
Reduced Kidney Function Is Associated with Increasing Red Blood Cell Folate Concentration and Changes in Folate Form Distributions (NHANES 2011–2018)

 , , ,
, , ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Demographic Characteristics
2.2. Kidney Biomarkers, Liver Biomarkers, and Blood Folate Concentrations
2.3. Usual Intake
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
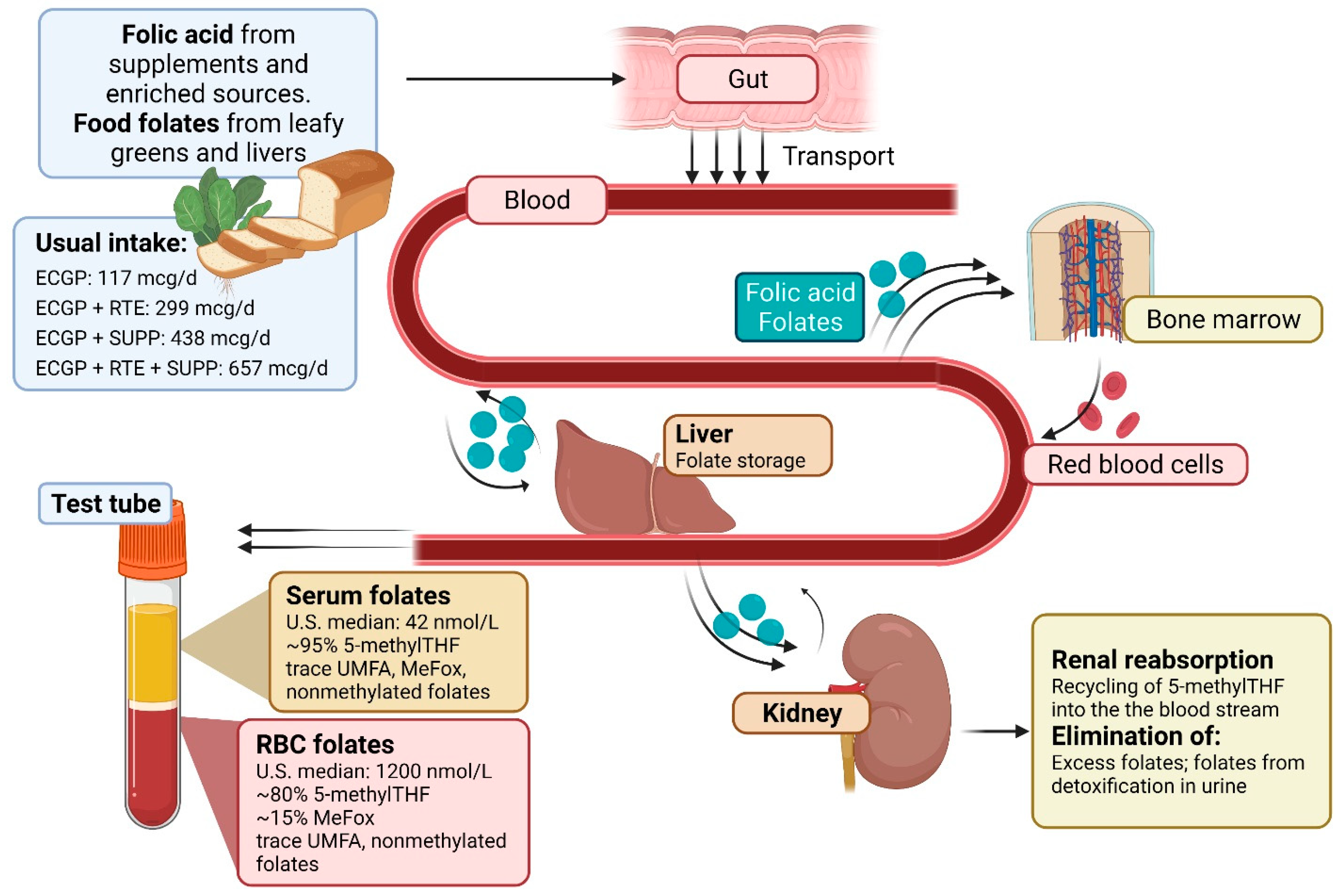
3.2. Folic Acid Usual Intake
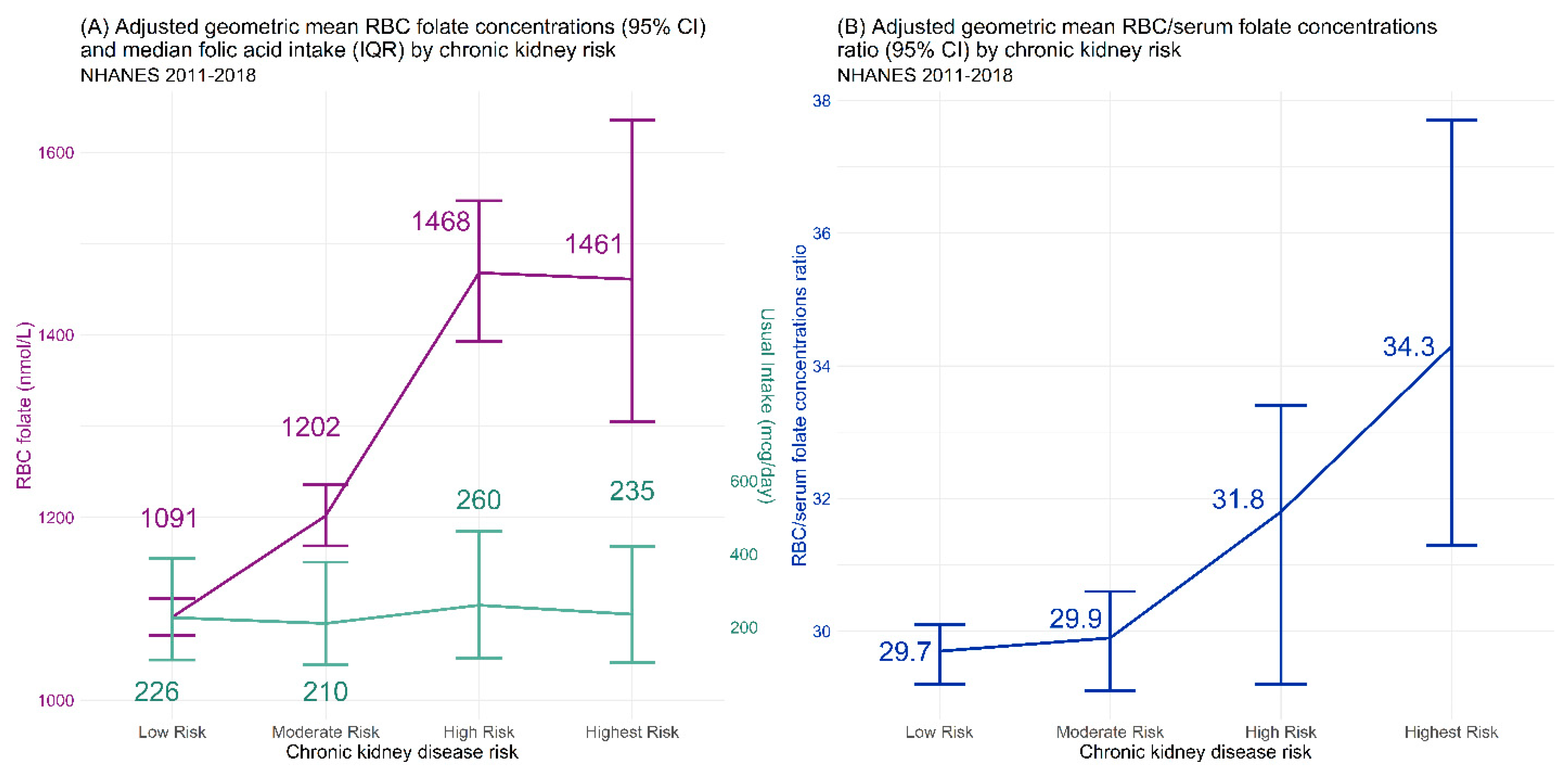
3.3. RBC Folate Concentrations
3.4. Serum Total Folate and Folate Forms
3.5. RBC/Serum Ratio
3.6. Liver Measures
4. Discussion
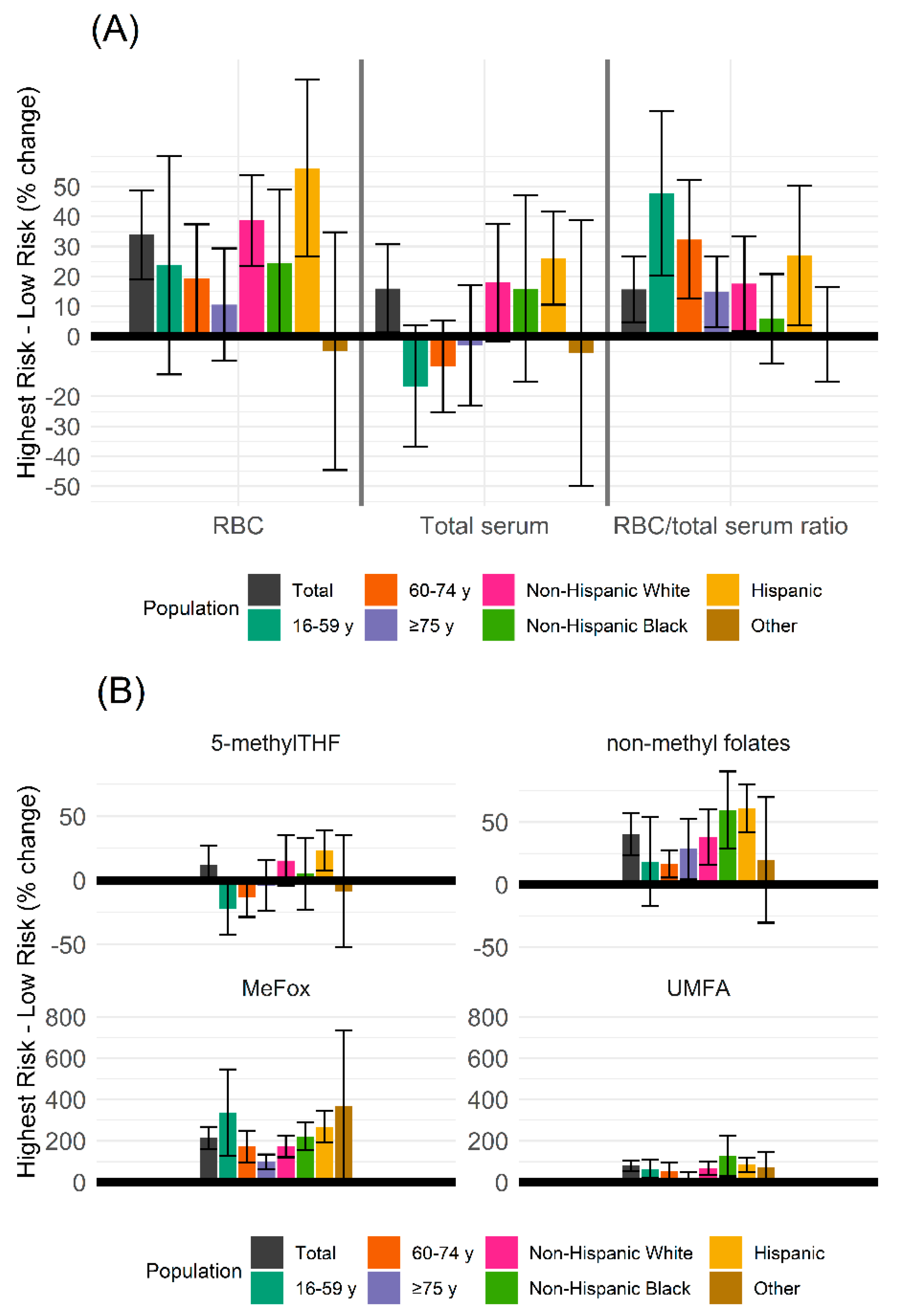
4.1. RBC and Serum Total Folates
4.2. Serum Folate Forms
4.3. Liver Biomarkers
4.4. Implications for Researchers
4.5. Limitations and Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 5,10-methenylTHF | 5,10-methenyletrahydrofolate |
| 5-formylTHF | 5-formyltetrahydrofolate |
| 5-methylTHF | 5-methyltetrahydrofolate |
| ACR | Albumin-to-creatinine ratio |
| aGM | Adjusted geometric mean |
| ALT | Alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | Body mass index |
| CKD | Chronic kidney disease |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| DFE | Dietary folate equivalents |
| ECGP | Enriched cereal grain product |
| eGFR | Estimated glomerular filtration rate |
| GED | General Equivalency Diploma |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| NHANES | National Health and Nutrition Examination Survey |
| MEC | Mobile examination center |
| NCI | National Cancer Institute |
| MeFox | Pyrazino-s-triazine derivative of 4-α-hydroxy-5-methyltetrahydrofolate |
| PIR | Poverty-income ratio |
| RBC | Red blood cell |
| RTE | Ready-to-eat cereals |
| SUP | Folic acid containing supplements |
| THF | Tetrahydrofolate |
| UMFA | Unmetabolized folic acid |
References
- National Toxicology Program. NTP Monograph: Identifying Research Needs for Assessing Safe Use of High Intakes of Folic Acid; US Department of Health and Human Services: Washington, DC, USA, 2015; pp. 1–51.
- Samodelov, S.L.; Gai, Z.; Kullak-Ublick, G.A.; Visentin, M. Renal Reabsorption of Folates: Pharmacological and Toxicological Snapshots. Nutrients 2019, 11, 2353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowrance, W.T.; Ordonez, J.; Udaltsova, N.; Russo, P.; Go, A.S. CKD and the risk of incident cancer. J. Am. Soc. Nephrol. 2014, 25, 2327–2334. [Google Scholar] [CrossRef] [Green Version]
- Bozack, A.K.; Hall, M.N.; Liu, X.; Ilievski, V.; Lomax-Luu, A.M.; Parvez, F.; Siddique, A.B.; Shahriar, H.; Uddin, M.N.; Islam, T.; et al. Folic acid supplementation enhances arsenic methylation: Results from a folic acid and creatine supplementation randomized controlled trial in Bangladesh. Am. J. Clin. Nutr. 2019, 109, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Kurzius-Spencer, M.; da Silva, V.; Thomson, C.A.; Hartz, V.; Hsu, C.H.; Burgess, J.L.; O’Rourke, M.K.; Harris, R.B. Nutrients in one-carbon metabolism and urinary arsenic methylation in the National Health and Nutrition Examination Survey (NHANES) 2003–2004. Sci. Total Environ. 2017, 607–608, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubey, M.; Shea, T.B. Potentiation of arsenic neurotoxicity by folate deprivation: Protective role of S-adenosyl methionine. Nutr. Neurosci. 2007, 10, 199–204. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES) 2011–2012; Centers for Disease Control and Prevention, National Center for Health Statistics: Atlanta, GA, USA, 2012.
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES) 2013–2014; Centers for Disease Control and Prevention, National Center for Health Statistics: Atlanta, GA, USA, 2014.
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES) 2015–2016; Centers for Disease Control and Prevention, National Center for Health Statistics: Atlanta, GA, USA, 2016.
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES) 2017–2018; Centers for Disease Control and Prevention, National Center for Health Statistics: Atlanta, GA, USA, 2018.
- Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Laboratory Procedures; U.S. Department of Human and Health Services, Centers for Disease Control: Hyattsville, MD, USA, 2011.
- Centers for Disease Control and Prevention. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/BIOPRO_J.htm (accessed on 21 December 2021).
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [Green Version]
- Yeung, L.F.; Cogswell, M.E.; Carriquiry, A.L.; Bailey, L.B.; Pfeiffer, C.M.; Berry, R.J. Contributions of enriched cereal-grain products, ready-to-eat cereals, and supplements to folic acid and vitamin B-12 usual intake and folate and vitamin B-12 status in US children: National Health and Nutrition Examination Survey (NHANES), 2003–2006. Am. J. Clin. Nutr. 2011, 93, 172–185. [Google Scholar] [CrossRef] [Green Version]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, J.F., 3rd; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development-Folate Review. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.M.; Sternberg, M.R.; Fazili, Z.; Lacher, D.A.; Zhang, M.; Johnson, C.L.; Hamner, H.C.; Bailey, R.L.; Rader, J.I.; Yamini, S.; et al. Folate status and concentrations of serum folate forms in the US population: National Health and Nutrition Examination Survey 2011–2012. Br. J. Nutr. 2015, 113, 1965–1977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazili, Z.; Sternberg, M.R.; Potischman, N.; Wang, C.Y.; Storandt, R.J.; Yeung, L.; Yamini, S.; Gahche, J.J.; Juan, W.; Qi, Y.P.; et al. Demographic, Physiologic, and Lifestyle Characteristics Observed with Serum Total Folate Differ Among Folate Forms: Cross-Sectional Data from Fasting Samples in the NHANES 2011–2016. J. Nutr. 2020, 150, 851–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiffer, C.M.; Sternberg, M.R.; Fazili, Z.; Yetley, E.A.; Lacher, D.A.; Bailey, R.L.; Johnson, C.L. Unmetabolized folic acid is detected in nearly all serum samples from US children, adolescents, and adults. J. Nutr. 2015, 145, 520–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visentin, M.; Diop-Bove, N.; Zhao, R.; Goldman, I.D. The intestinal absorption of folates. Annu. Rev. Physiol. 2014, 76, 251–274. [Google Scholar] [CrossRef] [Green Version]
- Zhao, R.; Matherly, L.H.; Goldman, I.D. Membrane transporters and folate homeostasis: Intestinal absorption and transport into systemic compartments and tissues. Expert Rev. Mol. Med. 2009, 11, e4. [Google Scholar] [CrossRef] [Green Version]
- Kamen, B.A.; Smith, A.K. A review of folate receptor alpha cycling and 5-methyltetrahydrofolate accumulation with an emphasis on cell models in vitro. Adv. Drug Deliv. Rev. 2004, 56, 1085–1097. [Google Scholar] [CrossRef]
- Crider, K.S.; Qi, Y.P.; Devine, O.; Tinker, S.C.; Berry, R.J. Modeling the impact of folic acid fortification and supplementation on red blood cell folate concentrations and predicted neural tube defect risk in the United States: Have we reached optimal prevention? Am. J. Clin. Nutr. 2018, 107, 1027–1034. [Google Scholar] [CrossRef]
- Chen, M.Y.; Rose, C.E.; Qi, Y.P.; Williams, J.L.; Yeung, L.F.; Berry, R.J.; Hao, L.; Cannon, M.J.; Crider, K.S. Defining the plasma folate concentration associated with the red blood cell folate concentration threshold for optimal neural tube defects prevention: A population-based, randomized trial of folic acid supplementation. Am. J. Clin. Nutr. 2019, 109, 1452–1461. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.M.; Sternberg, M.R.; Zhang, M.; Fazili, Z.; Storandt, R.J.; Crider, K.S.; Yamini, S.; Gahche, J.J.; Juan, W.; Wang, C.Y.; et al. Folate status in the US population 20 y after the introduction of folic acid fortification. Am. J. Clin. Nutr. 2019, 110, 1088–1097. [Google Scholar] [CrossRef]
- Saydah, S.H.; Pavkov, M.E.; Zhang, C.; Lacher, D.A.; Eberhardt, M.S.; Burrows, N.R.; Narva, A.S.; Eggers, P.W.; Williams, D.E. Albuminuria prevalence in first morning void compared with previous random urine from adults in the National Health and Nutrition Examination Survey, 2009–2010. Clin. Chem. 2013, 59, 675–683. [Google Scholar] [CrossRef] [Green Version]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [Green Version]
- Delgado, C.; Baweja, M.; Crews, D.C.; Eneanya, N.D.; Gadegbeku, C.A.; Inker, L.A.; Mendu, M.L.; Miller, W.G.; Moxey-Mims, M.M.; Roberts, G.V.; et al. A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. J. Am. Soc. Nephrol. 2021, 79, 268–288.e1. [Google Scholar] [CrossRef] [PubMed]
- Plantinga, L.C.; Boulware, L.E.; Coresh, J.; Stevens, L.A.; Miller, E.R., 3rd; Saran, R.; Messer, K.L.; Levey, A.S.; Powe, N.R. Patient awareness of chronic kidney disease: Trends and predictors. Arch. Intern. Med. 2008, 168, 2268–2275. [Google Scholar] [CrossRef] [PubMed]
- Ojodu, J.; Hulihan, M.M.; Pope, S.N.; Grant, A.M. Prevention. Incidence of sickle cell trait--United States, 2010. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 1155–1158. [Google Scholar] [PubMed]
- Naik, R.P.; Derebail, V.K.; Grams, M.E.; Franceschini, N.; Auer, P.L.; Peloso, G.M.; Young, B.A.; Lettre, G.; Peralta, C.A.; Katz, R.; et al. Association of sickle cell trait with chronic kidney disease and albuminuria in African Americans. JAMA 2014, 312, 2115–2125. [Google Scholar] [CrossRef]
- Key, N.S.; Derebail, V.K. Sickle-cell trait: Novel clinical significance. Hematol. Am. Soc. Hematol. Educ. Program. 2010, 2010, 418–422. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Low Risk | Moderate Risk | High Risk | Highest Risk | p Value 2 | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | Weighted % (95% CI) | n | Weighted % (95% CI) | n | Weighted % (95% CI) | n | Weighted % (95% CI) | ||
| Total | 15,238 | 2070 | 562 | 255 | |||||
| Age | |||||||||
| 16–59 | 11,855 | 80.6 (79.2, 82.0) | 982 | 41.4 (48.5, 54.3) | 156 | 33.2 (27.1, 39.3) | 47 | 23.2 (15.1, 32.3) | <0.0001 |
| 60–74 | 2710 | 15.8 (14.5, 17.0) | 665 | 30.4 (27.6, 33.2) | 175 | 25.5 (20.3, 30.8) | 82 | 27.3 (19.9, 34.7) | |
| ≥75 | 673 | 3.7 (3.3, 4.1) | 423 | 18.2 (16.2, 20.2) | 231 | 41.3 (36.6, 46.0) | 126 | 49.5 (41.3, 57.7) | |
| Sex | 0.0003 | ||||||||
| Male | 7296 | 48.1 (47.1, 49.22) | 918 | 40.8 (37.4, 44.2) | 271 | 42.4 (35.9, 48.8) | 147 | 48.0 (40.9, 55.1) | |
| Female | 7942 | 51.9 (50.8, 52.9) | 1152 | 59.2 (55.8, 62.6) | 291 | 57.6 (51.2, 64.1) | 108 | 52.0 (44.8, 59.1) | |
| Race/Hispanic origin | <0.0001 | ||||||||
| Non-Hispanic White | 5529 | 63.7 (59.9, 67.4) | 875 | 66.9 (62.4, 71.3) | 273 | 71.3 (66.4, 76.2) | 108 | 63.2 (54.1, 72.3) | |
| Non-Hispanic Black | 3313 | 10.9 (8.9, 12.9) | 488 | 12.1 (9.2, 14.9) | 130 | 12.5 (9.3, 15.6) | 67 | 15.8 (10.1, 21.6) | |
| Hispanic | 3931 | 16.2 (13.6, 18.8) | 464 | 13.0 (9.9, 16.0) | 102 | 9.6 (6.7, 12.5) | 52 | 11.2 (6.7, 15.7) | |
| Other | 2465 | 9.3 (8.0, 10.5) | 243 | 8.1 (6.3, 9.9) | 57 | 6.7 (4.4, 8.9) | 28 | 9.8 (5.1, 14.5) | |
| Education | <0.0001 | ||||||||
| <High School | 3819 | 16.6 (14.9, 18.3) | 618 | 20.9 (18.4, 23.3) | 157 | 21.9 (18.1, 25.7) | 80 | 24.3 (17.6, 31.0) | |
| High School graduate/GED | 3288 | 21.6 (20.1, 23.2) | 478 | 23.3 (20.4, 26.2) | 134 | 22.0 (17.6, 26.4) | 71 | 32.1 (23.8, 40.4) | |
| >High School | 8104 | 61.6 (59.1, 64.1) | 971 | 55.8 (52.0, 59.6) | 270 | 56.1 (50.8, 61.4) | 104 | 43.6 (36.3, 50.9) | |
| Missing | 27 | — | 3 | — | 1 | — | 0 | — | |
| Poverty/Income Ratio | 0.0001 | ||||||||
| <1.0 | 3153 | 14.7 (12.9, 16.4) | 461 | 16.9 (13.8, 18.2) | 125 | 17.2 (11.3, 23.1) | 59 | 23.7 (15.9, 31.5) | |
| 1.0—1.9 | 3384 | 17.6 (16.2, 18.9) | 529 | 20.9 (18.3, 23.5) | 158 | 24.1 (18.3, 30.0) | 71 | 24.3 (19.0, 29.6) | |
| 2.0—3.9 | 3507 | 24.9 (23.0, 26.7) | 468 | 25.6 (22.6, 28.6) | 120 | 23.7 (19.6, 27.8) | 65 | 25.1 (18.6, 31.6) | |
| ≥4.0 | 3545 | 33.3 (30.6, 36.1) | 384 | 28.7 (24.7, 32.7) | 91 | 25.1 (19.3, 30.9) | 28 | — | |
| Missing | 1649 | — | 228 | — | 68 | — | 32 | — | |
| BMI | <0.0001 | ||||||||
| Underweight (BMI < 18.5) | 310 | 1.7 (1.4, 2.0) | 55 | 2.5 (1.6, 3.4) | 12 | — | 3 | — | |
| Normal Weight (18.5 ≤ BMI < 25) | 4665 | 30.0 (28.6, 32.4) | 506 | 24.6 (22.2, 27.0) | 103 | 17.5 (14.0, 21.0) | 54 | 19.1 (13.2, 25.1) | |
| Overweight (25 ≤ BMI < 30) | 4735 | 31.8 (30.5, 33.1) | 591 | 28.1 (25.0, 31.2) | 176 | 32.3 (26.6, 38.0) | 80 | 26.6 (19.5, 33.8) | |
| Obese (BMI ≥ 30) | 5424 | 36.0 (34.5, 37.5) | 894 | 43.8 (40.7, 46.9) | 257 | 46.2 (40.2, 52.1) | 110 | 50.9 (41.3, 60.5) | |
| Missing | 104 | — | 24 | — | 14 | — | 8 | — | |
| Folic Acid source | 0.23 | ||||||||
| ECGP only | 8355 | 51.2 (49.5, 52.9) | 1100 | 49.2 (45.6, 52.7) | 270 | 42.4 (36.7, 48.0) | 133 | 49.0 (39.8, 58.1) | |
| ECGP + SUP | 3049 | 21.9 (20.7, 23.1) | 419 | 22.4 (19.5, 25.4) | 125 | 25.9 (20.4, 31.6) | 52 | 27.7 (17.2, 38.3) | |
| ECGP + RTE | 2690 | 17.5 (16.7, 18.3) | 380 | 19.0 (16.2, 21.8) | 110 | 20.4 (15.6, 25.2) | 49 | 16.0 (10.2, 21.9) | |
| ECGP + RTE + SUP | 1138 | 9.3 (8.4, 10.3) | 171 | 9.4 (7.6, 11.1) | 57 | 11.3 (8.0, 14.6) | 21 | — | |
| Missing | 6 | — | 0 | — | 0 | — | 0 | — | |
| n | Folic Acid (µg) | Natural Food Folate (DFE) | Total Folate (DFE) 2 | Total Folic Acid (µg) 3 | |
|---|---|---|---|---|---|
| Total | 18,127 | 225 (108, 390) | 201 (146, 264) | 610 (372, 914) | 366 (223, 548) |
| Age | |||||
| 16–59 y | 13,041 | 219 (112, 369) | 206 (149, 270) | 603 (381, 884) | 362 (229, 530) |
| 60–74 y | 3633 | 243 (101, 450) | 202 (149, 264) | 648 (369, 1014) | 389 (221, 606) |
| ≥75 y | 1453 | 268 (111, 481) | 172 (129, 219) | 647 (362, 1013) | 388 (217, 608) |
| p value 4 | 0.27 | 0.063 | 0.14 | 0.14 | |
| Race/Hispanic origin | |||||
| Hispanic | 4550 | 190 (93, 318) | 209 (146, 281) | 555 (342, 810) | 333 (205, 486) |
| Non-Hispanic White | 6785 | 244 (120, 423) | 200 (142, 258) | 649 (403, 969) | 389 (242, 581) |
| Non-Hispanic Black | 3999 | 179 (86, 308) | 168 (120, 220) | 489 (291, 736) | 293 (175, 442) |
| Other | 2793 | 222 (108, 374) | 216 (156, 286) | 624 (391, 907) | 374 (235, 544) |
| p value | 0.38 | 0.88 | 0.59 | 0.59 | |
| Folic acid source | |||||
| ECGP only | 9864 | 116 (78, 160) | 194 (140, 255) | 404 (305, 511) | 242 (183, 307) |
| ECGP + RTE | 3229 | 315 (276, 625) | 202 (147, 266) | 746 (625, 877) | 448 (375, 526) |
| ECGP + SUP | 3647 | 434 (272, 625) | 216 (161, 280) | 970 (688, 1299) | 582 (413, 779) |
| ECGP + RTE + SUP | 1387 | 653 (488, 839) | 220 (167, 283) | 1340 (1043, 1675) | 804 (626, 1005) |
| p value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| CKD risk | |||||
| Low Risk | 15,238 | 226 (110, 389) | 206 (150, 270) | 617 (381, 917) | 370 (229, 550) |
| Moderate Risk | 2070 | 212 (97, 381) | 189 (139, 246) | 577 (349, 880) | 346 (209, 528) |
| High Risk | 563 | 257 (112, 459) | 176 (132, 225) | 644 (363, 999) | 386 (218, 599) |
| Highest Risk | 250 | 234 (103, 419) | 150 (108, 198) | 558 (307, 893) | 335 (184, 535) |
| p value | 0.61 | 0.93 | 0.72 | 0.72 |
| CKD Risk Group | |||||
|---|---|---|---|---|---|
| Analyte | Low Risk | Moderate Risk | High Risk | Highest Risk | p Value 2 |
| RBC folate (nmol/L) | |||||
| Overall | 1089 (1069, 1110) | 1189 (1158, 1220) | 1488 (1419, 1561) | 1443 (1302, 1598) | <0.0001 |
| 16–59 | 1053 (1032, 1074) | 1075 (1035, 1117) | 1277 (1169, 1394) | 1345 (1084, 1669) | 0.0008 |
| 60–74 | 1231 (1195, 1267) | 1263 (1202, 1329) | 1432 (1328, 1543) | 1377 (1212, 1563) | 0.0072 |
| ≥75 | 1387 (1330, 1446) | 1445 (1365, 1529) | 1736 (1621, 1859) | 1512 (1285, 1780) | 0.0008 |
| Hispanic | 998 (983, 1013) | 1097 (1047, 1149) | 1092 (1013, 1176) | 1460 (1186, 1799) | <0.0001 |
| Non-Hispanic White | 1161 (1139, 1184) | 1243 (1202, 1286) | 1645 (1555, 1739) | 1578 (1421, 1752) | <0.0001 |
| Non-Hispanic Black | 866 (847, 886) | 973 (919, 1029) | 1127 (1021, 1244) | 1081 (894, 1307) | <0.0001 |
| Other | 1049 (1026, 1072) | 1193 (1121, 1268) | 1173 (1056, 1304) | 1079 (792, 1469) | 0.022 |
| Serum folate (nmol/L) 3 | |||||
| Overall | 37.1 (36.3, 38.0) | 40.2 (38.8, 41.7) | 48.0 (44.3, 52.1) | 42.8 (37.8, 48.4) | <0.0001 |
| 16–59 | 35.3 (34.5, 36.1) | 35.7 (33.8, 37.8) | 34.7 (32.0, 37.6) | 30.4 (24.1, 38.2) | 0.77 |
| 60–74 | 44.3 (42.3, 46.4) | 41.3 (39.0, 43.8) | 44.7 (39.1, 51.0) | 38.0 (32.5, 44.4) | 0.066 |
| ≥75 | 55.3 (52.3, 58.6) | 54.5 (50.2, 59.2) | 66.9 (59.4, 75.4) | 53.6 (45.2, 63.5) | 0.18 |
| Hispanic | 34.9 (34.2, 35.7) | 38.2 (36.2, 40.3) | 38.0 (33.5, 43.2) | 44.5 (38.8, 51.1) | <0.0001 |
| Non-Hispanic White | 39.1 (38.1, 40.2) | 41.9 (40.1, 43.8) | 52.7 (47.5, 58.4) | 45.1 (38.1, 53.5) | <0.0001 |
| Non-Hispanic Black | 29.6 (28.7, 30.4) | 31.4 (29.5, 33.5) | 34.3 (30.1, 39.0) | 34.8 (27.1, 44.7) | 0.022 |
| Other | 37.0 (35.8, 38.3) | 42.8 (39.4, 46.6) | 42.7 (35.7, 51.1) | 36.5 (25.1, 53.2) | 0.06 |
| 5-methylTHF (nmol/L) | |||||
| Overall | 34.5 (33.7, 35.3) | 37.3 (36.0, 38.7) | 44.0 (40.5, 47.7) | 38.4 (33.8, 43.7) | <0.0001 |
| 16–59 | 32.8 (32.0, 33.5) | 33.3 (31.4, 35.3) | 32.0 (29.2, 35.0) | 26.4 (20.4, 34.1) | 0.62 |
| 60–74 | 41.2 (39.3, 43.2) | 38.4 (36.2, 40.7) | 40.4 (35.9, 45.4) | 34.0 (28.9, 40.0) | 0.02 |
| ≥75 | 51.0 (48.3, 53.9) | 50.1 (46.1, 54.4) | 61.4 (54.4, 69.3) | 49.0 (41.4, 58.0) | 0.20 |
| Hispanic | 32.6 (31.8, 33.4) | 35.7 (33.8, 37.8) | 35.0 (30.3, 40.5) | 40.5 (35.2, 46.6) | <0.0001 |
| Non-Hispanic White | 36.4 (35.4, 37.3) | 39.0 (37.3, 40.7) | 48.2 (43.4, 53.5) | 41.1 (34.5, 48.9) | <0.0001 |
| Non-Hispanic Black | 26.9 (26.2, 27.7) | 28.6 (26.7, 30.6) | 31.0 (27.2, 35.4) | 28.7 (22.3, 37.0) | 0.071 |
| Other | 34.7 (33.5, 35.9) | 39.8 (36.6, 43.3) | 39.6 (33.4, 47.0) | 33.2 (22.6, 48.6) | 0.11 |
| UMFA (nmol/L) | |||||
| Overall | 0.81 (0.78, 0.84) | 0.89 (0.84, 0.94) | 1.22 (1.09, 1.37) | 1.46 (1.26, 1.68) | <0.0001 |
| 16–59 | 0.77 (0.74, 0.79) | 0.73 (0.69, 0.78) | 0.74 (0.62, 0.88) | 1.25 (0.94, 1.66) | 0.90 |
| 60–74 | 0.95 (0.89, 1.02) | 0.97 (0.87, 1.08) | 1.24 (0.96, 1.62) | 1.48 (1.12, 1.95) | 0.02 |
| ≥75 | 1.34 (1.16, 1.54) | 1.34 (1.15, 1.56) | 1.87 (1.61, 2.18) | 1.55 (1.30, 1.85) | 0.023 |
| Hispanic | 0.68 (0.64, 0.71) | 0.72 (0.66, 0.79) | 0.78 (0.71, 0.86) | 1.28 (1.02, 1.59) | <0.0001 |
| Non-Hispanic White | 0.87 (0.83, 0.90) | 0.94 (0.87, 1.02) | 1.37 (1.19, 1.58) | 1.45 (1.20, 1.76) | <0.0001 |
| Non-Hispanic Black | 0.79 (0.76, 0.83) | 0.87 (0.80, 0.95) | 1.04 (0.89, 1.22) | 1.79 (1.19, 2.70) | <0.0001 |
| Other | 0.67 (0.64, 0.71) | 0.74 (0.60, 0.91) | 0.81 (0.54, 1.22) | 1.15 (0.74, 1.80) | 0.036 |
| Non-methyl folates (nmol/L) 4 | |||||
| Overall | 1.2 (1.1, 1.2) | 1.2 (1.2, 1.3) | 1.5 (1.4, 1.6) | 1.6 (1.4, 1.8) | <0.0001 |
| 16–59 | 1.1 (1.1, 1.2) | 1.1 (1.1, 1.2) | 1.3 (1.1, 1.4) | 1.3 (1.0, 1.6) | 0.024 |
| 60–74 | 1.3 (1.2, 1.4) | 1.3 (1.2, 1.4) | 1.5 (1.3, 1.7) | 1.4 (1.3, 1.6) | 0.13 |
| ≥75 | 1.5 (1.4, 1.6) | 1.6 (1.4, 1.7) | 1.8 (1.6, 2.0) | 1.9 (1.5, 2.3) | 0.0006 |
| Hispanic | 1.1 (1.0, 1.3) | 1.2 (1.1, 1.4) | 1.4 (1.1, 1.8) | 1.8 (1.6, 2.2) | <0.0001 |
| Non-Hispanic White | 1.2 (1.1, 1.2) | 1.2 (1.2, 1.3) | 1.6 (1.4, 1.7) | 1.6 (1.3, 1.9) | <0.0001 |
| Non-Hispanic Black | 1.1 (1.0, 1.3) | 1.3 (1.1, 1.4) | 1.4 (1.2, 1.6) | 1.8 (1.5, 2.2) | <0.0001 |
| Other | 1.1 (1.1, 1.2) | 1.3 (1.1, 1.4) | 1.3 (1.0, 1.6) | 1.5 (1.1, 2.0) | 0.0097 |
| MeFox (nmol/L) | |||||
| Overall | 1.4 (1.4, 1.5) | 1.8 (1.7, 1.8) | 2.7 (2.5, 2.9) | 4.4 (3.8, 5.0) | <0.0001 |
| 16–59 | 1.4 (1.4, 1.4) | 1.5 (1.4, 1.6) | 1.9 (1.6, 2.3) | 5.1 (3.8, 7.0) | <0.0001 |
| 60–74 | 1.6 (1.6, 1.7) | 1.9 (1.8, 2.1) | 2.8 (2.5, 3.2) | 4.3 (3.2, 5.8) | <0.0001 |
| ≥75 | 1.9 (1.8, 2.1) | 2.4 (2.2, 2.6) | 3.4 (3.1, 3.7) | 4.0 (3.4, 4.6) | <0.0001 |
| Hispanic | 1.2 (1.2, 1.3) | 1.4 (1.3, 1.6) | 1.9 (1.6, 2.2) | 4.2 (3.3, 5.2) | <0.0001 |
| Non-Hispanic White | 1.6 (1.5, 1.6) | 1.9 (1.8, 2.0) | 3.0 (2.8, 3.2) | 4.2 (3.6, 4.9) | <0.0001 |
| Non-Hispanic Black | 1.1 (1.1, 1.1) | 1.4 (1.3, 1.5) | 1.7 (1.3, 2.1) | 3.7 (3.0, 4.4) | <0.0001 |
| Other | 1.5 (1.4, 1.5) | 1.6 (1.4, 1.8) | 2.3 (1.8, 2.9) | 5.6 (3.4, 9.2) | <0.0001 |
| RBC/serum ratio | |||||
| Overall | 29.3 (28.9, 29.7) | 29.6 (28.8, 30.3) | 31.0 (29.0, 33.2) | 33.8 (30.8, 37.1) | 0.0046 |
| 16–59 | 29.9 (29.4, 30.3) | 30.0 (28.8, 31.3) | 36.8 (32.8, 41.3) | 44.2 (37.1, 52.5) | 0.0012 |
| 60–74 | 27.8 (26.9, 28.7) | 30.6 (29.3, 31.9) | 32.0 (28.7, 35.8) | 36.2 (31.0, 42.4) | <0.0001 |
| ≥75 | 25.0 (24.1, 25.9) | 26.5 (25.2, 27.9) | 25.9 (24.1, 27.9) | 28.4 (26.0, 31.1) | 0.028 |
| Hispanic | 28.6 (28.0, 29.1) | 28.7 (27.6, 29.9) | 28.7 (26.0, 31.7) | 33.8 (27.6, 41.5) | 0.13 |
| Non-Hispanic White | 29.7 (29.1, 30.3) | 29.7 (28.7, 30.6) | 31.2 (28.6, 34.1) | 35.0 (30.6, 40.0) | 0.042 |
| Non-Hispanic Black | 29.3 (28.7, 30.0) | 30.8 (29.4, 32.2) | 32.9 (30.1, 35.9) | 30.5 (26.8, 34.8) | 0.02 |
| Other | 28.3 (27.6, 29.0) | 27.8 (26.2, 29.6) | 27.5 (23.7, 31.9) | 29.5 (25.0, 34.8) | 0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, A.; Yeung, L.F.; Ríos Burrows, N.; Rose, C.E.; Fazili, Z.; Pfeiffer, C.M.; Crider, K.S. Reduced Kidney Function Is Associated with Increasing Red Blood Cell Folate Concentration and Changes in Folate Form Distributions (NHANES 2011–2018). Nutrients 2022, 14, 1054. https://doi.org/10.3390/nu14051054
Wang A, Yeung LF, Ríos Burrows N, Rose CE, Fazili Z, Pfeiffer CM, Crider KS. Reduced Kidney Function Is Associated with Increasing Red Blood Cell Folate Concentration and Changes in Folate Form Distributions (NHANES 2011–2018). Nutrients. 2022; 14(5):1054. https://doi.org/10.3390/nu14051054
Chicago/Turabian StyleWang, Arick, Lorraine F. Yeung, Nilka Ríos Burrows, Charles E. Rose, Zia Fazili, Christine M. Pfeiffer, and Krista S. Crider. 2022. "Reduced Kidney Function Is Associated with Increasing Red Blood Cell Folate Concentration and Changes in Folate Form Distributions (NHANES 2011–2018)" Nutrients 14, no. 5: 1054. https://doi.org/10.3390/nu14051054
APA StyleWang, A., Yeung, L. F., Ríos Burrows, N., Rose, C. E., Fazili, Z., Pfeiffer, C. M., & Crider, K. S. (2022). Reduced Kidney Function Is Associated with Increasing Red Blood Cell Folate Concentration and Changes in Folate Form Distributions (NHANES 2011–2018). Nutrients, 14(5), 1054. https://doi.org/10.3390/nu14051054