
Associations between Hunger and Psychological Outcomes: A Large-Scale Ecological Momentary Assessment Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ecological Momentary Assessment
2.3. Other Covariates
2.4. Statistical Analysis
2.5. Ethical Statement
3. Results
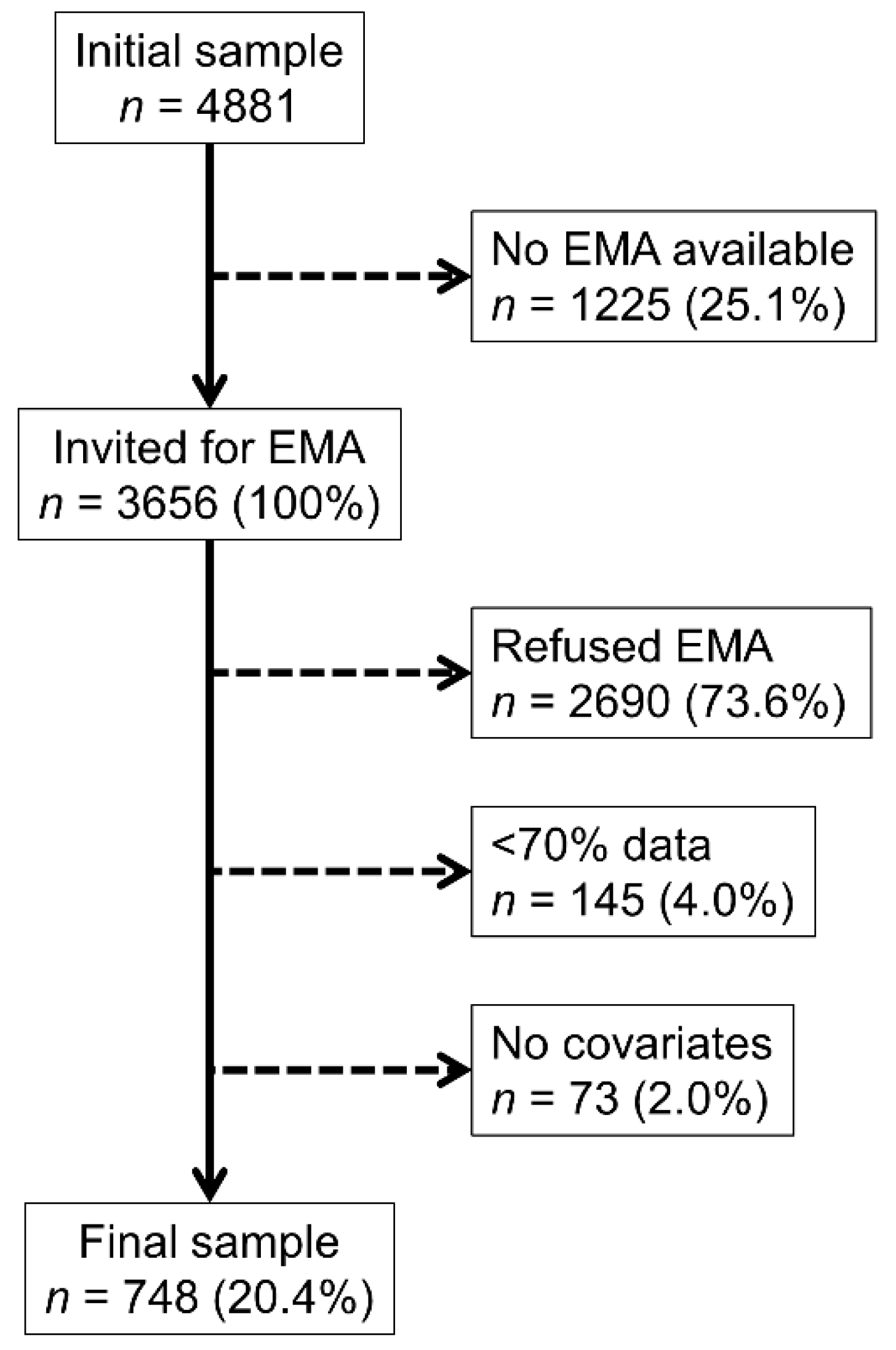
3.1. Selection Procedures and Characteristics of Participants
3.2. Levels of Hunger and Psychological States According to Assessment Period
3.3. Hunger Influencing Later Psychological States
3.4. Psychological States Influencing Later Hunger
4. Discussion
4.1. Levels of Hunger and Psychological States According to Assessment Period
4.2. Hunger Influencing Later Psychological States
4.3. Psychological States Influencing Later Hunger
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| CoLaus | NIH Family Study |
| 8. Environnement pendant la mesure | 2. Context of assessment (environment, social contact) |
| Les questions suivantes portent sur vos activités et ce que vous ressentez maintenant. | The following questions are about what you are doing and how you feel right now. |
| 8.3. Que faites-vous présentement? choix multiple | What are you doing at this moment? |
| Rien ou attendre | Nothing or waiting |
| Faire la sieste/se reposer | Napping/Resting |
| Manger | Eating |
| Tâches ménagères | Household chores |
| Travail salarié ou bénévole | Working (paid or volunteer) |
| Des courses | Shopping |
| Soins d’hygiène personnels | Personal hygiene care |
| Loisirs physiques ou sport | Physical leisure or sports |
| Entrainement personnel | Personal exercise |
| Promener le chien | Walking the dog |
| Voyager ou se déplacer | Traveling or commuting |
| Regarder la télé | Watching TV |
| Ecouter de la musique | Listening to music |
| Utiliser un ordinateur ou appareil électronique | Using a computer/electronic device |
| Parler au téléphone | Talking on the phone |
| Parler face à face | Talking in-person |
| Autre loisir non-physique | Other nonphysical leisure |
| Autre activité | Other activity |
| 9. Etat physique et émotionnel (humeur) | 3. Emotional and physical states (mood circumplex) |
| 9.1. A quel degré vous sentez-vous heureux maintenant? choix simple | How happy versus sad do you feel right now? |
| 1 Très gai/heureux | 1 Very cheerful/happy |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très triste/déprimé/malheureux | 7 Very sad/depressed/unhappy |
| 9.2. A quel degré vous sentez-vous anxieux maintenant? choix simple | How relaxed vs. anxious do you feel right now? |
| 1 Très détendu/calme | 1 Very Relaxed/Calm |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très anxieux/nerveux | 7 Very Anxious/Nervous |
| 9.3. À quel degré êtes-vous actif maintenant? choix simple | How inactive vs active do you feel right now? |
| 1 Très inactif | 1 Very Inactive/Quiet |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très actif | 7 Very Active/Aroused |
| 9.4. A quel degré vous sentez-vous énergique maintenant? choix simple | How tired vs energetic do you feel right now? |
| 1 Très fatigué/léthargique | 1 Very Tired/Sluggish |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très animé/excité | 7 Very Lively/Excited |
| 9.5. A quel degré vous sentez-vous concentré en ce moment? choix simple | How well can you concentrate or focus right now? |
| 1 Très concentré/attentif | 1 Very focused, attentive |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très déconcentré/distrait | 7 Very unfocused, distracted |
| 9.6. A quel degré vous sentez-vous irritable ou en colère présentement? choix simple | How irritable or easily angered do you feel right now? |
| 1 Pas du tout irritable/en colère | 1 Not at all Irritable/Angry |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très irritable/en colère | 7 Very Irritable/Angry |
| 9.7. Quelle est votre vivacité d’esprit en ce moment? choix simple | How quick is your thinking? |
| 1 Très vivace/beaucoup d’idées | 1 Very quick, lots of ideas |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très lent/difficulté à réfléchir | 7 Slow, cannot think of things |
| 9.8. A quel degré ressentez-vous du plaisir ou de la joie dans vos activités? choix simple | How much are you able to enjoy and feel pleasure in things? |
| 1 Beaucoup de plaisir | 1 Really enjoying things |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Aucune joie ou plaisir | 7 No pleasure or enjoyment |
| 9.9. A quel degré vous sentez vous agité ou impatient par rapport à d’habitude? choix simple | How fidgety or restless do you feel right now compared to your usual self? |
| 1 Pas du tout agité | 1 Not at all restless |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Très agité/impatient | 7 Very restless, fidgety, cannot sit still |
| 9.10. A quel degré avez-vous faim maintenant? choix simple | How hungry do you feel right now? |
| 1 Pas faim du tout | 1 Not at all hungry, full |
| 2 | 2 |
| 3 | 3 |
| 4 | 4 |
| 5 | 5 |
| 6 | 6 |
| 7 Extrêmement faim | 7 Extremely hungry |
| 11. Nutrition, boissons, substances | 5. Food, drink, substances |
| 11.2. Quel a été votre repas le plus consistant depuis le dernier signal? choix simple | How much did you eat? |
| Rien | |
| Juste un snack | Just a snack |
| Un petit repas | A small meal |
| Un repas normal, complet | A regular, full meal |
| Un repas copieux | A large meal |
References
- Cardi, V.; Leppanen, J.; Treasure, J. The effects of negative and positive mood induction on eating behaviour: A meta-analysis of laboratory studies in the healthy population and eating and weight disorders. Neurosci. Biobehav. Rev. 2015, 57, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Rohles, F.H., Jr.; Wilson, L.M. Hunger as a catalyst in aggression. Behaviour 1974, 48, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Symmonds, M.; Emmanuel, J.J.; Drew, M.E.; Batterham, R.L.; Dolan, R.J. Metabolic state alters economic decision making under risk in humans. PLoS ONE 2010, 5, e11090. [Google Scholar] [CrossRef] [Green Version]
- Herbert, B.M.; Herbert, C.; Pollatos, O.; Weimer, K.; Enck, P.; Sauer, H.; Zipfel, S. Effects of short-term food deprivation on interoceptive awareness, feelings and autonomic cardiac activity. Biol. Psychol. 2012, 89, 71–79. [Google Scholar] [CrossRef]
- Vicario, C.M.; Kuran, K.A.; Rogers, R.; Rafal, R.D. The effect of hunger and satiety in the judgment of ethical violations. Brain Cogn. 2018, 125, 32–36. [Google Scholar] [CrossRef]
- Taylor, L.A.; Rachman, S.J. The effects of blood sugar level changes on cognitive function, affective state, and somatic symptoms. J. Behav. Med. 1988, 11, 279–291. [Google Scholar] [CrossRef]
- Hermanns, N.; Kubiak, T.; Kulzer, B.; Haak, T. Emotional changes during experimentally induced hypoglycaemia in type 1 diabetes. Biol. Psychol. 2003, 63, 15–44. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, N.; Scheff, C.; Kulzer, B.; Weyers, P.; Pauli, P.; Kubiak, T.; Haak, T. Association of glucose levels and glucose variability with mood in type 1 diabetic patients. Diabetologia 2007, 50, 930–933. [Google Scholar] [CrossRef] [Green Version]
- Bushman, B.J.; Dewall, C.N.; Pond, R.S., Jr.; Hanus, M.D. Low glucose relates to greater aggression in married couples. Proc. Natl. Acad. Sci. USA 2014, 111, 6254–6257. [Google Scholar] [CrossRef] [Green Version]
- MacCormack, J.K.; Lindquist, K.A. Feeling hangry? When hunger is conceptualized as emotion. Emotion 2019, 19, 301–319. [Google Scholar] [CrossRef]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Anderberg, R.H.; Hansson, C.; Fenander, M.; Richard, J.E.; Dickson, S.L.; Nissbrandt, H.; Bergquist, F.; Skibicka, K.P. The stomach-derived hormone ghrelin increases impulsive behavior. Neuropsychopharmacology 2016, 41, 1199–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalsen, A.; Frey, U.H.; Merse, S.; Siffert, W.; Dobos, G.J. Hunger and mood during extended fasting are dependent on the GNB3 C825T polymorphism. Ann. Nutr. Metab 2009, 54, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.M.; Engel, S.G.; Wonderlich, S.A. Ecological momentary assessment in eating disorders research: Recent findings and promising new directions. Curr. Opin. Psychiatry 2020, 33, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Haedt-Matt, A.A.; Keel, P.K. Revisiting the affect regulation model of binge eating: A meta-analysis of studies using ecological momentary assessment. Psychol. Bull. 2011, 137, 660. [Google Scholar] [CrossRef] [Green Version]
- Reichenberger, J.; Richard, A.; Smyth, J.M.; Fischer, D.; Pollatos, O.; Blechert, J. It’s craving time: Time of day effects on momentary hunger and food craving in daily life. Nutrition 2018, 55–56, 15–20. [Google Scholar] [CrossRef]
- Huh, J.; Shiyko, M.; Keller, S.; Dunton, G.; Schembre, S.M. The time-varying association between perceived stress and hunger within and between days. Appetite 2015, 89, 145–151. [Google Scholar] [CrossRef] [Green Version]
- Firmann, M.; Mayor, V.; Vidal, P.M.; Bochud, M.; Pecoud, A.; Hayoz, D.; Paccaud, F.; Preisig, M.; Song, K.S.; Yuan, X.; et al. The CoLaus study: A population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndrome. BMC Cardiovasc. Disord 2008, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Preisig, M.; Waeber, G.; Vollenweider, P.; Bovet, P.; Rothen, S.; Vandeleur, C.; Guex, P.; Middleton, L.; Waterworth, D.; Mooser, V.; et al. The PsyCoLaus study: Methodology and characteristics of the sample of a population-based survey on psychiatric disorders and their association with genetic and cardiovascular risk factors. BMC Psychiatry 2009, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Merikangas, K.R.; Cui, L.; Heaton, L.; Nakamura, E.; Roca, C.; Ding, J.; Qin, H.; Guo, W.; Shugart, Y.Y.; Zarate, C.; et al. Independence of familial transmission of mania and depression: Results of the NIMH family study of affective spectrum disorders. Mol. Psychiatry 2014, 19, 214–219. [Google Scholar] [CrossRef]
- Larsen, R.J.; Diener, E. Promises and problems with the circumplex model of emotion. In Emotion; Clark, M.S., Ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1992; pp. 25–59. [Google Scholar]
- Zautra, A.J.; Guarnaccia, C.A.; Dohrenwend, B.P. Measuring small life events. Am. J. Commu. Psychol. 1986, 14, 629–655. [Google Scholar] [CrossRef]
- Lamers, F.; Swendsen, J.; Cui, L.; Husky, M.; Johns, J.; Zipunnikov, V.; Merikangas, K.R. Mood reactivity and affective dynamics in mood and anxiety disorders. J. Abnorm Psychol. 2018, 127, 659–669. [Google Scholar] [CrossRef]
- DeWall, C.N.; Pond, R.S.; Bushman, B.J. Sweet revenge: Diabetic symptoms predict less forgiveness. Pers. Individ. Differ. 2010, 49, 823–826. [Google Scholar] [CrossRef]
- Fuhrer, R.; Rouillon, F. La version française de l’échelle CES-D (Center for Epidemiologic Studies-Depression scale). Description et traduction de l’échelle d’autoévaluation. Psychiatr. Psychobiol. 1989, 4, 163–166. [Google Scholar] [CrossRef]
- Peeters, F.; Berkhof, J.; Delespaul, P.; Rottenberg, J.; Nicolson, N.A. Diurnal mood variation in major depressive disorder. Emotion 2006, 6, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowe, E.; Daly, M.; Delaney, L.; Carroll, S.; Malone, K.M. The intra-day dynamics of affect, self-esteem, tiredness, and suicidality in Major Depression. Psychiatry Res. 2019, 279, 98–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strahler, J.; Nater, U.M. Differential effects of eating and drinking on wellbeing-An ecological ambulatory assessment study. Biol. Psychol. 2018, 131, 72–88. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.S.; Boolani, A.; Conroy, D.A.; Dunietz, T.; Jansen, E.C. Skipping breakfast and mood: The role of sleep. Nutr. Health 2021, 27, 373–379. [Google Scholar] [CrossRef]
- Sanna, F.; Loy, F.; Piras, R.; Moat, A.; Masala, C. Age-related cognitive decline and the olfactory identification deficit are associated to increased level of depression. Front. Neurosci. 2021, 15, 599593. [Google Scholar] [CrossRef]
- Chen, B.; Masala, C.; Oleszkiewicz, A.; Englmaier, V.; Gunder, N.; Menzel, S.; Haehner, A.; Hummel, T. Nonlinear association between chemosensory dysfunction and body mass index. J. Sens. Stud. 2022, 37, e12715. [Google Scholar] [CrossRef]
- Liguori, C.A.; Nikolaus, C.J.; Nickols-Richardson, S.M. Cognitive distraction at mealtime decreases amount consumed in healthy young adults: A randomized crossover exploratory study. J. Nutr. 2020, 150, 1324–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgs, S. Manipulations of attention during eating and their effects on later snack intake. Appetite 2015, 92, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Smyth, J.M.; Pickering, T.; Schwartz, J. Daily mood variability: Forms of diurnal patterns and determinants of diurnal patterns. J. Appl. Soc. Psychol. 1996, 26, 1286–1305. [Google Scholar] [CrossRef]
- Giurgiu, M.; Koch, E.D.; Plotnikoff, R.C.; Ebner-Priemer, U.W.; Reichert, M. Breaking up sedentary behavior optimally to enhance mood. Med. Sci. Sport. Exerc. 2020, 52, 457–465. [Google Scholar] [CrossRef]


{kind=link}
| Included | Declined/Insufficient Data | p-Value | |
|---|---|---|---|
| n | 748 | 2908 | |
| Female (%) | 422 (56.4) | 1595 (54.8) | 0.442 |
| Age (years) | 60.0 ± 9.3 | 63.2 ± 10.4 | <0.001 |
| Age groups (%) | <0.001 | ||
| 45–54.9 | 261 (34.9) | 785 (27.0) | |
| 55–64.9 | 258 (34.5) | 894 (30.7) | |
| 65+ | 229 (30.6) | 1229 (42.3) | |
| Married (%) | 434 (58.0) | 1475 (51.1) | 0.001 |
| Smoking status (%) | 0.052 | ||
| Never | 318 (42.5) | 1065 (40.9) | |
| Former | 306 (40.9) | 1004 (38.5) | |
| Current | 124 (16.6) | 536 (20.6) | |
| Body mass index (kg/m2) | 26.7 ± 4.9 | 26.4 ± 4.8 | 0.071 |
| BMI categories (%) | 0.140 | ||
| Normal | 305 (40.8) | 1083 (41.9) | |
| Overweight | 281 (37.5) | 1025 (39.6) | |
| Obese | 162 (21.7) | 477 (18.5) | |
| Diabetes (%) | 49 (6.6) | 309 (11.7) | <0.001 |
| Number of drinks per week | 4 [1–8] | 3 [0–8] | <0.001 § |
| Alcohol consumption (%) | 591 (79.0) | 1670 (69.9) | <0.001 |
| CESD score | 8 [3–13] | 8 [4–14] | <0.216 § |
| Depressed (%) | 85 (12.8) | 220 (11.6) | 0.395 |
| Variables | Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | Model 4 | p-Value |
|---|---|---|---|---|---|---|---|---|
| Hunger intensity | ||||||||
| Sadness | 0.018 (0.008; 0.027) | <0.001 | 0.003 (−0.008; 0.014) | 0.607 | 0.004 (−0.007; 0.015) | 0.447 | 0.009 (−0.002; 0.020) | 0.103 |
| Anxiety | 0.027 (0.016; 0.038) | <0.001 | 0.007 (−0.005; 0.019) | 0.259 | 0.011 (−0.001; 0.023) | 0.071 | 0.017 (0.005; 0.030) | 0.006 |
| Feeling active | 0.082 (0.061; 0.103) | <0.001 | 0.029 (0.007; 0.051) | 0.009 | 0.029 (0.007; 0.051) | 0.010 | 0.041 (0.018; 0.063) | <0.001 |
| Feeling lively | 0.042 (0.028; 0.056) | <0.001 | 0.021 (0.007; 0.036) | 0.005 | 0.019 (0.004; 0.034) | 0.011 | 0.021 (0.006; 0.036) | 0.006 |
| Feeling distracted | −0.030 (−0.045; −0.015) | <0.001 | 0.000 (−0.016; 0.016) | 0.985 | −0.001 (−0.017; 0.015) | 0.949 | −0.005 (−0.022; 0.011) | 0.528 |
| Anhedonia | 0.007 (−0.005; 0.020) | 0.232 | −0.008 (−0.021; 0.006) | 0.254 | −0.005 (−0.018; 0.009) | 0.488 | −0.001 (−0.015; 0.013) | 0.908 |
| Anger | 0.009 (−0.001; 0.020) | 0.082 | −0.001 (−0.012; 0.011) | 0.891 | 0.001 (−0.010; 0.013) | 0.829 | 0.004 (−0.008; 0.016) | 0.509 |
| Slow thinking | −0.036 (−0.049; −0.024) | <0.001 | −0.016 (−0.029; −0.003) | 0.016 | −0.016 (−0.029; −0.003) | 0.018 | −0.019 (−0.033; −0.006) | 0.004 |
| Restlessness | 0.007 (−0.006; 0.019) | 0.287 | −0.010 (−0.024; 0.003) | 0.143 | −0.009 (−0.023; 0.005) | 0.195 | −0.003 (−0.016; 0.011) | 0.726 |
| Previous eating | ||||||||
| Sadness | −0.015 (−0.060; 0.029) | 0.495 | −0.035 (−0.080; 0.009) | 0.122 | 0.002 (−0.043; 0.046) | 0.934 | −0.015 (−0.060; 0.030) | 0.511 |
| Anxiety | −0.028 (−0.078; 0.022) | 0.268 | −0.059 (−0.110; −0.009) | 0.021 | −0.035 (−0.085; 0.015) | 0.173 | −0.056 (−0.107; −0.006) | 0.030 |
| Feeling active | 0.151 (0.058; 0.243) | 0.001 | 0.068 (−0.023; 0.159) | 0.144 | 0.116 (0.025; 0.208) | 0.012 | 0.079 (−0.014; 0.171) | 0.095 |
| Feeling lively | 0.070 (0.008; 0.132) | 0.026 | 0.026 (−0.034; 0.087) | 0.395 | 0.020 (−0.040; 0.081) | 0.509 | 0.017 (−0.045; 0.078) | 0.597 |
| Feeling distracted | −0.086 (−0.152; −0.019) | 0.012 | −0.031 (−0.097; 0.035) | 0.354 | −0.052 (−0.118; 0.014) | 0.124 | −0.038 (−0.105; 0.029) | 0.264 |
| Anhedonia | −0.065 (−0.120; −0.009) | 0.022 | −0.085 (−0.141; −0.030) | 0.003 | −0.047 (−0.103; 0.009) | 0.098 | −0.059 (−0.115; −0.002) | 0.041 |
| Anger | −0.012 (−0.059; 0.035) | 0.620 | −0.027 (−0.075; 0.021) | 0.264 | −0.016 (−0.064; 0.032) | 0.512 | −0.024 (−0.073; 0.024) | 0.331 |
| Slow thinking | −0.080 (−0.134; −0.026) | 0.004 | −0.038 (−0.091; 0.016) | 0.167 | −0.031 (−0.084; 0.022) | 0.256 | −0.019 (−0.073; 0.035) | 0.493 |
| Restlessness | 0.012 (−0.045; 0.068) | 0.684 | −0.018 (−0.075; 0.039) | 0.534 | −0.005 (−0.062; 0.052) | 0.868 | −0.021 (−0.078; 0.036) | 0.470 |
| Variables | Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | Model 4 | p-Value |
|---|---|---|---|---|---|---|---|---|
| Sadness | 0.035 (0.006; 0.063) | 0.016 | 0.008 (−0.020; 0.036) | 0.583 | 0.009 (−0.019; 0.037) | 0.546 | 0.002 (−0.025; 0.030) | 0.871 |
| Anxiety | 0.023 (−0.002; 0.049) | 0.070 | 0.022 (−0.003; 0.047) | 0.085 | 0.023 (−0.002; 0.048) | 0.066 | 0.021 (−0.003; 0.045) | 0.089 |
| Feeling active | 0.028 (0.013; 0.042) | <0.001 | 0.050 (0.036; 0.064) | <0.001 | 0.050 (0.036; 0.064) | <0.001 | 0.048 (0.034; 0.062) | <0.001 |
| Feeling lively | 0.023 (0.001; 0.046) | 0.044 | 0.046 (0.024; 0.068) | <0.001 | 0.045 (0.023; 0.067) | <0.001 | 0.023 (0.001; 0.046) | 0.044 |
| Feeling distracted | −0.019 (−0.039; 0.001) | 0.058 | −0.039 (−0.059; −0.019) | <0.001 | −0.039 (−0.058; −0.019) | <0.001 | −0.039 (−0.058; −0.019) | <0.001 |
| Anhedonia | 0.028 (0.005; 0.052) | 0.019 | 0.002 (−0.021; 0.025) | 0.849 | 0.003 (−0.020; 0.027) | 0.768 | −0.004 (−0.027; 0.018) | 0.696 |
| Anger | 0.009 (−0.001; 0.020) | 0.082 | 0.008 (−0.018; 0.035) | 0.535 | 0.009 (−0.017; 0.036) | 0.490 | 0.007 (−0.019; 0.032) | 0.609 |
| Slow thinking | −0.023 (−0.046; 0.001) | 0.063 | −0.057 (−0.080; −0.034) | <0.001 | −0.057 (−0.080; −0.034) | <0.001 | −0.059 (−0.082; −0.036) | <0.001 |
| Restlessness | 0.031 (0.008; 0.054) | 0.008 | 0.040 (0.018; 0.062) | <0.001 | 0.040 (0.018; 0.063) | <0.001 | 0.038 (0.016; 0.059) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Rivaz, R.; Swendsen, J.; Berthoz, S.; Husky, M.; Merikangas, K.; Marques-Vidal, P. Associations between Hunger and Psychological Outcomes: A Large-Scale Ecological Momentary Assessment Study. Nutrients 2022, 14, 5167. https://doi.org/10.3390/nu14235167
de Rivaz R, Swendsen J, Berthoz S, Husky M, Merikangas K, Marques-Vidal P. Associations between Hunger and Psychological Outcomes: A Large-Scale Ecological Momentary Assessment Study. Nutrients. 2022; 14(23):5167. https://doi.org/10.3390/nu14235167
Chicago/Turabian Stylede Rivaz, Romain, Joel Swendsen, Sylvie Berthoz, Mathilde Husky, Kathleen Merikangas, and Pedro Marques-Vidal. 2022. "Associations between Hunger and Psychological Outcomes: A Large-Scale Ecological Momentary Assessment Study" Nutrients 14, no. 23: 5167. https://doi.org/10.3390/nu14235167
APA Stylede Rivaz, R., Swendsen, J., Berthoz, S., Husky, M., Merikangas, K., & Marques-Vidal, P. (2022). Associations between Hunger and Psychological Outcomes: A Large-Scale Ecological Momentary Assessment Study. Nutrients, 14(23), 5167. https://doi.org/10.3390/nu14235167