
Validation of a Low-protein Semi-Quantitative Food Frequency Questionnaire

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Construct Validity (Ability to Differentiate between Different Subjects)—Study Subjects
2.2. Content Validity (Checked by Experts in the Field)—Food Frequency Questionnaire Development
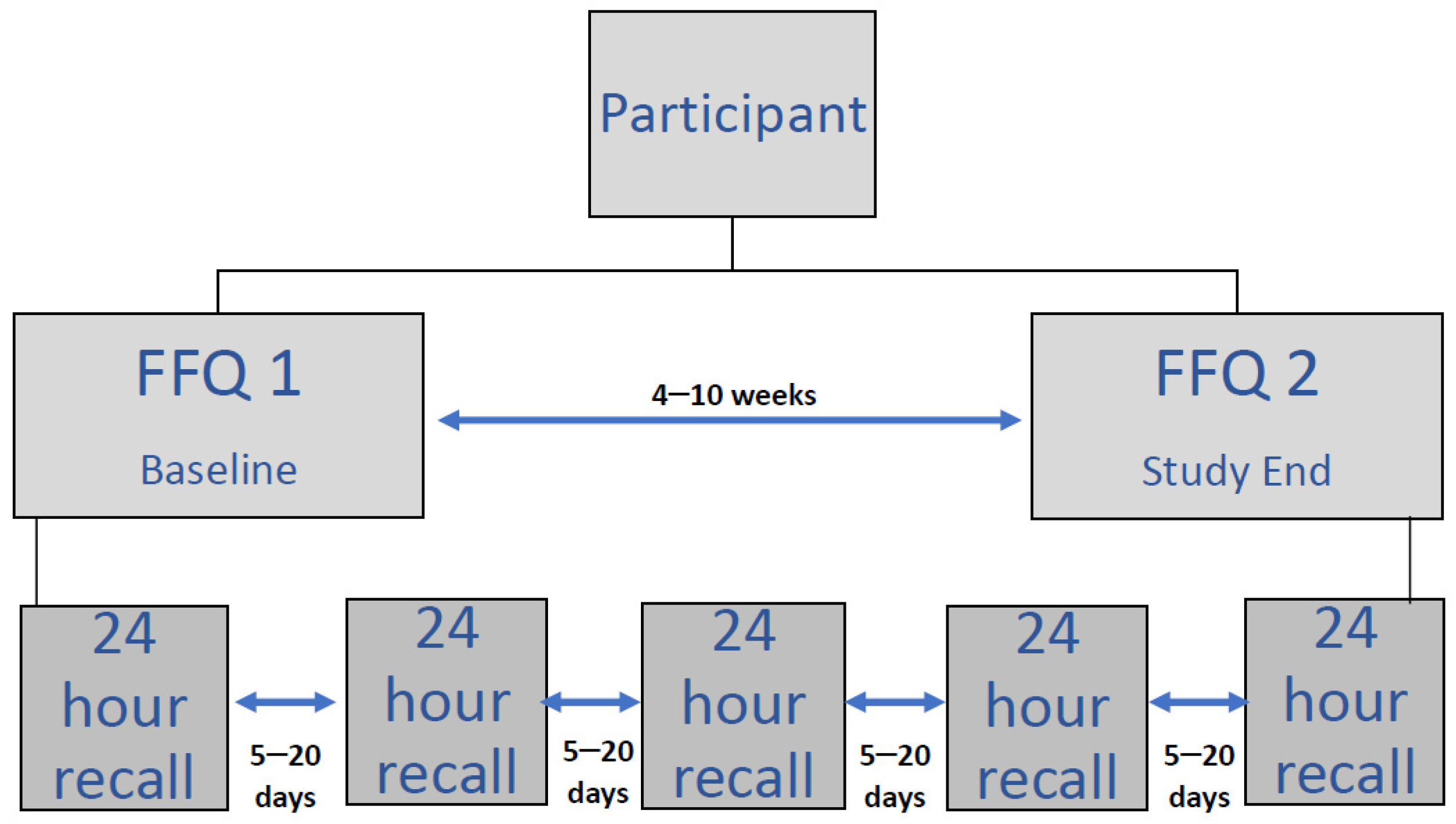
2.3. Reproducibility—Food Frequency Questionnaire
2.4. Portion Size Booklet
2.5. FFQ Database
2.6. Criterion Validity (Comparison with an Existing Standard)—24-h Dietary Recalls
2.7. Anthropometry
2.8. Statistics—Sample Size
2.9. Data Analysis
2.10. Ethical Approval
3. Results
3.1. Subjects
3.1.1. PKU Group
3.1.2. Control Group
3.2. Demographics and Anthropometry
3.3. Meal Patterns—FFQ 1 vs. FFQ 2 (Reproducibility) vs. Dietary Recalls (Criterion Validity-Comparison with an Existing Standard)
3.4. Protein Exchanges and Protein Substitute Intake
3.5. Macronutrient Intake
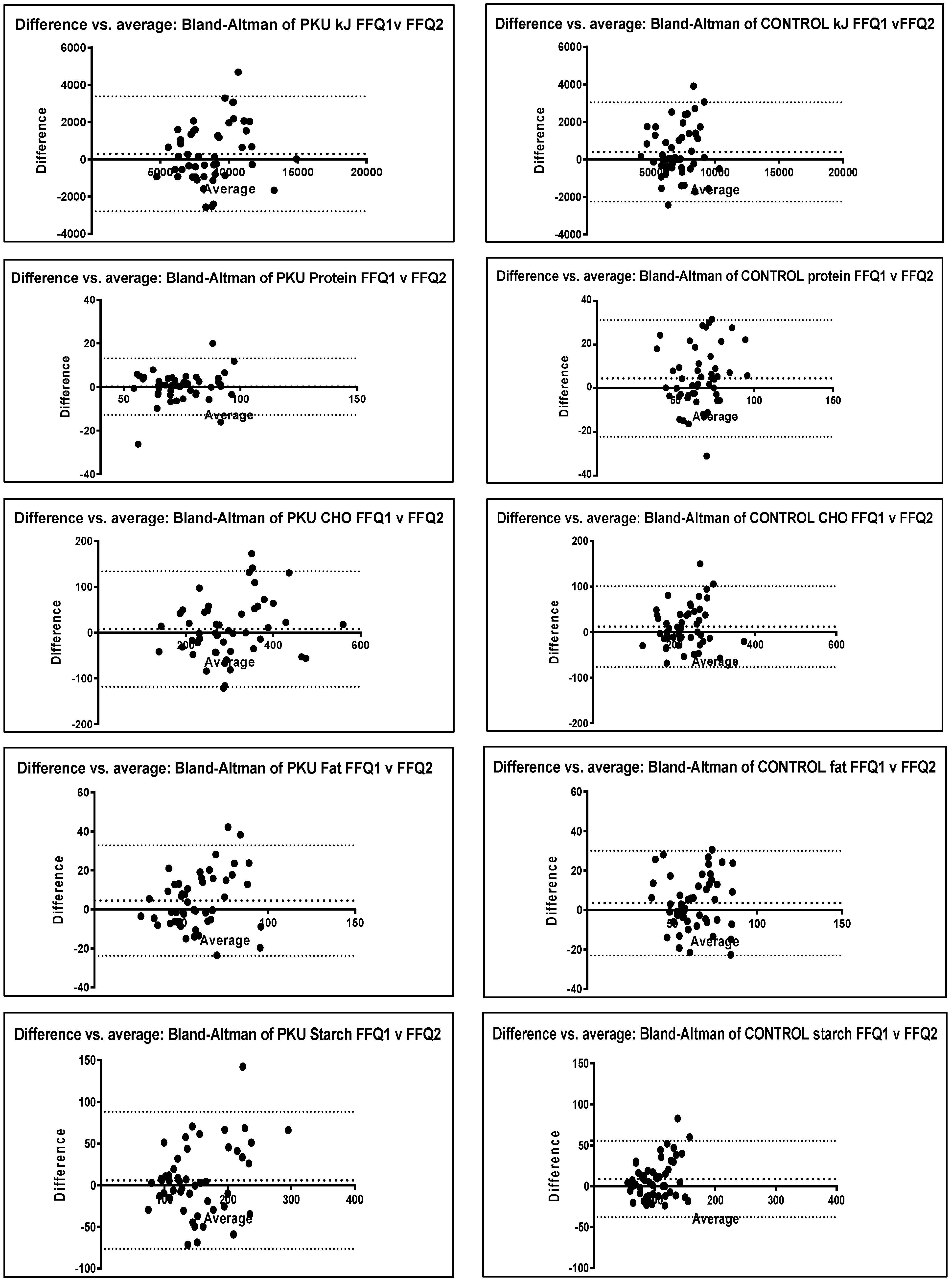
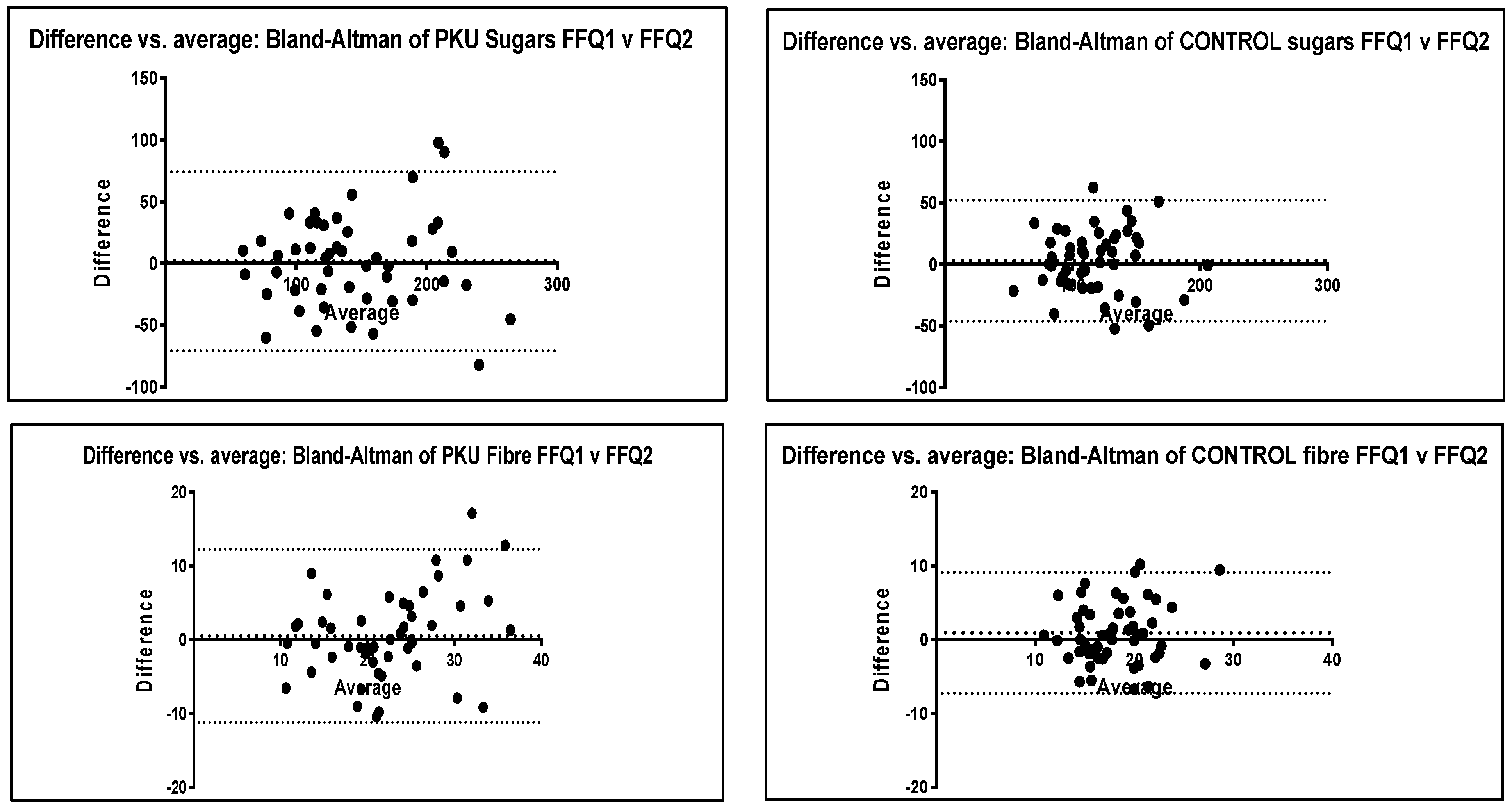
3.5.1. Reproducibility (A Measure of Whether the FFQ Produces the Same Results at Different Times)—FFQ 1 vs. FFQ 2
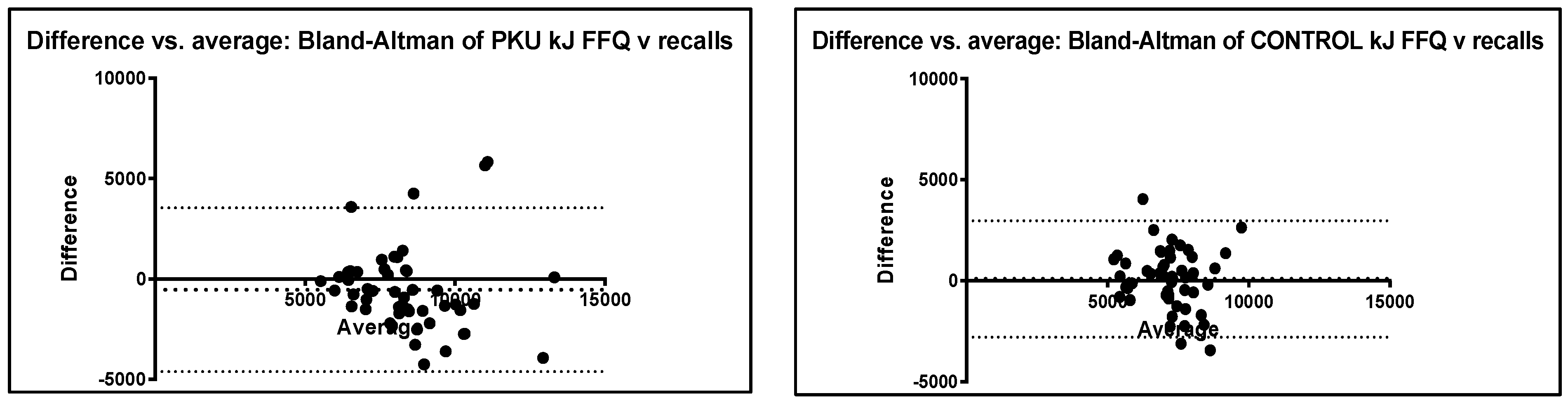
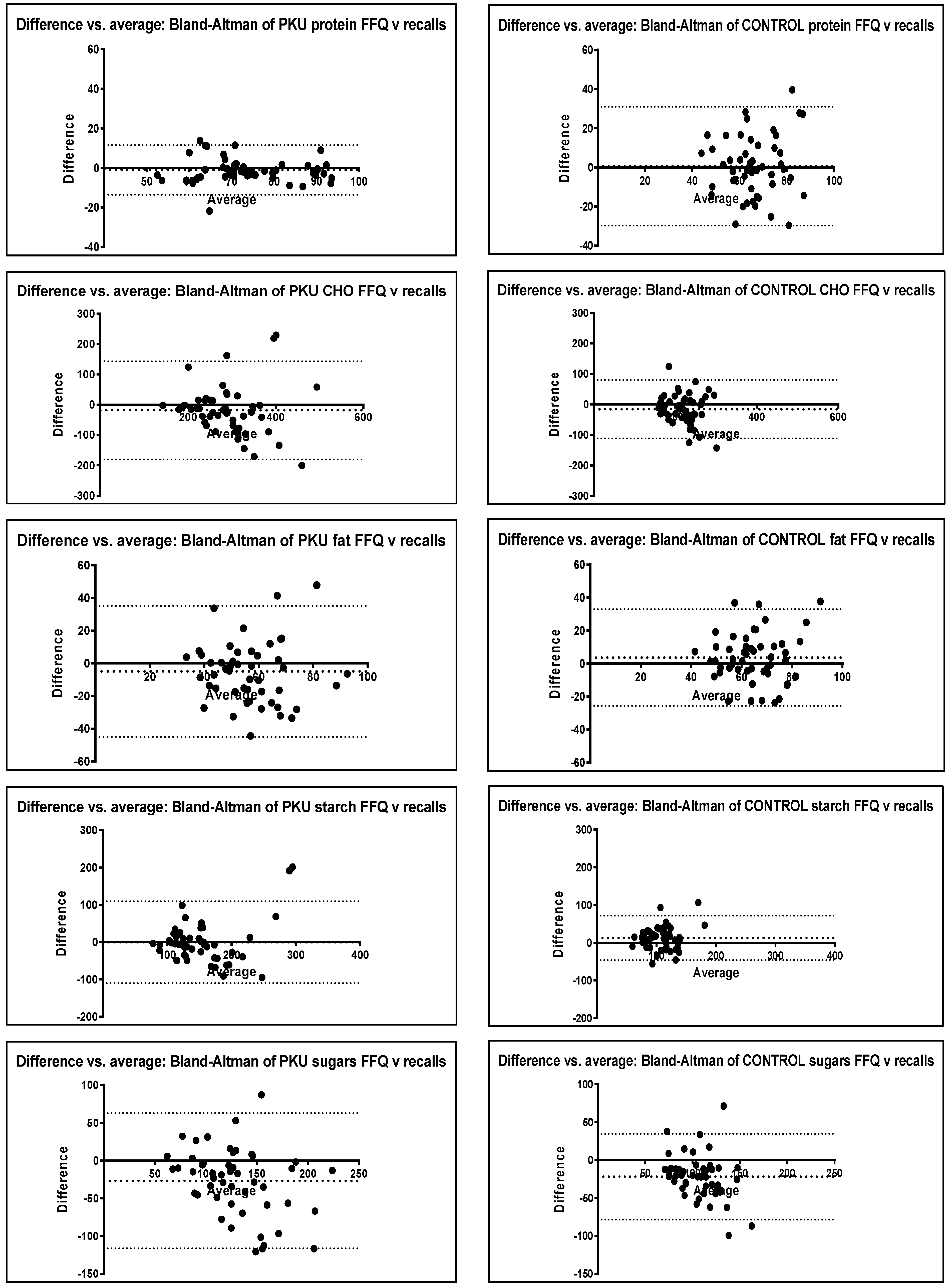
3.5.2. Criterion Validity (Comparison with an Existing Standard)—FFQ vs. Dietary recalls
3.5.3. Construct Validity (Ability to Distinguish between Different Groups)—PKU FFQ vs. Control FFQ
3.6. FFQ Individual Food Items
3.6.1. Reproducibility (A Measure of Whether the FFQ Produces the Same Results at Different Times)—FFQ 1 vs. FFQ 2
3.6.2. Criterion Validity (Comparison with an Existing Standard)—FFQ vs. Dietary Recalls
3.6.3. Construct Validity (Ability to Distinguish between Different Groups)—PKU FFQ vs. Control FFQ
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosini, G.L.; Emmett, P.M.; Northstone, K.; Howe, L.D.; Tilling, K.; Jebb, S.A. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int. J. Obes. 2012, 36, 1299–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohde, C.; Mütze, U.; Weigel, J.F.W.; Ceglarek, U.; Thiery, J.; Kiess, W.; Beblo, S. Unrestricted consumption of fruits and vegetables in phenylketonuria: No major impact on metabolic control. Eur. J. Clin. Nutr. 2012, 66, 633–638. [Google Scholar] [CrossRef]
- Evans, S.; Daly, A.; Chahal, S.; MacDonald, J.; MacDonald, A. Food acceptance and neophobia in children with phenylketonuria: A prospective controlled study. J. Hum. Nutr. Diet. 2016, 29, 427–433. [Google Scholar] [CrossRef]
- Daly, A.; Evans, S.; Pinto, A.; Ashmore, C.; Rocha, J.C.; MacDonald, A. A 3 Year Longitudinal Prospective Review Examining the Dietary Profile and Contribution Made by Special Low Protein Foods to Energy and Macronutrient Intake in Children with Phenylketonuria. Nutrients 2020, 12, 3153. [Google Scholar] [CrossRef]
- Evans, S.; Daly, A.; Chahal, S.; Ashmore, C.; MacDonald, J.; MacDonald, A. The influence of parental food preference and neophobia on children with phenylketonuria (PKU). Mol. Genet. Metab. Rep. 2018, 14, 10–14. [Google Scholar] [CrossRef]
- MacDonald, A.; Harris, G.; Rylance, G.; Asplin, D.; Booth, I.W. Abnormal feeding behaviours in phenylketonuria. J. Hum. Nutr. Diet. 1997, 10, 163–170. [Google Scholar] [CrossRef]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Viau, K.S.; Ernst, S.L. Food Frequency Questionnaire. Top. Clin. Nutr. 2014, 29, 332–342. [Google Scholar] [CrossRef]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Howard, K. Validating Questionnaires. 2008. Available online: https://www.researchgate.net/profile/Julio_Torales/post/To_perform_a_questionnaire_study_how_to_validate_the_questionnaire/attachment/59d638ff79197b8077996361/AS%3A399936555372544%401472363713499/download/Validating_Questionnaires.pdf (accessed on 6 March 2022).
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Collingridge, D. Validating a Questionnaire. 2014. Available online: https://www.methodspace.com/blog/validating-a-questionnaire (accessed on 6 March 2022).
- McCance and Widdowson. The Composition of Foods 7th edn. 2015. Available online: https://www.gov.uk/government/publications/composition-of-foods-integrated-dataset-cofid (accessed on 19 May 2016).
- Nutritics, Research Edition Professional Premium. 2019. v5.7. Available online: https://www.nutritics.com/p/home (accessed on 7 March 2022).
- Dumartheray, E.W.; Krieg, M.A.; Cornuz, J.; Whittamore, D.R.; Lovell, D.P.; Burckhardt, P.; Lanham-New, S.A. Validation and reproducibility of a semi-quantitative Food Frequency Questionnaire for use in elderly Swiss women. J. Hum. Nutr. Diet. 2006, 19, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.F.; Collins, C.E.; Sibbritt, D.W.; Dibley, M.J.; Garg, M.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, L.C.; McNeill, G.; Macdiarmid, J.I.; Masson, L.F.; Holmes, B.A. Dietary patterns of school-age children in Scotland: Association with socio-economic indicators, physical activity and obesity. Br. J. Nutr. 2010, 103, 319–334. [Google Scholar] [CrossRef] [Green Version]
- Vereecken, C.; Covents, M.; Maes, L. Comparison of a food frequency questionnaire with an online dietary assessment tool for assessing preschool children’s dietary intake. J. Hum. Nutr. Diet. 2010, 23, 502–510. [Google Scholar] [CrossRef]
- Xia, W.; Sun, C.; Zhang, L.; Zhang, X.; Wang, J.; Wang, H.; Wu, L. Reproducibility and relative validity of a food frequency questionnaire developed for female adolescents in Suihua, North China. PLoS ONE 2011, 6, e19656. [Google Scholar] [CrossRef] [Green Version]
- Azarias, H.G.D.A.; Marques-Rocha, J.L.; Miranda, A.E.D.S.; Dos Santos, L.C.; Gomes Domingos, A.L.; Hermsdorff, H.H.M.; Bressan, J.; Oliveira, F.L.P.D.; Leal, A.C.G.; Pimenta, A.M. Online Food Frequency Questionnaire From the Cohort of Universities of Minas Gerais (CUME Project, Brazil): Construction, Validity, and Reproducibility. Front Nutr. 2021, 8, 709915. [Google Scholar] [CrossRef]
- Burrows, T.; Goldman, S.; Rollo, M. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labelled water. Eur. J. Clin. Nutr. 2020, 74, 669–681. [Google Scholar] [CrossRef]
- Burrows, T.L.; Martin, R.J.; Collins, C.E. A Systematic Review of the Validity of Dietary Assessment Methods in Children when Compared with the Method of Doubly Labeled Water. J. Am. Diet. Assoc. 2010, 110, 1501–1510. [Google Scholar] [CrossRef]
- Sailer, M.; Elizondo, G.; Martin, J.; Harding, C.O.; Gillingham, M.B. Nutrient intake, body composition, and blood phenylalanine control in children with phenylketonuria compared to healthy controls. Mol. Genet. Metab. Rep. 2020, 23, 100599. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Daly, A.; Wildgoose, J.; Cochrane, B.; Chahal, S.; Ashmore, C.; Loveridge, N.; MacDonald, A. Growth, Protein and Energy Intake in Children with PKU Taking a Weaning Protein Substitute in the First Two Years of Life: A Case-Control Study. Nutrients 2019, 11, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, H.J.; White, F.; MacDonald, A.; Rutherford, P.J.; Favre, E. Fat intakes of children with PKU on low phenylalanine diets. J. Hum. Nutr. Diet. 2005, 18, 395–400. [Google Scholar] [CrossRef]
- Viau, K.S.; Jones, J.L.; Murtaugh, M.A.; Gren, L.H.; Stanford, J.B.; Bilder, D.A. Phone-based motivational interviewing to increase self-efficacy in individuals with phenylketonuria. Mol. Genet. Metab. Rep. 2016, 6, 27–33. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PKU | CONTROL | |||||||
|---|---|---|---|---|---|---|---|---|
| FFQ 1 n = 50 | FFQ 2 n = 50 | 24-h Dietary Recalls ** n = 50 | p Value | FFQ 1 n = 50 | FFQ 2 n = 50 | 24-h Dietary Recalls ** n = 50 | p Value | |
| Median no. meals eaten/day | 5 | 4 | 5 | 0.01 # | 5 | 5 | 5 | 0.37 # |
| % eating breakfast (n) | 92 (46) | 94 (47) | 100 (50) | 1 * | 100 (50) | 100 (50) | 100 (50) | 1 * |
| % eating midday meal (n) | 100 (50) | 98 (49) | 100 (50) | 1 * | 100 (50) | 100 (50) | 100 (50) | 1 * |
| % eating evening meal (n) | 100 (50) | 100 (50) | 100 (50) | 1 * | 100 (50) | 100 (50) | 100 (50) | 1 * |
| % eating mid-morning snack (n) | 62 (31) | 38 (19) | 48 (24) | 0.027 * | 78 (39) | 74 (37) | 60 (30) | 0.815 * |
| % eating afternoon snack (n) | 70 (35) | 52 (26) | 70 (35) | 0.100 * | 55 (28) | 62 (31) | 74 (37) | 0.685 * |
| % eating bedtime snack (n) | 40 (20) | 46 (23) | 52 (26) | 0.686 * | 46 (23) | 54 (27) | 58 (29) | 0.549 * |
| % miss meals 1 x/week (n) | 10 (5) | 6 (3) | 8 (4) | 0.715 * | 10 (5) | 8 (4) | 8 (4) | 1 * |
| % miss meals > 1 x/week (n) | 12 (6) | 8 (4) | 2 (1) | 0.741 * | 2 (1) | 0 (0) | 0 (0) | 1 * |
| FFQ 1 n = 50 | FFQ 2 n = 50 | 24-h Dietary Recalls ** n = 50 | p Value | |
|---|---|---|---|---|
| Median no. 1 g natural protein (50 mg phenylalanine) exchanges/day (range) | 5.5 (3–25) | 5.5 (3–25) | 5.0 (2–23.5) | 0.02 # |
| % eating prescribed protein exchanges at every meal (n) | 62 (31) | 60 (30) | 66 (33) | 1 * |
| % actually eating prescribed protein exchanges at every main meal (n) | 74 (37) | 60 (30) | 46 (23) | 0.202 * |
| Median no. meals/snacks per day that prescribed protein exchanges are consumed (range) | 3 (1–6) | 3 (1–6) | 3 (1–5) | 1 * |
| % eating prescribed protein exchanges at breakfast (n) | 78 (39) | 72 (36) | 68 (34) | 0.645 * |
| % eating prescribed protein exchanges at midday meal (n) | 94 (47) | 86 (43) | 88 (44) | 0.318 * |
| % eating prescribed protein exchanges at evening meal (n) | 96 (48) | 100 (50) | 82 (41) | 0.495 * |
| % eating prescribed protein exchanges at mid-morning snack (n) | 4 (2) | 2 (1) | 4 (2) | 1 * |
| % eating prescribed protein exchanges at mid-afternoon snack (n) | 14 (7) | 14 (7) | 14 (7) | 1 * |
| % eating prescribed protein exchanges at bedtime snack (n) | 10 (5) | 4 (2) | 20 (10) | 0.436 * |
| Median no. times/day protein substitute dose taken (range) | 3 (3–5) | 3 (3–5) | 3 (3–5) | 1 * |
| % taking protein substitute dose at breakfast (n) | 100 (50) | 100 (50) | 100 (50) | 1 * |
| % taking protein substitute dose at midday meal (n) | 78 (39) | 72 (36) | 78 (39) | 0.645 * |
| % taking protein substitute dose at evening meal (n) | 74 (37) | 68 (34) | 62 (31) | 0.660 * |
| % taking protein substitute with morning snack (n) | 10 (5) | 12 (6) | 10 (5) | 1 * |
| % taking protein substitute with afternoon snack (n) | 36 (18) | 34 (17) | 26 (13) | 1 * |
| % taking protein substitute with bedtime snack (n) | 48 (24) | 56 (28) | 66 (33) | 0.548 * |
| PKU | CONTROL | Spearman Rank Correlation (r) | Wilcoxon Signed Rank (p value) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FFQ 1 | FFQ 2 | FFQ Average | Diet Recalls | FFQ 1 | FFQ 2 | FFQ Average | Diet Recalls | PKU FFQ 1 vs. 2 | PKU FFQ vs. DR | Ctrl FFQ 1 vs. 2 | Ctrl FFQ vs. DR | PKU FFQ 1 vs. 2 | PKU FFQ vs. DR | Ctrl FFQ 1 vs. 2 | Ctrl FFQ vs. DR | PKU FFQ vs. Ctrl FFQ | ||
| KJ/day | median | 8116.8 | 8591.1 | 8259.7 | 7851.8 | 7011.7 | 6779.4 | 7144.2 | 7163.0 | 0.723 | 0.500 | 0.633 | 0.334 | 0.19 | 0.005 | 0.10 | 0.57 | <0.0001 |
| (IQR) | (7078–11,288) | (6824–9446) | (7312–10,064) | (6806–8927) | (6008–8678) | (6274–7804) | (6157–8216) | (6318–7878) | ||||||||||
| CHO g/day | median | 277.3 | 293.7 | 287.8 | 267.1 | 226.9 | 215.4 | 221.0 | 208.0 | 0.682 | 0.601 | 0.651 | 0.408 | 0.62 | 0.01 | 0.17 | 0.02 | <0.0001 |
| (IQR) | (229–394) | (237–343) | (241–356) | (231–315) | (191–271) | (194–247) | (186–262) | (183–233) | ||||||||||
| Sugars g/day | median | 135.7 | 128.8 | 131.2 | 107.0 | 112.2 | 111.6 | 115.7 | 95.7 | 0.78 | 0.464 | 0.719 | 0.550 | 0.78 | 0.0001 | 0.38 | <0.0001 | 0.01 |
| (IQR) | (105–172) | (103–173) | (108–178) | (92–134) | (92–138) | (97–130) | (94–135) | (77–108) | ||||||||||
| Starch g/day | median | 136.3 | 146.8 | 144.2 | 140.5 | 102.8 | 96.7 | 100.1 | 116.8 | 0.731 | 0.600 | 0.742 | 0.493 | 0.51 | 0.25 | 0.05 | 0.004 | <0.0001 |
| (IQR) | (114–183) | (105–187) | (114–195) | (117–167) | (81–132) | (79–115) | (82–124) | (93–133) | ||||||||||
| Fat g/day | median | 57.4 | 55.7 | 58.2 | 52.0 | 61.1 | 59.4 | 60.7 | 65.7 | 0.691 | 0.271 | 0.614 | 0.381 | 0.07 | 0.04 | 0.11 | 0.11 | 0.23 |
| (IQR) | (49–76) | (48–68) | (49–69) | (43–61) | (54–77) | (54–69) | (54–73) | (57–75) | ||||||||||
| Total protein equivalent g/day | median | 72.9 | 73.2 | 72.6 | 71.8 | 66.7 | 63.4 | 65.6 | 64.6 | 0.913 | 0.848 | 0.523 | 0.344 | 0.37 | 0.08 | 0.04 | 0.91 | 0.0009 |
| (IQR) | (65–84) | (66–82) | (65–83) | (68–80) | (55–77) | (55–73) | (57–74) | (56–76) | ||||||||||
| Fibre g/day | median | 20.4 | 22.6 | 21.5 | 18.1 | 18.0 | 17.4 | 17.8 | 17.0 | 0.673 | 0.445 | 0.514 | 0.427 | 0.70 | 0.001 | 0.26 | 0.02 | 0.0005 |
| (IQR) | (16–27) | (18–25) | (19–26) | (14–22) | (15–33) | (15–20) | (15–21) | (14–20) | ||||||||||
| % Energy CHO | median | 58.8 | 58.6 | 59.3 | 59.0 | 51.3 | 51.1 | 50.7 | 49.0 | 0.768 | 0.689 | 0.492 | 0.414 | 0.35 | 0.94 | 0.85 | 0.02 | <0.0001 |
| (IQR) | (55–62) | (55–61) | (56–62) | (55–64) | (48–54) | (48–53) | (49–53) | (47–52) | ||||||||||
| % Energy Fat | median | 26.6 | 25.4 | 26.1 | 25.1 | 33.1 | 33.6 | 33.3 | 35.7 | 0.628 | 0.333 | 0.422 | 0.402 | 0.04 | 0.44 | 0.56 | 0.005 | <0.0001 |
| (IQR) | (23–29) | (23–29) | (24–29) | (22–29) | (31–36) | (32–35) | (32–35) | (32–37) | ||||||||||
| % Energy Protein | median | 14.5 | 15.4 | 14.3 | 15.3 | 15.4 | 15.5 | 15.5 | 15.2 | 0.777 | 0.729 | 0.622 | 0.290 | 0.34 | 0.21 | 0.45 | 0.89 | 0.12 |
| (IQR) | (12–18) | (13–17) | (13–17) | (14–18) | (15–17) | (14–17) | (15–16) | (11–15) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, S.; Ashmore, C.; Daly, A.; Jackson, R.; Pinto, A.; MacDonald, A. Validation of a Low-protein Semi-Quantitative Food Frequency Questionnaire. Nutrients 2022, 14, 1595. https://doi.org/10.3390/nu14081595
Evans S, Ashmore C, Daly A, Jackson R, Pinto A, MacDonald A. Validation of a Low-protein Semi-Quantitative Food Frequency Questionnaire. Nutrients. 2022; 14(8):1595. https://doi.org/10.3390/nu14081595
Chicago/Turabian StyleEvans, Sharon, Catherine Ashmore, Anne Daly, Richard Jackson, Alex Pinto, and Anita MacDonald. 2022. "Validation of a Low-protein Semi-Quantitative Food Frequency Questionnaire" Nutrients 14, no. 8: 1595. https://doi.org/10.3390/nu14081595
APA StyleEvans, S., Ashmore, C., Daly, A., Jackson, R., Pinto, A., & MacDonald, A. (2022). Validation of a Low-protein Semi-Quantitative Food Frequency Questionnaire. Nutrients, 14(8), 1595. https://doi.org/10.3390/nu14081595