
Investigating the Effectiveness of Very Low-Calorie Diets and Low-Fat Vegan Diets on Weight and Glycemic Markers in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis
 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration of Review Protocol
2.2. Databases and Search Terms
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias
2.6. Outcomes
2.7. Intervention Groups
2.8. Data Synthesis and Analysis
2.9. Subgroups Used to Explain Heterogeneity
3. Results
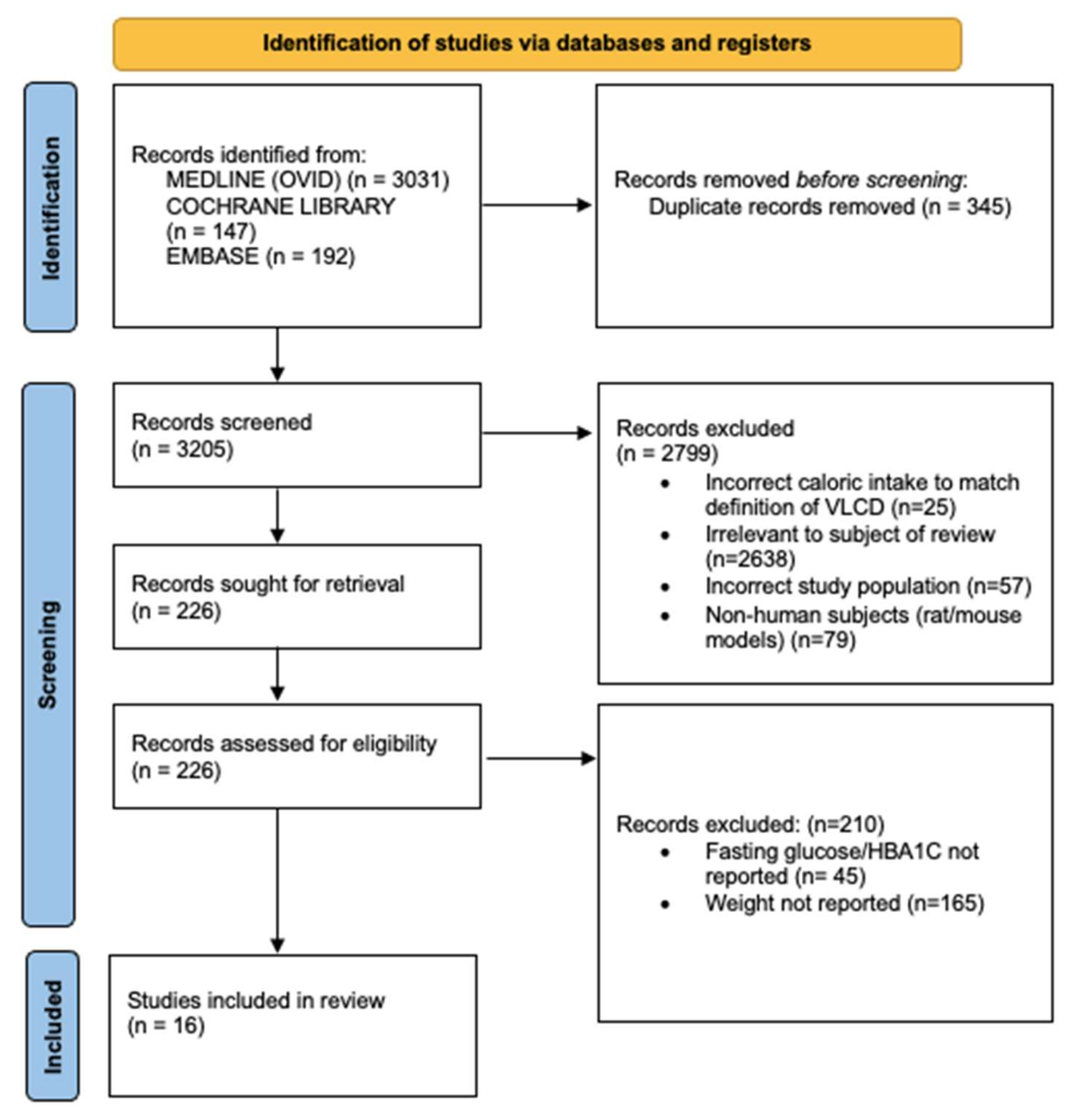
3.1. Database Search
3.2. Study Characteristics
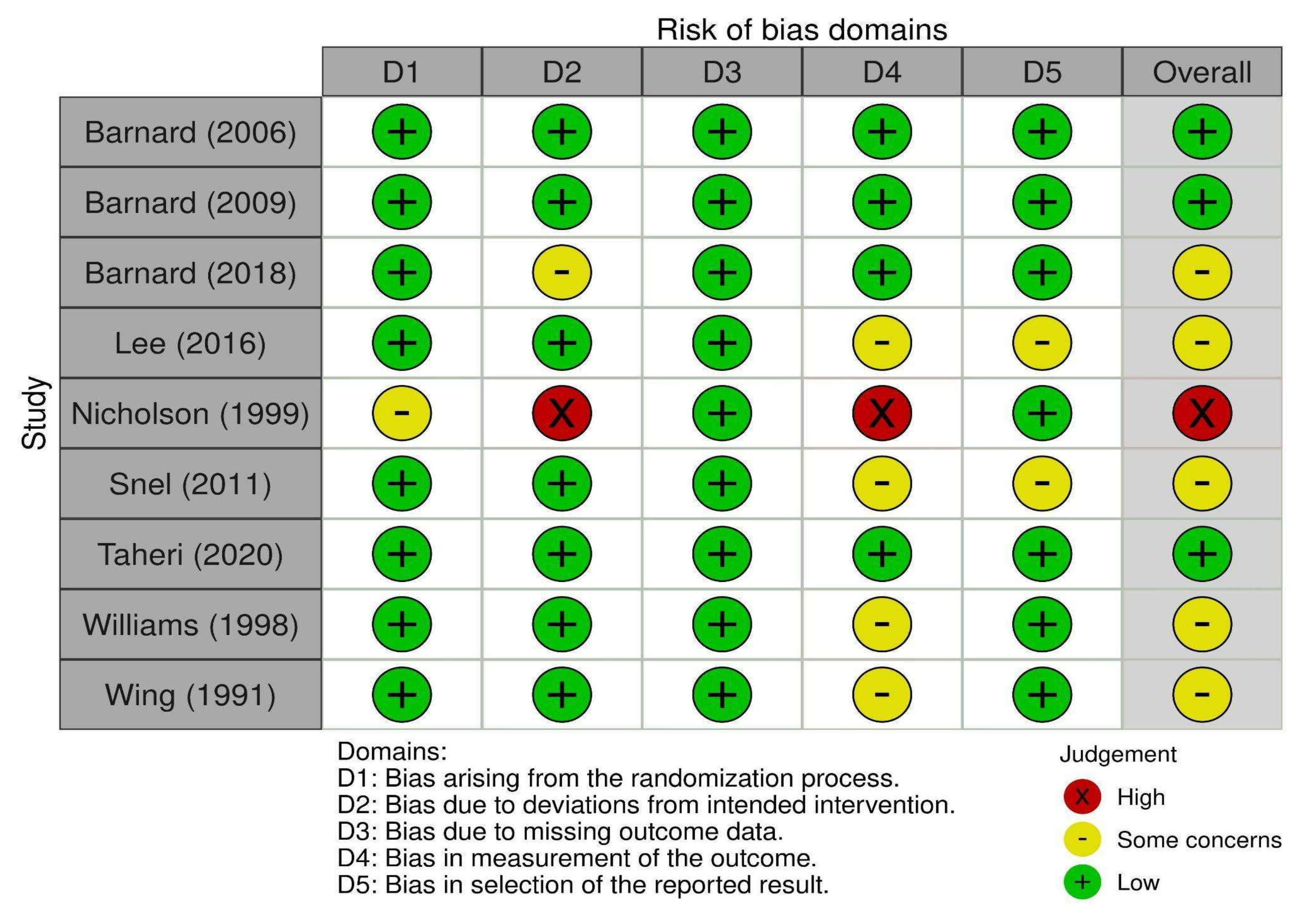
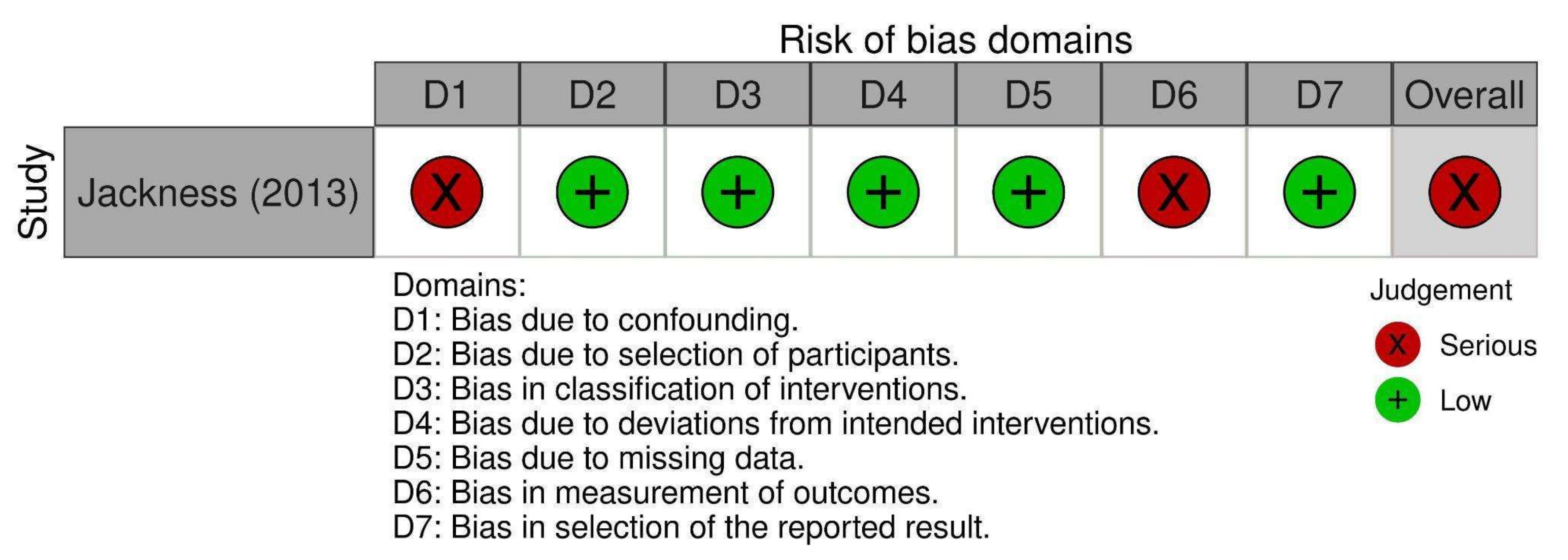
3.3. Risk of Bias
3.4. Comparison of Vegan Diets vs. Control Diets
3.4.1. Primary Outcomes
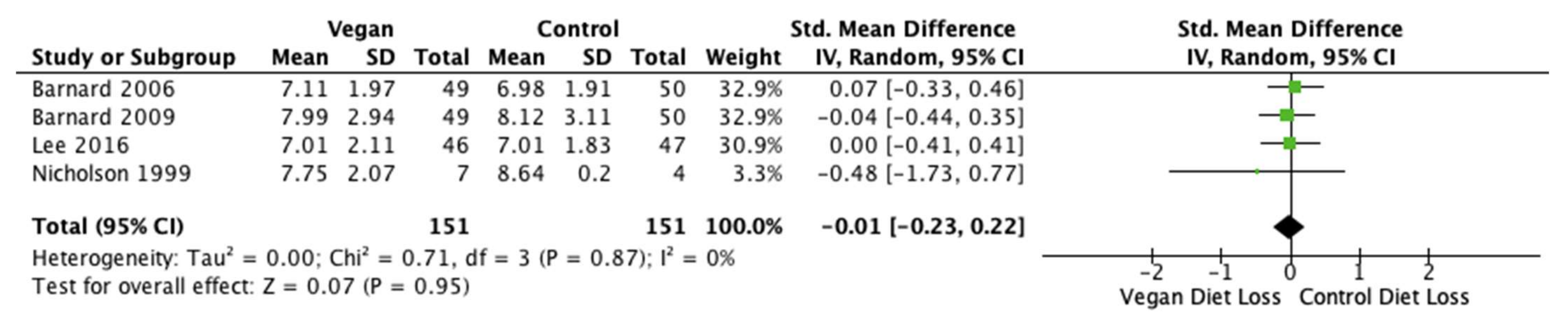
Body Weight
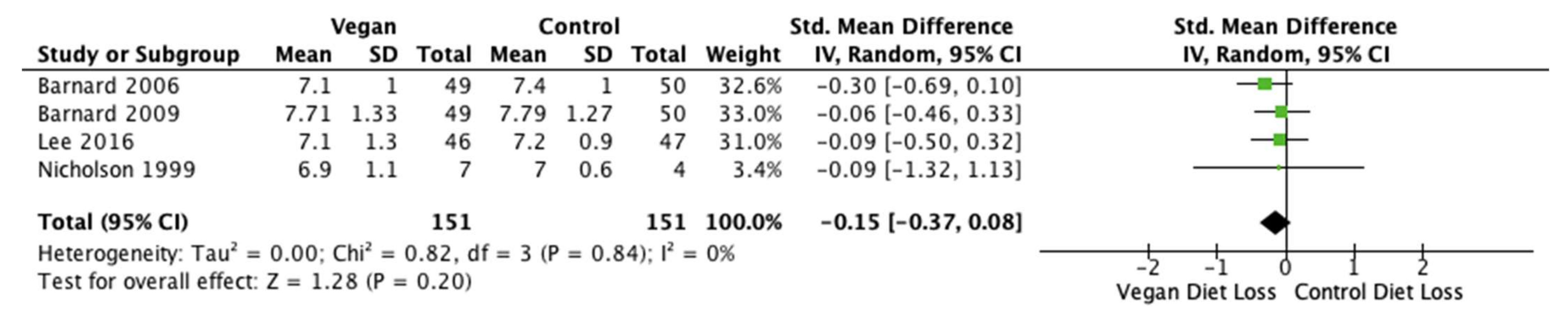
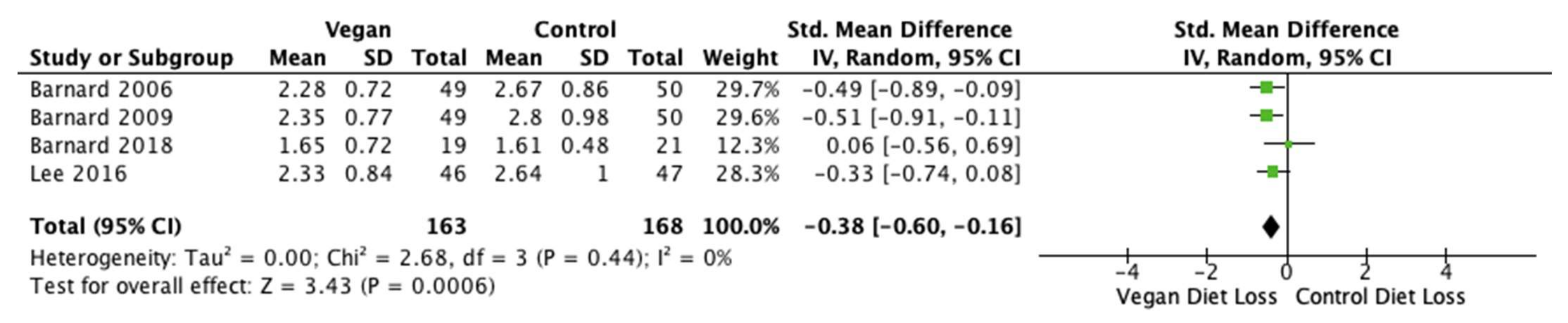
Fasting Glucose and HbA1c
3.4.2. Secondary Outcomes
Body Mass Index (BMI)
Triglycerides
Waist and Hip Circumferences and Waist-To-Hip Ratio
Total Cholesterol
HDL Cholesterol
LDL Cholesterol
3.5. Comparison of VLCD vs. Control
3.5.1. Primary Outcomes
Body Weight
Fasting Glucose
HbA1c
3.5.2. Secondary Outcomes
Body Mass Index (BMI)
Triglycerides
Waist and Hip Circumferences and Waist-To-Hip Ratio
Total Cholesterol
Fasting Insulin
HDL Cholesterol
LDL Cholesterol
Systolic Blood Pressure
Diastolic Blood Pressure
Urinary Albumin
4. Discussion
4.1. Summary of Main Findings
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowley, W.R.; Bezold, C.; Arikan, Y.; Byrne, E.; Krohe, S. Diabetes 2030: Insights from yesterday, today, and future trends. Popul. Health Manag. 2017, 20, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Facts & Figures. International Diabetes Federation. 2021. Available online: https://idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 18 August 2022).
- Karter, A.J.; Nundy, S.; Parker, M.M.; Moffet, H.H.; Huang, E.S. Incidence of remission in adults with type 2 diabetes: The diabetes & aging study. Diabetes Care 2014, 37, 3188–3195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 8. Obesity Management for the Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44 (Suppl. S1), S100–S110. [Google Scholar] [CrossRef]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: A systematic review and meta-analysis of randomized clinical trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef]
- Terranova, C.O.; Brakenridge, C.L.; Lawler, S.P.; Eakin, E.G.; Reeves, M.M. Effectiveness of lifestyle-based weight loss interventions for adults with type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2015, 17, 371–378. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2007, 30 (Suppl. S1), S48–S65. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, A.A.; Choudhari, P.K.; Mahajan, R.R.; Sayyad, M.G.; Pratyush, D.D.; Hasan, I.; Javherani, R.S.; Bothale, M.M.; Purandare, V.B.; Unnikrishnan, A.G. Effect of a low-calorie diet on restoration of normoglycemia in obese subjects with type 2 diabetes. Indian J. Endocrinol. Metab. 2017, 21, 776–780. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Giugliano, D. The effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care 2014, 37, 1824–1830. [Google Scholar] [CrossRef] [Green Version]
- Gregg, E.W.; Chen, H.; Wagenknecht, L.E.; Clark, J.M.; Delahanty, L.M.; Bantle, J.; Pownall, H.J.; Johnson, K.C.; Safford, M.M.; Kitabchi, A.E.; et al. Association of an intensive lifestyle intervention with remission of type 2 diabetes. JAMA 2012, 308, 2489–2496. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE) Clinical Guidelines. Very-low-calorie diets. In Obesity: Identification, Assessment and Management of Overweight and Obesity in Children, Young People and Adults: Partial Update of CG43; National Clinical Guideline Centre: London, UK, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK311324/ (accessed on 18 August 2022).
- Henry, R.R.; Scheaffer, L.; Olefsky, J.M. Glycemic effects of intensive caloric restriction and isocaloric refeeding in noninsulin-dependent diabetes mellitus. J Clin. Endocrinol. Metab. 1985, 61, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.A.; Gwynne, J.T.; Switzer, B.R.; Herbst, C.; White, G. Effects of caloric restriction and weight loss on glycemic control, insulin release and resistance, and atherosclerotic risk in obese patients with type II diabetes mellitus. Am. J. Med. 1984, 77, 7–17. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.L.; Hollingsworth, K.G.; Aribisala, B.S.; Chen, M.J.; Mathers, J.C.; Taylor, R. Reversal of type 2 diabetes: Normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011, 54, 2506–2514. [Google Scholar] [CrossRef] [Green Version]
- Malandrucco, I.; Pasqualetti, P.; Giordani, I.; Manfellotto, D.; De Marco, F.; Alegiani, F.; Sidoti, A.M.; Picconi, F.; Di Flaviani, A.; Frajese, G.; et al. Very-low-calorie diet: A quick therapeutic tool to improve β cell function in morbidly obese patients with type 2 diabetes. Am. J. Clin. Nutr. 2012, 95, 609–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathananthan, M.; Shah, M.; Edens, K.L.; Grothe, K.B.; Piccinini, F.; Farrugia, L.P.; Micheletto, F.; Man, C.D.; Cobelli, C.; Rizza, R.A.; et al. Six and 12 weeks of caloric restriction increases β cell function and lowers fasting and postprandial glucose concentrations in people with type 2 diabetes. J. Nutr. 2015, 145, 2046–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, P.J.; Bennion, L.J.; Flock, E.V.; Nagulesparan, M.; Mott, D.; Roth, J.; Unger, R.H.; Bennett, P.H. Diet-induced improvement of abnormalities in insulin and glucagon secretion and in insulin receptor binding in diabetes mellitus. J. Clin. Endocrinol. Metab. 1979, 48, 999–1007. [Google Scholar] [CrossRef]
- Steven, S.; Taylor, R. Restoring normoglycaemia by use of a very low calorie diet in long-and short-duration Type 2 diabetes. Diabet. Med. 2015, 32, 1149–1155. [Google Scholar] [CrossRef]
- Steven, S.; Hollingsworth, K.G.; Al-Mrabeh, A.; Avery, L.; Aribisala, B.; Caslake, M.; Taylor, R. Very low-calorie diet and 6 months of weight stability in type 2 diabetes: Pathophysiological changes in responders and nonresponders. Diabetes Care 2016, 39, 808–815. [Google Scholar] [CrossRef] [Green Version]
- Wing, R.R.; Marcus, M.D.; Salata, R.; Epstein, L.H.; Miaskiewicz, S.; Blair, E.H. Effects of a very-low-calorie diet on long-term glycemic control in obese type 2 diabetic subjects. Arch. Intern. Med. 1991, 151, 1334–1340. [Google Scholar] [CrossRef]
- Lonnie, M.; Johnstone, A.M. The public health rationale for promoting plant protein as an important part of a sustainable and healthy diet. Nutr. Bull. 2020, 45, 281–293. [Google Scholar] [CrossRef]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef] [PubMed]
- Lanou, A.J.; Svenson, B. Reduced cancer risk in vegetarians: An analysis of recent reports. Cancer Manag. Res. 2011, 3, 1–8. [Google Scholar] [CrossRef]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in US adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Barnard, N.D.; Cohen, J.; Jenkins, D.J.; Turner-McGrievy, G.; Gloede, L.; Jaster, B.; Seidl, K.; Green, A.A.; Talpers, S. A low-fat vegan diet improves glycemic control and cardiovascular risk factors in a randomized clinical trial in individuals with type 2 diabetes. Diabetes Care 2006, 29, 1777–1783. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Plant-based foods and prevention of cardiovascular disease: An overview. Am. J. Clin. Nutr. 2003, 78, 544S–551S. [Google Scholar] [CrossRef] [Green Version]
- Kahleova, H.; Levin, S.; Barnard, N. Cardio-metabolic benefits of plant-based diets. Nutrients 2017, 9, 848. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Barnard, N.D.; Cohen, J.; Jenkins, D.J.; Gloede, L.; Green, A.A. Changes in nutrient intake and dietary quality among participants with type 2 diabetes following a low-fat vegan diet or a conventional diabetes diet for 22 weeks. J. Am. Diet. Assoc. 2008, 108, 1636–1645. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kendall, C.W.; Marchie, A.; Faulkner, D.A.; Wong, J.M.; de Souza, R.; Emam, A.; Parker, T.L.; Vidgen, E.; Trautwein, E.A.; et al. Direct comparison of a dietary portfolio of cholesterol-lowering foods with a statin in hypercholesterolemic participants. Am. J. Clin. Nutr. 2005, 81, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Termannsen, A.D.; Clemmensen, K.K.B.; Thomsen, J.M.; Nørgaard, O.; Díaz, L.J.; Torekov, S.S.; Quist, J.S.; Færch, K. Effects of vegan diets on cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2022, 23, e13462. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franz, M.; Bantle, J.; Beebe, C.; Brunzell, J.; Chiasson, J.-L.; Garg, A.; Holzmeister, L.A.; Hoogwerf, B.; Mayer-Davis, E.; Mooradian, A.D.; et al. Evidence-Based Nutrition Principles and Recommendations for the Treatment and Prevention of Diabetes and Related Complications. Diabetes Care 2003, 26 (Suppl. S1), S51–S61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, S.-H.; Kim, S.-R.; Kim, D.-J.; Oh, S.-J.; Lee, H.-J.; Shim, K.-H.; Woo, M.-H.; Kim, J.-Y.; Kim, N.-H.; Kim, J.-T.; et al. 2011 Clinical Practice Guidelines for Type 2 Diabetes in Korea. Diabetes Metab. J. 2011, 35, 431–436. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Teeuwisse, W.M.; Widya, R.L.; Paulides, M.; Lamb, H.J.; Smit, J.W.; de Roos, A.; Van Buchem, M.A.; Pijl, H.; van der Grond, J. Short-term caloric restriction normalizes hypothalamic neuronal responsiveness to glucose ingestion in patients with type 2 diabetes. Diabetes 2012, 61, 3255–3259. [Google Scholar] [CrossRef] [Green Version]
- Barnard, N.D.; Katcher, H.I.; Jenkins, D.J.; Cohen, J.; Turner-McGrievy, G. Vegetarian and vegan diets in type 2 diabetes management. Nutr. Rev. 2009, 67, 255–263. [Google Scholar] [CrossRef]
- Nicholson, A.S.; Sklar, M.; Barnard, N.D.; Gore, S.; Sullivan, R.; Browning, S. Toward improved management of NIDDM: A randomized, controlled, pilot intervention using a lowfat, vegetarian diet. Prev. Med. 1999, 29, 87–91. [Google Scholar] [CrossRef]
- Jackness, C.; Karmally, W.; Febres, G.; Conwell, I.M.; Ahmed, L.; Bessler, M.; McMahon, D.J.; Korner, J. Very Low–Calorie diet mimics the early beneficial effect of Roux-en-Y gastric bypass on insulin sensitivity and β-cell function in type 2 diabetic patients. Diabetes 2013, 62, 3027–3032. [Google Scholar] [CrossRef]
- Snel, M.; Jonker, J.T.; Hammer, S.; Kerpershoek, G.; Lamb, H.J.; Meinders, A.E.; Pijl, H.; De Roos, A.; Romijn, J.A.; Smit, J.W.; et al. Long-term beneficial effect of a 16-week very low calorie diet on pericardial fat in obese type 2 diabetes mellitus patients. Obesity 2012, 20, 1572–1576. [Google Scholar] [CrossRef] [PubMed]
- Jazet, I.M.; Schaart, G.; Gastaldelli, A.; Ferrannini, E.; Hesselink, M.K.; Schrauwen, P.; Romijn, J.A.; Maassen, J.A.; Pijl, H.; Ouwens, D.M.; et al. Loss of 50% of excess weight using a very low energy diet improves insulin-stimulated glucose disposal and skeletal muscle insulin signalling in obese insulin-treated type 2 diabetic patients. Diabetologia 2008, 51, 309–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Škrha, J.; Kunešová, M.; Hilgertova, J.; Weiserova, H.; Křížová, J.; Kotrlikova, E. Short-term very low calory diet reduces oxidative stress in obese type 2 diabetic patients. Physiol. Res. 2005, 54, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.M.; Kim, S.A.; Lee, I.K.; Kim, J.G.; Park, K.G.; Jeong, J.Y.; Jeon, J.H.; Shin, J.Y.; Lee, D.H. Effect of a brown rice based vegan diet and conventional diabetic diet on glycemic control of patients with type 2 diabetes: A 12-week randomized clinical trial. PLoS ONE 2016, 11, e0155918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, N.D.; Levin, S.M.; Gloede, L.; Flores, R. Turning the waiting room into a classroom: Weekly classes using a vegan or a portion-controlled eating plan improve diabetes control in a randomized translational study. J. Acad. Nutr. Diet. 2018, 118, 1072–1079. [Google Scholar] [CrossRef] [Green Version]
- Snel, M.; van Diepen, J.A.; Stijnen, T.; Pijl, H.; Romijn, J.A.; Meinders, A.E.; Voshol, P.; Jazet, I.M. Immediate and long-term effects of addition of exercise to a 16-week very low calorie diet on low-grade inflammation in obese, insulin-dependent type 2 diabetic patients. Food Chem. Toxicol. 2011, 49, 3104–3111. [Google Scholar] [CrossRef]
- Taheri, S.; Zaghloul, H.; Chagoury, O.; Elhadad, S.; Ahmed, S.H.; El Khatib, N.; Abou Amona, R.; El Nahas, K.; Suleiman, N.; Alnaama, A.; et al. Effect of intensive lifestyle intervention on bodyweight and glycaemia in early type 2 diabetes (DIADEM-I): An open-label, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2020, 8, 477–489. [Google Scholar] [CrossRef]
- Williams, K.V.; Mullen, M.L.; Kelley, D.E.; Wing, R.R. The effect of short periods of caloric restriction on weight loss and glycemic control in type 2 diabetes. Diabetes Care 1998, 21, 2–8. [Google Scholar] [CrossRef]
- McCarty, M.F. An elevation of triglycerides reflecting decreased triglyceride clearance may not be pathogenic–relevance to high-carbohydrate diets. Med. Hypotheses 2004, 63, 1065–1073. [Google Scholar] [CrossRef]
- Barnard, N.D.; Scialli, A.R.; Turner-McGrievy, G.; Lanou, A.J.; Glass, J. The effects of a low-fat, plant-based dietary intervention on body weight, metabolism, and insulin sensitivity. Am. J. Med. 2005, 118, 991–997. [Google Scholar] [CrossRef]
- Kahleova, H.; Matoulek, M.; Malinska, H.; Oliyarnik, O.; Kazdova, L.; Neskudla, T.; Skoch, A.; Hajek, M.; Hill, M.; Kahle, M.; et al. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with Type 2 diabetes. Diabet. Med. 2011, 28, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haghighatdoost, F.; Bellissimo, N.; de Zepetnek, J.O.T.; Rouhani, M.H. Association of vegetarian diet with inflammatory biomarkers: A systematic review and meta-analysis of observational studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Michas, G.; Mozaffarian, D. Unprocessed red and processed meats and risk of coronary artery disease and type 2 diabetes—An updated review of the evidence. Curr. Atheroscler. Rep. 2012, 14, 515–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zuurmond, M.G.; van der Schaft, N.; Nano, J.; Wijnhoven, H.A.H.; Ikram, M.A.; Franco, O.H.; Voortman, T. Plant versus animal based diets and insulin resistance, prediabetes and type 2 diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2018, 33, 883–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, T.H.; Pan, W.H.; Lin, M.N.; Lin, C.L. Vegetarian diet, change in dietary patterns, and diabetes risk: A prospective study. Nutr. Diabetes 2018, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahleova, H.; Tura, A.; Hill, M.; Holubkov, R.; Barnard, N.D. A plant-based dietary intervention improves beta-cell function and insulin resistance in overweight adults: A 16-week randomized clinical trial. Nutrients 2018, 10, 189. [Google Scholar] [CrossRef] [Green Version]
- Sparks, L.M.; Xie, H.; Koza, R.A.; Mynatt, R.; Hulver, M.W.; Bray, G.A.; Smith, S.R. A high-fat diet coordinately downregulates genes required for mitochondrial oxidative phosphorylation in skeletal muscle. Diabetes 2005, 54, 1926–1933. [Google Scholar] [CrossRef] [Green Version]
- Meex, R.C.; Blaak, E.E.; van Loon, L.J. Lipotoxicity plays a key role in the development of both insulin resistance and muscle atrophy in patients with type 2 diabetes. Obes. Rev. 2019, 20, 1205–1217. [Google Scholar] [CrossRef] [Green Version]
- Goff, L.M.; Bell, J.D.; So, P.W.; Dornhorst, A.; Frost, G.S. Veganism and its relationship with insulin resistance and intramyocellular lipid. Eur. J. Clin. Nutr. 2005, 59, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Wadden, T.A.; Stunkard, A.J. Controlled trial of very low calorie diet, behavior therapy, and their combination in the treatment of obesity. J. Consult. Clin. Psychol. 1986, 54, 482–488. [Google Scholar] [CrossRef]
- Sellahewa, L.; Khan, C.; Lakkunarajah, S.; Idris, I. A systematic review of evidence on the use of very low calorie diets in people with diabetes. Curr. Diabetes Rev. 2017, 13, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Lim (2011) [16] | Snel (2012) [43] | Jazet (2008) [44] | Skrha (2005) [45] | Steven & Taylor (2015) [20] | Teeuwisse (2012) [39] | |
|---|---|---|---|---|---|---|---|
| 1 | Was the study question or objective clearly stated? | √ | √ | √ | √ | √ | √ |
| 2 | Were the eligibility/selection criteria for the study population prespecified and clearly described? | √ | √ | √ | √ | √ | √ |
| 3 | Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? | √ | √ | √ | √ | √ | √ |
| 4 | Were all eligible participants that met the prespecified entry criteria enrolled? | NR | NR | NR | NR | NR | NR |
| 5 | Was the sample size sufficiently large to provide confidence in the findings? | √ | √ | √ | ✕ | ✕ | √ |
| 6 | Was the test/service/intervention clearly described and delivered consistently across the study population? | √ | √ | √ | √ | √ | √ |
| 7 | Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants? | √ | √ | √ | √ | √ | √ |
| 8 | Were the people assessing the outcomes blinded to the participants’ exposures/interventions? | √ | NR | NR | NR | NR | NR |
| 9 | Was the loss to follow-up after baseline ≤ 20%? Were those lost to follow-up accounted for in the analysis? | √ | O | √ | √ | √ | √ |
| 10 | Did the statistical methods examine changes in outcome measures form before to after the intervention? Were statistical tests done that provided p values for the pre-to-post changes? | √ | √ | √ | √ | √ | √ |
| 11 | Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| 12 | If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.) did the statistical analysis take into account the use of individual-level data to determine the effects at the group level? | NA | NA | NA | NA | NA | NA |
| Summary Quality 1 | ii | i | i | i | i | i | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashyap, A.; Mackay, A.; Carter, B.; Fyfe, C.L.; Johnstone, A.M.; Myint, P.K. Investigating the Effectiveness of Very Low-Calorie Diets and Low-Fat Vegan Diets on Weight and Glycemic Markers in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4870. https://doi.org/10.3390/nu14224870
Kashyap A, Mackay A, Carter B, Fyfe CL, Johnstone AM, Myint PK. Investigating the Effectiveness of Very Low-Calorie Diets and Low-Fat Vegan Diets on Weight and Glycemic Markers in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(22):4870. https://doi.org/10.3390/nu14224870
Chicago/Turabian StyleKashyap, Anjali, Alexander Mackay, Ben Carter, Claire L. Fyfe, Alexandra M. Johnstone, and Phyo K. Myint. 2022. "Investigating the Effectiveness of Very Low-Calorie Diets and Low-Fat Vegan Diets on Weight and Glycemic Markers in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis" Nutrients 14, no. 22: 4870. https://doi.org/10.3390/nu14224870
APA StyleKashyap, A., Mackay, A., Carter, B., Fyfe, C. L., Johnstone, A. M., & Myint, P. K. (2022). Investigating the Effectiveness of Very Low-Calorie Diets and Low-Fat Vegan Diets on Weight and Glycemic Markers in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients, 14(22), 4870. https://doi.org/10.3390/nu14224870