
Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease
 ,
,  , ,
, ,  , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Enrolment, Inclusion Criteria, and Data Collection
- -
- General: age, sex, smoking, comorbidities (diabetes and obesity);
- -
- Clinical history: type of IBD (CD, UC, IBD-U), year of diagnosis of IBD, topographical location, drug therapy taken (no therapy, topical or systemic steroid therapy, biological drug), comorbidity;
- -
- IBD clinical activity: remission, mild, moderate, and severe. Evaluated on the basis of two different scores, the Mayo Clinic Partial in patients with UC and the Harvey– Bradshaw Index in patients with CD;
- -
- Vitamin D data: dose of VD taken, level of 25-hydroxy (OH) VD in serum;
- -
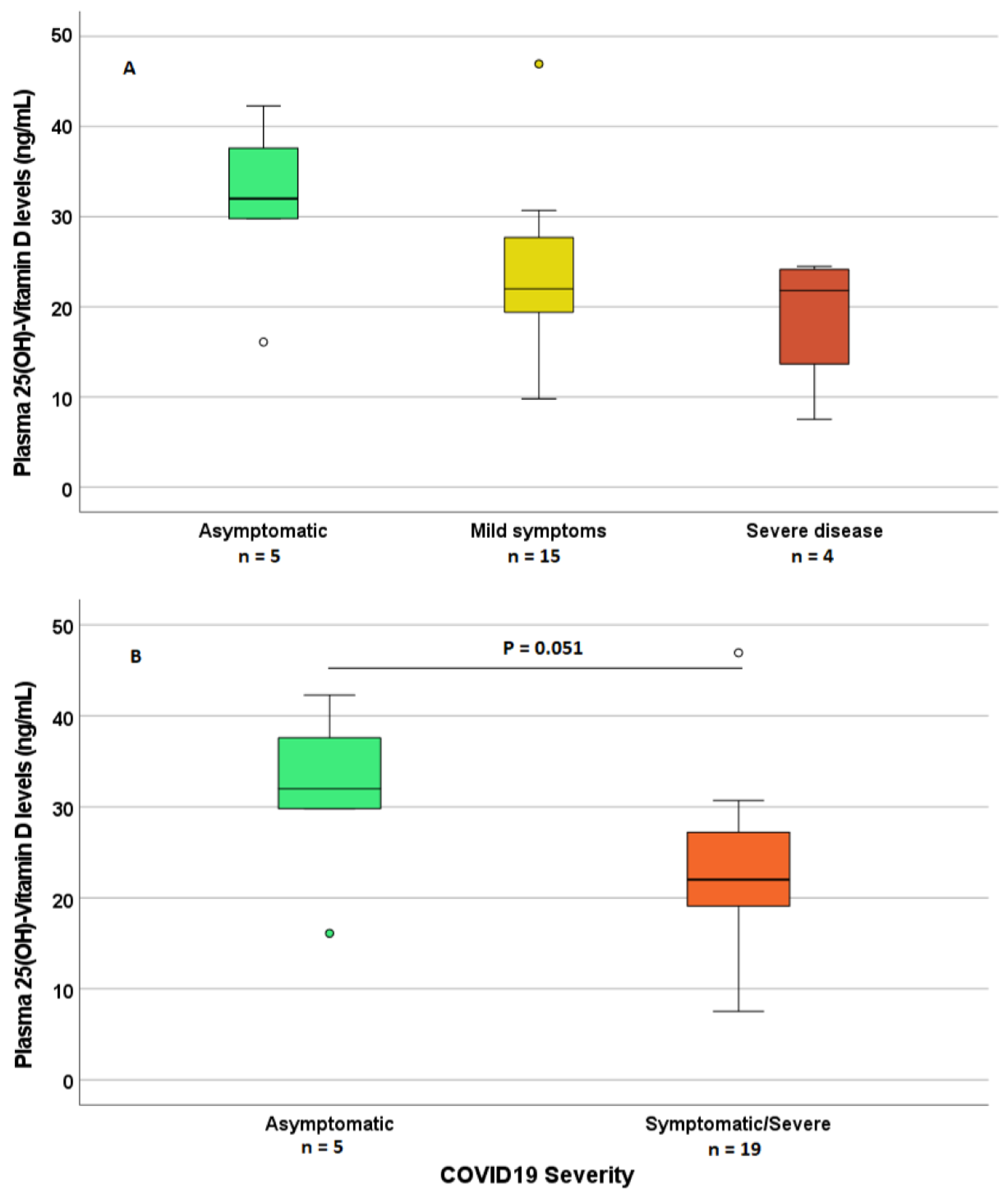
- COVID-19 data: serological evidence of previous SARS-CoV-2 infection (positive or negative SARS-CoV-2 IgG and anti-SARS-CoV-2 IgG dose), COVID-19 symptoms (fever, cough, dyspnea, diarrhea, vomiting, headache, anosmia, ageusia, pneumonia, hospitalization, ventilation, sequelae), type of therapy taken for COVID-19, any changes in therapy for IBD during infection. Patients with a doubtful anti-SARS-CoV-2 IgG level, having a positive history of virus infection, were considered positive. Severity on COVID-19 was divided into 3 groups: asymptomatic COVID-19 (absence of clinically appreciable symptoms), mild COVID-19 (at least 1 among cough, rhinitis, fever, anosmia/ageusia), and severe COVID-19 (patients with pneumonia/hospitalization).
2.2. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. General Patients’ Characteristics and COVID-19
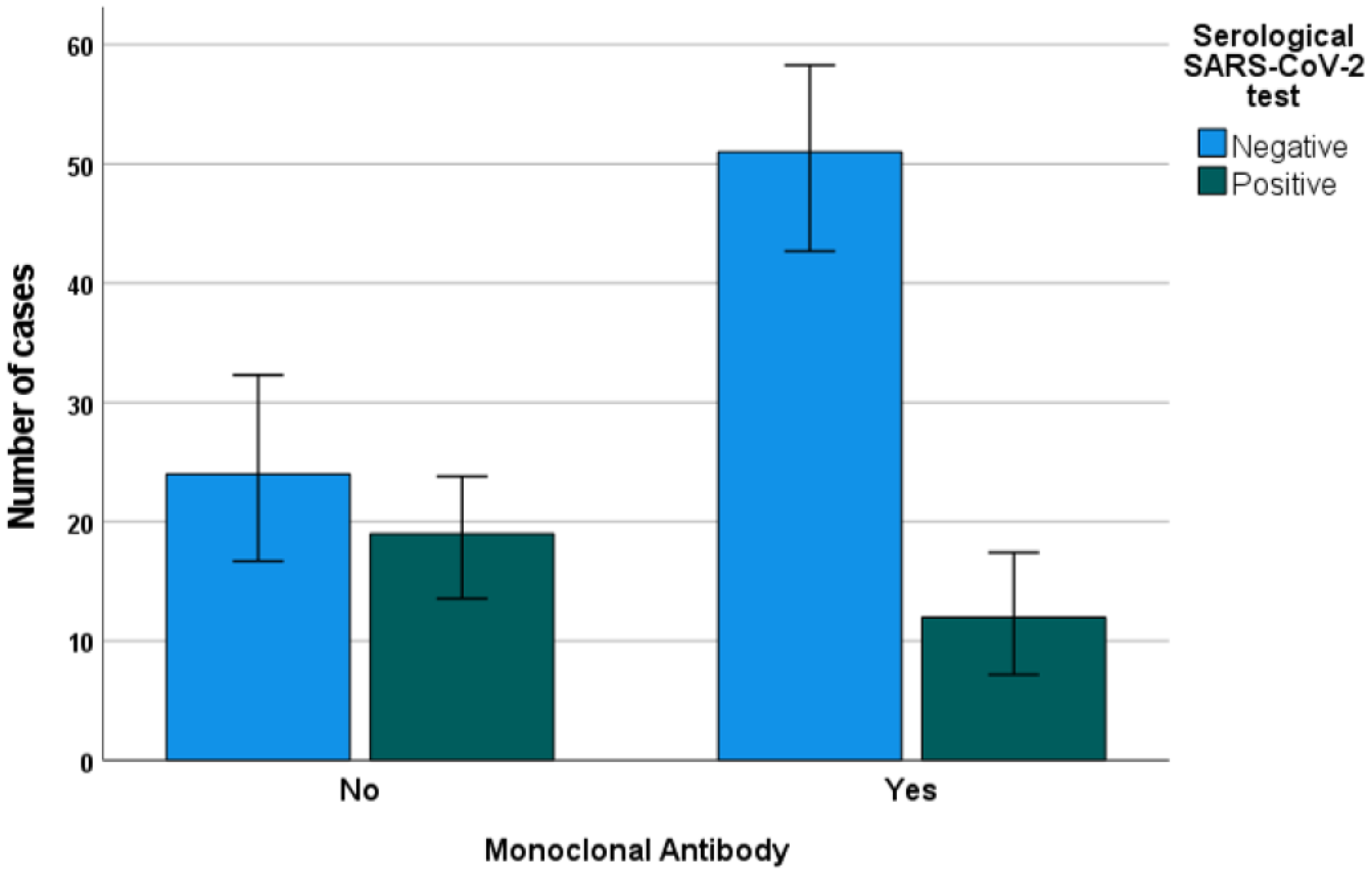
3.3. IBD Features, Treatment, and COVID-19
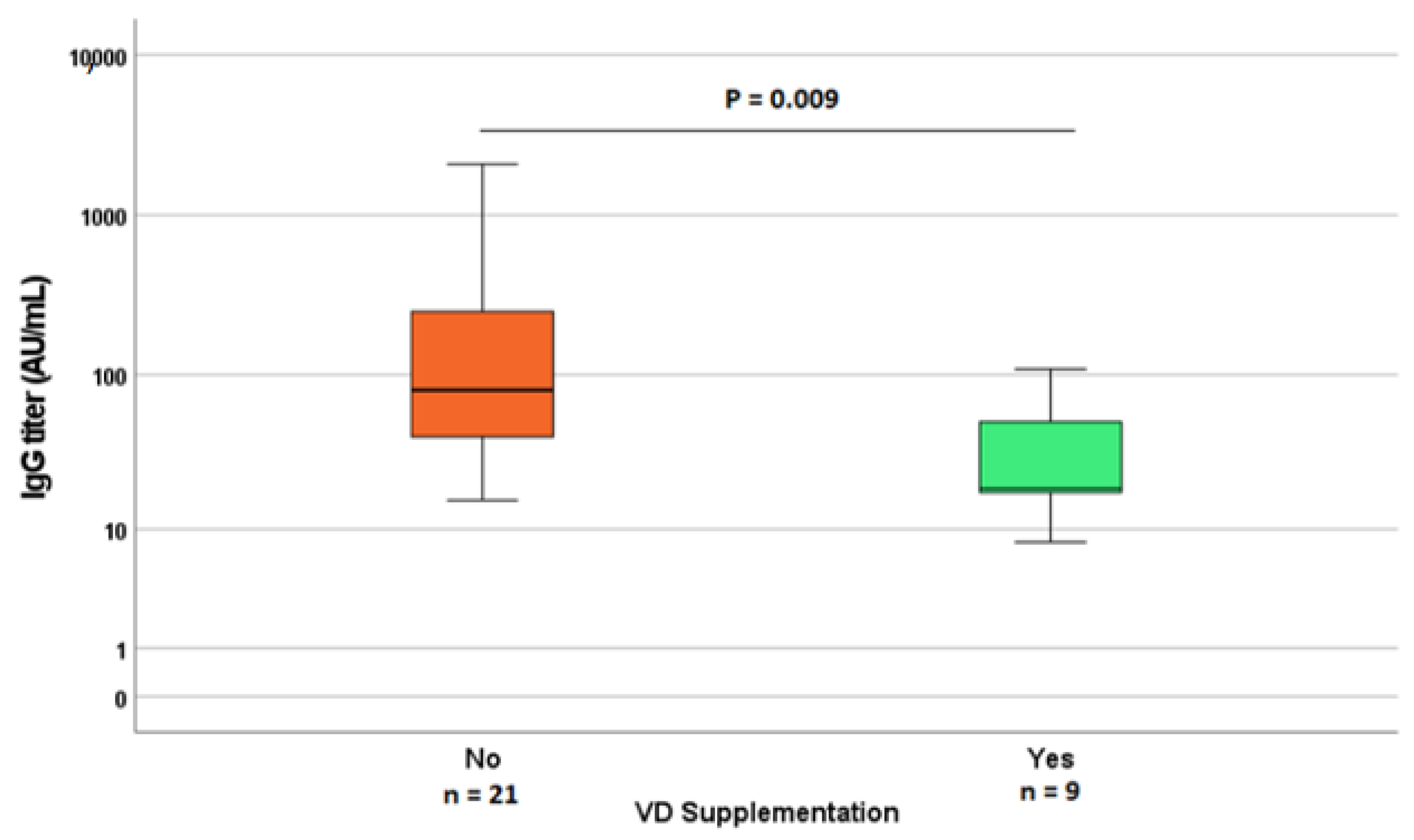
3.4. Vitamin D Concentration, Supplementation, IBD, and COVID-19
3.5. Predictors of COVID-19 Positivity/Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; Liu, D.; Deng, F. The Role of Vitamin D in Immune System and Inflammatory Bowel Disease. J. Inflamm. Res. 2022, 15, 3167–3185. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.L. Clinical presentations of inflammatory bowel disease: East meets West. J. Chin. Med. Assoc. 2017, 80, 51–52. [Google Scholar] [CrossRef] [Green Version]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Du, C.; Zhang, Y.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.; Lian, X.; Song, F.; Ma, H.; Lian, Z.; Liang, Y.; Qin, T.; Chen, W.; Wang, S. Clinical features of severe patients infected with 2019 novel coronavirus: A systematic review and meta-analysis. Ann. Transl. Med. 2020, 8, 576. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Hao, S.R.; Jia, H.Y.; Cai, H.; Zhang, X.L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.H.; Lui, R.N.; Sung, J.J. Covid-19 and the digestive system. J. Gastroenterol. Hepatol. 2020, 35, 744–748. [Google Scholar] [CrossRef]
- Neurath, M.F. COVID-19 and immunomodulation in IBD. Gut 2020, 69, 1335–1342. [Google Scholar] [CrossRef]
- Courbebaisse, M.; Cavalier, E. Vitamin D in 2020: An Old Pro-Hormone with Potential Effects beyond Mineral Metabolism. Nutrients 2020, 12, 3378. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Boglione, L.; Cusato, J.; De Nicolo, A.; Cariti, G.; Di Perri, G.; D’Avolio, A. Role of CYP27B1+2838 promoter polymorphism in the treatment of chronic hepatitis B HBeAg negative with PEG-interferon. J. Viral Hepat. 2014, 22, 318–327. [Google Scholar] [CrossRef]
- Matheu, V.; Back, O.; Mondoc, E.; Issazadeh-Navikas, S. Dual effects of vitamin D-induced alteration of TH1/TH2 cytokine expression: Enhancing IgE production and decreasing airway eosinophilia in murine allergic airway disease. J. Allergy Clin. Immunol. 2003, 112, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Dipasquale, V.; Lo Presti, G.; Milani, G.P.; Corsello, A.; Agostoni, C.; Romano, C. Vitamin D in Prevention of Autoimmune Diseases. Front. Biosci. Landmark 2022, 27, 288. [Google Scholar] [CrossRef] [PubMed]
- Dragasevic, S.; Stankovic, B.; Kotur, N.; Milutinovic, A.S.; Milovanovic, T.; Stojkovic Lalosevic, M.; Stojanovic, M.; Pavlovic, S.; Popovic, D. Genetic Aspects of Micronutrients Important for Inflammatory Bowel Disease. Life 2022, 12, 1623. [Google Scholar] [CrossRef] [PubMed]
- Anbarcioglu, E.; Kirtiloglu, T.; Ozturk, A.; Kolbakir, F.; Acikgoz, G.; Colak, R. Vitamin D deficiency in patients with aggressive periodontitis. Oral Dis. 2018, 25, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Azrielant, S.; Shoenfeld, Y. Vitamin D and the Immune System. Isr. Med. Assoc. J. 2017, 19, 510–511. [Google Scholar]
- Zhang, H.L.; Wu, J. Role of vitamin D in immune responses and autoimmune diseases, with emphasis on its role in multiple sclerosis. Neurosci. Bull. 2010, 26, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Cusato, J.; Allegra, S.; Boglione, L.; De Nicolo, A.; Baietto, L.; Cariti, G.; Di Perri, G.; D’Avolio, A. Vitamin D pathway gene variants and HCV-2/3 therapy outcomes. Antivir. Ther. 2014, 20, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Arora, J.; Patel, D.R.; Nicol, M.J.; Field, C.J.; Restori, K.H.; Wang, J.; Froelich, N.E.; Katkere, B.; Terwilliger, J.A.; Weaver, V.; et al. Vitamin D and the Ability to Produce 1,25(OH)(2)D Are Critical for Protection from Viral Infection of the Lungs. Nutrients 2022, 14, 3061. [Google Scholar] [CrossRef]
- Arboleda, J.F.; Urcuqui-Inchima, S. Vitamin D Supplementation: A Potential Approach for Coronavirus/COVID-19 Therapeutics? Front. Immunol. 2020, 11, 1523. [Google Scholar] [CrossRef]
- Wang, C.; Wang, S.; Li, D.; Chen, P.; Han, S.; Zhao, G.; Chen, Y.; Zhao, J.; Xiong, J.; Qiu, J.; et al. Human Cathelicidin Inhibits SARS-CoV-2 Infection: Killing Two Birds with One Stone. ACS Infect. Dis. 2021, 7, 1545–1554. [Google Scholar] [CrossRef]
- Gallelli, L.; Mannino, G.C.; Luciani, F.; de Sire, A.; Mancuso, E.; Gangemi, P.; Cosco, L.; Monea, G.; Averta, C.; Minchella, P.; et al. Vitamin D Serum Levels in Subjects Tested for SARS-CoV-2: What Are the Differences among Acute, Healed, and Negative COVID-19 Patients? A Multicenter Real-Practice Study. Nutrients 2021, 13, 3932. [Google Scholar] [CrossRef] [PubMed]
- D’Avolio, A.; Avataneo, V.; Manca, A.; Cusato, J.; De Nicolo, A.; Lucchini, R.; Keller, F.; Cantu, M. 25-Hydroxyvitamin D Concentrations Are Lower in Patients with Positive PCR for SARS-CoV-2. Nutrients 2020, 12, 1359. [Google Scholar] [CrossRef] [PubMed]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics with COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef] [PubMed]
- Sanson, G.; De Nicolo, A.; Zerbato, V.; Segat, L.; Koncan, R.; Di Bella, S.; Cusato, J.; di Masi, A.; Palermo, A.; Caironi, P.; et al. A combined role for low vitamin D and low albumin circulating levels as strong predictors of worse outcome in COVID-19 patients. Ir. J. Med. Sci. 2022, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, J.B.; Norton, E.C.; McCullough, J.S.; Meltzer, D.O.; Lavigne, J.; Fiedler, V.C.; Gibbons, R.D. Association between vitamin D supplementation and COVID-19 infection and mortality. Sci. Rep. 2022, 12, 19397. [Google Scholar] [CrossRef]
- Martineau, A.R. Vitamin D in the prevention or treatment of COVID-19. Proc. Nutr. Soc. 2022, 1–18. [Google Scholar] [CrossRef]
- Martineau, A.R.; Cantorna, M.T. Vitamin D for COVID-19: Where are we now? Nat. Rev. Immunol. 2022, 22, 529–530. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohns Colitis 2018, 13, 144–164. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011.
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Kolls, J.K.; Garry, R.F. Role of the T cell vitamin D receptor in severe COVID-19. Nat. Immunol. 2021, 23, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Chauss, D.; Freiwald, T.; McGregor, R.; Yan, B.; Wang, L.; Nova-Lamperti, E.; Kumar, D.; Zhang, Z.; Teague, H.; West, E.E.; et al. Autocrine vitamin D signaling switches off pro-inflammatory programs of TH1 cells. Nat. Immunol. 2022, 23, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Dickie, L.J.; Church, L.D.; Coulthard, L.R.; Mathews, R.J.; Emery, P.; McDermott, M.F. Vitamin D3 down-regulates intracellular Toll-like receptor 9 expression and Toll-like receptor 9-induced IL-6 production in human monocytes. Rheumatology 2010, 49, 1466–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Leung, D.Y.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W.; Goleva, E. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. J. Immunol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, H.; Wu, H.; Li, H.; Liu, L.; Guo, J.; Li, C.; Shih, D.Q.; Zhang, X. Protective role of 1,25(OH)2 vitamin D3 in the mucosal injury and epithelial barrier disruption in DSS-induced acute colitis in mice. BMC Gastroenterol. 2012, 12, 57. [Google Scholar] [CrossRef] [Green Version]
- ISTAT. Primi risultati dell’indagine di sieroprevalenza sul SARS-CoV-2. Available online: https://www.istat.it/it/archivio/246156 (accessed on 24 September 2022).
- Vatn, M.H.; Sandvik, A.K. Inflammatory bowel disease. Scand. J. Gastroenterol. 2015, 50, 748–762. [Google Scholar] [CrossRef]
- Balestrieri, P.; Ribolsi, M.; Guarino, M.P.L.; Emerenziani, S.; Altomare, A.; Cicala, M. Nutritional Aspects in Inflammatory Bowel Diseases. Nutrients 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Calcagno, A.; Ghisetti, V.; Emanuele, T.; Trunfio, M.; Faraoni, S.; Boglione, L.; Burdino, E.; Audagnotto, S.; Lipani, F.; Nigra, M.; et al. Risk for SARS-CoV-2 Infection in Healthcare Workers, Turin, Italy. Emerg. Infect. Dis. 2020, 27, 303–305. [Google Scholar] [CrossRef]
- De Nicolò, A.; Avataneo, V.; Cusato, J.; Palermiti, A.; Mula, J.; De Vivo, E.; Antonucci, M.; Bonora, S.; Calcagno, A.; Di Perri, G.; et al. Analytical Validation and Clinical Application of Rapid Serological Tests for SARS-CoV-2 Suitable for Large-Scale Screening. Diagnostics 2021, 11, 869. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Stralin, K.; Gorin, J.B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168.e14. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Yue, S.; Xue, W. Increased risk for COVID-19 in patients with vitamin D deficiency. Nutrition 2021, 84, 111106. [Google Scholar] [CrossRef] [PubMed]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2020, 93, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Villasis-Keever, M.A.; Lopez-Alarcon, M.G.; Miranda-Novales, G.; Zurita-Cruz, J.N.; Barrada-Vazquez, A.S.; Gonzalez-Ibarra, J.; Martinez-Reyes, M.; Grajales-Muniz, C.; Santacruz-Tinoco, C.E.; Martinez-Miguel, B.; et al. Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial. Arch. Med. Res. 2022, 53, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcala Diaz, J.F.; Lopez Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Antonangelo, L.; Gualano, B.; Pereira, R.M.R. Effect of a Single High-Dose Vitamin D3 on the Length of Hospital Stay of Severely 25-Hydroxyvitamin D-Deficient Patients with COVID-19. Clinics 2021, 76, e3549. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef]
- Zurita-Cruz, J.; Fonseca-Tenorio, J.; Villasis-Keever, M.; Lopez-Alarcon, M.; Parra-Ortega, I.; Lopez-Martinez, B.; Miranda-Novales, G. Efficacy and safety of vitamin D supplementation in hospitalized COVID-19 pediatric patients: A randomized controlled trial. Front. Pediatr. 2022, 10, 943529. [Google Scholar] [CrossRef]
- Benskin, L.L. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Front. Public Health 2020, 8, 513. [Google Scholar] [CrossRef]
- Mehta, A.K.; Gracias, D.T.; Croft, M. TNF activity and T cells. Cytokine 2016, 101, 14–18. [Google Scholar] [CrossRef]
- Coperchini, F.; Ricci, G.; Croce, L.; Denegri, M.; Ruggiero, R.; Villani, L.; Magri, F.; Chiovato, L.; Rotondi, M. Modulation of ACE-2 mRNA by inflammatory cytokines in human thyroid cells: A pilot study. Endocrine 2021, 74, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Bezzio, C.; Saibeni, S.; Variola, A.; Allocca, M.; Massari, A.; Gerardi, V.; Casini, V.; Ricci, C.; Zingone, F.; Amato, A.; et al. Outcomes of COVID-19 in 79 patients with IBD in Italy: An IG-IBD study. Gut 2020, 69, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Bezzio, C.; Armuzzi, A.; Furfaro, F.; Ardizzone, S.; Milla, M.; Carparelli, S.; Orlando, A.; Caprioli, F.A.; Castiglione, F.; Vigano, C.; et al. Therapies for inflammatory bowel disease do not pose additional risks for adverse outcomes of SARS-CoV-2 infection: An IG-IBD study. Aliment. Pharmacol. Ther. 2021, 54, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Siew, C.; Hilmi, I.N.; Blake, A.; Bhayat, F.; Adsul, S.; Khan, Q.R.; Wu, D.C. Low Frequency of Opportunistic Infections in Patients Receiving Vedolizumab in Clinical Trials and Post-Marketing Setting. Inflamm. Bowel Dis. 2018, 24, 2431–2441. [Google Scholar] [CrossRef]
- ECCO. Update on COVID-19 and IBD. Available online: https://ioibd.org/ioibd-update-on-covid19-for-patients-with-crohns-disease-and-ulcerative-colitis/ (accessed on 25 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Total Number | 106 |
|---|---|
| Gender [Male–Female]; n (%) | 63/43 (59.4%/40.6%) |
| Median Age (y.o.; IQR) | 45 (38–56) |
| Median years from IBD diagnosis (IQR) | 12.0 (5.8–20.0) |
| Smoke [yes/ex/no] (%) | 17/25/64 (16.0%/23.6%/60.4%) |
| Type of IBD [CD–UC–IBD-U]; n (%) | 63/39/4 (59.4/36.8/3.8) |
| Use of Mesalazine; n (%) | 60 (56.6%) |
| Use of corticosteroids; n (%) | 13 (12.3%) |
| Use of Monoclonal Antibodies [yes/no]; n (%) | 63/43 (59.4%/40.6%) Anti-TNF: 30 Vedolizumab: 20 Ustekinumab: 7 Anti-IL-23: 6 |
| Vitamin D supplementation (yes/no) | 43/63 (40.6%/59.4%) |
| Median Vitamin D levels (ng/mL; IQR) | 21.9 (14.8–28.7) |
| Vitamin D status (<20 ng/mL; 20–30 ng/mL; >30 ng/mL); n (%) | 45/38 /23 (42.5%/35.8%/21.7%) |
| COVID-19 Anamnesis (yes/no); n (%) | 24/82 (19.8–80.2) |
| COVID-19 Severity [No sympt./Mild/Severe]; n | 5/15/4 |
| Serological Anti-SARS-CoV2 Ag [Positive/Negative] (%) | 30/76 (28.3%/71.7%) |
| Anti-SARS-CoV2 titer (AU/mL) | 4.81 (3.80–18.05) |
| Univariate Logistic Regression Analysis | ||
|---|---|---|
| Predictor | p Value | Odds Ratio (Conf. Interval 95%) |
| Vitamin D supplementation (yes = 1; no = 0) | 0.050 | 0.395 (0.156–1.000) |
| Use of Monoclonal Antibodies (yes = 1; no = 0) | 0.012 | 0.327 (0.136–0.783) |
| Use of Mesalazine (yes = 1; no = 0) | 0.032 | 2.750 (1.090–6.940) |
| Crohn’s Disease (yes = 1; no = 0) | 0.036 | 0.398 (0.168–0.943) |
| Sex (Male = 1; Female = 0) | 0.036 | 0.398 (0.168–0.943) |
| Multivariate Logistic Regression analysis | ||
| Covariate | p value | Odds Ratio (conf. interval 95%) |
| VD supplementation (yes = 1; no = 0) | 0.002 | 0.166 (0.053–0.517) |
| Use of Monoclonal Antibodies (yes = 1; no = 0) | 0.007 | 0.227 (0.078–0.662) |
| Use of Mesalazine (yes = 1; no = 0) | 0.046 | 2.968 (1.021–8.623) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Nicolò, A.; Cusato, J.; Bezzio, C.; Saibeni, S.; Vernero, M.; Disabato, M.; Caviglia, G.P.; Ianniello, A.; Manca, A.; D’Avolio, A.; et al. Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease. Nutrients 2023, 15, 169. https://doi.org/10.3390/nu15010169
De Nicolò A, Cusato J, Bezzio C, Saibeni S, Vernero M, Disabato M, Caviglia GP, Ianniello A, Manca A, D’Avolio A, et al. Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease. Nutrients. 2023; 15(1):169. https://doi.org/10.3390/nu15010169
Chicago/Turabian StyleDe Nicolò, Amedeo, Jessica Cusato, Cristina Bezzio, Simone Saibeni, Marta Vernero, Michela Disabato, Gian Paolo Caviglia, Alice Ianniello, Alessandra Manca, Antonio D’Avolio, and et al. 2023. "Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease" Nutrients 15, no. 1: 169. https://doi.org/10.3390/nu15010169
APA StyleDe Nicolò, A., Cusato, J., Bezzio, C., Saibeni, S., Vernero, M., Disabato, M., Caviglia, G. P., Ianniello, A., Manca, A., D’Avolio, A., & Ribaldone, D. G. (2023). Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease. Nutrients, 15(1), 169. https://doi.org/10.3390/nu15010169