USA | 40 | Not specified | P, T |
| Homer, C.S. [35] | Updated clinical practice guidelines on pregnancy care | Australian Health Ministers’ Conference and the Community and Disability Services Ministers’ Conference | 2018 | Australia | 11 | Health professionals | P, D |
| Jacob, C.M. [36] | Management of prepregnancy, pregnancy, and postpartum obesity from the FIGO Pregnancy and Non-Communicable Diseases Committee: A FIGO (International Federation of Gynecology and Obstetrics) guideline | International Federation of Gynecology and Obstetrics | 2020 | International | 77 | Healthcare practitioners | P, D, T |
| Koren, G. [37] | Cancer chemotherapy and pregnancy | Society of Obstetricians and Gynaecologists of Canada. | 2013 | Canada | 88 | Healthcare practitioners | P, T |
| Lausman, A. [38] | Intrauterine growth restriction: screening, diagnosis, and management | Society of Obstetricians and Gynaecologists of Canada | 2013 | Canada | 55 | Not specified | P, D, T |
| Marsh, J.C. [39] | Guidelines for the diagnosis and management of aplastic anaemia | General Haematology Task Force of the British Committee for Standards in Haematology | 2009 | UK | 174 | Health professionals | D, T |
| Maxwell, C. [40] | Guideline No. 391, Pregnancy and Maternal Obesity Part 1: Preconception and Prenatal Care | Society of Obstetricians and Gynaecologists of Canada (SOGC) | 2019 | Canada | 178 | Healthcare practitioners | P. T |
| Maxwell, C. [41] | Guideline No. 392, Pregnancy and Maternal Obesity Part 2: Team Planning for Delivery and Postpartum Care | Society of Obstetricians and Gynaecologists of Canada (SOGC) | 2019 | Canada | 149 | Healthcare practitioners | P, D T |
| Mottola, M.F. [42] | 2019 Canadian guideline for physical activity throughout pregnancy | Society of Obstetricians and Gynaecologists of Canada’s (SOGC) Maternal Fetal Medicineand Guideline Management and Oversight Committees | 2018 | Canada | 40 | Obstetric care providers, policymakers, and fitness professionals | P |
| Muraro, A. [43] | EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy | European Academy of Allergy and Clinical Immunology’s (EAACI) | 2014 | Europe | 98 | Medical secondary care, primary care, and nursing | P, T |
| NICE [44] | Antenatal care for uncomplicated pregnancies | National Institute for Health and Care Excellence: Guidelines | 2019 | UK | Not specified | Healthcare providers | P, D, T |
| NICE [45] | Diabetes in pregnancy: management from preconception to the postnatal period | National Institute for Health and Care Excellence: Guidelines | 2020 | UK | Not specified | Healthcare providers | P, D, T |
| NICE [46] | Weight management before, during, and after pregnancy | National Institute for Health and Care Excellence: Guidelines | 2010 | UK | 15 | Health professionals | P, D, T |
| Pavord, S. [47] | UK guidelines on the management of iron deficiency in pregnancy | British Committee for Standards in Haematology | 2012 | UK | 81 | Healthcare professionals | P, D, T |
| Piccinini, V.H. [48] | Canadian Adult Obesity Clinical Practice Guidelines: Weight Management Over the Reproductive Years for Adult Women Living with Obesity | The Canadian Association of Bariatric Physicians and Surgeons (CABPS) | 2020 | Canada | 126 | Primary care providers | P, T |
| Ryan, K. [49] | Significant haemoglobinopathies: guidelines for screening and diagnosis | British Society for Haematology | 2010 | UK | 19 | Not specified | D |
| Sentilhes, L. [50] | Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF) | French College of Gynecologists and Obstetricians (CNGOF) | 2016 | France | 11 | Obstetricians or Health professional | P, T |
| Siu, A.L. [51] | Screening for Iron Deficiency Anemia and Iron Supplementation in Pregnant Women to Improve Maternal Health and Birth Outcomes: U.S. Preventive Services Task Force Recommendation Statement | U.S. Preventive Services Task Force (USPSTF) | 2015 | USA | 27 | Not specified | D, T |
| SMFM [52] | Society for Maternal–Fetal Medicine Consult Series #50: The role of activity restriction in obstetric management: (Replaces Consult Number 33, August 2014) | Society for Maternal–Fetal Medicine | 2020 | USA | 47 | Obstetricians and maternal–fetal medicinesubspecialists | T |
| WHO [53] | Proper maternal nutrition during pregnancy planning and pregnancy: a healthy start in life | Ministry of Health of Latvia and the WHO Regional Office for Europe | 2017 | Europe | 27 | Not specified | P |
| WHO [54] | Guideline: daily iron supplementation in adult women and adolescent girls | WHO Guidelines Approved by the Guidelines Review Committee | 2016 | International | 28 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [55] | Guideline: intermittent iron and folic acid supplementation in nonanaemic pregnant women | WHO Guidelines Approved by the Guidelines Review Committee | 2011 | International | 32 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [56] | Guideline: sodium intake for adults and children | WHO Guidelines Approved by the Guidelines Review Committee | 2012 | International | 62 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [57] | Guideline: sugar intake for adults and children, World Health Organization | WHO Guidelines Approved by the Guidelines Review Committee | 2015 | International | 61 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [58] | Guideline: vitamin A supplementation in pregnant women | WHO Guidelines Approved by the Guidelines Review Committee | 2011 | International | 33 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [59] | WHO antenatal care recommendations for a positive pregnancy experience: nutritional interventions update: multiple micronutrient supplements during pregnancy | WHO Guidelines Approved by the Guidelines Review Committee | 2020 | International | 50 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [60] | WHO antenatal care recommendations for a positive pregnancy experience: nutritional interventions update: vitamin D supplements during pregnancy | WHO Guidelines Approved by the Guidelines Review Committee | 2020 | International | 56 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P |
| WHO [61] | WHO recommendations on antenatal care for a positive pregnancy experience | WHO Guidelines Approved by the Guidelines Review Committee | 2016 | International | 214 | Policymakers, expert advisers, and organizations involved in nutrition actions for public health | P, D |
| Clinical Guideline | AGREE II Domains (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Scope and Purpose | Stakeholder Involvement | Rigour of Development | Clarity of Presentation | Applicability | Editorial Independence | Overall Assessment | Quality of Guidelines | |
| 12. Management of diabetes in pregnancy [20] | 89 | 92 | 90 | 94 | 88 | 96 | 83 | High quality |
| 2019 Canadian guideline for physical activity throughout pregnancy [42] | 100 | 97 | 92 | 100 | 96 | 88 | 92 | High quality |
| ACOG Practice Bulletin No 156: Obesity in Pregnancy [19] | 83 | 75 | 71 | 94 | 75 | 54 | 67 | Low quality |
| Adolescent Pregnancy Guidelines [32] | 97 | 86 | 81 | 100 | 67 | 75 | 83 | High quality |
| Antenatal care for uncomplicated pregnancies [44] | 100 | 97 | 100 | 100 | 94 | 92 | 100 | High quality |
| Breastfeeding during pregnancy: position paper of the Italian Society of Perinatal Medicine and the Task Force on Breastfeeding, Ministry of Health, Italy [24] | 83 | 69 | 57 | 25 | 38 | 88 | 58 | Low quality |
| Canadian Adult Obesity Clinical Practice Guidelines: Weight Management Over the Reproductive Years for Adult Women Living with Obesity [48] | 94 | 86 | 75 | 92 | 88 | 58 | 83 | High quality |
| Cancer chemotherapy and pregnancy [37] | 89 | 92 | 90 | 94 | 88 | 96 | 83 | High quality |
| Care of Women with Obesity in Pregnancy: Green-top Guideline No. 72 [29] | 86 | 58 | 97 | 97 | 65 | 96 | 83 | High quality |
| Clinical practice guidelines for vitamin D in the United Arab Emirates [33] | 94 | 72 | 51 | 89 | 73 | 29 | 67 | Low quality |
| Clinical Practice Guidelines: Pregnancy Care [22] | 69 | 56 | 56 | 83 | 48 | 71 | 58 | Low quality |
| Diabetes in pregnancy: management from preconception to the postnatal period [45] | 100 | 100 | 84 | 100 | 98 | 92 | 92 | High quality |
| EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy [43] | 75 | 89 | 97 | 97 | 85 | 96 | 92 | High quality |
| Folate supplementation during the preconception period, pregnancy and puerperium. Polish Society of Gynecologists and Obstetricians Guidelines [23] | 39 | 28 | 21 | 64 | 4 | 8 | 17 | Low quality |
| Guideline No. 391, Pregnancy and Maternal Obesity Part 1: Preconception and Prenatal Care [40] | 97 | 83 | 100 | 94 | 60 | 83 | 83 | High quality |
| Guideline No. 392, Pregnancy and Maternal Obesity Part 2: Team Planning for Delivery and Postpartum Care [41] | 100 | 100 | 85 | 100 | 96 | 92 | 92 | High quality |
| Guideline: daily iron supplementation in adult women and adolescent girls [54] | 100 | 86 | 98 | 100 | 90 | 100 | 100 | High quality |
| Guideline: intermittent iron and folic acid supplementation in nonanemic pregnant women [55] | 100 | 83 | 96 | 92 | 100 | 83 | 92 | High quality |
| Guideline: sodium intake for adults and children [56] | 100 | 83 | 98 | 100 | 88 | 100 | 92 | High quality |
| Guideline: sugars intake for adults and children. World Health Organization [57] | 100 | 83 | 98 | 100 | 100 | 100 | 92 | High quality |
| Guideline: vitamin A supplementation in pregnant women [58] | 100 | 89 | 98 | 100 | 96 | 100 | 100 | High quality |
| Guidelines for the diagnosis and management of aplastic anemia [39] | 92 | 81 | 65 | 92 | 50 | 58 | 58 | Low quality |
| Intrauterine growth restriction: screening, diagnosis, and management [38] | 81 | 33 | 53 | 89 | 33 | 4 | 50 | Low quality |
| Iodine supplementation during pregnancy and lactation. Position statement of the working group on disorders related to iodine deficiency and thyroid dysfunction of the Spanish Society of Endocrinology and Nutrition [30] | 83 | 56 | 42 | 42 | 27 | 54 | 50 | Low quality |
| Management of prepregnancy, pregnancy, and postpartum obesity from the FIGO Pregnancy and Non-Communicable Diseases Committee: A FIGO (International Federation of Gynecology and Obstetrics) guideline [36] | 100 | 94 | 86 | 100 | 92 | 100 | 92 | High quality |
| Management of Women with Obesity in Pregnancy [26] | 100 | 89 | 92 | 94 | 83 | 92 | 67 | Low quality |
| No. 239-Obesity in Pregnancy [28] | 86 | 39 | 63 | 86 | 33 | 21 | 50 | Low quality |
| Position of the American Dietetic Association and American Society for Nutrition: obesity, reproduction, and pregnancy outcomes [21] | 75 | 47 | 22 | 56 | 25 | 29 | 25 | Low quality |
| Practice parameter update: management issues for women with epilepsy—focus on pregnancy (an evidence-based review): vitamin K, folic acid, blood levels, and breastfeeding: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society [34] | 100 | 81 | 73 | 92 | 75 | 75 | 58 | Low quality |
| Proper maternal nutrition during pregnancy planning and pregnancy: a healthy start in life [53] | 89 | 81 | 63 | 83 | 63 | 96 | 67 | Low quality |
| Prophylaxis of vitamin D deficiency: Polish Recommendations 2009 [25] | 58 | 53 | 10 | 81 | 38 | 29 | 50 | Low quality |
| Screening for Iron Deficiency Anemia and Iron Supplementation in Pregnant Women to Improve Maternal Health and Birth Outcomes: U.S. Preventive Services Task Force Recommendation Statement [51] | 97 | 47 | 58 | 69 | 54 | 100 | 58 | Low quality |
| Setting maternity care standards for women with obesity in pregnancy [31] | 83 | 72 | 73 | 83 | 52 | 92 | 67 | Low quality |
| Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF) [50] | 81 | 67 | 73 | 78 | 67 | 96 | 67 | Low quality |
| Significant haemoglobinopathies: guidelines for screening and diagnosis [49] | 81 | 92 | 58 | 89 | 58 | 8 | 50 | Low quality |
| Society for Maternal–Fetal Medicine Consult Series #50: The role of activity restriction in obstetric management: (Replaces Consult Number 33, August 2014) [52] | 75 | 44 | 53 | 72 | 42 | 50 | 58 | Low quality |
| SOGC Clinical Practice Guidelines: Obesity in Pregnancy. No. 239, February 2010 [27] | 83 | 39 | 63 | 81 | 31 | 38 | 50 | Low quality |
| UK guidelines on the management of iron deficiency in pregnancy [47] | 75 | 64 | 67 | 78 | 54 | 100 | 67 | Low quality |
| Updated clinical practice guidelines on pregnancy care [35] | 97 | 94 | 90 | 100 | 63 | 88 | 83 | High quality |
| Weight management before, during and after pregnancy [46] | 100 | 100 | 92 | 100 | 94 | 100 | 92 | High quality |
| WHO antenatal care recommendations for a positive pregnancy experience: nutritional interventions update: multiple micronutrient supplements during pregnancy [59] | 89 | 86 | 90 | 86 | 75 | 100 | 83 | High quality |
| WHO antenatal care recommendations for a positive pregnancy experience: nutritional interventions update: vitamin D supplements during pregnancy [60] | 89 | 89 | 90 | 92 | 85 | 100 | 92 | High quality |
| WHO recommendations on antenatal care for a positive pregnancy experience [61] | 89 | 92 | 88 | 92 | 85 | 100 | 92 | High quality |
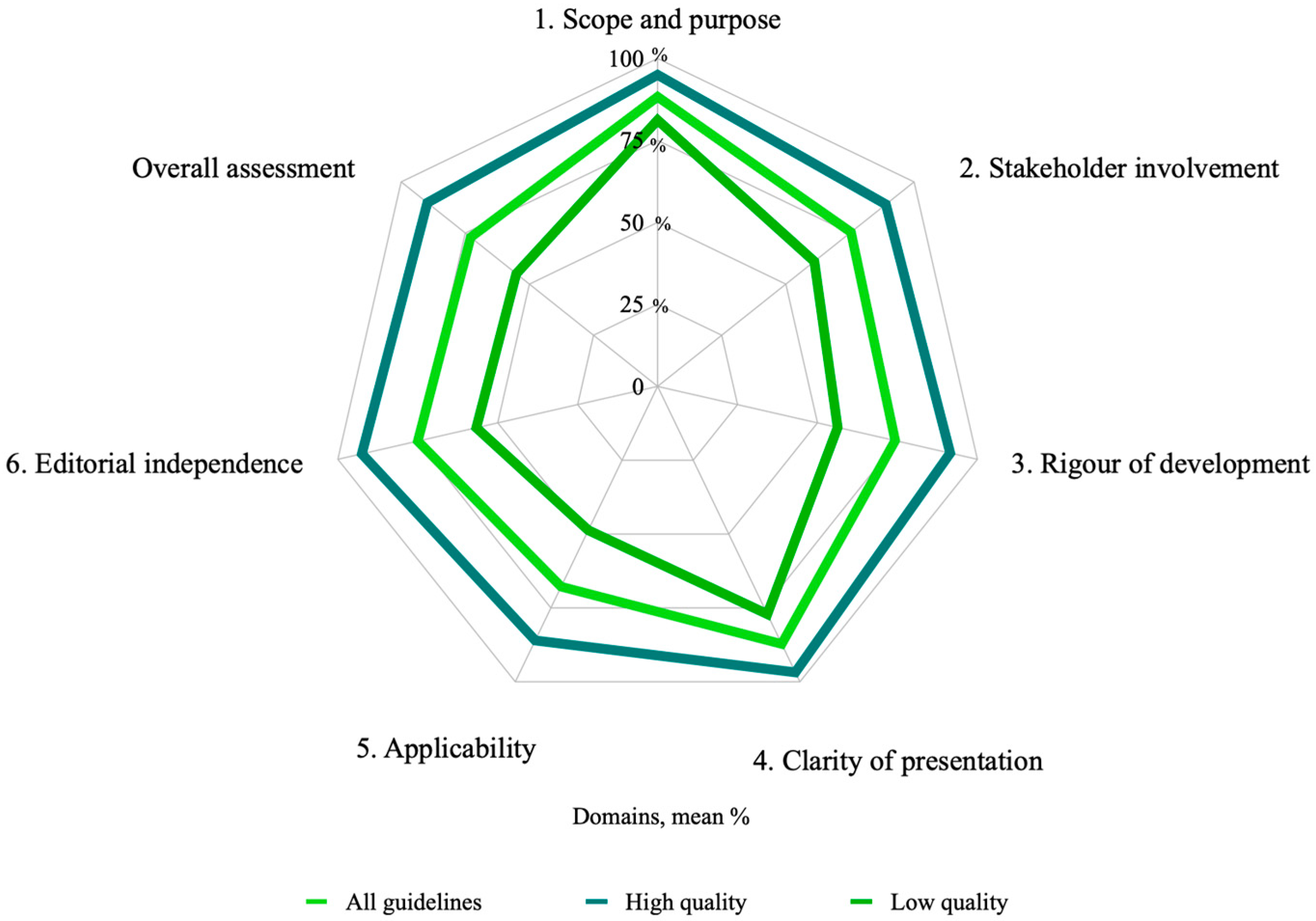
| Mean (range) | 88.3 (range 39 to 100%) | 75.4 (range 28 to 100%) | 74.3 (range 10 to 100%) | 87.2 (range 25 to 100%) | 67.8 (range 4 to 100%) | 75 (range 4 to 100%) | 72.9 (range 17 to 100%) | |
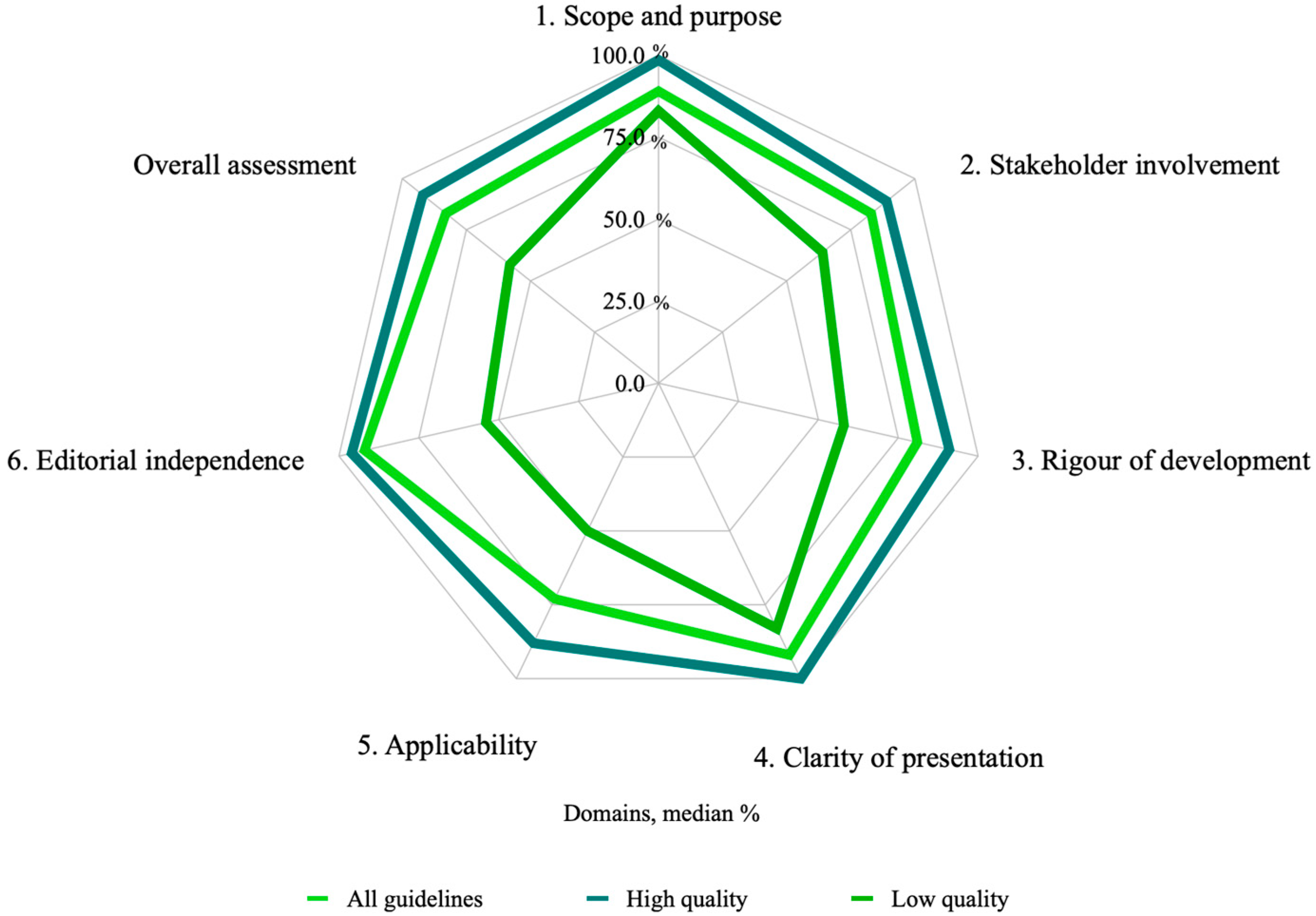
| Median (range) | 89 (range 39 to 100%) | 83 (range 28 to 100%) | 81 (range 10 to 100%) | 92 (range 25 to 100%) | 73 (range 4 to 100%) | 92 (range 4 to 100%) | 83 (range 17 to 100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Manrique, C.; Ancira-Moreno, M.; Burrola-Méndez, S.; Omaña-Guzmán, I.; Hoyos-Loya, E.; Hernández-Cordero, S.; Trejo-Domínguez, A.; Mazariegos, M.; Smith, N.; Alonso-Carmona, S.; et al. Quality Appraisal of Nutritional Guidelines to Prevent, Diagnose, and Treat Malnutrition in All Its Forms during Pregnancy. Nutrients 2022, 14, 4579. https://doi.org/10.3390/nu14214579
Muñoz-Manrique C, Ancira-Moreno M, Burrola-Méndez S, Omaña-Guzmán I, Hoyos-Loya E, Hernández-Cordero S, Trejo-Domínguez A, Mazariegos M, Smith N, Alonso-Carmona S, et al. Quality Appraisal of Nutritional Guidelines to Prevent, Diagnose, and Treat Malnutrition in All Its Forms during Pregnancy. Nutrients. 2022; 14(21):4579. https://doi.org/10.3390/nu14214579
Chicago/Turabian StyleMuñoz-Manrique, Cinthya, Mónica Ancira-Moreno, Soraya Burrola-Méndez, Isabel Omaña-Guzmán, Elizabeth Hoyos-Loya, Sonia Hernández-Cordero, Alejandra Trejo-Domínguez, Mónica Mazariegos, Natalia Smith, Scarlett Alonso-Carmona, and et al. 2022. "Quality Appraisal of Nutritional Guidelines to Prevent, Diagnose, and Treat Malnutrition in All Its Forms during Pregnancy" Nutrients 14, no. 21: 4579. https://doi.org/10.3390/nu14214579
APA StyleMuñoz-Manrique, C., Ancira-Moreno, M., Burrola-Méndez, S., Omaña-Guzmán, I., Hoyos-Loya, E., Hernández-Cordero, S., Trejo-Domínguez, A., Mazariegos, M., Smith, N., Alonso-Carmona, S., Mier-Cabrera, J., Tavano-Colaizzi, L., Sánchez-Múzquiz, B., Avendaño-Álvarez, F., Muciño-Sandoval, K., Rodríguez-Moguel, N. C., Padilla-Camacho, M., Espino-y-Sosa, S., Ibarra-González, L., & Medina-Avilés, C. (2022). Quality Appraisal of Nutritional Guidelines to Prevent, Diagnose, and Treat Malnutrition in All Its Forms during Pregnancy. Nutrients, 14(21), 4579. https://doi.org/10.3390/nu14214579