
Effect of Obesity Surgery on Taste

 , and
, and
Abstract
:1. Introduction
1.1. Physiology of Taste
- The sensory domain is concerned with the detection, recognition and perception of the intensity of a stimulus, e.g., does this cake taste sweet and how sweet? The detection threshold is defined as the minimum concentration at which a participant identifies a taste stimulus different from water, whereas the recognition threshold is defined as the minimum concentration at which a participant recognizes the quality of the taste stimulus. Taste intensity can be defined as the magnitude of a quality of the taste; it affects the liking of foods, and determines food choice and consumption [10].
- The hedonic domain refers to the reward driving ingestion of a stimulus, e.g., how much do I want this cake and how much do I like it when I eat it?Food reward can be divided into appetitive and consummatory components. Appetitive reward reflects the effort made to pursue the desired food, and consummatory reward is the pleasure derived upon ingesting the food [11]. The two reward behaviour components can be studied in isolation and combination, depending on the required outcome. The direct behavioural method used to study appetitive food reward is the progressive ratio task (PRT) [12,13]. In the PRT, the subject must work for a rewarding stimulus; for example, this could involve clicking a computer mouse several times which measures motivational incentive or reward strength of a stimulus [12]. Consummatory behaviour can be assessed using a taste reactivity test [14]. This test has not been used in human studies but only in animal studies. The stimulus is delivered directly to the oral cavity, and the facial reactions are videotaped [14]. The common positive responses in the animals included paw licking and tongue protrusions, while the common negative response included chin rubbing and gape [15]. The brief access test is another method that can measure both components of the reward domain. This test has also been used in animal models only. A small amount of the taste stimulus is presented for a short duration (around 10 s), and a lick monitoring system (gustometer) is used to measure the animal licking responses [16]. It measures the amount of effort the animal makes to approach the stimulus, i.e., appetitive reward. It also reflects the consummatory reward domain by measuring the repetitive licks per unit over the test duration [16].
- The physiological domain comprises the body’s reactions to sensing, i.e., the smell or sight of food. These reactions lead to the activation of pathways to help with digestion and maintenance of homeostasis. Salivation is the most apparent response and can be triggered by the mere thought of food but usually increases when food is present in the oral cavity [17]. There are links between the physiological and reward domains. It has been reported that people with obesity have a higher rate of salivation to food cues [18,19]. People with obesity also have a slower habituation rate (reduced salivation to the same food within a meal), possibly causing more food intake, as saliva helps dissolve food molecules and improves the ability to taste [18,20,21,22]. Another taste-related cephalic response is pre-absorptive insulin release, studied extensively in animals [23,24,25,26] and humans [27,28,29,30], however, not in relation to taste.
1.2. Taste and Obesity
1.3. Aims and Objectives
- Collated results from individual studies in the literature reporting taste in cross-sectional and longitudinal studies of obesity surgery.
- How heterogeneity in study methodology, design, protocol and analysis might explain differences between studies;
- Differences between results particularly in terms of type of obesity surgery.
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Inclusion Criteria
- Studies published in English.
- Articles published between January 1980 to May 2021.
- Studies conducted on adolescents or adults aged ≥15 years of either gender.
- Participants in the intervention group diagnosed with obesity with BMI >30 kg/m2.
- Assessments of obesity surgery (RYGB or single anastomosis gastric bypass, VSG, adjustable gastric banding (AGB), vertical banded gastroplasty, pancreato-biliary diversion).
- Studies using physical taste stimuli or food as a measurement scale to assess taste change in the sensory domain (detection and/or recognition), reward domain (consummatory and/or appetitive), or physiological domain (differences in salivation).
- Studies that investigated the effect of obesity surgery on taste function either by comparing pre- vs. post-obesity surgery or cross-sectional including post-obesity surgery in patients and un-operated control groups.
2.1.2. Exclusion Criteria
- Studies conducted on animals.
- Reviews, editorials, letters and meeting abstracts.
- Articles assessing non-obesity procedures (e.g., gastrectomy secondary to gastric cancer); patients with obesity who did not undergo surgery or patients pre-surgically without post-surgical follow-up; and articles assessing satiety or hunger instead of gustation.
2.2. Database Search
2.3. Keywords/Terms Used
2.4. Data Extraction
2.5. Outcome Measure
3. Results
3.1. Study Design
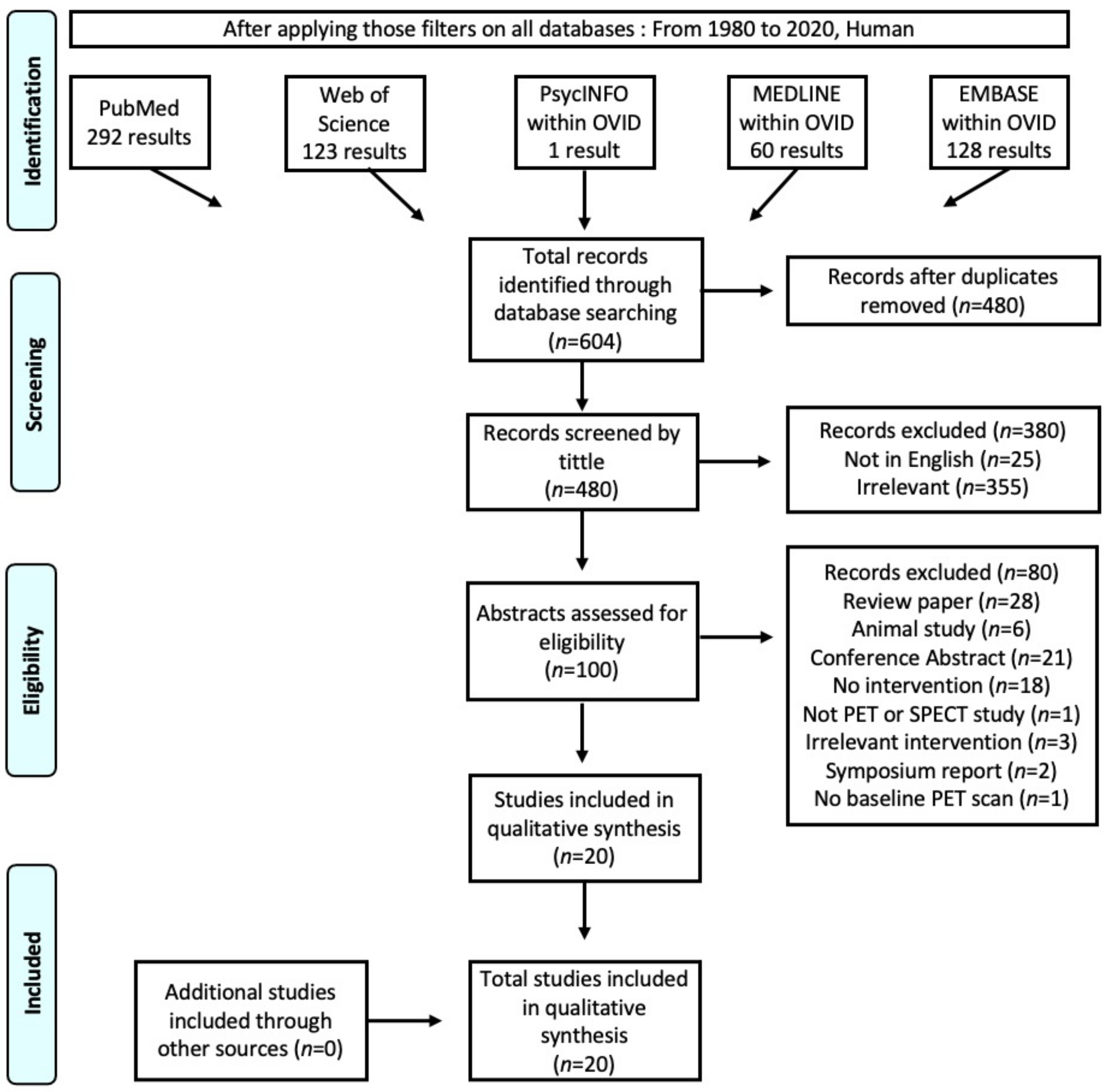
Search Results and Selection of Studies
3.2. Demographic Data
3.3. Study Protocols
3.3.1. Nutritional Status before the Taste Test
3.3.2. Time since the Intervention
3.4. Findings
3.4.1. Sensory Domain
Taste Detection after Obesity Surgery
Taste Recognition after Obesity Surgery
Taste Intensity after Obesity Surgery
3.4.2. Reward Domain
Appetitive Reward
Consummatory Reward
3.4.3. Physiological Domain
4. Discussion
4.1. Sensory Domain
4.2. Reward Domain
4.2.1. Appetitive Reward
4.2.2. Consummatory Reward
4.3. Physiological Domain
5. Limitation of the Included Studies
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miras, A.D.; Roux, C.W. Bariatric surgery and taste: Novel mechanisms of weight loss. Curr. Opin. Gastroenterol. 2010, 26, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Nance, K.; Acevedo, M.B.; Pepino, M.Y. Changes in taste function and ingestive behavior following bariatric surgery. Appetite 2020, 146, 104423. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Penney, N.; Darzi, A.; Purkayastha, S. Taste changes after bariatric surgery: A systematic review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [Green Version]
- Oliveira-Maia, A.J.; Roberts, C.D.; Simon, S.A.; Nicolelis, M.A.L. Gustatory and reward brain circuits in the control of food intake. Adv. Tech. Stand. Neurosurg. 2011, 36, 31–59. [Google Scholar]
- Gutierrez, R.; Fonseca, E.; Simon, S.A. The neuroscience of sugars in taste, gut-reward, feeding circuits, and obesity. Cell Mol. Life Sci. 2020, 77, 3469–3502. [Google Scholar] [CrossRef] [PubMed]
- Breslin, P.A.; Spector, A.C. Mammalian taste perception. Curr. Biol. 2008, 18, R148–R155. [Google Scholar] [CrossRef] [Green Version]
- Mizushige, T.; Inoue, K.; Fushiki, T. Why is fat so tasty? Chemical reception of fatty acid on the tongue. J. Nutr. Sci. Vitaminol. 2007, 53, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, G.; Oliveira-Maia, A.J. Sweet taste and obesity. Eur. J. Intern. Med. 2021, 92, 3–10. [Google Scholar] [CrossRef]
- Spector, A.C.; Glendinning, J.I. Linking peripheral taste processes to behavior. Curr. Opin. Neurobiol. 2009, 19, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Bartoshuk, L.M. The psychophysics of taste. Am. J. Clin. Nutr. 1978, 31, 1068–1077. [Google Scholar] [CrossRef]
- Burge, J.C.; Schaumburg, J.Z.; Choban, P.S.; Disilvestror, A.; Flancbaum, L. Changes in patients’ taste acuity after roux-en-Y gastric bypass for clinically severe obesity. J. Am. Diet. Assoc. 1995, 95, 666–670. [Google Scholar] [CrossRef]
- Münzberg, H.; Laque, A.; Yu, S.; Rezai-Zadeh, K.; Berthoud, H.-R. Appetite and body weight regulation after bariatric surgery. Obes. Rev. 2015, 16 (Suppl. 1), 77–90. [Google Scholar] [CrossRef] [Green Version]
- Miras, A.D.; Jackson, R.N.; Jackson, S.N.; Goldstone, A.P.; Olbers, T.; Hackenberg, T.; Spector, A.C.; le Roux, C.W. Gastric bypass surgery for obesity decreases the reward value of a sweet-fat stimulus as assessed in a progressive ratio task. Am. J. Clin. Nutr. 2012, 96, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Grill, H.J.; Norgren, R. The taste reactivity test. I. Mimetic responses to gustatory stimuli in neurologically normal rats. Brain Res. 1978, 143, 263–279. [Google Scholar] [CrossRef]
- Berridge, K. Measuring hedonic impact in animals and infants: Microstructure of affective taste reactivity patterns. Neurosci. Biobehav. Rev. 2000, 24, 173–198. [Google Scholar] [CrossRef]
- Al-Najim, W.; Docherty, N.G.; Le Roux, C.W. Food intake and eating behavior after bariatric surgery. Physiol. Rev. 2018, 98, 1113–1141. [Google Scholar] [CrossRef] [Green Version]
- Smeets, P.; Erkner, A.; De Graaf, C. Cephalic phase responses and appetite. Nutr. Rev. 2010, 68, 643–655. [Google Scholar] [CrossRef]
- Epstein, L.H.; Paluch, R.; Coleman, K.J. Differences in Salivation to Repeated Food Cues in Obese and Nonobese Women. Psychosom. Med. 1996, 58, 160–164. [Google Scholar] [CrossRef]
- Nirenberg, T.D.; Miller, P.M. Salivation: An assessment of food craving? Behav. Res. Ther. 1982, 20, 405–407. [Google Scholar] [CrossRef]
- Bond, D.S.; Raynor, H.; Vithiananthan, S.; Sax, H.C.; Pohl, D.; Roye, G.D.; Ryder, B.A.; Wing, R.R. Differences in Salivary Habituation to a Taste Stimulus in Bariatric Surgery Candidates and Normal-Weight Controls. Obes. Surg. 2009, 19, 873–878. [Google Scholar] [CrossRef]
- Temple, J.L.; Giacomelli, A.M.; Roemmich, J.N.; Epstein, L.H. Overweight children habituate slower than non-overweight children to food. Physiol. Behav. 2007, 91, 250–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, D.S.; Raynor, H.; McCaffery, J.; Wing, R.R. Salivary habituation to food stimuli in successful weight loss maintainers, obese and normal-weight adults. Int. J. Obes. 2010, 34, 593–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, E.G.; Trimble, E.R.; Renold, A.E.; Berthoud, H.R. Importance of preabsorptive insulin release on oral glucose tolerance: Studies in pancreatic islet transplanted rats. Gut 1980, 21, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthoud, H.R.; Bereiter, D.; Trimble, E.R.; Siegel, E.G.; Jeanrenaud, B. Cephalic phase, reflex insulin secretion neuroanatomical and physiological characterization. Diabetologia 1981, 20, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Berthoud, H.R.; Jeanrenaud, B. Sham feeding-induced cephalic phase insulin release in the rat. Am. J. Physiol. 1982, 242, E280–E285. [Google Scholar] [CrossRef]
- Berthoud, H.R.; Trimble, E.R.; Siegel, E.G.; Bereiter, D.A.; Jeanrenaud, B. Cephalic-phase insulin secretion in normal and pancreatic islet-transplanted rats. Am. J. Physiol. 1980, 238, E336–E340. [Google Scholar] [CrossRef]
- Wiedemann, S.J.; Rachid, L.; Illigens, B.; Böni-Schnetzler, M.; Donath, M.Y. Evidence for cephalic phase insulin release in humans: A systematic review and meta-analysis. Appetite 2020, 155, 104792. [Google Scholar] [CrossRef] [PubMed]
- Simon, C.; Schlienger, J.; Sapin, R.; Imler, M. Cephalic phase insulin secretion in relation to food presentation in normal and overweight subjects. Physiol. Behav. 1986, 36, 465–469. [Google Scholar] [CrossRef]
- Teff, K.L.; Levin, B.E.; Engelman, K. Oral sensory stimulation in men: Effects on insulin, C-peptide, and catecholamines. Am. J. Physiol. 1993, 265, R1223–R1230. [Google Scholar] [CrossRef] [PubMed]
- Teff, K.L.; Mattes, R.D.; Engelman, K. Cephalic phase insulin release in normal weight males: Verification and reliability. Am. J. Physiol. 1991, 261, E430–E436. [Google Scholar] [CrossRef]
- Boesveldt, S.; de Graaf, K. The differential role of smell and taste for eating behavior. Perception 2017, 46, 307–319. [Google Scholar] [CrossRef]
- Han, P.; Bagenna, B.; Fu, M. The sweet taste signalling pathways in the oral cavity and the gastrointestinal tract affect human appetite and food intake: A review. Int. J. Food Sci. Nutr. 2019, 70, 125–135. [Google Scholar] [CrossRef]
- Low, Y.Q.; Lacy, K.; Keast, R. The role of sweet taste in satiation and satiety. Nutrition 2014, 6, 3431–3450. [Google Scholar] [CrossRef] [Green Version]
- Iab, T.S.; Dando, R. Satiety, taste and the cephalic phase: A crossover designed pilot study into taste and glucose response. Foods 2020, 9, 1578. [Google Scholar] [CrossRef]
- Skrandies, W.; Zschieschang, R. Olfactory and gustatory functions and its relation to body weight. Physiol. Behav. 2015, 142, 1–4. [Google Scholar] [CrossRef]
- Harnischfeger, F.; Dando, R. Obesity-induced taste dysfunction, and its implications for dietary intake. Int. J. Obes. 2021, 45, 1644–1655. [Google Scholar] [CrossRef]
- Rohde, K.; Schamarek, I.; Blüher, M. Consequences of obesity on the sense of taste: Taste buds as treatment targets? Diabetes Metab. J. 2020, 44, 509–528. [Google Scholar] [CrossRef]
- Kittrell, H.; Graber, W.; Mariani, E.; Czaja, K.; Hajnal, A.; Di Lorenzo, P.M. Taste and odor preferences following Roux-en-Y surgery in humans. PLoS ONE 2018, 13, e01995088. [Google Scholar] [CrossRef]
- Hardikar, S.; Höchenberger, R.; Villringer, A.; Ohla, K. Higher sensitivity to sweet and salty taste in obese compared to lean individuals. Appetite 2017, 111, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Archer, N.; Shaw, J.; Cochet-Broch, M.; Bunch, R.; Poelman, A.; Barendse, W.; Duesing, K. Obesity is associated with altered gene expression in human tastebuds. Int. J. Obes. 2019, 43, 1475–1484. [Google Scholar] [CrossRef]
- Aguayo, G.; Vaillant, M.; Arendt, C.; Bachim, S.; Pull, C.B. Taste preference and psychopathology. Bull. Soc. Sci. Med. Grand-Duche Luxemb. 2012, 2, 7–14. [Google Scholar]
- Berthoud, H.-R.; Zheng, H. Modulation of taste responsiveness and food preference by obesity and weight loss. Physiol. Behav. 2012, 107, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Welbourn, R.; Hollyman, M.; Kinsman, R.; Dixon, J.; Liem, R.; Ottosson, J.; Ramos, A.; Vage, V.; Al-Sabah, S.; Brown, W.; et al. Bariatric surgery worldwide: Baseline demographic description and one-year outcomes from the Fourth IFSO Global Registry Report 2018. Obes. Surg. 2019, 29, 782–795. [Google Scholar] [CrossRef] [Green Version]
- Behary, P.; Miras, A. Food preferences and underlying mechanisms after bariatric surgery. Proc. Nutr. Soc. 2015, 74, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holinski, F.; Menenakos, C.; Haber, G.; Olze, H.; Ordemann, J. Olfactory and gustatory function after bariatric surgery. Obes. Surg. 2015, 25, 2314–2320. [Google Scholar] [CrossRef] [PubMed]
- Pepino, M.Y.; Bradley, J.C.D.; Eagon, S.; Sullivan, N.A.A.; Klein, S. Changes in Taste Perception and Eating Behavior after Bariatric Surgery-Induced Weight Loss in Women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef] [PubMed]
- Shoar, S.; Naderan, M.; Shoar, N.; Modukuru, V.R.; Mahmoodzadeh, H. Alteration pattern of taste perception after bariatric surgery: A systematic review of four taste domains. Obes. Surg. 2019, 29, 1542–1550. [Google Scholar] [CrossRef]
- Abdeen, G.N.; Miras, A.D.; Alqhatani, A.R.; Le Roux, C.W. Sugar detection threshold after laparoscopic sleeve gastrectomy in adolescents. Obes. Surg. 2018, 28, 1302–1307. [Google Scholar]
- El Labban, S.; Safadi, B.; Olabi, A. Effect of Roux-en-Y gastric bypass and sleeve gastrectomy on taste acuity and sweetness acceptability in postsurgical subjects. Nutrition 2016, 32, 1299–1302. [Google Scholar] [CrossRef]
- Bueter, M.; Miras, A.D.H.; Chichger, W.; Fenske, M.A.; Ghatei, S.R.; Bloom, R.J.; Unwin, T.A.; Lutz, A.C.S.; le Roux, C.W. Alterations of sucrose preference after roux-en-Y gastric bypass. Physiol. Behav. 2011, 104, 709–721. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.S.; Andersen, I.N.S.; Lange, B.; Ritz, C.; Le Roux, C.W.; Schmidt, J.B.; Sjödin, A.; Bredie, W.L. Bariatric surgery leads to short-term effects on sweet taste sensitivity and hedonic evaluation of fatty food stimuli. Obesity 2019, 27, 1796–1804. [Google Scholar] [CrossRef]
- Scruggs, D.M.; Buffington, C.; Cowan, G.S.M., Jr. Taste acuity of the morbidly obese before and after gastric bypass surgery. Obes. Surg. 1994, 4, 24–28. [Google Scholar] [CrossRef]
- Ribeiro, G.; Camacho, M.; Fernandes, A.B.; Cotovio, G.; Torres, S.; Oliveira-Maia, A.J. Reward-related gustatory and psychometric predictors of weight loss following bariatric surgery: A multicenter cohort study. Am. J. Clin. Nutr. 2021, 113, 751–761. [Google Scholar] [CrossRef]
- Altun, H.; Hanci, D.; Altun, H.; Batman, B.; Serin, R.K.; Karip, A.B.; Akyuz, U. Improved gustatory sensitivity in morbidly obese patients after laparoscopic sleeve gastrectomy. Ann. Otol. Rhinol. Laryngol. 2016, 125, 536–540. [Google Scholar] [CrossRef]
- Goldstone, A.P.; Miras, A.D.; Scholtz, S.; Jackson, S.; Neff, K.J.; Penicaud, L.; Geoghegan, J.; Chhina, N.; Durighel, G.; Bell, J.D.; et al. Link between increased satiety gut hormones and reduced food reward following gastric bypass surgery for obesity. J. Clin. Endocrinol. Metab. 2016, 101, 599–609. [Google Scholar] [CrossRef]
- Abdeen, G.N.; Miras, A.D.; Alqahtani, A.R.; le Roux, C.W. Vertical sleeve gastrectomy in adolescents reduces the appetitive reward value of a sweet and fatty reinforcer in a progressive ratio task. Surg. Obes. Relat. Dis. 2019, 15, 194–199. [Google Scholar] [CrossRef]
- Smith, K.R.; Papantoni, A.; Veldhuizen, M.G.; Kamath, V.; Harris, C.; Moran, T.H.; Carnell, S.; Steele, K.E. Taste-related reward is associated with weight loss following bariatric surgery. J. Clin. Investig. 2020, 130, 4370–4381. [Google Scholar] [CrossRef]
- Nance, K.; Eagon, J.C.; Klein, S.; Pepino, M.Y. Effects of sleeve gastrectomy vs. roux-en-Y gastric bypass on eating behavior and sweet taste perception in subjects with obesity. Nutrients 2017, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Scholtz, S.; Miras, A.; Chhina, N.; Prechtl, C.G.; Sleeth, M.L.; Daud, N.M.; Ismail, N.A.; Durighel, G.; Ahmed, A.R.; Olbers, T.; et al. Obese patients after gastric bypass surgery have lower brain-hedonic responses to food than after gastric banding. Gut 2014, 63, 891–902. [Google Scholar] [CrossRef] [Green Version]
- Ekmekcioglu, C.; Maedge, J.; Lam, L.; Blasche, G.; Shakeri-Leidenmühler, S.; Kundi, M.; Ludvik, B.; Langer, F.B.; Prager, G.; Schindler, K.; et al. Salt taste after bariatric surgery and weight loss in obese persons. PeerJ 2016, 4, e2086. [Google Scholar] [CrossRef] [Green Version]
- Joseph, P.V.; Mennella, J.A.; Cowart, B.J.; Pepino, M.Y. Psychophysical tracking method to assess taste detection thresholds in children, adolescents, and adults: The taste detection threshold (TDT) test. J. Vis. Exp. 2021, e62384. [Google Scholar] [CrossRef]
- Shelton, B.R.; Scarrow, I. Two-alternative versus three-alternative procedures for threshold estimation. Percept. Psychophys. 1984, 35, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, C.; Kallert, S.; Renner, B.; Stiassny, K.; Temmel, A.F.P.; Hummel, T.; Kobal, G. Quantitative assessment of gustatory function in a clinical context using impregnated ‘’taste strips’’. Rhinology 2003, 41, 2–6. [Google Scholar]
- Schwenger, K.J.; Alghamdi, M.M.; Ghorbani, Y.; Jackson, T.D.; Okrainec, A.; Allard, J.P. Hyposalivation is prevalent in bariatric patients but improves after surgery. Surg. Obes. Relat. Dis. 2020, 16, 1407–1413. [Google Scholar] [CrossRef] [PubMed]
- Marsicano, J.A.; Grec, P.G.D.M.; Belarmino, L.B.; Ceneviva, R.; Peres, S.H.D.C.S. Interfaces between bariatric surgery and oral health: A longitudinal survey. Acta Cir. Bras. 2011, 26 (Suppl. 2), 79–83. [Google Scholar] [CrossRef] [Green Version]
- Netto, B.D.; Moreira, E.A.; Patino, J.S.; Beninca, J.P.; Jordao, A.A.; Frode, T.S. Influence of roux-en-Y gastric bypass surgery on vitamin C, myeloperoxidase, and oral clinical manifestations: A 2-year follow-up study. Nutr. Clin. Pract. 2012, 27, 114–121. [Google Scholar] [CrossRef] [PubMed]
- De Moura-Grec, P.G.; Yamashita, J.M.; Marsicano, J.; Ceneviva, R.; Leite, C.V.D.S.; de Brito, G.B.; Brienze, S.L.A.; Sales-Peres, S.H.D.C. Impact of bariatric surgery on oral health conditions: 6-months cohort study. Int. Dent. J. 2014, 64, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Gondivkar, S.M.; Indurkar, A.; Degwekar, S.; Bhowate, R. Evaluation of gustatory function in patients with diabetes mellitus type 2. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 876–880. [Google Scholar] [CrossRef]
- Chaudhari, N.; Roper, S.D. The cell biology of taste. J. Cell Biol. 2010, 190, 285–296. [Google Scholar] [CrossRef] [Green Version]
- Umabiki, M.; Tsuzaki, K.; Kotani, K.; Nagai, N.; Sano, Y.; Matsuoka, Y.; Kitaoka, K.; Okami, Y.; Sakane, N.; Higashi, A. The improvement of sweet taste sensitivity with decrease in serum leptin levels during weight loss in obese females. Tohoku J. Exp. Med. 2010, 220, 267–271. [Google Scholar] [CrossRef] [Green Version]
- Ullrich, J.; Ernst, B.; Wilms, B.; Thurnheer, M.; Schultes, B. Roux-en Y gastric bypass surgery reduces hedonic hunger and improves dietary habits in severely obese subjects. Obes. Surg. 2013, 23, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Schultes, B.; Ernst, B.; Wilms, B.; Thurnheer, M.; Hallschmid, M. Hedonic hunger is increased in severely obese patients and is reduced after gastric bypass surgery. Am. J. Clin. Nutr. 2010, 92, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Ernst, B.; Thurnheer, M.; Wilms, B.; Schultes, B. Differential Changes in Dietary Habits after Gastric Bypass Versus Gastric Banding Operations. Obes. Surg. 2009, 19, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Mathes, C.M.; Bohnenkamp, R.A.; Le Roux, C.; Spector, A.C. Reduced sweet and fatty fluid intake after Roux-en-Y gastric bypass in rats is dependent on experience without change in stimulus motivational potency. Am. J. Physiol. Integr. Comp. Physiol. 2015, 309, R864–R874. [Google Scholar] [CrossRef]
- Tichansky, D.S.; Glatt, A.R.; Madan, A.K.; Harper, J.; Tokita, K.; Boughter, J.D. Decrease in sweet taste in rats after gastric bypass surgery. Surg. Endosc. 2011, 25, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Mathes, C.M.; Bueter, M.; Smith, K.R.; Lutz, T.A.; le Roux, C.W.; Spector, A.C. Roux-en-Y gastric bypass in rats increases sucrose taste-related motivated behavior independent of pharmacological glp-1-receptor modulation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2012, 302, R751–R767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson-Pérez, H.; Chambers, A.P.; A Sandoval, D.; Stefater, A.M.; Woods, S.C.; Benoit, S.C.; Seeley, R.J. The effect of vertical sleeve gastrectomy on food choice in rats. Int. J. Obes. 2013, 37, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirion-Delalande, C.; Gervais, F.; Fisch, C.; Cuiné, J.; Baron-Bodo, V.; Moingeon, P.; Mascarell, L. Comparative analysis of the oral mucosae from rodents and non-rodents: Application to the nonclinical evaluation of sublingual immunotherapy products. PLoS ONE 2017, 12, e0183398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeSesso, J.; Jacobson, C. Anatomical and physiological parameters affecting gastrointestinal absorption in humans and rats. Food Chem. Toxicol. 2001, 39, 209–228. [Google Scholar] [CrossRef]
- Bueter, M.; le Roux, C.W. Gastrointestinal hormones, energy balance and bariatric surgery. Int. J. Obes. 2011, 35 (Suppl. 3), S35–S39. [Google Scholar] [CrossRef] [Green Version]
- Iatridi, V.; Hayes, J.E.; Yeomans, M.R. Quantifying sweet taste liker phenotypes: Time for some consistency in the classification criteria. Nutrients 2019, 11, 129. [Google Scholar] [CrossRef] [Green Version]
- Kenler, H.; Brolin, R.E.; Cody, R.P. Changes in eating behavior after horizontal gastroplasty and Roux-en-Y gastric bypass. Am. J. Clin. Nutr. 1990, 52, 87–92. [Google Scholar] [CrossRef]
- Netto, B.D.M.; Earthman, C.P.; Farias, G.; Masquio, D.C.L.; Clemente, A.P.G.; Peixoto, P.; Bettini, S.C.; von Der Heyde, M.E.; Dâmaso, A.R. Eating patterns and food choice as determinant of weight loss and improvement of metabolic profile after RYGB. Nutrition 2017, 33, 125–131. [Google Scholar] [CrossRef]
- Gero, D.; Dib, F.; Ribeiro-Parenti, L.; Arapis, K.; Chosidow, D.; Marmuse, J.-P. Desire for Core Tastes Decreases After Sleeve Gastrectomy: A Single-Center Longitudinal Observational Study with 6-Month Follow-up. Obes. Surg. 2017, 27, 2919–2926. [Google Scholar] [CrossRef]
- Makaronidis, J.M.; Batterham, R.L. Potential Mechanisms Mediating Sustained Weight Loss Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Endocrinol. Metab. Clin. N. Am. 2016, 45, 539–552. [Google Scholar] [CrossRef]
- Ammon, B.S.; Bellanger, D.E.; Geiselman, P.J.; Primeaux, S.D.; Yu, Y.; Greenway, F.L. Short-Term Pilot Study of the Effect of Sleeve Gastrectomy on Food Preference. Obes. Surg. 2015, 25, 1094–1097. [Google Scholar] [CrossRef]
- Olbers, T.; Bjorkman, S.; Lindroos, A.; Maleckas, A.; Lonn, L.; Sjostrom, L.; Lonroth, H. Body composition, dietary intake, and energy expenditure after laparoscopic roux-en-Y gastric bypass and laparoscopic vertical banded gastroplasty: A randomized clinical trial. Ann. Surg. 2006, 244, 715–722. [Google Scholar] [CrossRef]
- Le Roux, C.W.; Bueter, M.; Theis, N.; Werling, M.; Ashrafian, H.; Lowenstein, C.; Athanasiou, T.; Bloom, S.R.; Spector, A.C.; Olbers, T.; et al. Gastric bypass reduces fat intake and preference. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 301, R1057–R1066. [Google Scholar] [CrossRef] [Green Version]
- Hajnal, A.; Kovacs, P.; Ahmed, T.; Meirelles, K.; Lynch, C.J.; Cooney, R.N. Gastric bypass surgery alters behavioral and neural taste functions for sweet taste in obese rats. Am. J. Physiol. Liver Physiol. 2010, 299, G967–G979. [Google Scholar] [CrossRef] [Green Version]
- Scarpellini, E.; Arts, J.; Karamanolis, G.; Laurenius, A.; Siquini, W.; Suzuki, H.; Ukleja, A.; Van Beek, A.; Vanuytsel, T.; Bor, S.; et al. International consensus on the diagnosis and management of dumping syndrome. Nat. Rev. Endocrinol. 2020, 16, 448–466. [Google Scholar] [CrossRef]
- Tack, J.; Arts, J.; Caenepeel, P.; De Wulf, D.; Bisschops, R. Pathophysiology, diagnosis and management of postoperative dumping syndrome. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Ukleja, A. Dumping Syndrome: Pathophysiology and Treatment. Nutr. Clin. Pract. 2005, 20, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.E.; King, W.; Chen, J.-Y.; Devlin, M.J.; Flum, D.; Garcia, L.; Inabet, W.; Pender, J.R.; Kalarchian, M.; Khandelwal, S.; et al. Course of depressive symptoms and treatment in the longitudinal assessment of bariatric surgery (LABS-2) study. Obesity 2014, 22, 1799–1806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halmi, K.A.; Mason, E.; Falk, J.R.; Stunkard, A. Appetitive behavior after gastric bypass for obesity. Int. J. Obes. 1981, 5, 457–464. [Google Scholar]
- Linner, J.H. Comparative effectiveness of gastric bypass and gastroplasty: A clinical study. Arch. Surg. 1982, 117, 695–700. [Google Scholar] [CrossRef]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef] [Green Version]
- Emous, M.; Wolffenbuttel, B.H.; van Dijk, G.; Totté, E.; van Beek, A.P. Long-term self-reported symptom prevalence of early and late dumping in a patient population after sleeve gastrectomy, primary, and revisional gastric bypass surgery. Surg. Obes. Relat. Dis. 2018, 14, 1173–1181. [Google Scholar] [CrossRef]
- Ahmad, A.; Kornrich, D.B.; Krasner, H.; Eckardt, S.; Ahmad, Z.; Braslow, A.; Broggelwirth, B. Prevalence of Dumping Syndrome After Laparoscopic Sleeve Gastrectomy and Comparison with Laparoscopic Roux-en-Y Gastric Bypass. Obes. Surg. 2019, 29, 1506–1513. [Google Scholar] [CrossRef]
- Chen, K.; Yan, J.; Suo, Y.; Li, J.; Wang, Q.; Lv, B. Nutritional status alters saccharin intake and sweet receptor mRNA expression in rat taste buds. Brain Res. 2010, 1325, 53–62. [Google Scholar] [CrossRef]
- Cooper, R.M.; Bilash, I.; Zubek, J.P. The effect of age on taste sensitivity. J. Gerontol. 1959, 14, 56–58. [Google Scholar] [CrossRef]
- Cowart, B.J. Development of taste perception in humans: Sensitivity and preference throughout the life span. Psychol. Bull. 1981, 90, 43–73. [Google Scholar] [CrossRef]
- Yoshinaka, M.; Ikebe, K.; Uota, M.; Ogawa, T.; Okada, T.; Inomata, C.; Takeshita, H.; Mihara, Y.; Gondo, Y.; Masui, Y.; et al. Age and sex differences in the taste sensitivity of young adult, young-old and old-old Japanese. Geriatr. Gerontol. Int. 2015, 16, 1281–1288. [Google Scholar] [CrossRef]
- Frank-Podlech, S.; Wilms, B.; Veit, R.; Ernst, B.; Thurnheer, M.; Kullmann, S.; Fritsche, A.; Birbaumer, N.; Preissl, H.; Schultes, B. Altered brain activity in severely obese women may recover after Roux-en Y gastric bypass surgery. Int. J. Obes. 2014, 38, 341–348. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; Van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Schachter, J.; Martel, J.; Lin, C.-S.; Chang, C.-J.; Wu, T.-R.; Lu, C.-C.; Ko, Y.-F.; Lai, H.-C.; Ojcius, D.M.; Young, J.D. Effects of obesity on depression: A role for inflammation and the gut microbiota. Brain Behav. Immun. 2018, 69, 1–8. [Google Scholar] [CrossRef]
- Reichenberger, J.; Kuppens, P.; Liedlgruber, M.; Wilhelm, F.H.; Tiefengrabner, M.; Ginzinger, S.; Blechert, J. No haste, more taste: An EMA study of the effects of stress, negative and positive emotions on eating behavior. Biol. Psychol. 2018, 131, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Hur, K.; Choi, J.S.; Zheng, M.; Shen, J.; Wrobel, B. Association of alterations in smell and taste with depression in older adults. Laryngoscope Invest. Otolaryngol 2018, 3, 94–99. [Google Scholar] [CrossRef]
- Amsterdam, J.D.; Settle, R.; Doty, R.L.; Abelman, E.; Winokur, A. Taste and smell perception in depression. Biol. Psychiatry 1987, 22, 1481–1485. [Google Scholar] [CrossRef]
- Platte, P.; Herbert, C.; Pauli, P.; Breslin, P.A.S. Oral perceptions of fat and taste stimuli are modulated by affect and mood induction. PLoS ONE 2013, 8, e65006. [Google Scholar] [CrossRef] [Green Version]
- Saluja, P.; Shetty, V.; Dave, A.; Arora, M.; Hans, V.; Madan, A. Comparative evaluation of the effect of menstruation, pregnancy and menopause on salivary flow rate, Ph and gustatory function. J. Clin. Diagn. Res. 2014, 8, ZC81–ZC85. [Google Scholar] [CrossRef]
- Elliott, S.A.; Ng, J.; Leow, M.K.-S.; Henry, C.J.K. The influence of the menstrual cycle on energy balance and taste preference in Asian Chinese women. Eur. J. Nutr. 2015, 54, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Brindisi, M.-C.; Brondel, L.; Meillon, S.; Barthet, S.; Grall, S.; Fenech, C.; Liénard, F.; Schlich, P.; Astruc, K.; Mouillot, T.; et al. Proof of concept: Effect of GLP-1 agonist on food hedonic responses and taste sensitivity in poor controlled type 2 diabetic patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2489–2494. [Google Scholar] [CrossRef] [PubMed]
- Kadouh, H.; Chedid, V.; Halawi, H.; Burton, D.D.; Clark, M.M.; Khemani, D.; Vella, A.; Acosta, A.; Camilleri, M. GLP-1 Analog Modulates Appetite, Taste Preference, Gut Hormones, and Regional Body Fat Stores in Adults with Obesity. J. Clin. Endocrinol. Metab. 2020, 105, 1552–1563. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.-K.; Martin, B.; Golden, E.; Dotson, C.D.; Maudsley, S.; Kim, W.; Jang, H.-J.; Mattson, M.P.; Drucker, D.J.; Egan, J.M.; et al. Modulation of taste sensitivity by GLP-1 signaling. J. Neurochem. 2008, 106, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Dotson, C.D.; Shin, Y.-K.; Ji, S.G.; Drucker, D.J.; Maudsley, S.; Munger, S.D. Modulation of Taste Sensitivity by GLP-1 Signaling in Taste Buds. Ann. N.Y. Acad. Sci. 2009, 1170, 98–101. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.; Passilly-Degrace, P.; Chevrot, M.; Ancel, D.; Sparks, S.M.; Drucker, D.J.; Besnard, P. Lipid-mediated release of GLP-1 by mouse taste buds from circumvallate papillae: Putative involvement of GPR120 and impact on taste sensitivity. J. Lipid Res. 2012, 53, 2256–2265. [Google Scholar] [CrossRef] [Green Version]
- Takai, S.; Yasumatsu, K.; Inoue, M.; Iwata, S.; Yoshida, R.; Shigemura, N.; Yanagawa, Y.; Drucker, D.J.; Margolskee, R.F.; Ninomiya, Y. Glucagon-like peptide-1 is specifically involved in sweet taste transmission. FASEB J. 2015, 29, 2268–2280. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Maudsley, S.; White, C.M.; Egan, J.M. Hormones in the naso-oropharynx: Endocrine modulation of taste and smell. Trends Endocrinol. Metab. 2009, 20, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Halatchev, I.G.; Cone, R.D. Peripheral administration of PYY3–36 produces conditioned taste aversion in mice. Cell Metab. 2005, 1, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Chelikani, P.K.; Haver, A.C.; Reidelberger, R.D. Dose-dependent effects of peptide YY(3-36) on conditioned taste aversion in rats. Peptides 2006, 27, 3193–3201. [Google Scholar] [CrossRef]
- Kulve, J.S.T.; Veltman, D.J.; Gerdes, V.E.; van Bloemendaal, L.; Barkhof, F.; Deacon, C.F.; Holst, J.J.; Drent, M.L.; Diamant, M.; Ijzerman, R.G. elevated postoperative endogenous glp-1 levels mediate effects of roux-en-Y gastric bypass on neural responsivity to food cues. Diabetes Care 2017, 40, 1522–1529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-L.; Yang, Q.; Hajnal, A.; Rogers, A.M. A pilot functional MRI study in Roux-en-Y gastric bypass patients to study alteration in taste functions after surgery. Surg. Endosc. 2016, 30, 892–898. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Psychophysical Task | Stimulus Presentation | Stimulus | |
|---|---|---|---|
| Detection and recognition threshold | Constant stimuli: In which taste stimuli are presented randomly and performance is assessed allowing for the derivation of a psychometric function. A “hit” is defined as when the participant correctly reported that the stimulus was different from water when stimulus was presented. A “false alarm” is defined as when the participant incorrectly reported that the stimulus was different from water when water was presented [50]. 2-Alternative Forced Choice (2-AFC): Participants are asked to differentiate the tastant from water, in multiple trials. The test begins at a concentration at which the tastant can be detected/recognised. After two correct trials, the test moves to a lower concentration, while a single incorrect trial leads to a higher concentration. The threshold is calculated based on the reversal concentrations. This type of test is sometimes referred to as a staircase [61]. 3-Alternative Forced Choice (3-AFC): Two samples of water and a sample of tastant are tasted at separate times for each trial. The detection threshold is the lowest concentration to receive two successive correct responses by the subjects just above the immediate lower concentration at which two successive incorrect responses are given or simply as the lowest concentration, the difference between the three drops can be detected. The recognition threshold refers to the concentration at which the subject can identify the taste quality [62]. Burghart taste strip test: The technique is based on strips made from filter paper which were impregnated with different taste solutions (four concentrations each for sweet, sour, salty and bitter). These strips are placed on the tongue and subjects are asked to identify the taste quality [63]. | Method of limits: Target tastants are offered in increasing (ascending) or decreasing (descending) concentrations. The threshold refers to the minimum concentration for taste detection. Method of constant stimuli: Stimuli of variable concentrations are presented in a random order to participants. Concentrations range from those which are known to be subthreshold and supra-threshold. The threshold is the concentration of the stimulus, perceived in more than half of the presentations. Adaptive method: The initial stimulus is a known supra-threshold stimulus, and is followed by stimuli of concentrations that decrease in predefined steps. The series is stopped when the stimulus strength becomes subthreshold. Then, the step is halved and increasing concentrations are given until the subject perceives the taste again. This process is repeated several times, reversing each time, until the step size reaches the preset minimal value. With this method, the threshold value can be delineated very accurately. | Solutions Model foods/beverages Filter papers |
| Intensity | Category scales: These are numeric scales and generally comprise descriptors equally spaced across a line (e.g., ranging from “1 = no taste” to “9 = extreme taste”). Common examples are the 9-point scale or visual analogue scale (VAS). General labelled magnitude scale (gLMS): This comprises a top anchor (‘strongest imaginable sensation of any kind’), an opposite anchor (‘barely detectable’) and intermediate labels. | Random order: stimuli are presented in a random order of intensity. Increasing concentrations: stimuli are presented in an order of increasing intensity | Solutions Model foods/beverages Filter papers |
| Author (year) | N | Group (s) | % Female | Age (y) | T2DM (%) | Time after Intervention (months) | Baseline BMI (kg/m2) | Weight Loss (% or kg) | Time Since Last Meal (h) | Taste Modality | Stimuli and Concentration | Methodology | Key Results (Post vs. Pre Surgery) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scruggs 1994 [52] | 6 10 | RYGB NWC | 100% 100% | 34.1 ± 7.8 36.7 ± 6.9 | ? | 1, 2, 3 n/a | 44.2 ± 7.1 20.6 ± 1.9 | 15, 10, 7 kg n/a | ? | sweet sour salty bitter | sucrose (6–5800 mM) HCl (0.5–500 mM) NaCl (6–6100 mM) urea (90–5000 mM) | 3-AFC [62] | ↑ SW a, SO, SA, BI |
| Bueter 2011 [50] | 99 | RYGB NWC | 88.9% 77.8% | ? | ? | 2 2 | 44.8 ± 5.4 22.0 ± 3.0 | 14 kg | ? | sweet | sucrose (2.1, 6.25, 12.5, 25, 50, 100 and 300 mM) | constant stimuli [50] | ↑ SW |
| Pepino 2014 [46] | 17 10 | RYGB AGB | 100% 100% | 42.1 ± 8.4 46.8 ± 13.9 | 0 0 | ~20% WL ~20% WL | 46.3 ± 7.7 48.5 ± 10.5 | 20.3 ± 3.0 kg 18.4 ± 2.0 kg | 12 h | sweet salty savoury | sucrose, glucose, NaCl, and MSG: (1 to 1 × 10−4 M) | 2-AFC [61] | ↔ SW (s, g), SA, SAV b |
| Holinski 2015 [45] | 37/ 4/ 3 23 | VSG/AGB/RYGB NOC | 65.9% 56.2% | 47.1 ± 9.8 39.5 ± 13.5 | 0 0 | 6 6 | 48.6 ± 7.5 23.4 ± 3.8 | 29.5 kg (20.6%) 0.1 kg (0.1%) | ? | sweet sour salty bitter | sucrose (0.4, 0.2, 0.1 and 0.05 g/mL) citric acid (0.3, 0.165, 0.09 and 0.05 g/mL) NaCl (0.25, 0.1, 0.04 and 0.016 g/mL) quinine HCl (0.006, 0.0024, 0.0009 and 0.0004 g/mL) | Burghart taste strip [63] | ↑ SW, SO, SA, BI b |
| Altun 2016 [54] | 52 | VSG | 57.7% | 38.5 ± 9.4 | ? | 1, 3 | 45.8 ± 7.2 | 1m: 25 ± 7.1% c 3m: 43.9 ± 10.3% c | 1 h | sweet sour salty bitter | sucrose (0.4, 0.2, 0.1, 0.05 g/mL) citric acid (0.3, 0.165, 0.09, 0.05 g/mL) NaCl (0.25, 0.1, 0.04, 0.016 g/mL) quinine HCl (0.006, 0.0024, 0.0009, 0.0004 g/mL) | Burghart taste strip [63] | ↑ SW, SO, SA, BI |
| Ekmekcioglu 2016 [60] | 19 29 | RYGB/SAGB NOC | 63.6% 48.3% | 46.3 ± 10.0 41.0 ± 12.8 | 30.3% 0 | 3 n/a | 43.2 ± 5.7 23.6 ± 3.0 | 21.8% n/a | ? | salty | NaCl (~0.003 to ~0.034 mol/L or ~0.16 g/L to ~2 g/L) | 3-AFC [62] | ↑ SA |
| Nance 2017 [58] | 23 8 | RYGB VSG | 87.0% 87.5% | 43.0 ± 9.6 36.6 ± 9.9 | 0 0 | ~20% WL ~20% WL | 46.9 ± 7.5 53.3 ± 8.7 | 19.8 ± 3.7% 19.3 ± 1.8% | 12 h | sweet salty savoury | sucrose, glucose, NaCl, and MSG: (1 × 10−4 to 1 M) | 2-AFC [61] | ↔ SW, SA, SAV |
| Abdeen 2018 [48] | 14 10 | VSG OOC | 71.4% 40.0% | 15.0 ± 1.9 15.1 ± 1.8 | ? | 3, 12 3 | 49.6 ± 5.9 32.0 ± 5.1 | 3m: 19.9 ± 1.2% 12m: 35.8 ± 1.3% | 12 h | sweet | sucrose (2.1, 6.25, 12.5, 25, 50, 100, AI9300 mM) | constant stimuli [50] | ↔ SW |
| Nielsen 2019 [51] | 21 8 29 | RYGB VSG NOC | 100% 100% 100% | 37.1 ± 9.9 45.0 ± 9.5 40.0 [10.4] | 0 0 0 | 1.5, 6, 18 1.5, 6, 18 n/a | 47.9 ± 6.5 43.5 ± 4.6 22.1 ± 2.4 | 18 m: 42.3 kg 18 m: 22.7 kg n/a | 1 h | sweet | sucrose (0 g/L, 0.34 g/L, 0.55 g/L, 0.94 g/L, 1.56 g/L, 2.59 g/L, 4.32 g/L, 7.2 g/L, 12 g/L) | 2-AFC [61] | ↔ SW b ↑ SW d ↔ SW e |
| Author (year) | N | Group (s) | % Female | Age at Baseline (y) | T2DM (%) | Time after Intervention (months) | Baseline BMI (kg/m2) | Weight Loss (% or kg) | Time Since Meal (h) | Taste Modality | Stimuli and Concentration | Methodology | Key Results (Post vs. Pre Surgery) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scruggs 1994 [52] | 6 10 | RYGB NWC | 100% 100% | 34.1 ± 7.8 36.7 ± 6.9 | ? | 1, 2, 3 n/a | 44.2 ± 7.1 20.6 ± 1.89 | 15, 10, 7 kg n/a | ? | Sweet Sour Salty Bitter | sucrose (6–5800 mM) HCl (0.5–500 mM) NaCl (6–6100 mM) urea (90–5000 mM) | 3-AFC [62] | ↑ SW a, SA, BI ↑↓ SO b |
| Burge 1995 [11] | 14 4 | RYGB VLCD | 57.1% | 38.4 ± 6 47 ± 6 | ? | 1.5, 3 1.5, 3 | 60.8 ± 11.8 43 ± 9 | ? | ? | Sweet Bitter | sucrose (0.01- 0.1 M) urea (0.01–0.5 M) | 2-AFC [61] | ↑ SW ↔ BI |
| Holinski 2015 [45] | 37/4/3 23 | VSG/AGB/RYGB NOC | 65.9% 56.2% | 47.1 ± 9.8 39.5 ± 13.5 | 0 0 | 6 6 | 48.6 ± 7.5 23.4 ± 3.8 | 29.5 kg (20.6%) 0.1 kg (0.1%) | ? | Sweet Sour Salty Bitter | sucrose (0.4, 0.2, 0.1, 0.05 g/mL) citric acid (0.3, 0.165, 0.09, 0.05 g/mL) NaCl (0.25, 0.1, 0.04, 0.016 g/mL) quinine HCl (0.006, 0.0024, 0.0009, 0.0004 g/mL) | Burghart taste strip [63] | ↑ SW, SO, SA, BI e |
| Altun 2016 [54] | 52 | VSG | 57.7% | 38.5 ± 9.4 | ? | 1, 3 | 45.8 ± 7.2 | 1m: 25 ±7.1% g 3m: 43.9 ±10.3% g | 1 h | Sweet Sour Salty Bitter | sucrose (0.4, 0.2, 0.1, 0.05 g/mL) citric acid (0.3, 0.165, 0.09, 0.05 g/mL) NaCl (0.25, 0.1, 0.04, 0.016 g/mL) quinine HCl (0.006, 0.0024, 0.0009, 0.0004 g/mL) | Burghart taste strip [63] | ↑ SW, SO, SA, BI |
| ElLabban 2016 [49] | 9 12 | RYGB VSG | 33.3% 75.0% | 37.0 ± 11.0 28.4 ± 7.2 | ? | 16.8 22.8 | 42.8 ± 3.6 41.3 ± 4.7 | 38.2 kg 35.9 kg | 2 h | Sweet Sour Salty Savoury | sucrose (64 mM) c citric acid 1-hydrate (8 mM) c sodium chloride (112 mM) c quinine sulfate (200 mM) c | 3-AFC [62] | ↔ SW, SA, BI d ↓ SO d |
| Nielsen 2019 [54] | 21 8 29 | RYGB VSG NOC | 100% 100% 100% | 37.1 ± 9.9 45.0 ± 9.5 40.0 [10.4] | 0 0 0 | 1.5, 6, 18 1.5, 6, 18 n/a | 47.9 ± 6.5 43.5 ± 4.6 22.1 ± 2.4 | 18 m: 42.3 kg 18 m: 22.7 kg n/a | 1 h | Sweet | sucrose (0 g/L, 0.34 g/L, 0.55 g/L, 0.94 g/L, 1.56 g/L, 2.59 g/L, 4.32 g/L, 7.2 g/L, 12 g/L) | 2-AFC [61] | ↔ SW e ↑ SW f |
| Author (year) | N | Group (s) | % Female | Age at Baseline (y) | T2DM (%) | Time after Intervention (months) | Baseline BMI (kg/m2) | Weight Loss (% or kg) | Time Since Meal (h) | Stimuli | Stimuli and Concentration | Methodology | Key Results (Post vs. Pre Surgery) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pepino 2014 [46] | 17 10 | RYGB/AGB | 100% 100% | 42.1 ± 8.4 46.8 ± 13.9 | 0 0 | ~20% WL ~20% WL | 46.3 ± 7.7 48.5 ± 10.5 | 20.3 ± 3.0 kg 18.4 ± 2.0 kg | 12 h | Sweet Sweet Salty Savoury | sucrose 0.00, 0.09, 0.36, 1.05 M glucose 0.00, 0.32, 0.56, 1.00 M NaCl 0.00, 0.056, 0.18, 0.56 M MSG 0.00, 0.02, 0.06, 0.18 M | gLMS solution random order | ↓ SW (s) a ↔ SW (g), SA, SAV b |
| Nance 2017 [58] | 23 8 | RYGB VSG | 87.0% 87.5% | 43.0 ± 9.6 36.6 ± 9.9 | 0 0 | ~20% WL ~20% WL | 46.9 ± 7.5 53.3 ± 8.7 | 19.8 ± 3.7% 19.3 ± 1.8% | 12 h | Sweet Sweet Salt Savoury | sucrose: 0, 90, 360, 1050 M glucose: 0, 320, 560, 1000 M NaCl: 0, 56, 180, 560 M MSG: 0, 20, 60, 180 M | gLMS solution ascending concentrations | ↔ SW, SA, SAV |
| Ribeiro 2021 [53] | 86 50 | RYGB/VSG OC | 87.5% 78% | 43.5 ± 10.3 43.0 ± 9.3 | 16.7% 26% | 12 ± 2.3 7.3 ± 4.3 | 42.9 ± 5.3 42.7 ± 5.0 | 31.9 ± 8.2% 1 ± 5.7% | 1 h | Sweet Sour Salty Bitter | sucrose (0.4, 0.2, 0.1, 0.05 g/mL) citric acid (0.3, 0.165, 0.09, 0.05 g/mL) NaCl (0.25, 0.1, 0.04, 0.016 g/mL) quinine HCL (0.006, 0.0024, 0.0009, 0.0004 g/mL) | gLMS taste strip ascending concentrations | ↔ SW, SO, SA, BI |
| Method | Procedures | |
|---|---|---|
| Appetitive reward domain | Progressive ratio task (PRT) | The subject must work for a rewarding stimulus; for example, this could involve clicking a computer mouse several times. The response requirement rises progressively until the subject stops making an effort for the reward, known as the breakpoint. The pioneering study of Hodos (1961) demonstrated that the number of responses made to obtain the last reward, termed the breakpoint, serves as an index of reward strength. |
| Consummatory reward domain | Category scales | Category scales are numeric and usually comprise descriptors equally spaced on a line (For example, from “1 = no taste” to “9 = extreme taste”. Common examples are the 9-point scale or the visual analogue scale (VAS). |
| General labelled hedonic scale (gLHS) | The gLHS assesses pleasantness. It includes a neutral midpoint extending in opposite directions. The top anchor indicates the ‘strongest liking of any kind ever experienced’, and the bottom anchor indicates the ‘strongest disliking of any kind ever experienced’, with intermediate labels in between. | |
| Two series forced-choice tracking procedure | Subjects are presented with different concentration pairs of the stimulus being tested (e.g., sucrose) to identify their preference. The procedure lasts until the subject either selects a particular stimulus concentration when it is paired with a higher or lower concentration together or chooses the highest or lowest concentration two times repeatedly. The entire task is repeated with concentration pairs presented in reverse. The most preferred stimulus level is determined by the geometric mean of the concentrations chosen during the two series. | |
| Just about right | The participants are asked whether a sensory characteristic of the stimulus (e.g., sucrose) is too high, too low, or just about right. The scales typically comprise 5 or 7 points, ranging from too little to too much for the different stimuli. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Alsheikh, A.S.; Alabdulkader, S.; Johnson, B.; Goldstone, A.P.; Miras, A.D. Effect of Obesity Surgery on Taste. Nutrients 2022, 14, 866. https://doi.org/10.3390/nu14040866
Al-Alsheikh AS, Alabdulkader S, Johnson B, Goldstone AP, Miras AD. Effect of Obesity Surgery on Taste. Nutrients. 2022; 14(4):866. https://doi.org/10.3390/nu14040866
Chicago/Turabian StyleAl-Alsheikh, Alhanouf S., Shahd Alabdulkader, Brett Johnson, Anthony P. Goldstone, and Alexander Dimitri Miras. 2022. "Effect of Obesity Surgery on Taste" Nutrients 14, no. 4: 866. https://doi.org/10.3390/nu14040866
APA StyleAl-Alsheikh, A. S., Alabdulkader, S., Johnson, B., Goldstone, A. P., & Miras, A. D. (2022). Effect of Obesity Surgery on Taste. Nutrients, 14(4), 866. https://doi.org/10.3390/nu14040866