
Health-Promoting Behaviors among Older Adults with Noncommunicable Diseases in Rural and Urban Areas during the New Normal Post-COVID-19 Era: A Structural Equation Modeling Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Setting and Participants
2.3. Research Instruments
2.4. Data Collection
2.5. Data Analyses
3. Results
3.1. Characteristics of Participants
3.2. Perceived Self-Efficacy, Health Literacy, Access to COVID-19 Preventive Material, Social Networks, and Health-Promoting Behaviors among Urban and Rural Older Adults with NCDs
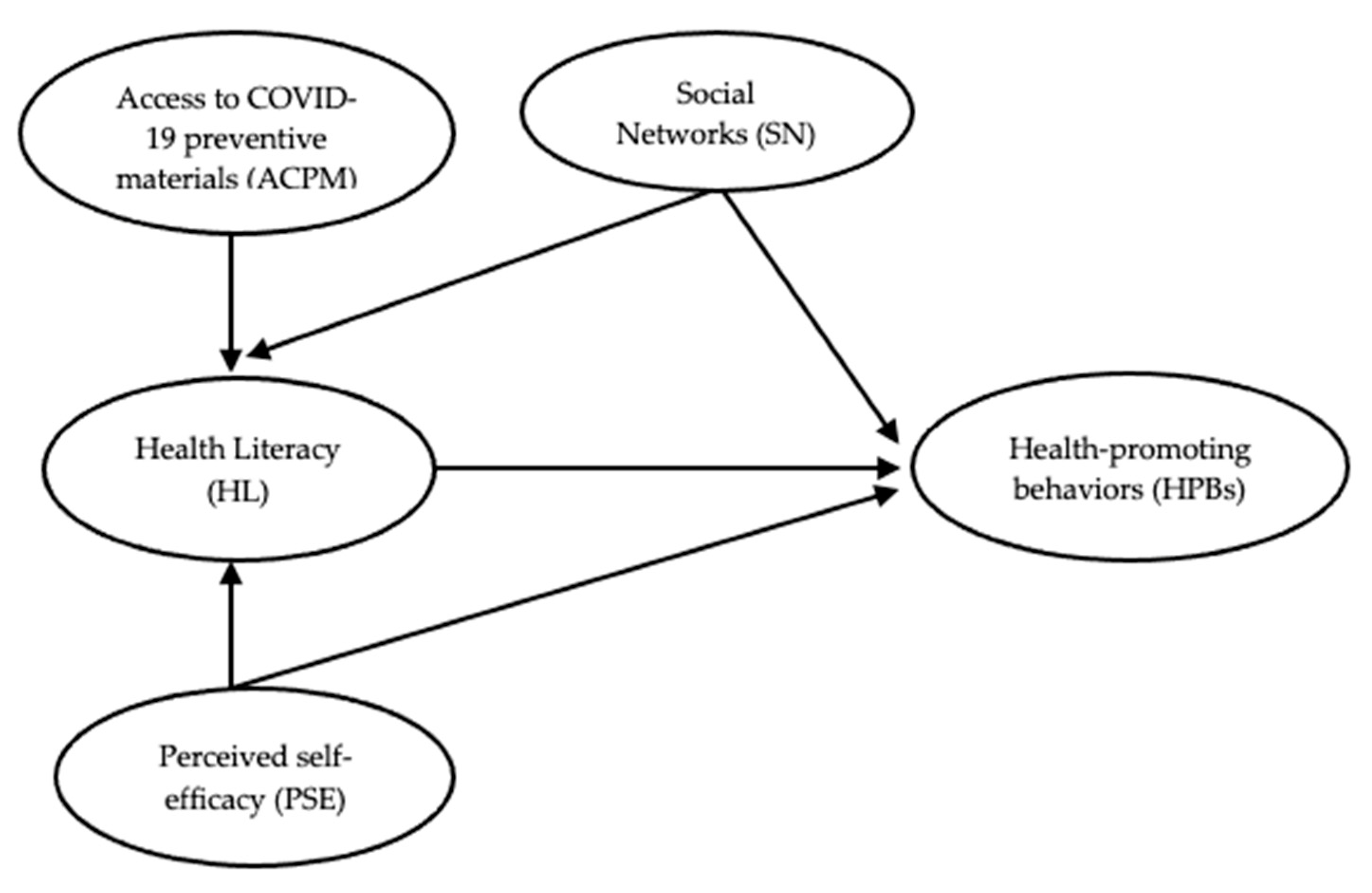
3.3. Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batista, C.; Shoham, S.; Ergonul, O.; Hotez, P.; Bottazzi, M.E.; Figueroa, J.P.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kang, G.; et al. Urgent needs to accelerate the race for COVID-19 therapeutics. EClinicalMedicine 2021, 36, 100911. [Google Scholar] [CrossRef] [PubMed]
- Bok, K.; Sitar, S.; Graham, B.S.; Mascola, J.R. Accelerated COVID-19 vaccine development: Milestones, lessons, and prospects. Immunity 2021, 54, 1636–1651. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Al-Thani, H.; El-Menyar, A. The emergence of new SARS-CoV-2 variant (Omicron) and increasing calls for COVID-19 vaccine boosters-The debate continues. Travel Med. Infect. Dis. 2022, 45, 102246. [Google Scholar] [CrossRef] [PubMed]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Fémy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected with Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 December 2022).
- Ruengorn, C.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T.; Thavorn, K.; Nochaiwong, S. Psychological Resilience and Adverse Mental Health Issues in the Thai Population during the Coronavirus Disease 2019 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13023. [Google Scholar] [CrossRef]
- Lu, G.; Zhang, Y.; Zhang, H.; Ai, J.; He, L.; Yuan, X.; Bao, S.; Chen, X.; Wang, H.; Cai, J.; et al. Geriatric risk and protective factors for serious COVID-19 outcomes among older adults in Shanghai Omicron wave. Emerg. Microbes Infect. 2022, 11, 2045–2054. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 8 December 2022).
- Kitchanapaibul, S.; Udplong, A.; Apidechkul, T.; Tamornpark, R.; Mulikaburt, T.; Srichan, P.; Suratana, S.; Yeemard, F.; Wongnuch, P. Experiences and expectations regarding COVID-19 prevention and control measures among the hill tribe population of northern Thailand: A qualitative study. BMC Public Health 2021, 21, 1060. [Google Scholar] [CrossRef]
- Daly, J.R.; Depp, C.; Graham, S.A.; Jeste, D.V.; Kim, H.-C.; Lee, E.E.; Nebeker, C. Health Impacts of the Stay-at-Home Order on Community-Dwelling Older Adults and How Technologies May Help: Focus Group Study. JMIR Aging 2021, 4, e25779. [Google Scholar] [CrossRef]
- Chantakeeree, C.; Sormunen, M.; Jullamate, P.; Turunen, H. Health-promoting Behaviors among Urban and Rural Older Thai Adults with Hypertension: A Cross-sectional Study. Pac. Rim Int. J. Nurs. Res. 2021, 25, 242–254. [Google Scholar]
- Pender, N.J.; Murdaugh, C.L.; Parsons, M.A. Health Promotion in Nursing Practice, 7th ed.; Pearson: Columbia, SC, USA, 2015. [Google Scholar]
- Zhu, D.; Ozaki, A.; Virani, S.S. Disease-Specific Excess Mortality during the COVID-19 Pandemic: An Analysis of Weekly US Death Data for 2020. Am. J. Public Health 2021, 111, 1518–1522. [Google Scholar] [CrossRef] [PubMed]
- Pothisiri, W.; Vicerra, P.M.M.; Buathong, T. Poverty, noncommunicable diseases, and perceived health risks among older adults during the COVID-19 pandemic in urban Thailand. Asian Soc. Work. Policy Rev. 2022, 16, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Cheng, Z.; Howard, V.J.; Judd, S.E.; Blair, S.N.; Sun, Y.; Hooker, S.P. Is adiposity associated with objectively measured physical activity and sedentary behaviors in older adults? BMC Geriatr. 2020, 20, 257. [Google Scholar] [CrossRef] [PubMed]
- Yusefi, A.R.; Barfar, E.; Daneshi, S.; Bayati, M.; Mehralian, G.; Bastani, P. Health literacy and health promoting behaviors among inpatient women during COVID-19 pandemic. BMC Women’s Health 2022, 22, 77. [Google Scholar] [CrossRef] [PubMed]
- Wungrath, J.; Autorn, N. Factors Influencing Health Promotion Behaviors and Prevention of COVID-19 among Elderly during the Second Wave of Pandemic in Chiang Mai, Thailand. Ann. Rom. Soc. Cell Biol. 2021, 25, 1702–1715. [Google Scholar]
- Posai, V.; Suksatan, W.; Choompunuch, B.; Koontalay, A.; Ounprasertsuk, J.; Sadang, J.M. Assessment of the Health-Promoting Behaviors of Hospitalized Patients with Non-Communicable Diseases during the Second Wave of COVID-19. J. Multidiscip. Healthc. 2021, 14, 2185–2194. [Google Scholar] [CrossRef]
- Yodmai, K.; Pechrapa, K.; Kittipichai, W.; Charupoonpol, P.; Suksatan, W. Factors Associated with Good COVID-19 Preventive Behaviors among Older Adults in Urban Communities in Thailand. J. Prim. Care Community Health 2021, 12, 21501327211036251. [Google Scholar] [CrossRef]
- Lee, M.K.; Oh, J. Health-Related Quality of Life in Older Adults: Its Association with Health Literacy, Self-Efficacy, Social Support, and Health-Promoting Behavior. Healthcare 2020, 8, 407. [Google Scholar] [CrossRef]
- Foundation of Thai Gerontology Research and Development Institute. Situation of the Thai Older Persons 2020; Institute for Population and Social Research, Mahidol University: Nakhon Pathom, Thailand, 2021. [Google Scholar]
- National Statistical Office. Reporting to a Study of Guidelines for Defining Urban and Rural Areas in Thailand. Available online: http://statstd.nso.go.th/download.aspx (accessed on 6 December 2022).
- Jackson, D.L. Sample Size and Number of Parameter Estimates in Maximum Likelihood Confirmatory Factor Analysis: A Monte Carlo Investigation. Struct. Equ. Model. A Multidiscip. J. 2001, 8, 205–223. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Health Education Division. Health Literacy and Health-Promoting Behavior Assessment Tools for the Village to Change Health Behavior. Available online: http://www.hed.go.th/linkHed/424 (accessed on 10 December 2021).
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an Abbreviated Version of the Lubben Social Network Scale among Three European Community-Dwelling Older Adult Populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, H.; Stuifbergen, A.; Oh, H.S.; Hall, S. Self-rated abilities for health practices: A health self-efficacy measure. J. Health Behav. Educ. Promot. 1993, 17, 42–50. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Publications: New York, NY, USA, 2005. [Google Scholar]
- Giena, V.P.; Thongpat, S.; Nitirat, P. Predictors of health-promoting behaviour among older adults with hypertension in Indonesia. Int. J. Nurs. Sci. 2018, 5, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Mszar, R.; Buscher, S.; McCann, D.; Taylor, H.L. Self-Efficacy, Perceived Barriers to Care, and Health-Promoting Behaviors among Franco-Americans across Cardiovascular Risk Factors: A Cross-Sectional Study. Am. J. Health Promot. 2020, 35, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. New Developments in Goal Setting and Task Performance; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Tan, F.C.J.H.; Oka, P.; Dambha-Miller, H.; Tan, N.C. The association between self-efficacy and self-care in essential hypertension: A systematic review. BMC Fam. Pract. 2021, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- DDo, B.N.; Nguyen, P.-A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of Health Literacy and Its Associations with Health-Related Behaviors, Depression among the Older People with and without Suspected COVID-19 Symptoms: A Multi-Institutional Study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D. Defining and measuring health literacy: What can we learn from literacy studies? Int. J. Public Health 2009, 54, 303. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Song, Y.; Park, J.; Utz, S. Patients’ Experiences of Diabetes Self-Management Education according to Health-Literacy Levels. Clin. Nurs. Res. 2020, 29, 285–292. [Google Scholar] [CrossRef]
- Ueno, H.; Ishikawa, H.; Suzuki, R.; Izumida, Y.; Ohashi, Y.; Yamauchi, T.; Kadowaki, T.; Kiuchi, T. The association between health literacy levels and patient-reported outcomes in Japanese type 2 diabetic patients. SAGE Open Med. 2019, 7, 2050312119865647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechrapa, K.; Yodmai, K.; Kittipichai, W.; Charupoonpol, P.; Suksatan, W. Health Literacy among Older Adults during COVID-19 Pandemic: A Cross-Sectional Study in an Urban Community in Thailand. Ann. Geriatr. Med. Res. 2021, 25, 309–317. [Google Scholar] [CrossRef] [PubMed]
- National Statistical Office of Thailand. Summary Survey of Household Socio-Economic Conditions in the First 6 Months of 2021. Available online: http://www.nso.go.th/sites/2014en/Survey/social/household/household/2021/pocketbookSES_64.pdf (accessed on 7 December 2022).
- Bukhman, G.; Mocumbi, A.O.; Atun, R.; Becker, A.E.; Bhutta, Z.; Binagwaho, A.; Clinton, C.; Coates, M.M.; Dain, K.; Ezzati, M.; et al. The Lancet NCDI Poverty Commission: Bridging a gap in universal health coverage for the poorest billion. Lancet 2020, 396, 991–1044. [Google Scholar] [CrossRef] [PubMed]
- Pizzi, M.A.; Richards, L.G. Promoting Health, Well-Being, and Quality of Life in Occupational Therapy: A Commitment to a Paradigm Shift for the Next 100 Years. Am. J. Occup. Ther. 2017, 71, 7104170010p1–7104170010p5. [Google Scholar] [CrossRef] [PubMed]
- Suksatan, W.; Teravecharoenchai, S.; Sarayuthpitak, J. Factors Associated with a Health-promoting Lifestyle among Adults and Older Adults in the Era of COVID-19: An Integrative Review. Open Access Maced. J. Med. Sci. 2022, 10, 725–732. [Google Scholar] [CrossRef]
- Oh, J. Factors affecting health promoting behavior among older women in Korea: A structural equation model. Health Promot. Int. 2021, 36, 924–932. [Google Scholar] [CrossRef]
- Allahverdipour, H.; Karimzadeh, Z.; Alizadeh, N.; Asghari Jafarabadi, M.; Javadivala, Z. Psychological well-being and happiness among Middle-aged women: A cross-sectional study. Health Care Women Int. 2021, 42, 28–42. [Google Scholar] [CrossRef]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Chang, Q.; Chan, C.H.; Yip, P.S.F. A meta-analytic review on social relationships and suicidal ideation among older adults. Soc. Sci. Med. 2017, 191, 65–76. [Google Scholar] [CrossRef]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Haro, J.M. The association of relationship quality and social networks with depression, anxiety, and suicidal ideation among older married adults: Findings from a cross-sectional analysis of the Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2015, 179, 134–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Health-Promoting Behaviors | p-Value | ||
|---|---|---|---|---|
| Urban (n = 125) | Rural (n = 125) | Total (n = 250) | ||
| n (%) | n (%) | n (%) | ||
| Sex | ||||
| Female | 92 (73.60) | 67 (53.60) | 159 (63.60) | 0.446 |
| Age (years): Mean ± SD | 70.59 ± 7.44 | 68.63 ± 7.41 | 69.61 ± 7.47 | 0.018 |
| 60–69 | 55 (44.00) | 77 (61.60) | 132 (52.80) | |
| 70–79 | 54 (43.20) | 34 (27.20) | 88 (35.20) | |
| >80 | 16 (12.80) | 14 (11.20) | 30 (12.00) | |
| Monthly income (US dollars): Mean ± SD | 193.58 ± 321.05 | 70.69 ± 64.91 | 132.14 ± 239.20 | 0.026 |
| <143 | 92 (73.60) | 115 (92.00) | 207 (82.80) | |
| 144–286 | 10 (8.00) | 10 (8.00) | 20 (8.00) | |
| 286–429 | 6 (4.80) | 0 (0.00) | 6 (2.40) | |
| >430 | 17 (13.60) | 0 (0.00) | 17 (6.80) | |
| Type of NCDs (Yes) * | 0.176 | |||
| Heart disease | 9 (7.20) | 11 (8.80) | 20 (8.00) | |
| Vascular disease | 15 (12.00) | 8 (6.40) | 23 (9.20) | |
| Diabetes | 67 (53.60) | 46 (36.80) | 113 (45.20) | |
| Hypertension | 82 (65.60) | 82 (65.60) | 164 (65.60) | |
| Cancer | 1 (0.80) | 1 (0.80) | 2 (0.80) | |
| Chronic obstructive pulmonary disease | 0 (0.00) | 3 (2.40) | 3 (1.20) | |
| Obesity | 9 (7.20) | 2 (16.0) | 11 (4.40) | |
| Variables | Interpretation | Urban (n = 125) | Rural (n = 125) | Total (n = 250) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| Perceived self-efficacy (PSE) | High | 80.54 | 17.7 | 72.42 | 16.50 | 76.48 | 17.55 | <0.001 | |
| Nutrition self-efficacy | High | 21.09 | 4.92 | 19.67 | 4.17 | 20.38 | 4.61 | 0.014 | |
| Stress management self-efficacy | High | 20.12 | 4.24 | 17.93 | 4.28 | 19.02 | 4.39 | <0.001 | |
| Exercise self-efficacy | Fair | 18.55 | 5.63 | 15.12 | 5.87 | 16.83 | 5.99 | <0.001 | |
| Health practice self-efficacy | High | 20.77 | 4.47 | 19.69 | 4.70 | 20.23 | 4.61 | 0.064 | |
| Health literacy (HL) | Good | 37.50 | 6.78 | 37.06 | 5.94 | 37.28 | 6.37 | 0.586 | |
| Access to COVID-19 preventive material (ACPM) | Good | 4.46 | 0.92 | 3.08 | 1.30 | 4.14 | 1.18 | <0.001 | |
| Social networks | More social engagement | 15.16 | 5.93 | 14.99 | 5.24 | 15.08 | 5.59 | 0.813 | |
| Health-promoting behaviors (HPBs) | Good | 68.13 | 7.16 | 66.73 | 7.81 | 67.44 | 7.51 | 0.141 | |
| Nutrition | Good | 18.91 | 2.79 | 18.28 | 2.97 | 18.59 | 2.89 | 0.084 | |
| Exercise | Fair | 6.11 | 2.12 | 6.08 | 1.84 | 6.09 | 1.98 | 0.899 | |
| Smoking | Very Good | 9.19 | 1.77 | 8.69 | 1.94 | 8.94 | 1.87 | 0.036 | |
| Alcohol drinking | Very Good | 4.61 | 0.90 | 4.53 | 0.98 | 4.57 | 0.94 | 0.505 | |
| Stress management | Fair | 5.23 | 1.04 | 5.78 | 1.28 | 5.50 | 1.19 | <0.001 | |
| Rational drug use | Very Good | 9.89 | 1.85 | 9.67 | 2.21 | 9.78 | 2.04 | 0.387 | |
| Preventive COVID-19 infection | Very Good | 14.17 | 1.67 | 13.68 | 1.57 | 13.93 | 1.64 | 0.019 | |
| Dependent Variables | R2 | Effects | Independent Variables | |||
|---|---|---|---|---|---|---|
| ACPM | PSE | SN | HL | |||
| HL | 0.72 | DE | −0.03 * (−0.85) | 0.81 *** (13.41) | 0.11 * (2.14) | – |
| IE | – | – | – | – | ||
| TE | −0.03 * (−0.85) | 0.81 *** (13.41) | 0.11 * (2.14) | – | ||
| HPBs | 0.81 | DE | 0.24 *** (3.55) | 0.40 *** (4.32) | 0.01 * (0.91) | 0.19 ** (2.36) |
| IE | −0.01 * (−0.09) | 0.15 ** (1.61) | 0.02 * (0.39) | – | ||
| TE | 0.23 *** (3.46) | 0.55 *** (5.92) | 0.03 * (0.51) | 0.19 ** (2.36) | ||
| χ2 = 71.936, df = 58, p-value = 0.103, χ2/df = 1.240; RMSEA = 0.031; SRMR = 0.042; GFI = 0.964; NFI = 0.964; CFI = 0.993 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suksatan, W.; Teravecharoenchai, S.; Sarayuthpitak, J. Health-Promoting Behaviors among Older Adults with Noncommunicable Diseases in Rural and Urban Areas during the New Normal Post-COVID-19 Era: A Structural Equation Modeling Analysis. Nutrients 2023, 15, 101. https://doi.org/10.3390/nu15010101
Suksatan W, Teravecharoenchai S, Sarayuthpitak J. Health-Promoting Behaviors among Older Adults with Noncommunicable Diseases in Rural and Urban Areas during the New Normal Post-COVID-19 Era: A Structural Equation Modeling Analysis. Nutrients. 2023; 15(1):101. https://doi.org/10.3390/nu15010101
Chicago/Turabian StyleSuksatan, Wanich, Supat Teravecharoenchai, and Jintana Sarayuthpitak. 2023. "Health-Promoting Behaviors among Older Adults with Noncommunicable Diseases in Rural and Urban Areas during the New Normal Post-COVID-19 Era: A Structural Equation Modeling Analysis" Nutrients 15, no. 1: 101. https://doi.org/10.3390/nu15010101
APA StyleSuksatan, W., Teravecharoenchai, S., & Sarayuthpitak, J. (2023). Health-Promoting Behaviors among Older Adults with Noncommunicable Diseases in Rural and Urban Areas during the New Normal Post-COVID-19 Era: A Structural Equation Modeling Analysis. Nutrients, 15(1), 101. https://doi.org/10.3390/nu15010101