
An Infant Formula with Large, Milk Phospholipid-Coated Lipid Droplets Supports Adequate Growth and Is Well-Tolerated in Healthy, Term Asian Infants: A Randomized, Controlled Double-Blind Clinical Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participating Centers
2.2. Study Design
2.3. Subjects
2.4. Study Products
2.5. Measurements
2.6. Statistics
3. Results
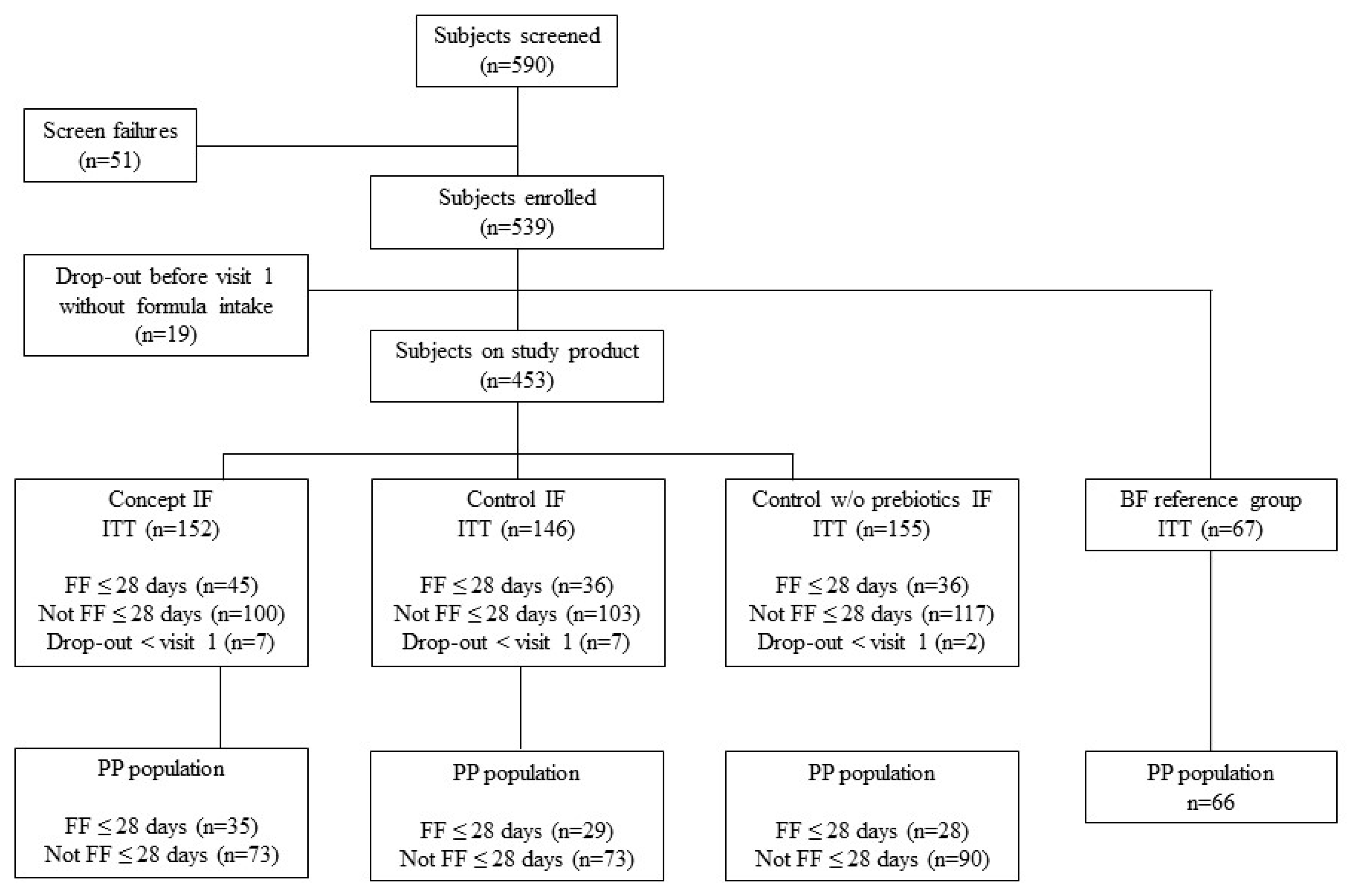
3.1. Study and Subject Characteristics
3.2. Study Product Intake
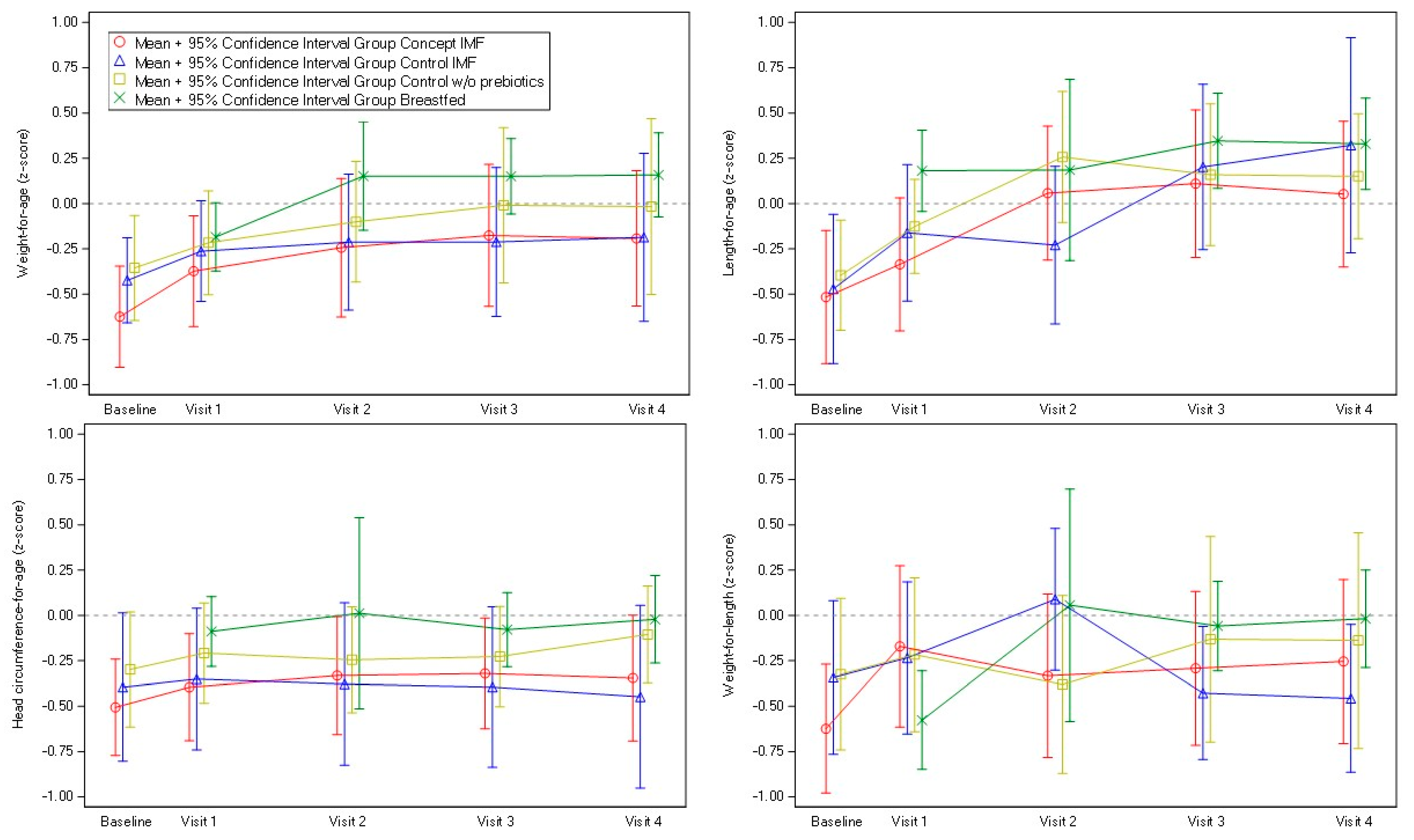
3.3. Growth Outcomes
3.4. Gastrointestinal Tolerance
3.5. Adverse Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eidelman, A.I. Breastfeeding and the use of human milk: An analysis of the American Academy of Pediatrics 2012 Breastfeeding Policy Statement. Breastfeed. Med. 2012, 7, 323–324. [Google Scholar] [CrossRef]
- WHO/UNICEF. Global Nutrition Targets 2025: Breastfeeding Policy Brief. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-14.7 (accessed on 20 January 2022).
- EFSA Panel on Dietetic Products, Scientific Opinion on the essential composition of infant and follow-on formulae. EFSA J. 2014, 12, 3760. [CrossRef] [Green Version]
- Jensen, R.G. Lipids in human milk. Lipids 1999, 34, 1243–1271. [Google Scholar] [CrossRef]
- Thakkar, S.K.; Giuffrida, F.; Cristina, C.H.; De Castro, C.A.; Mukherjee, R.; Tran, L.A.; Steenhout, P.; Lee le, Y.; Destaillats, F. Dynamics of human milk nutrient composition of women from Singapore with a special focus on lipids. Am. J. Hum. Biol. 2013, 25, 770–779. [Google Scholar] [CrossRef]
- Floris, L.M.; Stahl, B.; Abrahamse-Berkeveld, M.; Teller, I.C. Human milk fatty acid profile across lactational stages after term and preterm delivery: A pooled data analysis. Prostaglandins Leukot. Essent. Fatty Acids 2020, 156, 102023. [Google Scholar] [CrossRef] [Green Version]
- Gallier, S.; Gragson, D.; Jimenez-Flores, R.; Everett, D. Using confocal laser scanning microscopy to probe the milk fat globule membrane and associated proteins. J. Agric. Food Chem. 2010, 58, 4250–4257. [Google Scholar] [CrossRef] [Green Version]
- Lopez, C.; Menard, O. Human milk fat globules: Polar lipid composition and in situ structural investigations revealing the heterogeneous distribution of proteins and the lateral segregation of sphingomyelin in the biological membrane. Colloids Surf. B Biointerfaces 2011, 83, 29–41. [Google Scholar] [CrossRef]
- Michalski, M.C.; Briard, V.; Michel, F.; Tasson, F.; Poulain, P. Size distribution of fat globules in human colostrum, breast milk, and infant formula. J. Dairy Sci. 2005, 88, 1927–1940. [Google Scholar] [CrossRef] [Green Version]
- Innis, S.M. Dietary lipids in early development: Relevance to obesity, immune and inflammatory disorders. Curr. Opin. Endocrinol. Diabetes Obes. 2007, 14, 359–364. [Google Scholar] [CrossRef]
- Klemens, C.M.; Berman, D.R.; Mozurkewich, E.L. The effect of perinatal omega-3 fatty acid supplementation on inflammatory markers and allergic diseases: A systematic review. BJOG 2011, 118, 916–925. [Google Scholar] [CrossRef] [Green Version]
- Zou, L.; Pande, G.; Akoh, C.C. Infant Formula Fat Analogs and Human Milk Fat: New Focus on Infant Developmental Needs. Annu. Rev. Food Sci. Technol. 2016, 7, 139–165. [Google Scholar] [CrossRef]
- Gallier, S.; Vocking, K.; Post, J.A.; Van De Heijning, B.; Acton, D.; Van Der Beek, E.M.; Van Baalen, T. A novel infant milk formula concept: Mimicking the human milk fat globule structure. Colloids Surf. B Biointerfaces 2015, 136, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Armand, M.; Pasquier, B.; Andre, M.; Borel, P.; Senft, M.; Peyrot, J.; Salducci, J.; Portugal, H.; Jaussan, V.; Lairon, D. Digestion and absorption of 2 fat emulsions with different droplet sizes in the human digestive tract. Am. J. Clin. Nutr. 1999, 70, 1096–1106. [Google Scholar] [CrossRef]
- Borel, P.; Armand, M.; Pasquier, B.; Senft, M.; Dutot, G.; Melin, C.; Lafont, H.; Lairon, D. Digestion and absorption of tube-feeding emulsions with different droplet sizes and compositions in the rat. JPEN J. Parenter. Ente. Nutr. 1994, 18, 534–543. [Google Scholar] [CrossRef]
- Michalski, M.C.; Soares, A.F.; Lopez, C.; Leconte, N.; Briard, V.; Geloen, A. The supramolecular structure of milk fat influences plasma triacylglycerols and fatty acid profile in the rat. Eur. J. Nutr. 2006, 45, 215–224. [Google Scholar] [CrossRef]
- van den Braak, C.; Thomassen, G.; Acton, D.; Ludwig, T.; Abrahamse, E. A concept infant formula with large, phospholipid coated droplets demonstrates slow in vitro gastric lipolysis as compared to regular infant formula. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 740. [Google Scholar]
- Baumgartner, S.; van de Heijning, B.J.M.; Acton, D.; Mensink, R.P. Infant milk fat droplet size and coating affect postprandial responses in healthy adult men: A proof-of-concept study. Eur. J. Clin. Nutr. 2017, 71, 1108–1113. [Google Scholar] [CrossRef]
- Oosting, A.; van Vlies, N.; Kegler, D.; Schipper, L.; Abrahamse-Berkeveld, M.; Ringler, S.; Verkade, H.J.; van der Beek, E.M. Effect of dietary lipid structure in early postnatal life on mouse adipose tissue development and function in adulthood. Br. J. Nutr. 2014, 111, 215–226. [Google Scholar] [CrossRef] [Green Version]
- Baars, A.; Oosting, A.; Engels, E.; Kegler, D.; Kodde, A.; Schipper, L.; Verkade, H.J.; van der Beek, E.M. Milk fat globule membrane coating of large lipid droplets in the diet of young mice prevents body fat accumulation in adulthood. Br. J. Nutr. 2016, 115, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Teller, I.C.; Hoyer-Kuhn, H.; Bronneke, H.; Nosthoff-Horstmann, P.; Oosting, A.; Lippach, G.; Wohlfarth, M.; Rauh, M.; van der Beek, E.M.; Dotsch, J.; et al. Complex lipid globules in early-life nutrition improve long-term metabolic phenotype in intra-uterine growth-restricted rats. Br. J. Nutr. 2018, 120, 763–776. [Google Scholar] [CrossRef] [Green Version]
- Schipper, L.; van Dijk, G.; Broersen, L.M.; Loos, M.; Bartke, N.; Scheurink, A.J.; van der Beek, E.M. A Postnatal Diet Containing Phospholipids, Processed to Yield Large, Phospholipid-Coated Lipid Droplets, Affects Specific Cognitive Behaviors in Healthy Male Mice. J. Nutr. 2016, 146, 1155–1161. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.E.; Cormack, B.E.; Alexander, T.; Alsweiler, J.M.; Bloomfield, F.H. Advances in nutrition of the newborn infant. Lancet 2017, 389, 1660–1668. [Google Scholar] [CrossRef]
- Bourlieu, C.; Deglaire, A.; De Oliveira, S.C.; Menard, O.; Le Gouar, Y.; Carriere, F. Towards infant formula biomimetic of human milk structure and digestive behaviour. OCL 2017, 24, D206. [Google Scholar] [CrossRef] [Green Version]
- Shek, L.P.; Chong, Y.S.; Winokan, A.; Abrahamse-Berkeveld, M.; Van Der Beek, E.M.; Teoh, O.H.; On Behalf of The Venus Working Group. Evaluation of an Infant Formula with Large, Milk-Phospholipid Coated Lipid Droplets on Long-Term Growth and Development of Singaporean Infants: Randomized Controlled Trial Protocol. Nutrients 2021, 13, 2865. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Clinical Testing of Infant Formulas with Respect to Nutritional Suitability for Term Infants; American Academy for Administration: Elk Grove Village, IL, USA, 1988. [Google Scholar]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Bekkali, N.; Hamers, S.L.; Reitsma, J.B.; Van Toledo, L.; Benninga, M.A. Infant stool form scale: Development and results. J. Pediatr. 2009, 154, 521–526.e521. [Google Scholar] [CrossRef]
- Report of the Scientific Committee on Food on the Revision of Essential Requirements of Infant Formulae and Follow-on Formulae; European Commission: Brussels, Belgium, 2003.
- World Health Organization. WHO Multicentre Growth Reference Study Group: WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Drossman, D.A.; Dumitrascu, D.L. Rome III: New standard for functional gastrointestinal disorders. J. Gastrointestin Liver Dis. 2006, 15, 237–241. [Google Scholar]
- Timby, N.; Domellof, E.; Hernell, O.; Lonnerdal, B.; Domellof, M. Neurodevelopment, nutrition, and growth until 12 mo of age in infants fed a low-energy, low-protein formula supplemented with bovine milk fat globule membranes: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 860–868. [Google Scholar] [CrossRef] [Green Version]
- Billeaud, C.; Puccio, G.; Saliba, E.; Guillois, B.; Vaysse, C.; Pecquet, S.; Steenhout, P. Safety and tolerance evaluation of milk fat globule membrane-enriched infant formulas: A randomized controlled multicenter non-inferiority trial in healthy term infants. Clin. Med. Insights. Pediatr. 2014, 8, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Breij, L.M.; Abrahamse-Berkeveld, M.; Vandenplas, Y.; Jespers, S.N.J.; de Mol, A.C.; Khoo, P.C.; Kalenga, M.; Peeters, S.; van Beek, R.H.T.; Norbruis, O.F.; et al. An infant formula with large, milk phospholipid-coated lipid droplets containing a mixture of dairy and vegetable lipids supports adequate growth and is well tolerated in healthy, term infants. Am. J. Clin. Nutr. 2019, 109, 586–596. [Google Scholar] [CrossRef]
- Alexander, D.D.; Yan, J.; Bylsma, L.C.; Northington, R.S.; Grathwohl, D.; Steenhout, P.; Erdmann, P.; Spivey-Krobath, E.; Haschke, F. Growth of infants consuming whey-predominant term infant formulas with a protein content of 1.8 g/100 kcal: A multicenter pooled analysis of individual participant data. Am. J. Clin. Nutr. 2016, 104, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Natale, V.; Rajagopalan, A. Worldwide variation in human growth and the World Health Organization growth standards: A systematic review. BMJ Open 2014, 4, e003735. [Google Scholar] [CrossRef] [Green Version]
- Fenn, B.; Penny, M.E. Using the new World Health Organisation growth standards: Differences from 3 countries. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 316–321. [Google Scholar] [CrossRef]
- Bong, Y.; Shariff, A.A.; Mohamed, A.M.; Merican, A.F. Malaysian growth centiles for children under six years old. Ann. Hum. Biol. 2015, 42, 108–115. [Google Scholar] [CrossRef]
- Huang, X.; Chang, J.; Feng, W.; Xu, Y.; Xu, T.; Tang, H.; Wang, H.; Pan, X. Development of a New Growth Standard for Breastfed Chinese Infants: What Is the Difference from the WHO Growth Standards? PLoS ONE 2016, 11, e0167816. [Google Scholar] [CrossRef]
- Scholtens, P.A.; Goossens, D.A.; Staiano, A. Stool characteristics of infants receiving short-chain galacto-oligosaccharides and long-chain fructo-oligosaccharides: A review. World J. Gastroenterol. 2014, 20, 13446–13452. [Google Scholar] [CrossRef] [Green Version]
- Knol, J.; Scholtens, P.; Kafka, C.; Steenbakkers, J.; Gro, S.; Helm, K.; Klarczyk, M.; Schopfer, H.; Bockler, H.M.; Wells, J. Colon microflora in infants fed formula with galacto- and fructo-oligosaccharides: More like breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 36–42. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Schmitt, J.; Tandoi, L.; Rizzardi, S.; Boehm, G. Early dietary intervention with a mixture of prebiotic oligosaccharides reduces the incidence of allergic manifestations and infections during the first two years of life. J. Nutr. 2008, 138, 1091–1095. [Google Scholar] [CrossRef]
- Moro, G.; Arslanoglu, S.; Stahl, B.; Jelinek, J.; Wahn, U.; Boehm, G. A mixture of prebiotic oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age. Arch. Dis. Child. 2006, 91, 814–819. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Per 100 mL | Control w/o Prebiotics IF 1 | Control IF | Concept IF |
|---|---|---|---|
| Energy (kcal) | 66 | 66 | 66 |
| Fat (g) | 3.4 | 3.4 | 3.4 |
| Vegetable oil (g) | 3.3 | 3.3 | 3.2 |
| Dairy lipids (g) | - | - | 0.2 |
| Non-dairy lipids (g) | 0.1 | 0.1 | |
| Saturates | 1.5 | 1.5 | 1.5 |
| Monounsaturates | 1.3 | 1.3 | 1.3 |
| Polyunsaturates | 0.6 | 0.6 | 0.6 |
| Linoleic acid (mg) | 448 | 447 | 436 |
| Alpha linolenic acid (mg) | 83 | 82 | 81 |
| Arachidomic acid (mg) | 11 | 11 | 11 |
| Eicosapentaenoic acid (mg) | 1.4 | 1.4 | 1.8 |
| Docosahexaenoic acid (mg) | 6.4 | 6.4 | 6.4 |
| Milk phospholipids (mg) | - | - | 54.4 |
| Soy phospholipids (mg) | 4.5 | 4.5 | - |
| Protein (g) | 1.3 | 1.3 | 1.3 |
| Whey protein (g) | 0.8 | 0.8 | 0.8 |
| Casein (g) | 0.5 | 0.5 | 0.5 |
| Carbohydrates (g) | 7.6 | 7.3 | 7.3 |
| scGOS/lcFOS (9:1) (g) 2 | - | 0.8 | 0.8 |
| Vitamins | |||
| Vitamin A (μg RE) | 50 | 50 | 50 |
| Vitamin E (mg α-TE) | 1.1 | 1.1 | 1.1 |
| Alpha-tocopherol (mg) | 1.3 | 1.3 | 1.3 |
| Statistic | Control w/o Prebiotics IF 1 (n = 28) | Control IF (n = 29) | Concept IF (n = 35) | Breastfed (n = 66) | |
|---|---|---|---|---|---|
| Infant characteristics | |||||
| Sex | |||||
| Male | n (%) | 16 (57%) | 16 (55%) | 22 (63%) | 30 (45%) |
| Female | n (%) | 12 (43%) | 13 (45%) | 13 (37%) | 36 (55%) |
| Ethnicity | |||||
| Chinese | n (%) | 12 (43%) | 11 (38%) | 23 (66%) | 55 (83%) |
| Indian | n (%) | 16 (57%) | 13 (45%) | 11 (31%) | 8 (12%) |
| Malay | n (%) | 0 (0%) | 0 (0%) | 0 (0%) | 3 (5%) |
| Other | n (%) | 0 (0%) | 5 (17%) | 1 (3%) | 0 (0%) |
| Birth characteristics | |||||
| Weight (g) | Mean (SD) | 3159 (345) | 3102 (319) | 3059 (350) | 3138 (310) |
| Length(cm) | Mean (SD) | 49.3 (1.8) | 48.5 (1.5) | 48.2 (1.6) | 49.6 (2.1) |
| Head circumference (cm) | Mean (SD) | 33.8 (0.9) | 33.5 (1.2) | 33.6 (1.4) | 33.6 (1.0) |
| Caesarean section | n (%) | 8 (29%) | 4 (14%) | 11 (31%) | 10 (15%) |
| Gestational age (wk) | Mean (SD) | 38.9 (1.1) | 39.0 (1.1) | 38.9 (0.9) | 39.0 (1.1) |
| Maternal characteristics | |||||
| Maternal age (y) | Mean (SD) | 29.1 (6.2) | 29.7 (6.4) | 29.6 (5.6) | 30.5 (3.8) |
| Maternal university education (yes) | n (%) | 2 (7%) | 4 (14%) | 4 (11%) | 48 (73%) |
| Weight status 2 | |||||
| Underweight | n (%) | 6 (21%) | 4 (14%) | 5 (14%) | 9 (14%) |
| Normal | n (%) | 6 (21%) | 14 (48%) | 14 (40%) | 38 (58%) |
| Overweight | n (%) | 5 (18%) | 7 (24%) | 8 (23%) | 17 (26%) |
| Obese | n (%) | 11 (39%) | 4 (14%) | 8 (23%) | 2 (3%) |
| Smoking status | |||||
| Before pregnancy (no) | n (%) | 22 (79%) | 18 (62%) | 23 (66%) | 64 (97%) |
| During pregnancy (no) | n (%) | 25 (89%) | 23 (79%) | 26 (77%) | 65 (99%) |
| Parameter | Statistic | Age | Control w/o Prebiotics IF 2 | Control IF | Concept IF | Breastfed 3 |
|---|---|---|---|---|---|---|
| Stool frequency (n/d) | Median (Q1–Q3; N) | 1 mo | 2.2 (1.1–3.7; 136) a | 2.6 (1.1–4.7; 115) a | 2.6 (1.4–3.9; 126) a | 4.9 (3.0–6.3; 114) b |
| 2 mo | 1.1 (0.7–2.1; 122) a | 1.1 (0.6–2.2; 104) a | 1.3 (0.7–2.3; 119) a | 2.6 (1.4–5.1; 17) b | ||
| 3 mo | 0.9 (0.4–1.7; 147) a | 1.0 (0.6–1.6; 132) a | 1.0 (0.6–1.8; 140) a | 1.7 (0.6–3.3; 75) b | ||
| 4 mo | 0.9 (0.4–1.4; 147) a | 1.0 (0.7–1.4; 134) b | 1.0 (0.6–1.7; 143) b | 1.3 (0.6–2.4; 67) c | ||
| Stool consistency score | Mean (SD; N) | 1 mo | 2.2 (0.5; 136) a | 2.1 (0.5; 115) a | 2.0 (0.3; 126) b | 1.9 (0.3; 112) b |
| 2 mo | 2.1 (0.5; 122) | 2.0 (0.4; 102) | 2.0 (0.4; 118) | 1.9 (0.2; 17) | ||
| 3 mo | 2.1 (0.5; 145) a | 2.0 (0.4; 131) ab | 1.9 (0.5; 139) bc | 1.8 (0.4; 75) c | ||
| 4 mo | 2.1 (0.4; 144) a | 2.0 (0.4; 132) a | 1.9 (0.5; 142) b | 1.9 (0.4; 67) b | ||
| Percentage of days with ≥1 watery stool | Mean (SD; N), % | 1 mo | 5.9 (17.6; 136) a | 9.3 (21.8; 115) ab | 10.3 (23.4; 126) b | 14.9 (30.8; 114) ab |
| 2 mo | 10.9 (26.4; 122) | 9.3 (23.2; 104) | 10.2 (22.3; 119) | 8.4 (18.3; 17) | ||
| 3 mo | 7.0 (20.7; 147) a | 8.8 (20.9; 132) ab | 13.5 (25.0; 140) bc | 15.1 (24.3; 75) c | ||
| 4 mo | 4.8 (17.9; 147) a | 10.5 (23.8; 134) b | 17.4 (30.9; 143) b | 16.2 (29.3; 67)bc | ||
| Percentage of days with ≥1 hard stool or no stool | Median (Q1–Q3; N), % | 1 mo | 0.0 (0.0–28.6; 136) a | 0.0 (0.0–28.6; 115) a | 0.0 (0.0–14.3; 126) a | 0.0 (0.0–0.0; 114) b |
| 2 mo | 14.3 (0.0–42.9; 122) | 14.3 (0.0–42.9; 104) | 14.3 (0.0–42.9; 119) | 0.0 (0.0–14.3; 17) | ||
| 3 mo | 28.6 (0.0–57.1; 147) | 28.6 (0.0–57.1; 132) | 28.6 (0.0–57.1; 140) | 14.3 (0.0–42.9; 75) | ||
| 4 mo | 28.6 (0.0–51.7; 147) a | 14.3 (0.0–42.9; 134) ab | 28.6 (0.0–42.9; 143) ab | 0.0 (0.0–57.1; 67) b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teoh, O.H.; Lin, T.P.; Abrahamse-Berkeveld, M.; Winokan, A.; Chong, Y.S.; Yap, F.; Marintcheva-Petrova, M.; van der Beek, E.M.; Shek, L.P. An Infant Formula with Large, Milk Phospholipid-Coated Lipid Droplets Supports Adequate Growth and Is Well-Tolerated in Healthy, Term Asian Infants: A Randomized, Controlled Double-Blind Clinical Trial. Nutrients 2022, 14, 634. https://doi.org/10.3390/nu14030634
Teoh OH, Lin TP, Abrahamse-Berkeveld M, Winokan A, Chong YS, Yap F, Marintcheva-Petrova M, van der Beek EM, Shek LP. An Infant Formula with Large, Milk Phospholipid-Coated Lipid Droplets Supports Adequate Growth and Is Well-Tolerated in Healthy, Term Asian Infants: A Randomized, Controlled Double-Blind Clinical Trial. Nutrients. 2022; 14(3):634. https://doi.org/10.3390/nu14030634
Chicago/Turabian StyleTeoh, Oon Hoe, Tan Pih Lin, Marieke Abrahamse-Berkeveld, Antoinette Winokan, Yap Seng Chong, Fabian Yap, Maya Marintcheva-Petrova, Eline M. van der Beek, and Lynette P. Shek. 2022. "An Infant Formula with Large, Milk Phospholipid-Coated Lipid Droplets Supports Adequate Growth and Is Well-Tolerated in Healthy, Term Asian Infants: A Randomized, Controlled Double-Blind Clinical Trial" Nutrients 14, no. 3: 634. https://doi.org/10.3390/nu14030634
APA StyleTeoh, O. H., Lin, T. P., Abrahamse-Berkeveld, M., Winokan, A., Chong, Y. S., Yap, F., Marintcheva-Petrova, M., van der Beek, E. M., & Shek, L. P. (2022). An Infant Formula with Large, Milk Phospholipid-Coated Lipid Droplets Supports Adequate Growth and Is Well-Tolerated in Healthy, Term Asian Infants: A Randomized, Controlled Double-Blind Clinical Trial. Nutrients, 14(3), 634. https://doi.org/10.3390/nu14030634