
Real World Practice Study of the Effect of a Specific Oral Nutritional Supplement for Diabetes Mellitus on the Morphofunctional Assessment and Protein Energy Requirements

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
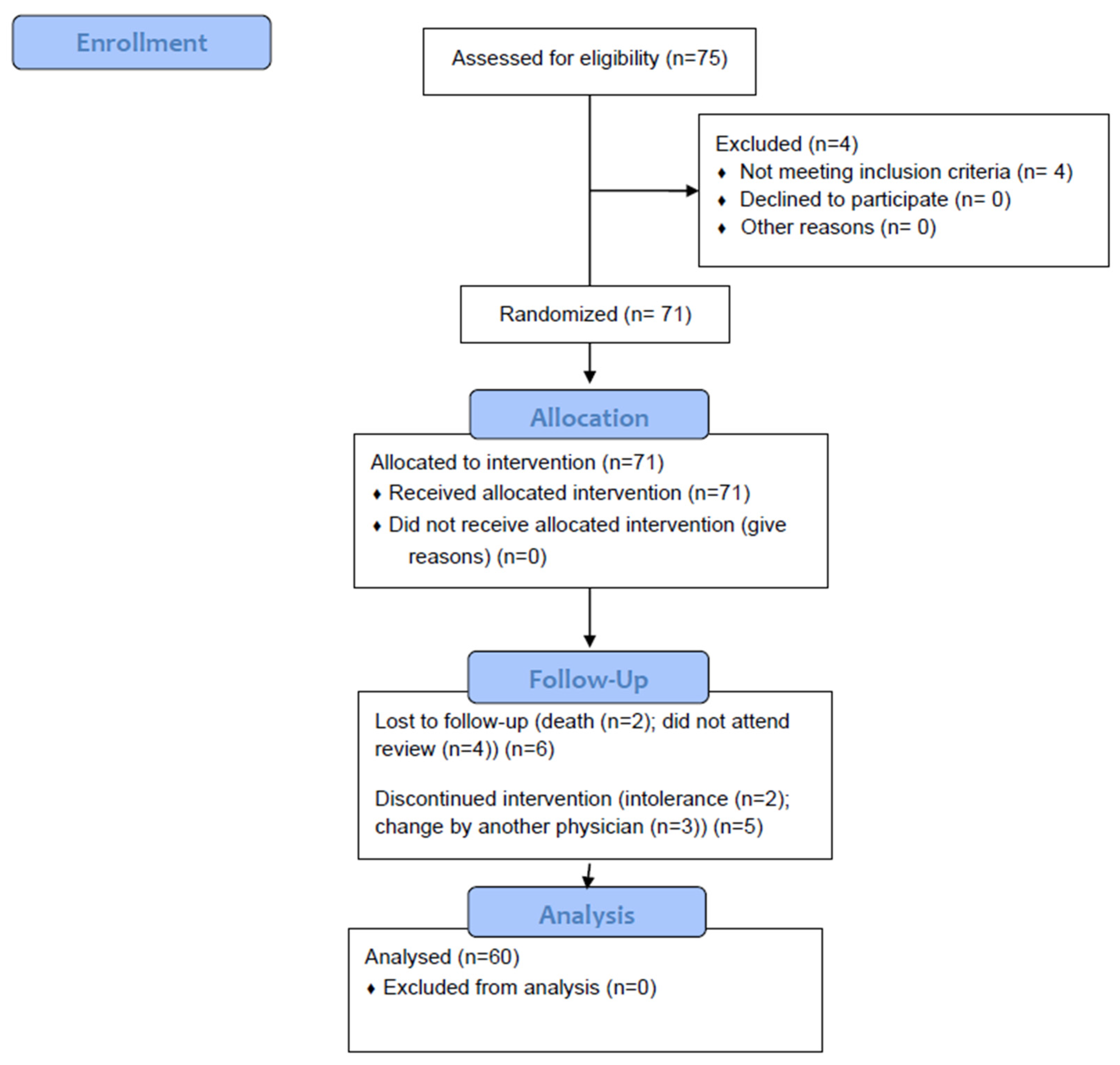
2.1. Design
2.2. Study Subjects
2.3. Nutritional Intervention
- Patients received education on adapted oral diet to increase calories and protein in patients with diabetes or carbohydrate metabolism disorders (prediabetes).
- Patients received nutritional education with a dietitian in adaptation of oral diet to increase protein–energy intake and they received education in consumption of oral nutritional supplementation. The adherence of these diets was assessed every fourteen days with a phone call by a dietitian to improve the calorie restriction and macronutrient distribution. The diet compliance was verified with a telephone nutritional questionnaire every fourteen days and a four-day nutritional questionnaire during face-to-face visits.
- Oral nutritional supplementation with a hyperproteic normocaloric formula specific for diabetes (carbohydrates with a low glycemic index, insoluble fiber) (Nutavant Plus Diabetica®) (Table 1). The amount (1 or 2 bottles) was adjusted according to the nutritional requirements of the patient and the estimation of usual intake [16,17].
2.4. Study Variables
- Clinical variables: Age (years); gender (male/female); systolic and diastolic blood pressure (mmHg); presence of concomitant pathologies.
- Anthropometry: The anthropometric variables measured were weight (kg); height (meters); body mass index (BMI) (weight/height × height) (kg/m2); arm circumference (AC); and calf circumference (CC). The percentage of weight loss was calculated: Start Weight Loss = ((Usual weight (kg) – Present weight (kg))/Usual weight) × 100; and 3 Months Weight Loss = ((Initial weight (kg) − 3 months weight)/Initial weight) × 100.
- Biochemical variables: They were performed with a Cobas c-711 autoanalyzer (Roche Diagnostics): Glucose (mg/dL); total cholesterol (mg/dL); HDL cholesterol (mg/dL); LDL cholesterol (mg/dL); triglycerides (mg/dL); albumin (g/dL); HbA1c (%), C-Reactive Protein (CRP) (mg/dL), prealbumin (mg/dL); and CRP/prealbumin ratio.
- Energy Expenditure and Nutritional Requirements: The energy expenditure of the patients was determined by means of the Harris–Benedict Equation multiplied by a Stress Factor of 1.3 and the protein requirements were determined by means of the factor 1–1.5 g of protein per kilogram of the patient’s adjusted weight. We based the requirements on the patient’s clinical situation and comorbidities as the recommendations made by the clinical guidelines of the European Society for Clinical Nutrition and Metabolism in surgery and oncology suggests. This decision was made because most of the patients had underlying oncological and/or surgical pathology [18,19].
- Nutritional questionnaire: All subjects completed a 4-day prospective nutritional questionnaire to assess calorie and macronutrient intake. This questionnaire was conducted before starting the intervention and 3 months after its start. The importance of not modifying dietary habits was insisted on so that it would be representative. All study participants were instructed to record food intake, daily and prospectively, with the help of food scales to facilitate precision in portion sizes. They were also asked about the way of preparing said foods. Records were reviewed by a dietitian and analyzed by a Dietsource® data processing computer system (Nestle, Geneve, Switzerland). Total calorie intake was used as an indicator of nutritional intake. No subject was taking dietary supplements or following any type of diet at the start of the study or in the 6 months prior to the study. Nutritional intake was measured in absolute values (in kilocalories (kcal) or grams (g)) and in percentages of the total caloric value. The nutritional questionnaire assessed the total energy intake, measured in kilocalories, as well as the different macronutrients: proteins, carbohydrates, fats and fiber, all of them measured in grams. The amount of protein ingested per kilogram of body weight was also calculated.
- Muscle functionality variables: Hand dynamometry (JAMAR® dynamometer): non-dominant hand dynamometry was performed with the patient seated and the arm at a right angle to the forearm. Three measurements were made and the average of the three measurements was made. The diagnostic criteria of low muscle strength proposed by the European Working Group on sarcopenia in older people (EWGSOP2) [20] were used. (<27 kg in men and <16 kg in women).
- Corporal Composition:
- Malnutrition and Sarcopenia diagnosis: The diagnosis of malnutrition was made using the Global Leadership Initiative on Malnutrition (GLIM) criteria, using the ASMI estimated by bioimpedance measurement measured by impedance measurement as an evaluation variable for muscle deterioration (ASMI muscle mass reduction < 7 kg/m2 in men was considered and <5.5 kg/m2 in women) [8]. On the other hand, the diagnosis of sarcopenia was made according to the revised criteria for sarcopenia of the EWGSOP2, using the ASMI estimated by bioimpedance as a determination of decreased muscle mass with handgrip strength to estimate the function to diagnose sarcopenia [20].
2.5. Data Analysis
3. Results
3.1. Sample Description
3.2. Nutrional Therapy Intervention
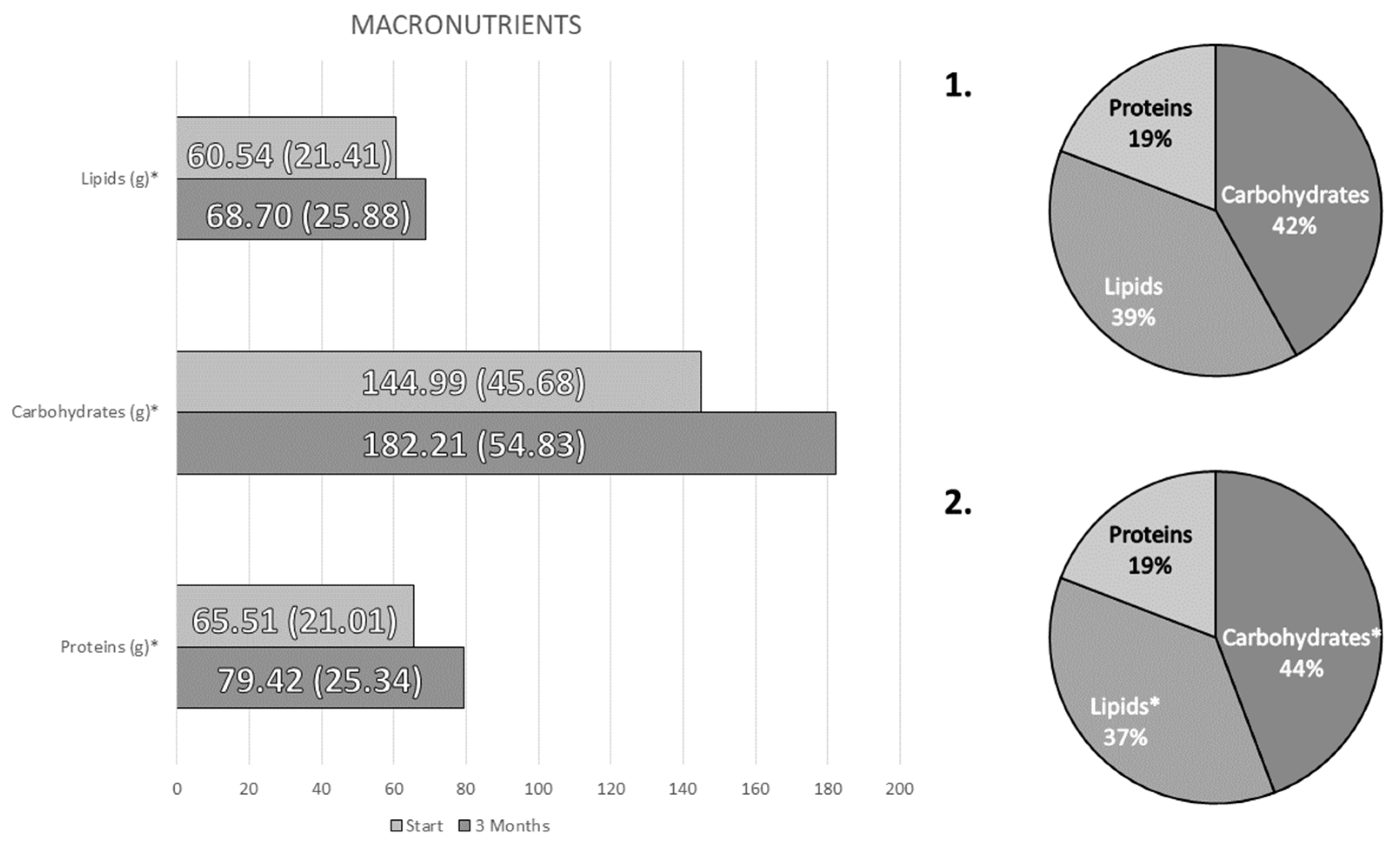
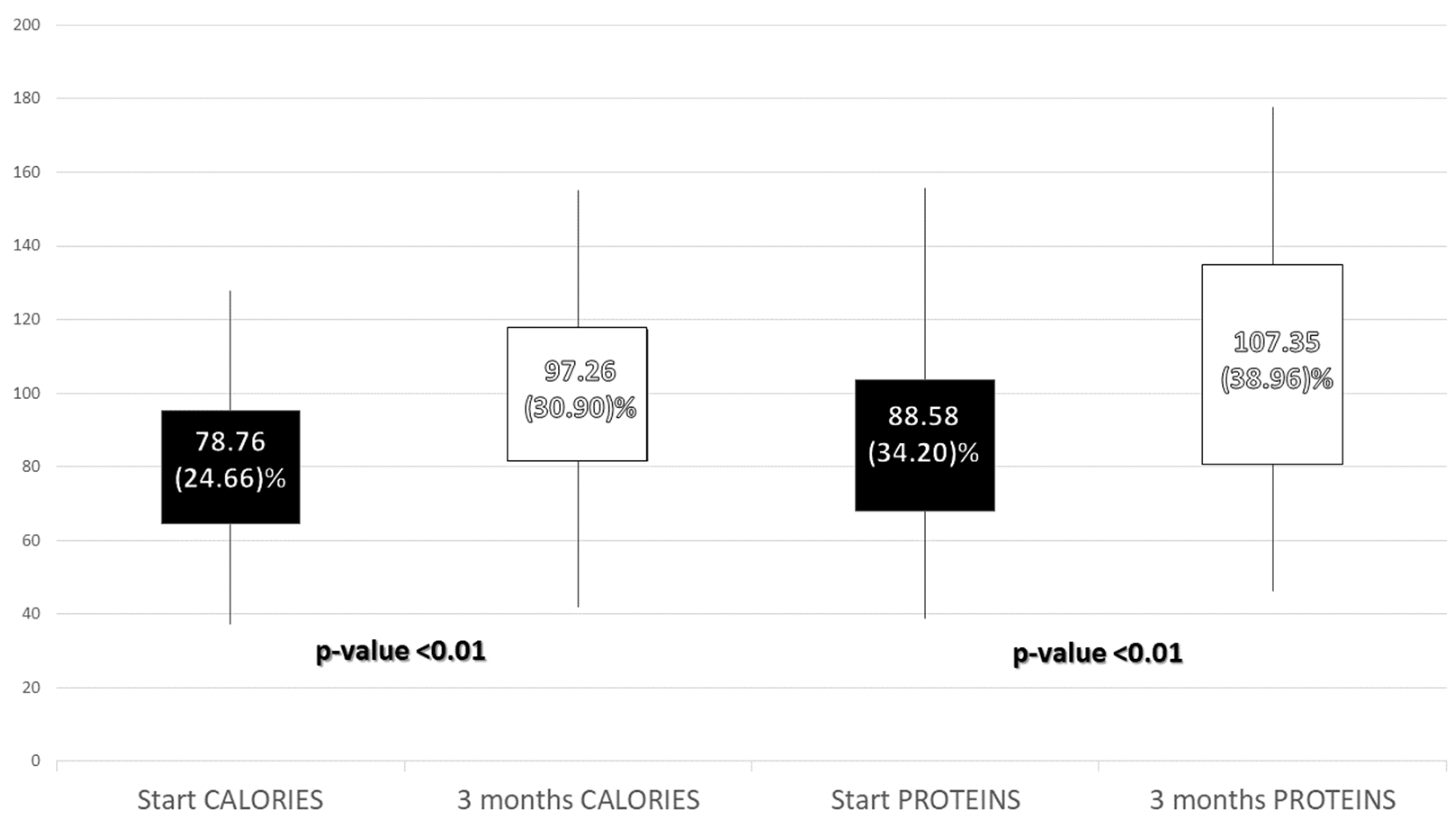
- Influence of the intervention on intake
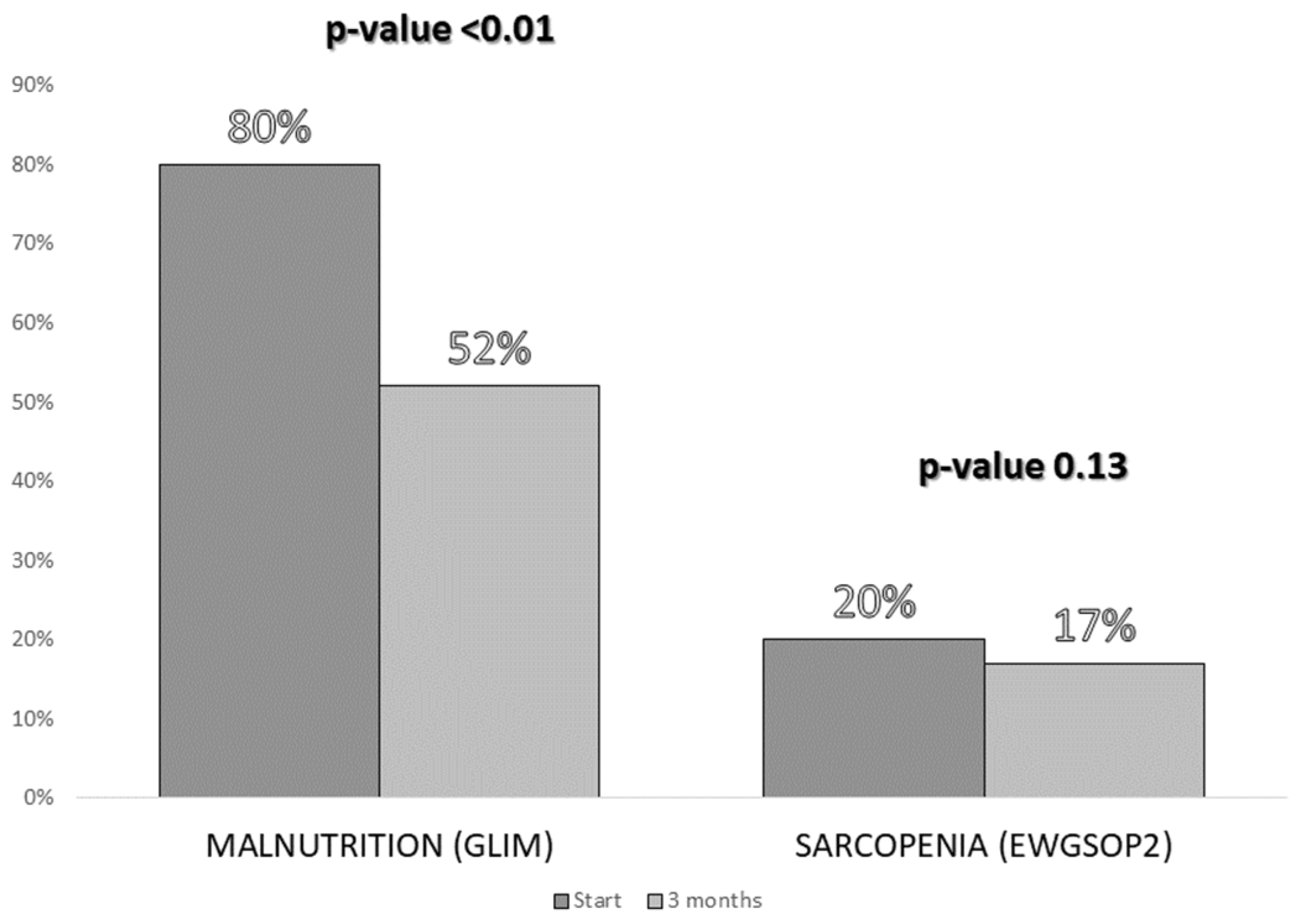
- Influence of the intervention on body composition
- Influence of the intervention on biochemical parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- León-Sanz, M.; Brosa, M.; Planas, M.; García-de-Lorenzo, A.; Celaya-Pérez, S.; Hernández, J.Á.; Predyces Group Researchers. PREDyCES study: The cost of hospital malnutrition in Spain. Nutrition 2015, 31, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Sanz París, A.; García, J.M.; Gómez-Candela, C.; Burgos, R.; Martín, Á.; Matía, P.; Study VIDA group. Malnutrition prevalence in hospitalized elderly diabetic patients. Nutr. Hosp. 2013, 28, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Serrano Valles, C.; López Gómez, J.J.; García Calvo, S.; Jiménez Sahagún, R.; Torres Torres, B.; Gómez Hoyos, E.; Buigues, A.O.; de Luis Román, D. Influencia del estado nutricional sobre la estancia media hospitalaria en el paciente con diabetes mellitus tipo 2. Endocrinol. Diabetes Nutr. 2020, 67, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Tan, Y.; Shi, Y.; Wang, X.; Liao, Z.; Wei, P. Diabetes and Sarcopenic Obesity: Pathogenesis, Diagnosis, and Treatments. Front. Endocrinol. 2020, 11, 568. [Google Scholar] [CrossRef]
- Takahashi, F.; Hashimoto, Y.; Kaji, A.; Sakai, R.; Okamura, T.; Kitagawa, N.; Okada, H.; Nakanishi, N.; Majima, S.; Senmaru, T.; et al. Sarcopenia Is Associated With a Risk of Mortality in People With Type 2 Diabetes Mellitus. Front. Endocrinol. 2021, 12, 783363. [Google Scholar] [CrossRef]
- Sugimoto, K.; Ikegami, H.; Takata, Y.; Katsuya, T.; Fukuda, M.; Akasaka, H.; Tabara, Y.; Osawa, H.; Hiromine, Y.; Rakugi, H. Glycemic Control and Insulin Improve Muscle Mass and Gait Speed in Type 2 Diabetes: The MUSCLES-DM Study. J. Am. Med. Dir. Assoc. 2021, 22, 834–838.e1. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef]
- García Almeida, J.M.; García García, C.; Vegas Aguilar, I.M.; Bellido Castañeda, V.; Bellido Guerrero, D. Morphofunctional assessment of patient´s nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar] [CrossRef] [PubMed]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Ballesteros Pomar, M.D.; Cornejo-Pareja, I.M.; Fernández Medina, B.; de Luis Román, D.A.; Guerrero, D.B.; Lesmes, I.B.; Madueño, F.J.T. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2022, S2530016422001471. [Google Scholar] [CrossRef]
- Pedrazzoli, P.; Caccialanza, R.; Cotogni, P.; Degli Esposti, L.; Perrone, V.; Sangiorgi, D.; Di Costanzo, F.; Gavazzi, C.; Santoro, A.; Pinto, C. The Advantages of Clinical Nutrition Use in Oncologic Patients in Italy: Real World Insights. Healthcare 2020, 8, 125. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, E.; Morita, S.; Nagashima, H.; Oshio, K.; Iwamoto, H.; Miyaji, K. Blood Glucose Response of a Low-Carbohydrate Oral Nutritional Supplement with Isomaltulose and Soluble Dietary Fiber in Individuals with Prediabetes: A Randomized, Single-Blind Crossover Trial. Nutrients 2022, 14, 2386. [Google Scholar] [CrossRef] [PubMed]
- Sanz-París, A.; Matía-Martín, P.; Martín-Palmero, Á.; Gómez-Candela, C.; Camprubi Robles, M. Diabetes-specific formulas high in monounsaturated fatty acids and metabolic outcomes in patients with diabetes or hyperglycaemia. A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 3273–3282. [Google Scholar] [CrossRef]
- de Souza, M.T.P.; Ozorio, G.A.; de Oliveira, G.N.; López, R.V.M.; Alves-Almeida, M.M.F.; Kulcsar, M.A.V.; Ribeiro, U., Jr.; Singer, P.; Waitzberg, D.L. Effect of age on resting energy expenditure in patients with cancer. Nutrition 2022, 102, 111740. [Google Scholar] [CrossRef]
- Long, C.L.; Schaffel, N.; Geiger, J.W.; Schiller, W.R.; Blakemore, W.S. Metabolic response to injury and illness: Estimation of energy and protein needs from indirect calorimetry and nitrogen balance. JPEN J. Parenter Enteral. Nutr. 1979, 3, 452–456. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Candela, C.; Luengo, L.M.; Cos, A.I.; Martínez-Roque, V.; Iglesias, C.; Zamora, P.; González-Barón, R. Subjective global assessment in neoplastic patients. Nutr. Hosp. 2003, 18, 353–357. [Google Scholar] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Lee, J.S.; Kuller, L.H.; Boudreau, R.; de Rekeneire, N.; Harris, T.B.; Kritchevsky, S.; Tylavsky, F.A.; Nevitt, M.; et al. Excessive Loss of Skeletal Muscle Mass in Older Adults With Type 2 Diabetes. Diabetes Care 2009, 32, 1993–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massimino, E.; Izzo, A.; Riccardi, G.; Della Pepa, G. The Impact of Glucose-Lowering Drugs on Sarcopenia in Type 2 Diabetes: Current Evidence and Underlying Mechanisms. Cells 2021, 10, 1958. [Google Scholar] [CrossRef]
- Eckel, J. Myokines in metabolic homeostasis and diabetes. Diabetologia 2019, 62, 1523–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Crockett, R.; Wang, X.-H. The Effect of Diabetes-Specific Enteral Nutrition Formula on Cardiometabolic Parameters in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2019, 11, 1905. [Google Scholar] [CrossRef] [Green Version]
- Maykish, A.; Sikalidis, A.K. Utilization of Hydroxyl-Methyl Butyrate, Leucine, Glutamine and Arginine Supplementation in Nutritional Management of Sarcopenia—Implications and Clinical Considerations for Type 2 Diabetes Mellitus Risk Modulation. J. Pers. Med. 2020, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Mustad, V.A.; Hegazi, R.A.; Hustead, D.S.; Budiman, E.S.; Rueda, R.; Maki, K.; Powers, M.; Mechanick, J.I.; Bergenstal, R.M.; Hamdy, O. Use of a diabetes-specific nutritional shake to replace a daily breakfast and afternoon snack improves glycemic responses assessed by continuous glucose monitoring in people with type 2 diabetes: A randomized clinical pilot study. BMJ Open Diabetes Res. Care 2020, 8, e001258. [Google Scholar] [CrossRef]
- Qian, F.; Korat, A.A.; Malik, V.; Hu, F.B. Metabolic Effects of Monounsaturated Fatty Acid-Enriched Diets Compared With Carbohydrate or Polyunsaturated Fatty Acid-Enriched Diets in Patients With Type 2 Diabetes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Diabetes Care 2016, 39, 1448–1457. [Google Scholar] [CrossRef] [Green Version]
- Angarita Dávila, L.; Bermúdez, V.; Aparicio, D.; Céspedes, V.; Escobar, M.C.; Durán-Agüero, S.; Cisternas, S.; de Assis Costa, J.; Rojas-Gómez, D.; Reyna, N.; et al. Effect of Oral Nutritional Supplements with Sucromalt and Isomaltulose versus Standard Formula on Glycaemic Index, Entero-Insular Axis Peptides and Subjective Appetite in Patients with Type 2 Diabetes: A Randomised Cross-Over Study. Nutrients 2019, 11, 1477. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diabetes Specific Formula (250 mL Bottle) | |
|---|---|
| Caloric Content (kcal) | 300 |
| Proteins (g (% TCV 1)) | 17 (22.66%) |
| Lipids (g (% TCV)) | 11.7 (35.1%) |
| Saturated (g) | 2.6 |
| MCT (g) | 1.7 |
| MUFA (g) | 5.9 |
| PUFA (g) | 2.8 |
| w-3 (g) | 0.83 |
| w-6 (g) | 1.88 |
| Carbohydrates (g (%TCV)) | 30 (40%) |
| Sugars (g) | 6.3 |
| Isomaltulose (g) | 3 |
| Minerals | |
| Sodium (mg) | 278 |
| Chloride (mg) | 113 |
| Potassium (mg) | 333 |
| Calcium (mg) | 275 |
| Phosphate (mg) | 238 |
| Magnesium (mg) | 50 |
| Iron (mg) | 2.8 |
| Zinc (mg) | 2 |
| Copper (mg) | 0,20 |
| Iodine (mg) | 30 |
| Selenium (mg) | 11 |
| Manganese (mg) | 0.40 |
| Chrome (mg) | 45 |
| Molybdenum (mg) | 10.6 |
| Fluoride (mg) | 0.58 |
| Vitamins | |
| Vitamin A (mg) | 160 |
| Vitamin D (mg) | 1.6 |
| Vitamin K (mg) | 15 |
| Vitamin C (mg) | 16 |
| Thiamin (mg) | 0.22 |
| Riboflavin (mg) | 0.28 |
| Vitamin B6 (mg) | 0.28 |
| Niacin (mg) | 3.3 |
| Folic Acid (mg) | 40 |
| Vitamin B12 (mg) | 0.50 |
| Pantothenic acid (mg) | 1.2 |
| Biotin (mg) | 10 |
| Vitamin E (mg) | 2.4 |
| Inositol (mg) | 38 |
| Choline (mg) | 38 |
| Osmolarity (mOsm/L) | 315 |
| Fiber (g) | 4.5 |
| Total | Men | Women | p-Value | |
|---|---|---|---|---|
| Sarcopenia (EWGSOP2) | 20% | 3.3% | 36.7% | <0.01 |
| Malnutrition (GLIM) | 80% | 86.7% | 73.3% | 0.19 |
| Diabetes Mellitus | 60% | 66.7% | 53.3% | 0.29 |
| Age (years) | 67.13 (14.9) | 68.70 (12.11) | 65.57 (15.89) | 0.39 |
| Anthropometry | ||||
| BMI (kg/m2) | 24.65 (5.35) | 25.53 (4.30) | 23.77 (6.18) | 0.20 |
| Braquial circumference (cm) | 24.71 (3.52) | 25.43 (2.53) | 23.99 (4.21) | 0,11 |
| Calf Circumference (cm) | 31.69 (3.61) | 32.75 (3.11) | 30.63 (3.81) | 0,02 |
| Handgrip Strength | ||||
| Handgrip Strength (kg) | 20.60 (8.26) | 25.42 (7.65) | 15.79 (5.67) | <0.01 |
| Bioelectrical Impedanciometry | ||||
| Resistance (ohm) | 545.4 (91.25) | 502.53 (75.11) | 588.27 (86.59) | <0.01 |
| Reactance (ohm) | 46.9 (9.26) | 44.7 (9.11) | 49.10 (9.01) | 0.06 |
| Fase Angle (°) | 4.95 | 5.11 (0.86) | 4.78 (0.66) | 0.11 |
| ASMI (kg/m2) | 6.43 (1.11) | 7.07 (0.91) | 5.79 (0.91) | <0.01 |
| FFMI (kg/m2) | 17.46 (3.05) | 18.27 (2.70) | 16.65 (3.20) | 0.04 |
| FMI (kg/m2) | 6.78 (3.32) | 6.58 (2.34) | 6.98 (4.10) | 0.64 |
| BCMI (kg/m2) | 8.29 (1.66) | 8.93 (1.69) | 7.64 (1.37) | <0.01 |
| %TBW | 56.17 (8.90) | 58.60 (4.49) | 53.75 (11.35) | 0.03 |
| Rectus Femoris Ultrasonography | ||||
| RFAI (cm2/m2) | 1.27 (0.47) | 1.36 (0.55) | 1.17 (0.35) | 0.14 |
| X/Y (cm2/m2) | 3.59 (1.57) | 3.39 (1.56) | 3.79 (1.57) | 0.34 |
| Total | Men | Women | p-Value | |
|---|---|---|---|---|
| Calories Requirement (kcal/day) | 1772 (178.12) | 1894 (149) | 1650 (107) | <0.01 |
| Calories Consumption (kcal/day) | 1364 (417) | 1333 (455) | 1433 (410) | 0.40 |
| Calories Consumption (%) | 78.76 (16.88) | 70.33 (22.83) | 86.87 (23.98) | 0.01 |
| Protein Requirements (g/day) | 79.26 (16.88) | 87.82 (12.33) | 70 (16.61) | <0.01 |
| Protein Consumption (g/day) | 1.15 (0.44) | 1.07 (0.41) | 1.22 (0.47) | 0.23 |
| Protein Consumption (%) | 88.58 (34.20) | 81.81 (31.27) | 94.13 (36.53) | 0.23 |
| Diabetes | No Diabetes | p-Value | |
|---|---|---|---|
| HbA1c (%) | 6.86 (1.19) | 6.03 (0.58) | <0.01 |
| Glucose (mg/dL) | 124.92 (38.19) | 94.62 (19.38) | <0.01 |
| Total cholesterol (mg/dL) | 153.75 (37.13) | 167 (39.95) | 0.19 |
| HDL cholesterol (mg/dL) | 57.81 (32.50) | 63.86 (23.60) | 0.45 |
| LDL cholesterol (mg/dL) | 79.54 (29,66) | 84.40 (23.93) | 0.53 |
| Tryglicerides (mg/dL) | 108.81 (54.06) | 81.79 (31.18) | 0.03 |
| Albumin (g/dL) | 4.06 (0.56) | 4.13 (0.38) | 0.59 |
| CRP/prealbumin | 0.43 (0.51) | 0.60 (0.89) | 0.37 |
| Start | 3 Months | p-Value | |
|---|---|---|---|
| Carbohydrates (g) | 144.99 (45.68) | 182.21 (54.83) | <0.01 |
| Fiber(g) | 12.53 (4.76) | 17.39 (7.14) | <0.01 |
| Proteins (g) | 65.51 (21.01) | 70.42 (25.34) | <0.01 |
| Lipids (g) | 60.54 (21.41) | 68.70 (25.88) | 0.03 |
| SFA (g) | 17.39 (8.42) | 19.77 (9.51) | 0.12 |
| SFA (%TCV) | 10.37 (8.2–14) | 9.69 (7.16–12.48) | 0.26 |
| MUFA (g) | 23.86 (10.99) | 28.94 (12.51) | 0.01 |
| MUFA (%TCV) | 15.35 (12.38–18.45) | 14.28 (12.53–18.45) | 0.55 |
| PUFA(g) | 6.17 (4.22) | 8.44 (3.68) | <0.01 |
| PUFA (%TCV) | 3.39 (2.86–4.56) | 4.09 (3.61–5.42) | <0.01 |
| EPA (g) | 0.08 (0.14) | 0.22 (0,56) | 0.12 |
| DHA (g) | 0.13 (0.20) | 0.16 (0.22) | 0.52 |
| Cholesterol (mg) | 300.85 (157.75) | 301.71 (196.96) | 0.37 |
| Minerals | |||
| Phosphorus (mg) | 881.10 (338.67) | 1116.27 (423.28) | <0.01 |
| Magnesium (mg) | 151.65 (60.31) | 202.09 (79.43) | <0.01 |
| Calcium (mg) | 708.59 (327.23) | 982.12 (377.23) | <0.01 |
| Iron (mg) | 7.71 (3.09) | 10.28 (4.17) | <0.01 |
| Zinc (mg) | 6.64 (3.25) | 8.09 (3.66) | <0.01 |
| Sodium (mg) | 1569.35 (845.39) | 1742.61 (824.38) | 0.12 |
| Potassium (mg) | 1943.22 (687.02) | 2205.49 (824.09) | 0.04 |
| Iodine (mg) | 30.83 (25.16) | 60.63 (33.64) | <0.01 |
| Selenium (mg) | 35.39 (24.01) | 50.66 (27.62) | 0.01 |
| Copper (mg) | 0.77 (0.54) | 0.93 (0.49) | 0.08 |
| Vitamins | |||
| Vitamin A (IU) | 1152.26 (1263.39) | 1347.76 (973.54) | 0.40 |
| Vitamin B1 (mg) | 0.89 (0.46) | 1.04 (0.72) | 0.20 |
| Vitamin B2 (mg) | 1.19 (0.59) | 1.51 (0.69) | <0.01 |
| Niacin (mg) | 11.96 (6.85) | 13.84 (6.77) | 0.10 |
| Vitamin B5 (mg) | 0.14 (0.42) | 1.22 (1.00) | <0.01 |
| Vitamin B6 (mg) | 1.17 (0.61) | 1.43 (0.68) | 0.01 |
| Folic Acid (mg) | 138.75 (75.32) | 174.29 (88.33) | 0.01 |
| Vitamin B12 (mg) | 5.54 (7.88) | 5.26 (4.50) | 0.83 |
| Vitamin C (mg) | 96.55 (67.59) | 109.29 (71.45) | 0.33 |
| Vitamin D (mg) | 4.02 (6.41) | 4.96 (5.57) | 0.40 |
| Vitamin E (mg) | 5.77 (3.33) | 7.62 (3.89) | <0.01 |
| Vitamin K (mg) | 1.52 (5.97) | 16.93 (15.81) | <0.01 |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Anthropometry | ||||||
| Baseline | 3 Months | p-Value | Baseline | 3 Months | p-Value | |
| %Weight Loss | 10.05 (7.03) | −0.25(5.57) | <0.01 | 12.84 (13.04) | −0.72 (4.95) | <0.01 |
| BMI (kg/m2) | 25.53 (4.30) | 24.72 (4.04) | 0.21 | 23.77 (6.18) | 23.11 (5.56) | 0.53 |
| Arm circumference (cm) | 25.43 (2.53) | 25.67 (2.77) | 0.32 | 23.99 (4.21) | 24.16 (3.91) | 0.65 |
| Calf Circumference (cm) | 32.75 (3.11) | 33.33 (2.75) | 0.16 | 24.16 (3.91) | 30.63 (3.81) | 0.18 |
| Handgrip Strength | ||||||
| Handgrip Strength (kg) | 23.81 (7.61) | 24.03 (8.81) | 0.44 | 14.77 (6.66) | 15.13 (5.69) | 0.95 |
| Bioelectrical Impedanciometry | ||||||
| Resistance (ohm) | 501 (76) | 502 (85) | 0.95 | 588 (86) | 586 (87) | 0.83 |
| Reactance (ohm) | 44.61 (9.43) | 45.86 (11.43) | 0.51 | 49.10(9.01) | 49.43(11.29) | 0.82 |
| Phase Angle (°) | 5.11 (0.89) | 5.24 (1.15) | 0.42 | 4.78 (0.66) | 4.81 (0.79) | 0.84 |
| ASMI (kg/m2) | 7.11 (0.91) | 7.15 (0.94) | 0.71 | 5.79 (0.91) | 5.81 (0.94) | 0.71 |
| FFMI (kg/m2) | 18.35 (2.76) | 18.34 (2.80) | 0.98 | 16.65 (3.20) | 16.29 (2.19) | 0.46 |
| FMI (kg/m2) | 6.80 (2.15) | 6.72 (2.25) | 0.76 | 6.98 (4.10) | 6.85 (4.07) | 0.51 |
| BCMI (kg/m2) | 8.97 (1.74) | 9.09 (2.00) | 0.48 | 7.64 (1.37) | 7.67 (1.40) | 0.79 |
| %TBW | 58.18 (4.13) | 58.28 (4.83) | 0.88 | 53.75 (11.35) | 55.91 (7.17) | 0.32 |
| Rectus Femoris Ultrasonography | ||||||
| RFAI (cm2/m2) | 1.36 (0.55) | 1.31 (0.57) | 0.31 | 1.18 (0.35) | 1.14 (0.37) | 0.19 |
| X/Y (cm2/m2) | 3.39 (1.56) | 3.55 (1.48) | 0.46 | 3.79 (1.57) | 3.56 (1.24) | 0.46 |
| Diabetes | No Diabetes | |||||
|---|---|---|---|---|---|---|
| Baseline | 3 Months | p-value | Baseline | 3 Months | p-Value | |
| HbA1c (%) | 6.87 (1.24) | 7.18 (1.09) | 0.02 | 6.05 (0.60) | 6.10 (0.62) | 0.30 |
| Glucose (mg/dL) | 123.56 (38.79) | 131.38 (29.76) | 0.10 | 94.62 (19.39) | 89.83 (20.03) | 0.55 |
| Total cholesterol (mg/dL) | 154 (37.01) | 158 (38.99) | 0.29 | 167 (39.95) | 172 (46.22) | 0.49 |
| HDL cholesterol (mg/dL) | 58 (33.48) | 60.94 (27.87) | 0.25 | 65.50 (23.94) | 63.7 (20.79) | 0.34 |
| LDL cholesterol (mg/dL) | 79.45 (30.55) | 83.62 (31.35) | 0.29 | 88.83 (19.56) | 95.83 (43.66) | 0.45 |
| Tryglicerides (mg/dL) | 109.89 (55.15) | 105.34 (50.23) | 0.26 | 81.79 (31.18) | 86.92 (29.17) | 0.32 |
| Albumin (g/dL) | 4.09 (0.53) | 4.25 (0.42) | 0.02 | 4.13 (0.38) | 4.02 (0.42) | 0.14 |
| CRP/prealbumin | 0.38 (0.51) | 0.70 (2.07) | 0.38 | 0.47 (0.74) | 0.26 (0.38) | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gómez, J.J.; Gutiérrez-Lora, C.; Izaola-Jauregui, O.; Primo-Martín, D.; Gómez-Hoyos, E.; Jiménez-Sahagún, R.; De Luis-Román, D.A. Real World Practice Study of the Effect of a Specific Oral Nutritional Supplement for Diabetes Mellitus on the Morphofunctional Assessment and Protein Energy Requirements. Nutrients 2022, 14, 4802. https://doi.org/10.3390/nu14224802
López-Gómez JJ, Gutiérrez-Lora C, Izaola-Jauregui O, Primo-Martín D, Gómez-Hoyos E, Jiménez-Sahagún R, De Luis-Román DA. Real World Practice Study of the Effect of a Specific Oral Nutritional Supplement for Diabetes Mellitus on the Morphofunctional Assessment and Protein Energy Requirements. Nutrients. 2022; 14(22):4802. https://doi.org/10.3390/nu14224802
Chicago/Turabian StyleLópez-Gómez, Juan J., Cristina Gutiérrez-Lora, Olatz Izaola-Jauregui, David Primo-Martín, Emilia Gómez-Hoyos, Rebeca Jiménez-Sahagún, and Daniel A. De Luis-Román. 2022. "Real World Practice Study of the Effect of a Specific Oral Nutritional Supplement for Diabetes Mellitus on the Morphofunctional Assessment and Protein Energy Requirements" Nutrients 14, no. 22: 4802. https://doi.org/10.3390/nu14224802
APA StyleLópez-Gómez, J. J., Gutiérrez-Lora, C., Izaola-Jauregui, O., Primo-Martín, D., Gómez-Hoyos, E., Jiménez-Sahagún, R., & De Luis-Román, D. A. (2022). Real World Practice Study of the Effect of a Specific Oral Nutritional Supplement for Diabetes Mellitus on the Morphofunctional Assessment and Protein Energy Requirements. Nutrients, 14(22), 4802. https://doi.org/10.3390/nu14224802