Evaluation of the Effects of the Tritordeum-Based Diet Compared to the Low-FODMAPs Diet on the Fecal Metabolome of IBS-D Patients: A Preliminary Investigation

 ,
,  , , ,
, , ,  , ,
, , 

Abstract
:
1. Introduction
2. Materials and Methods
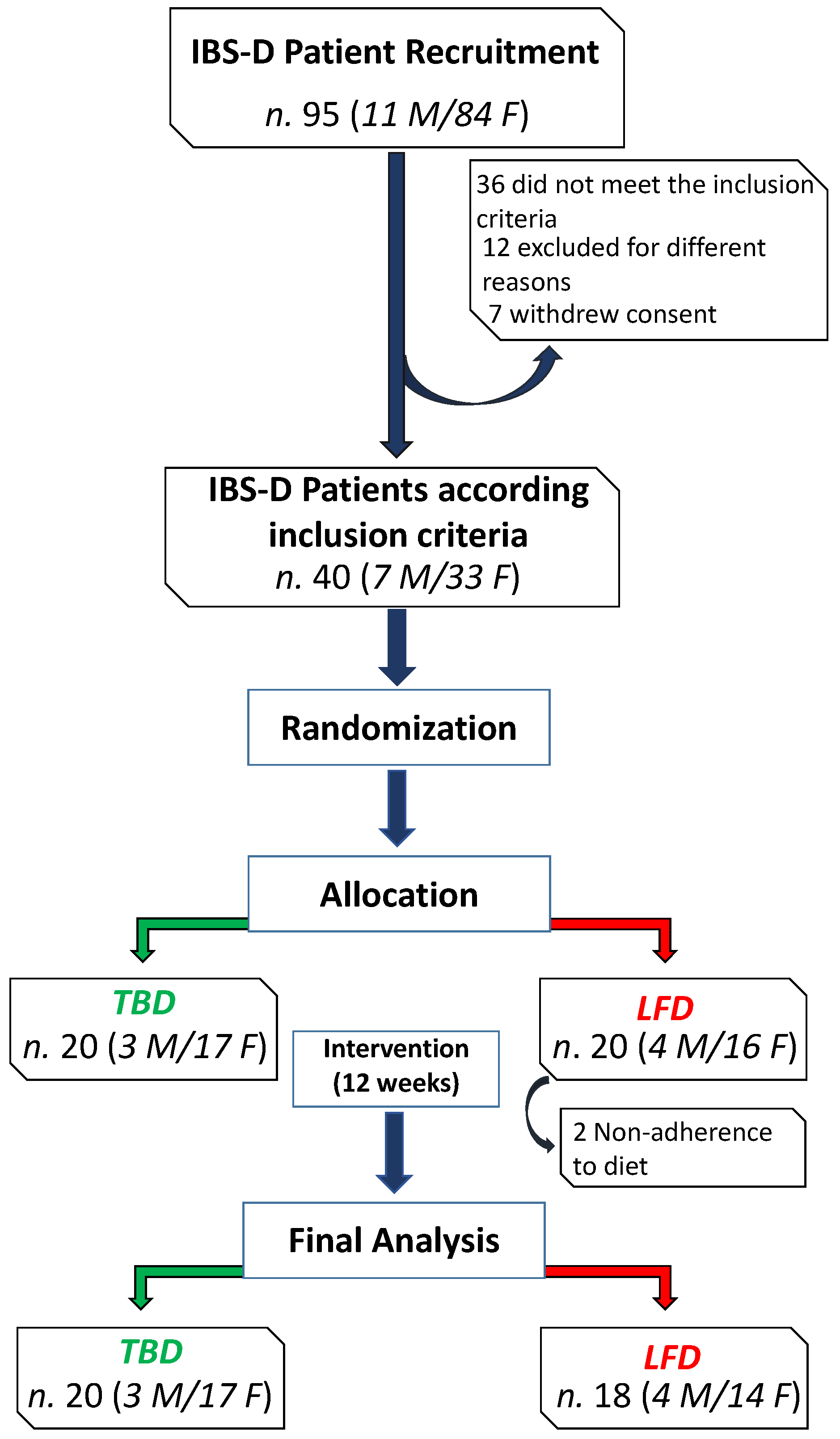
2.1. Subject Recruitment and Study Design
2.2. Characteristics of Tritordeum-Based Diet and Low-FODMAPs Diet
2.3. Symptom Profile
2.4. Fecal Metabolome
2.5. Quantitative Analysis of Targeted VOCs in Fecal Samples
2.6. Statistics
3. Results
3.1. Cohort, Baseline Characteristics and Diet
3.2. Symptom Evaluation
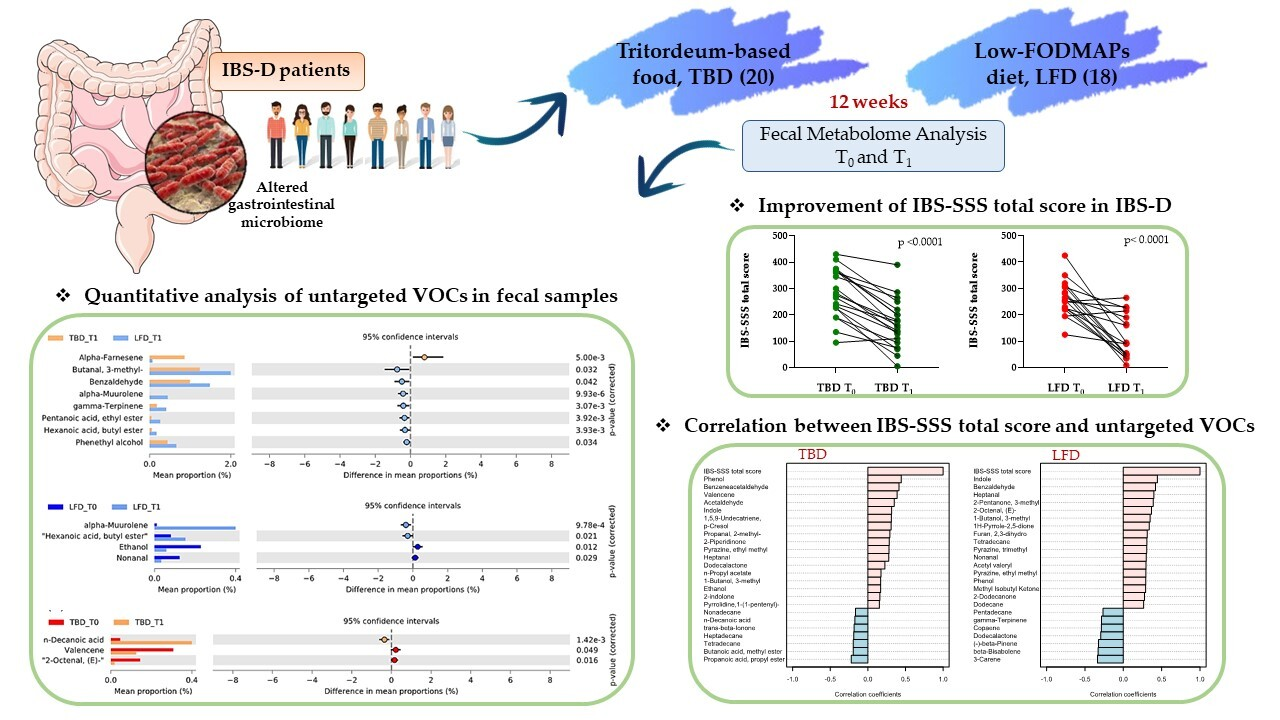
3.3. Fecal Metabolome Analysis
3.4. Correlations between IBS-SSS Score and Untargeted VOCs
3.5. Quantitative Analysis of Targeted VOCs in Fecal Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721. [Google Scholar] [CrossRef]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 30, 151–163. [Google Scholar] [CrossRef]
- Sobrado, C.W.; Corrêa, I.J.F.; Pinto, R.A.; Sobrado, L.F.; Nahas, S.C.; Cecconello, I. Diagnosis and treatment of constipation: A clinical update based on the Rome IV criteria. J. Coloproctol. 2018, 38, 137–144. [Google Scholar] [CrossRef]
- Bellini, M.; Tonarelli, S.; Barracca, F.; Morganti, R.; Pancetti, A.; Bertani, L.; de Bortoli, N.; Costa, F.; Mosca, M.; Marchi, S.; et al. A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up. Nutrients 2020, 12, 2360. [Google Scholar] [CrossRef]
- Altobelli, E.; Del Negro, V.; Angeletti, P.M.; Latella, G. Low-FODMAP Diet Improves Irritable Bowel Syndrome Symptoms: A Meta-Analysis. Nutrients 2017, 26, 940. [Google Scholar] [CrossRef]
- Linsalata, M.; Riezzo, G.; Orlando, A.; D’Attoma, B.; Prospero, L.; Tutino, V.; Notarnicola, M.; Russo, F. The Relationship between Low Serum Vitamin D Levels and Altered Intestinal Barrier Function in Patients with IBS Diarrhoea Undergoing a Long-Term Low-FODMAP Diet: Novel Observations from a Clinical Trial. Nutrients 2021, 13, 1011. [Google Scholar] [CrossRef]
- Orlando, A.; Tutino, V.; Notarnicola, M.; Riezzo, G.; Linsalata, M.; Clemente, C.; Prospero, L.; Martulli, M.; D’Attoma, B.; De Nunzio, V.; et al. Improved Symptom Profiles and Minimal Inflammation in IBS-D Patients Undergoing a Long-Term Low-FODMAP Diet: A Lipidomic Perspective. Nutrients 2020, 12, 1652. [Google Scholar] [CrossRef]
- Cubero, J.I.; Martin, A.; Millan, T.; Gómez-Cabrera, A.; De Haro, A. Tritordeum: A New Alloploid of Potential Importance as a Protein Source Crop 1. Crop Sci. 1986, 26, 1186–1190. [Google Scholar] [CrossRef]
- Martın, A.; Alvarez, J.B.; Martın, L.M.; Barro, F.; Ballesteros, J. The development of Tritordeum: A novel cereal for food processing. J. Cereal Sci. 1999, 30, 85–95. [Google Scholar] [CrossRef]
- Mellado-Ortega, E.; Hornero-Méndez, D. Carotenoid evolution during short-storage period of durum wheat (Triticum turgidum conv. durum) and tritordeum (× Tritordeum Ascherson et Graebner) whole-grain flours. Food Chem. 2016, 192, 714–723. [Google Scholar] [CrossRef]
- Eliášová, M.; Paznocht, L. Total phenolic content and antioxidant activity of tritordeum wheat and barley. Agron. Res. 2017, 15, 1287–1294. [Google Scholar]
- Roberfroid, M.B. Introducing inulin-type fructans. Br. J. Nutr. 2005, 93, S13–S25. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Riezzo, G.; Linsalata, M.; Orlando, A.; Tutino, V.; Prospero, L.; D’attoma, B.; Giannelli, G. Managing symptom profile of IBS-D patients with Tritordeum-based foods: Results from a pilot study. Front. Nutr. 2022, 9, 797192. [Google Scholar] [CrossRef]
- Sánchez-León, S.; Haro, C.; Villatoro, M.; Vaquero, L.; Comino, I.; González-Amigo, A.B.; Vivas, S.; Pastor, J.; Sousa, C.; Landa, B.B.; et al. Tritordeum breads are well tolerated with preference over gluten-free breads in non-celiac wheat-sensitive patients and its consumption induce changes in gut bacteria. J. Sci. Food Agric. 2021, 101, 3508–3517. [Google Scholar] [CrossRef]
- Iebba, V.; Totino, V.; Gagliardi, A.; Santangelo, F.; Cacciotti, F.; Trancassini, M.; Mancini, C.; Cicerone, C.; Corazziari, E.; Pantanella, F.; et al. Eubiosis and dysbiosis: The two sides of the microbiota. New Microbiol. 2016, 39, 1–12. [Google Scholar]
- Perrotta, G. The intestinal microbiota: Towards a multifactorial integrative model. Eubiosis and dysbiosis in morbid physical and psychological conditions. Arch. Clin. Gastroenterol. 2021, 7, 024–035. [Google Scholar]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef]
- Lauriero, G.; Abbad, L.; Vacca, M.; Celano, G.; Chemouny, J.M.; Calasso, M.; Berthelot, L.; Gesualdo, L.; De Angelis, M.; Monteiro, R.C. Fecal Microbiota Transplantation Modulates Renal Phenotype in the Humanized Mouse Model of IgA Nephropathy. Front. Immunol. 2021, 12, 694787. [Google Scholar] [CrossRef]
- Vitellio, P.; Celano, G.; Bonfrate, L.; Gobbetti, M.; Portincasa, P.; De Angelis, M. Effects of Bifidobacterium longum and Lactobacillus rhamnosus on Gut Microbiota in Patients with Lactose Intolerance and Persisting Functional Gastrointestinal Symptoms: A Randomised, Double-Blind, Cross-Over Study. Nutrients 2019, 11, 886. [Google Scholar] [CrossRef]
- Hsu, Y.L.; Chen, C.C.; Lin, Y.T.; Wu, W.K.; Chang, L.C.; Lai, C.H.; Wu, M.S.; Kuo, C.H. Evaluation and Optimization of Sample Handling Methods for Quantification of Short-Chain Fatty Acids in Human Fecal Samples by GC-MS. J. Proteome Res. 2019, 18, 1948–1957. [Google Scholar] [CrossRef]
- Shen, Q.; Zhao, L.; Tuohy, K. High-level dietary fibre up-regulates colonic fermentation and relative abundance of saccharolytic bacteria within the human faecal microbiota in vitro. Eur. J. Nutr. 2012, 51, 693–705. [Google Scholar] [CrossRef]
- Gonlachanvit, S.; Coleski, R.; Owyang, C.; Hasler, W. Inhibitory actions of a high fibre diet on intestinal gas transit in healthy volunteers. Gut 2004, 53, 1577–1582. [Google Scholar] [CrossRef]
- Zumarraga, L.; Suarez, F. Absence of gaseous symptoms during ingestion of commercial fibre preparations. Aliment. Pharmacol. Ther. 1997, 11, 1067–1072. [Google Scholar] [CrossRef]
- Elia, M.; Engfer, M.B.; Green, C.J.; Silk, D.B. Systematic review and meta-analysis: The clinical and physiological effects of fibre-containing enteral formulae. Aliment. Pharmacol. Ther. 2008, 27, 120–145. [Google Scholar] [CrossRef]
- Garner, C.E.; Smith, S.; de Lacy Costello, B.; White, P.; Spencer, R.; Probert, C.S.; Ratcliffem, N.M. Volatile organic compounds from feces and their potential for diagnosis of gastrointestinal disease. FASEB J. 2007, 21, 1675–1688. [Google Scholar] [CrossRef]
- Ahmed, I.; Greenwood, R.; Costello, B.; Ratcliffe, N.; Probert, C.S. Investigation of faecal volatile organic metabolites as novel diagnostic biomarkers in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2016, 43, 596–611. [Google Scholar] [CrossRef]
- Bilbrey, J.A.; Ortiz, Y.T.; Felix, J.S.; McMahon, L.R.; Wilkerson, J.L. Evaluation of the terpenes beta-caryophyllene, alpha-terpineol, and gamma-terpinene in the mouse chronic constriction injury model of neuropathic pain: Possible cannabinoid receptor involvement. Psychopharmacology 2022, 239, 1475–1486. [Google Scholar] [CrossRef]
- Zhgun, E.S.; Ilina, E.N. Fecal Metabolites As Non-Invasive Biomarkers of Gut Diseases. Acta Nat. 2020, 12, 4–14. [Google Scholar] [CrossRef]
- Topping, D.L.; Clifton, P.M. Short-chain fatty acids and human colonic function: Roles of resistant starch and nonstarch polysaccharides. Physiol. Rev. 2001, 81, 1031–1064. [Google Scholar] [CrossRef]
- Aravind, S.M.; Wichienchot, S.; Tsao, R.; Ramakrishnan, S.; Chakkaravarthi, S. Role of dietary polyphenols on gut microbiota, their metabolites and health benefits. Food Res. Int. 2021, 142, 110189. [Google Scholar] [CrossRef]
- Uchikawa, M.; Kato, M.; Nagata, A.; Sanada, S.; Yoshikawa, Y.; Tsunematsu, Y.; Sato, M.; Suzuki, T.; Hashidume, T.; Watanabe, K.; et al. Elevated levels of proinflammatory volatile metabolites in feces of high fat diet fed KK-A(y) mice. Sci. Rep. 2020, 10, 5681. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Yoon, J.-S.; Song, M.; Shin, C.-Y.; Chung, H.S.; Ryu, J.-C. Gene expression profiling of low dose exposure of saturated aliphatic aldehydes in A549 human alveolar epithelial cells. Toxicol. Environ. Health Sci. 2012, 4, 211–217. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef]
- Bonfrate, L.; Di Palo, D.M.; Celano, G.; Albert, A.; Vitellio, P.; De Angelis, M.; Gobbetti, M.; Portincasa, P. Effects of Bifidobacterium longum BB536 and Lactobacillus rhamnosus HN001 in IBS patients. Eur. J. Clin. Investig. 2020, 50, e13201. [Google Scholar] [CrossRef]
- Sam, Q.H.; Ling, H.; Yew, W.S.; Tan, Z.; Ravikumar, S.; Chang, M.W.; Chai, L.Y.A. The Divergent Immunomodulatory Effects of Short Chain Fatty Acids and Medium Chain Fatty Acids. Int. J. Mol. Sci. 2021, 22, 6453. [Google Scholar] [CrossRef]
- Lee, S.I.; Kang, K.S. Function of capric acid in cyclophosphamide-induced intestinal inflammation, oxidative stress, and barrier function in pigs. Sci. Rep. 2017, 7, 16530. [Google Scholar] [CrossRef]
- Geng, S.; Zhu, W.; Xie, C.; Li, X.; Wu, J.; Liang, Z.; Xie, W.; Zhu, J.; Huang, C.; Zhu, M.; et al. Medium-chain triglyceride ameliorates insulin resistance and inflammation in high fat diet-induced obese mice. Eur. J. Nutr. 2016, 55, 931–940. [Google Scholar] [CrossRef]
- Ringel-Kulka, T.; Choi, C.H.; Temas, D.; Kim, A.; Maier, D.M.; Scott, K.; Galanko, J.A.; Ringel, Y. Altered colonic bacterial fermentation as a potential pathophysiological factor in irritable bowel syndrome. Am. J. Gastroenterol. Suppl. 2015, 110, 1339. [Google Scholar] [CrossRef]
- Yusuf, F.; Adewiah, S.; Syam, A.F.; Fatchiyah, F. Altered profile of gut microbiota and the level short chain fatty acids in colorectal cancer patients. J. Phys. Conf. Ser. 2019, 1146, 012037. [Google Scholar] [CrossRef]
- Salem, A.E.; Singh, R.; Ayoub, Y.K.; Khairy, A.M.; Mullin, G.E. The gut microbiome and irritable bowel syndrome: State of art review. Arab. J. Gastroenterol. 2018, 19, 136–141. [Google Scholar]
- Tana, C.; Umesaki, Y.; Imaoka, A.; Handa, T.; Kanazawa, M.; Fukudo, S. Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Neurogastroenterol. Motil. 2010, 22, 512-e115. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | IBS-D Patients TBD (n = 20) | IBS-D Patients LFD (n = 18) | p |
|---|---|---|---|
| Age, years | 45.70 ± 10.20 | 42.90 ± 10.30 | 0.404 |
| Males/Females | 3/17 | 4/14 | |
| Weight (kg) | 69.80 ± 12.80 | 64.40 ± 13.30 | 0.293 |
| Height (m) | 1.62 ± 0.07 | 1.63 ± 0.10 | 0.823 |
| BMI (kg/m2) | 26.60 ± 4.70 | 24.03 ± 4.02 | 0.110 |
| Abdominal circumference (cm) | 93.50 ± 10.80 | 86.10 ± 10.40 | 0.060 |
| Waist circumference (cm) | 83.30 ± 13.30 | 77.02 ± 11.80 | 0.131 |
| TBD T0 (n = 20) | TBD T1 (n = 20) | p | LFD T0 (n = 18) | LFD1 (n = 18) | p | |
|---|---|---|---|---|---|---|
| Energy consumption (kcal) | 2206 ± 75 | 2235 ± 76 | 0.103 | 2142 ± 89 | 2136 ± 89 | 0.967 |
| Energy intake (kcal) | 1907 ± 137 | 1500 ± 27 | 0.021 | 2174 ± 176 | 1689 ± 93 | 0.014 |
| Basal metabolism (kcal) | 1454 ± 25 | 1471 ± 26 | 0.068 | 1500 ± 43 | 1505 ± 45 | 0.631 |
| Proteins (g) | 73 ± 4.5 | 75 ± 1.4 | 0.641 | 82.6 ± 6.1 | 83.3 ± 4.6 | 0.832 |
| Proteins (%) | 17 ± 0.4 | 20 ± 0.1 | <0.0001 | 16 ± 0.4 | 19 ± 0.2 | <0.0001 |
| Lipids (g) | 90 ± 8.9 | 50 ± 0.9 | <0.0001 | 94.1 ± 10.0 | 55 ± 3.4 | 0.0007 |
| Lipids (%) | 42 ± 1.5 | 30 ± 0.1 | <0.0001 | 36.3 ± 1.2 | 30.8 ± 0.2 | <0.0001 |
| Carbohydrates (g) | 192 ± 13 | 198 ± 4.1 | 0.615 | 229 ± 12 | 228 ± 14 | 0.609 |
| Carbohydrates (%) | 41 ± 1.8 | 50 ± 0.2 | <0.0001 | 47.7 ± 1.3 | 50.2 ± 0.3 | 0.02 |
| Alcohol (%) | 0.76 ± 0.3 | 0.49 ± 0.2 | 0.989 | 0.8 ± 0.3 | 0.29 ± 0.3 | 0.232 |
| Dietary fiber (g) | 14 ± 1.0 | 15 ± 0.4 | 0.383 | 16 ± 0.9 | 16 ± 0.9 | 0.330 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caponio, G.R.; Celano, G.; Calabrese, F.M.; Riezzo, G.; Orlando, A.; D’Attoma, B.; Ignazzi, A.; Vacca, M.; Porrelli, A.; Tutino, V.; et al. Evaluation of the Effects of the Tritordeum-Based Diet Compared to the Low-FODMAPs Diet on the Fecal Metabolome of IBS-D Patients: A Preliminary Investigation. Nutrients 2022, 14, 4628. https://doi.org/10.3390/nu14214628
Caponio GR, Celano G, Calabrese FM, Riezzo G, Orlando A, D’Attoma B, Ignazzi A, Vacca M, Porrelli A, Tutino V, et al. Evaluation of the Effects of the Tritordeum-Based Diet Compared to the Low-FODMAPs Diet on the Fecal Metabolome of IBS-D Patients: A Preliminary Investigation. Nutrients. 2022; 14(21):4628. https://doi.org/10.3390/nu14214628
Chicago/Turabian StyleCaponio, Giusy Rita, Giuseppe Celano, Francesco Maria Calabrese, Giuseppe Riezzo, Antonella Orlando, Benedetta D’Attoma, Antonia Ignazzi, Mirco Vacca, Annalisa Porrelli, Valeria Tutino, and et al. 2022. "Evaluation of the Effects of the Tritordeum-Based Diet Compared to the Low-FODMAPs Diet on the Fecal Metabolome of IBS-D Patients: A Preliminary Investigation" Nutrients 14, no. 21: 4628. https://doi.org/10.3390/nu14214628
APA StyleCaponio, G. R., Celano, G., Calabrese, F. M., Riezzo, G., Orlando, A., D’Attoma, B., Ignazzi, A., Vacca, M., Porrelli, A., Tutino, V., De Angelis, M., Giannelli, G., & Russo, F. (2022). Evaluation of the Effects of the Tritordeum-Based Diet Compared to the Low-FODMAPs Diet on the Fecal Metabolome of IBS-D Patients: A Preliminary Investigation. Nutrients, 14(21), 4628. https://doi.org/10.3390/nu14214628