
Effects of Additional Dietary Fiber Supplements on Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Studies




Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
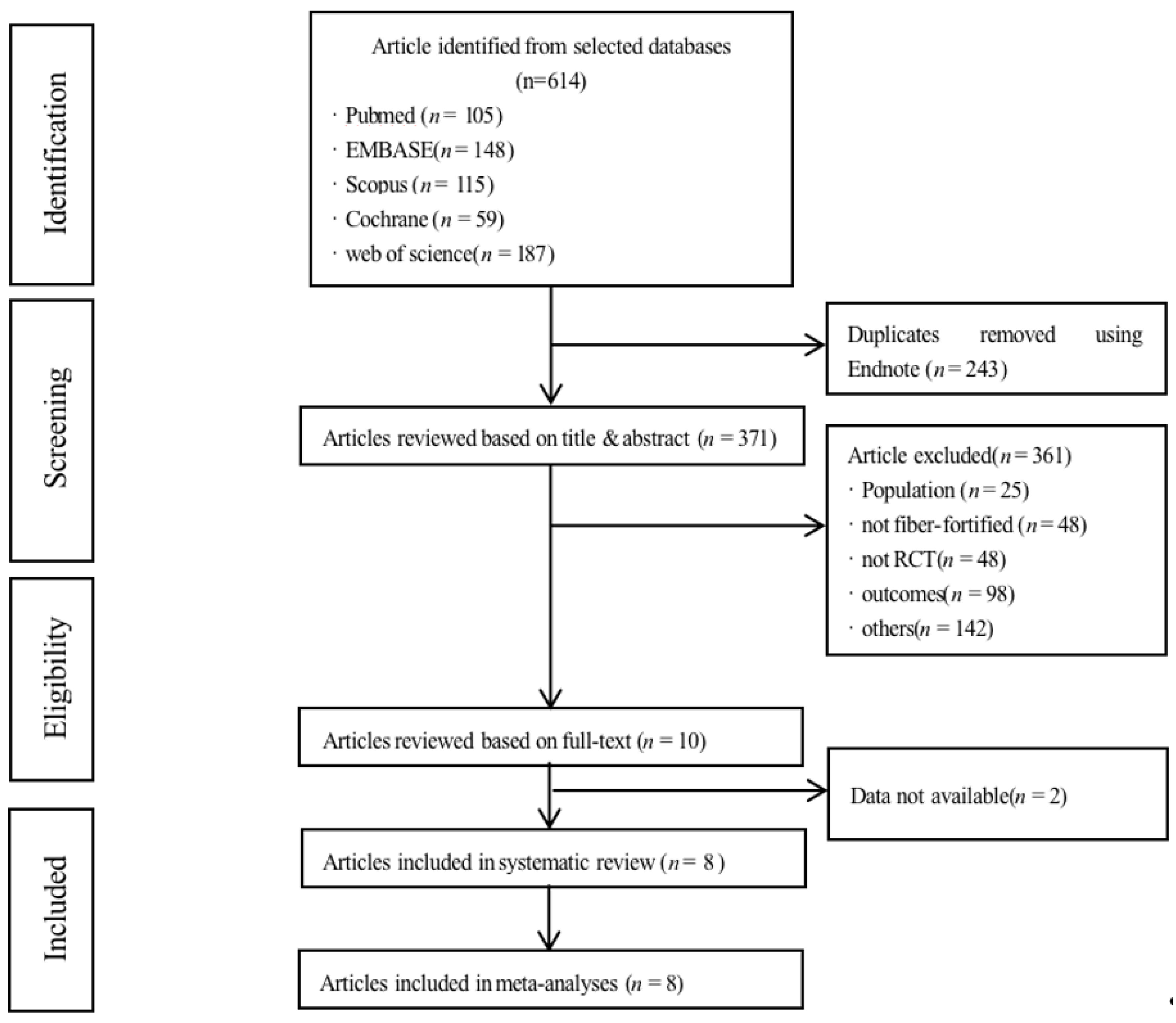
3.1. Search Results and Characteristics
3.2. Quality and Risk of Bias within Studies
3.3. Meta-Analyses
3.4. Serum Glucose Outcomes
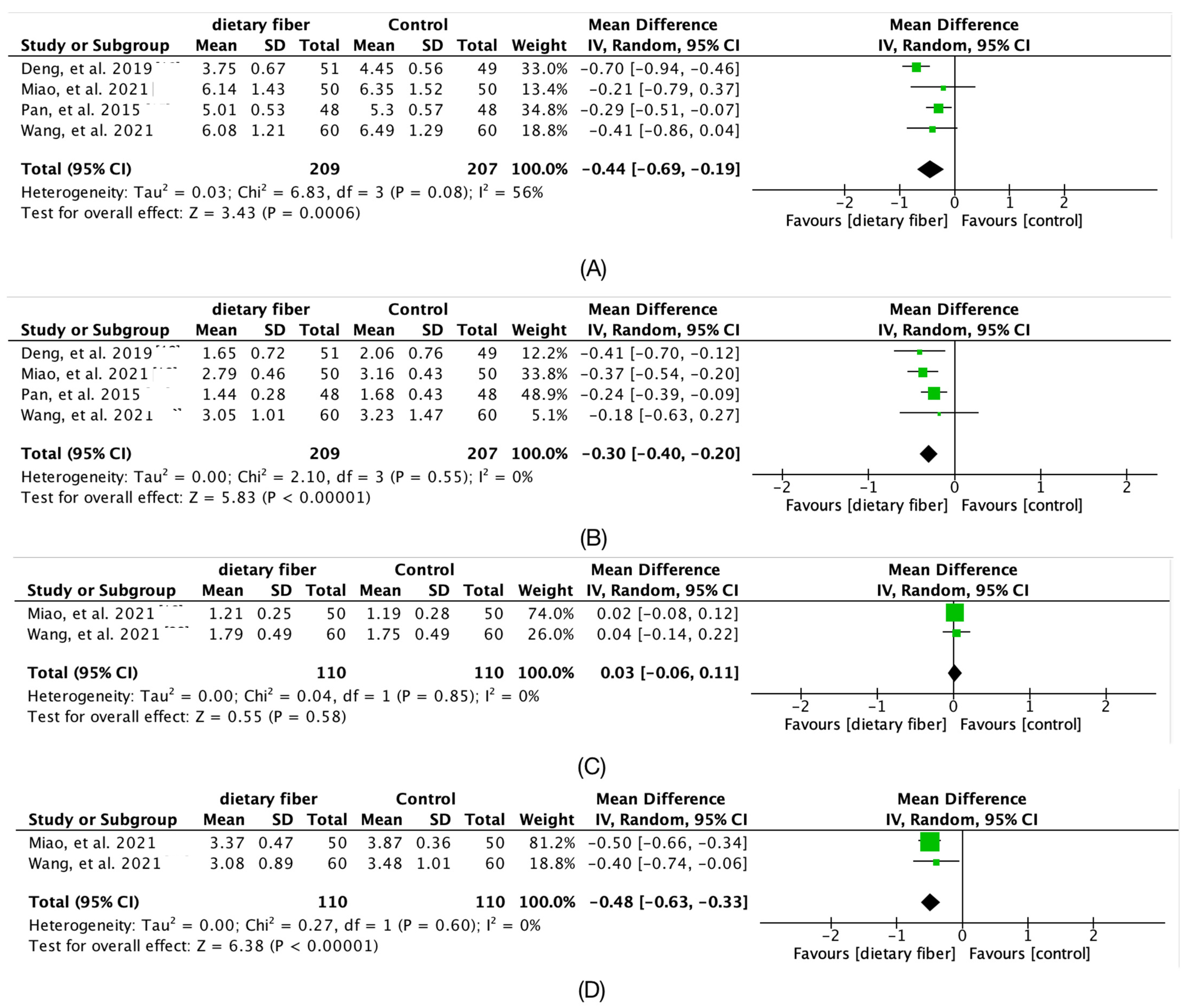
3.5. Serum Lipid Outcome
3.6. Pregnancy and Neonatal Outcomes
3.7. Subgroup Analyses on Fiber Type, Fiber Quantity
3.8. Fiber Type
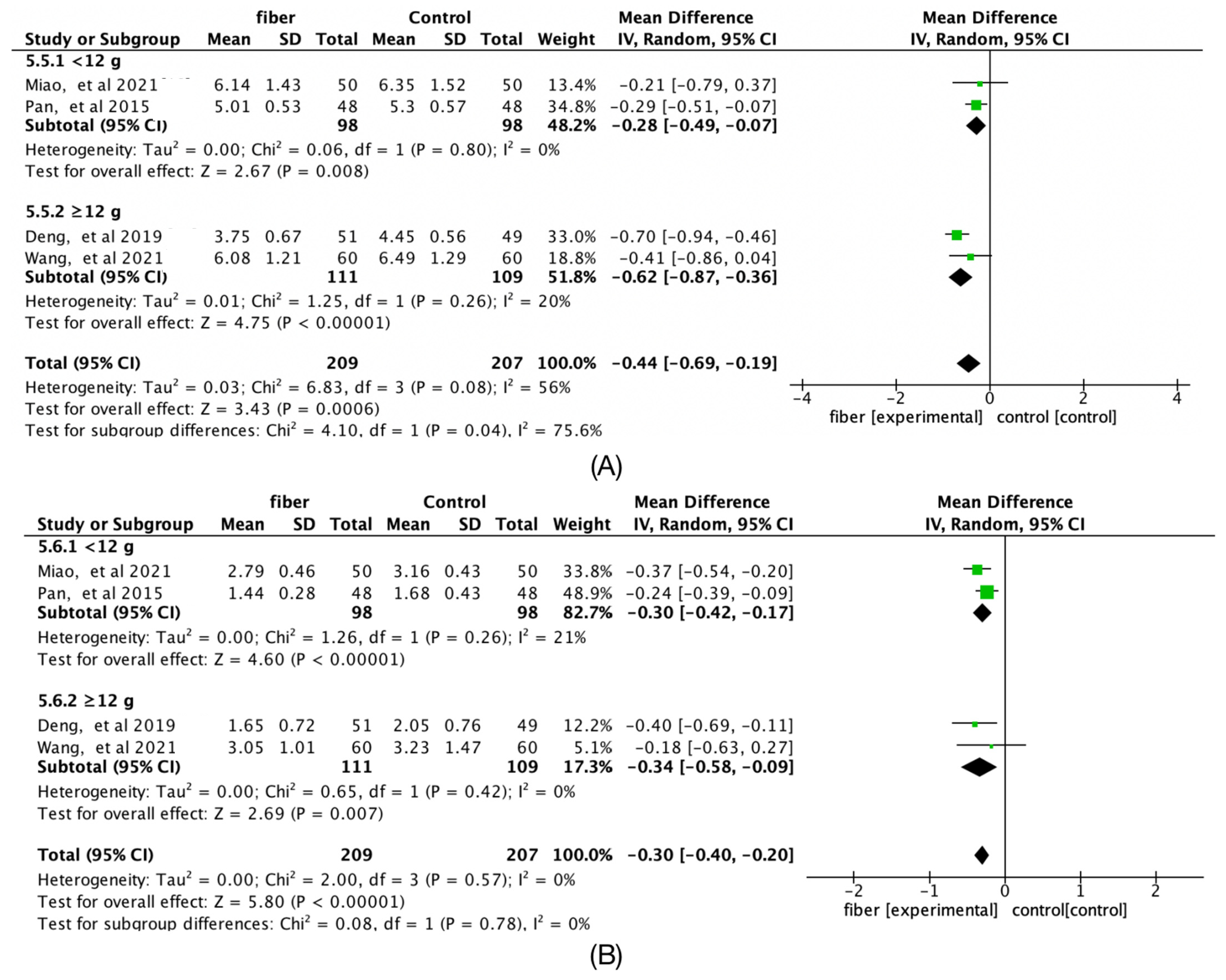
3.9. Fiber Quantity
3.10. Sensitivity Analyses and Publication Bias
4. Discussion
4.1. Effects of Fiber-Fortified Food on Serum Glucose Outcomes
4.2. Effects of Fiber-Fortified Food on Lipid Metabolism
4.3. Effects of Fiber-Fortified Food on Pregnancy and Neonatal Outcome
4.4. Strengths, Limitations, and Insights
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat. Rev. Dis. Primers 2019, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokomichi, H.; Mochizuki, M.; Shinohara, R.; Kushima, M.; Horiuchi, S.; Kojima, R.; Ooka, T.; Akiyama, Y.; Miyake, K.; Otawa, S.; et al. Gestational age, birth weight, and perinatal complications in mothers with. PLoS ONE 2022, 17, e0269610. [Google Scholar] [CrossRef]
- Phattanachindakun, B.; Watananirun, K.; Boriboonhirunsarn, D. Early universal screening of gestational diabetes in a university hospital in Thailand. J. Obstet. Gynaecol. 2022, 42, 1–7. [Google Scholar] [CrossRef]
- Marley, A.R.; Domingues, A.; Ghosh, T.; Turcotte, L.M.; Spector, L.G. Maternal Body Mass Index, Diabetes, and Gestational Weight Gain and Risk for. JNCI Cancer Spectr. 2022, 6, 2515–5091. [Google Scholar] [CrossRef] [PubMed]
- Mack, L.R.; Tomich, P.G. Gestational Diabetes: Diagnosis, Classification, and Clinical Care. Obstet. Gynecol. Clin. N. Am. 2017, 44, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Reynolds, C.M.; Vickers, M.H.; Baker, P.N.; Stanley, J.L. Nutritional Supplementation for the Prevention and/or Treatment of Gestational. Curr. Diab. Rep. 2019, 9, 73. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef]
- Zhang, X.; Gong, Y.; Della Corte, K.; Yu, D.; Xue, H.; Shan, S.; Tian, G.; Liang, Y.; Zhang, J.; He, F.; et al. Relevance of dietary glycemic index, glycemic load and fiber intake before and during pregnancy for the risk of gestational diabetes mellitus and maternal glucose homeostasis. Clin. Nutr. 2021, 40, 2791–2799. [Google Scholar] [CrossRef]
- Xu, Q.; Tao, Y.; Zhang, Y.; Zhang, X.; Xue, C.; Liu, Y. Dietary fiber intake, dietary glycemic load, and the risk of gestational diabetes. Asia Pac. J. Clin. Nutr. 2021, 30, 477–486. [Google Scholar]
- Basu, A.; Feng, D.; Planinic, P.; Ebersole, J.L.; Lyons, T.J.; Alexander, J.M. Dietary Blueberry and Soluble Fiber Supplementation Reduces Risk of Gestational. J. Nutr. 2021, 151, 1128–1138. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, S.G.; Cohen, A.W.; Herman, G.O.; Schwartz, S. Effect of dietary fiber on the oral glucose tolerance test in pregnancy. Am. J. Obstet. Gynecol. 1982, 5, 154–157. [Google Scholar] [CrossRef]
- Cesa, F.; Mariani, S.; Fava, A.; Rauseo, R.; Zanetti, H. The use of vegetable fibers in the treatment of pregnancy diabetes and/or excessive wight gain during pregnancy. Minerva Ginecol. 1990, 42, 271–274. [Google Scholar]
- Afaghi, A.; Ghanei, L.; Ziaee, A. Effect of low glycemic load diet with and without wheat bran on glucose control in gestational diabetes mellitus: A randomized trial. Indian J. Endocrinol. Metab. 2013, 17, 689–692. [Google Scholar]
- Pan, F.; Wan, C.-H.; Cheng, X.Y.; Wang, H.X. Effect of dietary fiber on gestational diabetes mellitus. Guangxi Med. 2015, 37, 1175–1177. [Google Scholar]
- Deng, Y.; Zhao, L.; Pan, F.; Wang, J. Efficacy of Interventions with Dietary Fiber and Resistance Exercise for Patients with Gestational Diabetes Mellitus and Hyperlipidemia:a Clinical Study. Chin. Gen. Pract. 2019, 22, 1598–1602. [Google Scholar]
- Lunqing, W.; Yu, P. Effect of whey protein and dietary fiber on blood glucose level and nutritional status in gestational diabetes mellitus. Guangxi Med. 2020, 42, 2223–2225+2229. [Google Scholar]
- Miao, M.; Yue, Z.; Mu, J.; Dai, Y.M. Effects of inulin fructan on glucose and lipid metabolism in pregnant women with gestational diabetes mellitus. Jiangsu J. Prev. Med. 2021, 32, 153–156. [Google Scholar]
- Barati, Z.; Iravani, M.; Karandish, M.; Haghighizadeh, M.H.; Masihi, S. The effect of oat bran consumption on gestational diabetes: A randomized controlled clinical trial. BMC Endocr. Disord. 2021, 21, 67. [Google Scholar] [CrossRef]
- Wang, H.K.; Cheng, D.C.; Yang, Y.M.; Wang, X.H.; Chen, Y.; Zhang, L.; Xiu, L.; Xu, X.M. The Role of High-Content Complex Dietary Fiber in Medical Nutrition Therapy for Gestational Diabetes Mellitus. Front. Pharmacol. 2021, 12, 684898. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, J.; Hu, T.; Xu, C.; Xie, N.; Chen, D. Interventional effect of dietary fiber on blood glucose and pregnancy outcomes in patients with gestational diabetes mellitus. J. Zhejiang Univ. 2021, 50, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Lattimer, J.M.; Haub, M.D. Effects of dietary fiber and its components on metabolic health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, C.S.; Nankervis, A.; Teede, H.; Aroni, R. Dietary intervention strategies for ethnic Chinese women with gestational. Nutr. Diet. 2019, 76, 211–232. [Google Scholar] [CrossRef] [PubMed]
- Sartorelli, D.S.; Zuccolotto DC, C.; Crivellenti, L.C.; Franco, L.J. Dietary patterns during pregnancy derived by reduced-rank regression and their association with gestational diabetes mellitus. Nutrition 2019, 60, 191–196. [Google Scholar] [CrossRef]
- Yu, K.; Ke, M.Y.; Li, W.H.; Zhang, S.Q.; Fang, X.C. The impact of soluble dietary fibre on gastric emptying, postprandial blood. Asia Pac. J. Clin. Nutr. 2014, 23, 210–218. [Google Scholar] [PubMed]
- Chen, C.; Zeng, Y.; Xu, J.; Zheng, H.; Liu, J.; Fan, R.; Zhu, W.; Yuan, L.; Qin, Y.; Chen, S.; et al. Therapeutic effects of soluble dietary fiber consumption on type 2 diabetes. Exp. Ther. Med. 2016, 12, 1232–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabisch, S.; Meyer, N.M.; Honsek, C.; Gerbracht, C.; Dambeck, U.; Kemper, M.; Osterhoff, M.A.; Birkenfeld, A.L.; Arafat, A.M.; Hjorth, M.F.; et al. Fasting Glucose State Determines Metabolic Response to Supplementation with insoluble cereal fibre: A secondary analysis of the optimal fibre trial (OptiFiT). Nutrients 2019, 11, 2385. [Google Scholar] [CrossRef]
- Pontifex, M.G.; Mushtaq, A.; Le Gall, G.; Rodriguez-Ramiro, I.; Blokker, B.A.; Hoogteijling, M.E.; Ricci, M.; Pellizzon, M.; Vauzour, D.; Müller, M. Differential Influence of Soluble Dietary Fibres on Intestinal and Hepatic. Nutrients 2021, 13, 4278. [Google Scholar] [CrossRef]
- Zhang, S.; Meng, G.; Zhang, Q.; Liu, L.; Yao, Z.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, T.; Wang, X.; et al. Dietary fiber intake and risk of prediabetes in China: Results from the TCLSIH. Br. J. Nutr. 2021, 12, 1–20. [Google Scholar]
- Li, L.; Pan, M.; Pan, S.; Li, W.; Zhong, Y.; Hu, J.; Nie, S. Effects of insoluble and soluble fibers isolated from barley on blood glucose. Food Chem. Toxicol. 2020, 135, 110937. [Google Scholar] [CrossRef]
- Kimura, Y.; Yoshida, D.; Hirakawa, Y.; Hata, J.; Honda, T.; Shibata, M.; Sakata, S.; Uchida, K.; Kitazono, T.; Ninomiya, T. Dietary fiber intake and risk of type 2 diabetes in a general Japanese. J. Diabetes Investig. 2021, 12, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Yao, B.; Fang, H.; Xu, W.; Yan, Y.; Xu, H.; Liu, Y.; Mo, M.; Zhang, H.; Zhao, Y. Dietary fiber intake and risk of type 2 diabetes: A dose-response analysis of prospective studies. Eur. J. Epidemiol. 2014, 29, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Surampudi, P.; Enkhmaa, B.; Anuurad, E.; Berglund, L. Lipid Lowering with Soluble Dietary Fiber. Curr. Atheroscler Rep. 2016, 18, 75. [Google Scholar] [CrossRef]
- Vuksan, V.; Jenkins, A.L.; Rogovik, A.L.; Fairgrieve, C.D.; Jovanovski, E.; Leiter, L.A. Viscosity rather than quantity of dietary fibre predicts cholesterol-lowering effect in healthy individuals. Br. J. Nutr. 2011, 106, 1349–1352. [Google Scholar] [CrossRef] [Green Version]
- Franco, B.M.; Latre, M.L.; Esteban EM, A.; Ordovás, J.M.; Casasnovas, J.A.; Peñalvo, J.L. Soluble and insoluble dietary fibre intake and risk factors for metabolic. Nutr. Hosp. 2014, 30, 1279–1288. [Google Scholar]
- Narayan, S.; Lakshmipriya, N.; Vaidya, R.; Bai, M.R.; Sudha, V.; Krishnaswamy, K.; Unnikrishnan, R.; Anjana, R.M.; Mohan, V. Association of dietary fiber intake with serum total cholesterol and low density. Indian J. Endocrinol. Metab. 2014, 18, 624–630. [Google Scholar]
- Eshriqui, I.; Franco-Sena, A.B.; Farias, D.R.; Freitas-Vilela, A.A.; Cunha, D.B.; Barros, E.G.; Emmett, P.M.; Kac, G. Prepregnancy Dietary Patterns Are Associated with Blood Lipid Level Changes during Pregnancy: A Prospective Cohort Study in Rio de Janeiro, Brazil. J. Acad. Nutr. Diet. 2017, 117, 1066–1079. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.A.; Walsh, J.M.; Byrne, J.; Curran, S.; McAuliffe, F.M. The influence of a low glycemic index dietary intervention on maternal dietary. Nutr. J. 2013, 12, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves-Santos, N.H.; Cocate, P.G.; Benaim, C.; Farias, D.R.; Emmett, P.M.; Kac, G. Prepregnancy Dietary Patterns and Their Association with Perinatal Outcomes. J. Acad. Nutr. Diet. 2019, 119, 1439–1451. [Google Scholar] [CrossRef]
- Gershuni, V.; Li, Y.; Elovitz, M.; Li, H.; Wu, G.D.; Compher, C.W. Maternal gut microbiota reflecting poor diet quality is associated with spontaneous preterm birth in a prospective cohort study. Am. J. Clin. Nutr. 2021, 113, 602–611. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NO | First Author, Year | Population Size and Description | Intervention Duration (Weeks) | Study Design | Control Food and Description | Fiber and Description |
|---|---|---|---|---|---|---|
| 1 | Ahmad, et al., 2013 [14] | 36 subjects with GDM(18 I; 13 C) | 2 | Parallel Single-blind | low GL diet | 15 g insoluble fiber (wheat bran) |
| 2 | Pan, et al., 2015 [15] | 96 subjects with GDM (48 I; 48 C) | 4 | Parallel Single-blind | Diet therapy | 10.5 g insoluble fiber (wheat fiber) |
| 3 | Deng, et al., 2019 [16] | 100 subjects with GDM (51 I; 49 C) | 12 | Parallel Single-blind | Basic dietary nutrition support treatment | 20 g soluble dietary fiber (Fiber polysaccharide) |
| 4 | Wu, et al., 2020 [17] | 84 subjects with GDM (42 I; 42 C) | 8 | Parallel Single-blind | Personalized diet control | 15 g soluble dietary fiber (Inulin, stachyose, microcrystalline cellulose, oat fiber) |
| 5 | Miao, et al., 2021 [18] | 100 subjects with GDM (50 I; 50 C) | 4 | Parallel Single-blind | Dietary guidelines | 10 g soluble dietary fiber (Inulin) |
| 6 | Zahra, et al., 2021 [19] | 104 subjects with GDM (53 I; 51 C) | 4 | Parallel Single-blind | Dietary guidelines | 30 g insoluble fiber (oat bran) |
| 7 | Wang, et al., 2021 [20] | 120 subjects with GDM (60 I; 60 C) | 8 | Parallel Single-blind | Dietary guidelines | 19 g complex dietary fiber (Ricnoat) |
| 8 | Zhang, et al., 2021 [21] | 112 subjects with GDM (56 I; 56 C) | 8 | Parallel Single-blind | Dietary guidelines | 9.5 g complex dietary fiber (Ricnoat) |
| Outcome | Hedges’ g [95% CI] | I2 Value (%) | p Value |
|---|---|---|---|
| fasting glucose | −0.3 [−0.49, −0.1] | 83 | 0.003 |
| Two-hour plasma glucose | −0.69 [−0.88, −0.51] | 49 | <0.001 |
| HbA1c | −0.5 [−0.68, −0.31] | 0 | <0.001 |
| Number of qualified blood glucose | 5.27 [2.56, 10.83] | 0 | <0.001 |
| TC | −0.44 [−0.69, −0.19] | 56 | <0.001 |
| TG | −0.3 [−0.4, −0.2] | 0 | <0.001 |
| HDL | −0.03 [−0.06, 0.11] | 0 | 0.58 |
| LDL | −0.48 [−0.63, −0.33] | 0 | <0.001 |
| preterm delivery | 0.4 [0.19, 0.84] | 0 | 0.01 |
| cesarean delivery | 0.6 [0.37, 0.97] | 0 | 0.04 |
| fetal distress | 0.51 [0.22, 1.19] | 0 | 0.12 |
| neonatal weight | −0.17 [−0.27, −0.07] | 0 | <0.001 |
| Outcome | Fiber Type | Fiber Quantity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Insoluble | Soluble | Complex | <12 g | ≥12 g | ||||||
| Hedges’g (95% CI) | I2(%) | Hedges’g (95% CI) | I2(%) | Hedges’g (95% CI) | I2(%) | Hedges’g (95% CI) | I2(%) | Hedges’g (95% CI) | I2(%) | |
| fasting glucose | −0.44 [−0.52, −0.35] | 33.8 | −0.38 [−0.88, 0.13] | 36.5 | −0.09 [−0.25, 0.08] | 29.7 | −0.15 [−0.29, −0.02] | 0 | −0.40 [−0.69, −0.11] | 87 |
| 2-h glucose | −0.77 [−0.94, −0.61] | 44.4 | −1.00 [−1.42, −0.59] | 15.5 | −0.44 [−0.62, −0.26] | 40.1 | −0.56 [−0.87, −0.24] | 54 | −0.84 [−1.22, −0.46] | 51 |
| TC | — | — | — | — | — | — | −0.28 [−0.49, −0.07] | 0 | −0.62 [−0.87, −0.36] | 20 |
| TG | — | — | — | — | — | — | −0.30 [−0.42, −0.17] | 21 | −0.34 [−0.58, −0.09] | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, J.; Wang, J.; Ma, W.; Miao, M.; Sun, G. Effects of Additional Dietary Fiber Supplements on Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Nutrients 2022, 14, 4626. https://doi.org/10.3390/nu14214626
Sun J, Wang J, Ma W, Miao M, Sun G. Effects of Additional Dietary Fiber Supplements on Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Nutrients. 2022; 14(21):4626. https://doi.org/10.3390/nu14214626
Chicago/Turabian StyleSun, Jihan, Jinjing Wang, Wenqing Ma, Miao Miao, and Guiju Sun. 2022. "Effects of Additional Dietary Fiber Supplements on Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Studies" Nutrients 14, no. 21: 4626. https://doi.org/10.3390/nu14214626
APA StyleSun, J., Wang, J., Ma, W., Miao, M., & Sun, G. (2022). Effects of Additional Dietary Fiber Supplements on Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Nutrients, 14(21), 4626. https://doi.org/10.3390/nu14214626