
Diet in Early Life Is Related to Child Mental Health and Personality at 8 Years: Findings from the Norwegian Mother, Father and Child Cohort Study (MoBa)

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
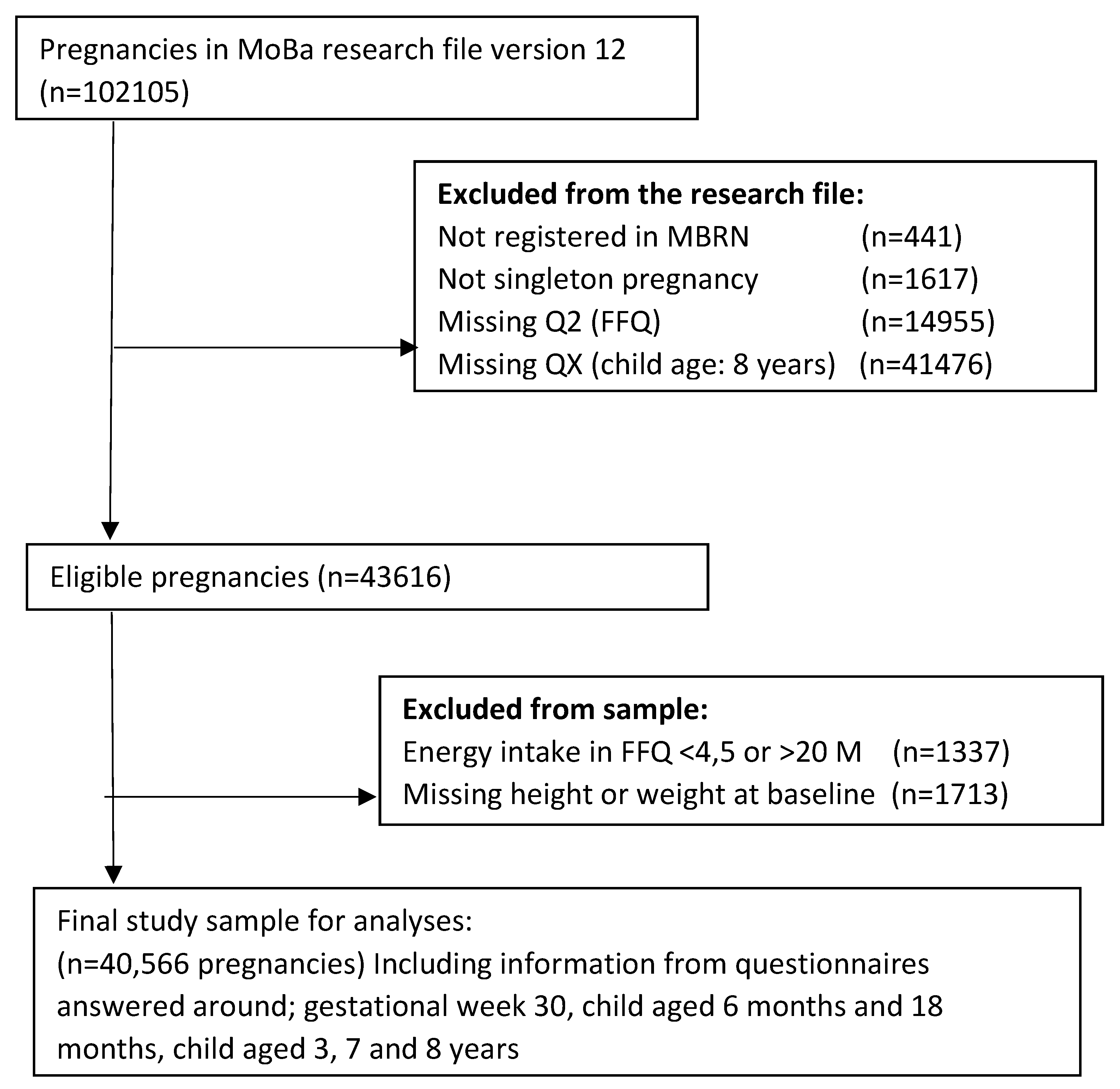
2.2. Study Population Inclusion and Exclusion Criteria
2.3. Exposure
2.4. Outcomes
2.5. Anxiety Symptoms
2.6. Depression Symptoms
2.7. Personality Traits
2.8. Potential Confounders
2.9. Ethics
2.10. Statistics
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Hanson, M.A.; Gluckman, P.D. Developmental origins of health and disease—Global public health implications. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 24–31. [Google Scholar] [CrossRef]
- Borge, T.C.; Aase, H.; Brantsæter, A.L.; Biele, G. The importance of maternal diet quality during pregnancy on cognitive and behavioural outcomes in children: A systematic review and meta-analysis. BMJ Open 2017, 7, e016777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzenberg, S.J.; Georgieff, M.K. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef] [Green Version]
- Cetin, I.; Bühling, K.; Demir, C.; Kortam, A.; Prescott, S.L.; Yamashiro, Y.; Yarmolinskaya, M.; Koletzko, B. Impact of Micronutrient Status during Pregnancy on Early Nutrition Programming. Ann. Nutr. Metab. 2019, 74, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiese, B.H.; Foley, K.P.; Spagnola, M. Routine and ritual elements in family mealtimes: Contexts for child well-being and family identity. New Dir. Child Adolesc. Dev. 2006, 111, 67–89. [Google Scholar] [CrossRef]
- Birch, L.L.; Doub, A.E. Learning to eat: Birth to age 2 y. Am. J. Clin. Nutr. 2014, 99, 723s–728s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2019 Mental Disorders Collaborators. Global, regional and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef]
- Jacka, F.N.; Ystrom, E.; Brantsaeter, A.L.; Karevold, E.; Roth, C.; Haugen, M.; Meltzer, H.M.; Schjolberg, S.; Berk, M. Maternal and early postnatal nutrition and mental health of offspring by age 5 years: A prospective cohort study. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- Borge, T.C.; Biele, G.; Papadopoulou, E.; Andersen, L.F.; Jacka, F.; Eggesbø, M.; Caspersen, I.H.; Aase, H.; Meltzer, H.M.; Brantsæter, A.L. The associations between maternal and child diet quality and child ADHD—Findings from a large Norwegian pregnancy cohort study. BMC Psychiatry 2021, 21, 139. [Google Scholar] [CrossRef] [PubMed]
- Mortaji, N.; Krzeczkowski, J.E.; Boylan, K.; Booij, L.; Perreault, M.; Van Lieshout, R.J. Maternal pregnancy diet, postnatal home environment and executive function and behavior in 3- to 4-y-olds. Am. J. Clin. Nutr. 2021, 114, 1418–1427. [Google Scholar] [CrossRef]
- Mahmassani, H.A.; Switkowski, K.M.; Scott, T.M.; Johnson, E.J.; Rifas-Shiman, S.L.; Oken, E.; Jacques, P.F. Maternal diet quality during pregnancy and child cognition and behavior in a US cohort. Am. J. Clin. Nutr. 2022, 115, 128–141. [Google Scholar] [CrossRef]
- Gosling, S.D.; Rentfrow, P.J.; Swann, W.B. A very brief measure of the Big-Five personality domains. J. Res. Personal. 2003, 37, 504–528. [Google Scholar] [CrossRef]
- Steel, P.; Schmidt, J.; Shultz, J. Refining the relationship between personality and subjective well-being. Psychol. Bull. 2008, 134, 138–161. [Google Scholar] [CrossRef] [Green Version]
- Lamers, S.M.A.; Westerhof, G.J.; Kovács, V.; Bohlmeijer, E.T. Differential relationships in the association of the Big Five personality traits with positive mental health and psychopathology. J. Res. Personal. 2012, 46, 517–524. [Google Scholar] [CrossRef]
- Schoeps, A.; Gontijo de Castro, T.; Peterson, E.R.; Wall, C.; D’Souza, S.; Waldie, K.E.; Morton, S. Associations between antenatal maternal diet and other health aspects with infant temperament in a large multiethnic cohort study: A path analysis approach. BMJ Open 2022, 12, e046790. [Google Scholar] [CrossRef]
- Sayal, K.; Heron, J.; Maughan, B.; Rowe, R.; Ramchandani, P. Infant temperament and childhood psychiatric disorder: Longitudinal study. Child Care Health Dev. 2014, 40, 292–297. [Google Scholar] [CrossRef] [Green Version]
- House, J.S.; Mendez, M.; Maguire, R.L.; Gonzalez-Nahm, S.; Huang, Z.; Daniels, J.; Murphy, S.K.; Fuemmeler, B.F.; Wright, F.A.; Hoyo, C. Periconceptional Maternal Mediterranean Diet Is Associated with Favorable Offspring Behaviors and Altered CpG Methylation of Imprinted Genes. Front. Cell Dev. Biol. 2018, 6, 107. [Google Scholar] [CrossRef]
- Hillesund, E.R.; Bere, E.; Haugen, M.; Øverby, N.C. Development of a New Nordic Diet score and its association with gestational weight gain and fetal growth—A study performed in the Norwegian Mother and Child Cohort Study (MoBa). Public Health Nutr. 2014, 17, 1909–1918. [Google Scholar] [CrossRef] [Green Version]
- Agnihotri, N.; Rudjord Hillesund, E.; Bere, E.; Wills, A.K.; Brantsæter, A.L.; Øverby, N.C. Development and description of New Nordic Diet scores across infancy and childhood in the Norwegian Mother, Father and Child Cohort Study (MoBa). Matern. Child Nutr. 2021, 17, e13150. [Google Scholar] [CrossRef] [PubMed]
- Vejrup, K.; Agnihotri, N.; Bere, E.; Schjølberg, S.; LeBlanc, M.; Hillesund, E.R.; Øverby, N.C. Adherence to a Healthy and Potentially Sustainable Nordic Diet is Associated with Child Development in The Norwegian Mother, Father and Child Cohort Study (MoBa). Nutr. J. 2022, 21, 46. [Google Scholar] [CrossRef] [PubMed]
- Luu, T.M.; Rehman Mian, M.O.; Nuyt, A.M. Long-Term Impact of Preterm Birth: Neurodevelopmental and Physical Health Outcomes. Clin. Perinatol. 2017, 44, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Sibai, B.; Dekker, G.; Kupferminc, M. Pre-eclampsia. Lancet 2005, 365, 785–799. [Google Scholar] [CrossRef]
- Magnus, P.; Birke, C.; Vejrup, K.; Haugan, A.; Alsaker, E.; Daltveit, A.K.; Handal, M.; Haugen, M.; Høiseth, G.; Knudsen, G.P.; et al. Cohort Profile Update: The Norwegian Mother and Child Cohort Study (MoBa). Int. J. Epidemiol. 2016, 45, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Irgens, L.M. The Medical Birth Registry of Norway. Epidemiological research and surveillance throughout 30 years. Acta Obstet. Gynecol. Scand. 2000, 79, 435–439. [Google Scholar] [PubMed]
- Health NIoP. Questionnaires from MoBa. 2022. Available online: https://www.fhi.no/en/studies/moba/for-forskere-artikler/questionnaires-from-moba/ (accessed on 12 December 2022).
- Brantsaeter, A.L.; Haugen, M.; Alexander, J.; Meltzer, H.M. Validity of a new food frequency questionnaire for pregnant women in the Norwegian Mother and Child Cohort Study (MoBa). Matern. Child Nutr. 2008, 4, 28–43. [Google Scholar] [CrossRef]
- Agnihotri, N.; Øverby, N.C.; Bere, E.; Wills, A.K.; Brantsæter, A.L.; Hillesund, E.R. Childhood adherence to a potentially healthy and sustainable Nordic diet and later overweight: The Norwegian Mother, Father and Child Cohort Study (MoBa). Matern. Child Nutr. 2021, 17, e13101. [Google Scholar] [CrossRef]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Birmaher, B.; Brent, D.A.; Chiappetta, L.; Bridge, J.; Monga, S.; Baugher, M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Angold, A.; Costello, E.J. Mood and Feelings Questionnaire (MFQ); Duke University: Durham, NC, USA, 1987. [Google Scholar]
- Angold, A.; Costello, E.J.; Messer, S.C.; Pickles, A.; Winder, F.; Silver, D. The development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int. J. Methods Pscychiatric Res. 1995, 5, 237–249. [Google Scholar]
- Sharp, C.; Goodyer, I.M.; Croudace, T.J. The Short Mood and Feelings Questionnaire (SMFQ): A unidimensional item response theory and categorical data factor analysis of self-report ratings from a community sample of 7-through 11-year-old children. J. Abnorm. Child Psychol. 2006, 34, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Vollrath, M.E.; Hampson, S.E.; Torgersen, S. Constructing a short form of the hierarchical personality inventory for children (HiPIC): The HiPIC-30. Pers. Ment. Health 2016, 10, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Mervielde, I.; De Fruyt, F. Construction of the hierarchical personality inventory for children (HiPIC). In Personality Psychology in Europe; Tilburg University Press: Tilburg, The Netherlands, 1999; Volume 7, pp. 107–127. [Google Scholar]
- Mervielde, I.; De Fruyt, F. Assessing children’s traits with the hierarchial personality inventory for children. In Big Five Assessment; De Raad, B., Perugini, M., Eds.; Hogrefe & Huber: Ashland, OH, USA, 2002; pp. 129–242. [Google Scholar]
- Vollrath, M.E.; Hampson, S.E.; Júlíusson, P.B. Children and eating. Personality and gender are associated with obesogenic food consumption and overweight in 6- to 12-year-olds. Appetite 2012, 58, 1113–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassaganya-Riera, J.; Berry, E.M.; Blaak, E.E.; Burlingame, B.; le Coutre, J.; van Eden, W.; El-Sohemy, A.; German, J.B.; Knorr, D.; Lacroix, C.; et al. Goals in Nutrition Science 2020–2025. Front. Nutr. 2020, 7, 606378. [Google Scholar] [CrossRef]
- Blomkvist, E.A.M.; Hillesund, E.R.; Helland, S.H.; Simhan, I.; Øverby, N.C. Diet and Neurodevelopmental Score in a Sample of One-Year-Old Children-A Cross-Sectional Study. Nutrients 2019, 11, 1676. [Google Scholar] [CrossRef] [Green Version]
- Brett, K.E.; Ferraro, Z.M.; Yockell-Lelievre, J.; Gruslin, A.; Adamo, K.B. Maternal-fetal nutrient transport in pregnancy pathologies: The role of the placenta. Int. J. Mol. Sci. 2014, 15, 16153–16185. [Google Scholar] [CrossRef] [Green Version]
- Hillesund, E.R.; Øverby, N.C.; Engel, S.M.; Klungsøyr, K.; Harmon, Q.E.; Haugen, M.; Bere, E. Associations of adherence to the New Nordic Diet with risk of preeclampsia and preterm delivery in the Norwegian Mother and Child Cohort Study (MoBa). Eur. J. Epidemiol. 2014, 29, 753–765. [Google Scholar] [CrossRef] [Green Version]
- Hanson, M.A.; Gluckman, P.D. Early developmental conditioning of later health and disease: Physiology or pathophysiology? Physiol. Rev. 2014, 94, 1027–1076. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, R.M.; Vollset, S.E.; Gjessing, H.K.; Skjaerven, R.; Melve, K.K.; Schreuder, P.; Alsaker, E.R.; Haug, K.; Daltveit, A.K.; Magnus, P. Self-selection and bias in a large prospective pregnancy cohort in Norway. Paediatr. Perinat. Epidemiol. 2009, 23, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Vollrath, M.E.; Torgersen, S.; Torgersen, L. Associations of children’s Big Five personality with eating behaviors. BMC Res. Notes 2018, 11, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| New Nordic Diet Score | N | Mean NND Score (SD) | Score Range | Median | Low Score % | Medium Score % | High Score % |
|---|---|---|---|---|---|---|---|
| Maternal pregnancy diet | 40,566 | 5.0 (2.0) | 0–10 | 5 | 24.6 | 34.8 | 40.6 |
| Child diet 6 months | 39,138 | 3.4 (1.3) | 0–6 | 3 | 24.9 | 55.5 | 19.6 |
| Child diet 18 months | 36,865 | 4.3 (1.7) | 0–9 | 4 | 32.5 | 43.5 | 24.0 |
| Child diet 3 years | 33,464 | 2.8 (1.4) | 0–6 | 3 | 19.1 | 49.4 | 31.5 |
| Child diet 7 years | 34,588 | 4.7 (1.7) | 0–9 | 5 | 24.7 | 43.5 | 31.8 |
| Mental Health | N | Mean (SD) | Median | Score Range | High Score * N (%) |
|---|---|---|---|---|---|
| Anxiety 1 | 40,151 | 6.0 (1.2) | 6 | 5–15 | 4119 (10.3) |
| Depression 2 | 39,532 | 14.9 (2.4) | 14 | 13–39 | 4607 (11.7) |
| Child Personality Traits 1 | N | Mean (SD) | Median | Range (Min–Max) |
|---|---|---|---|---|
| Extraversion | 40,055 | 21.9 (3.5) | 22 | 5–30 |
| Benevolence | 39,780 | 21.5 (3.7) | 22 | 6–30 |
| Neuroticism | 39,998 | 14.2 (3.2) | 14 | 5–29 |
| Conscientiousness | 39,984 | 21.9 (3.6) | 22 | 6–30 |
| Imagination | 39,987 | 23.6 (3.3) | 24 | 6–30 |
| NND Score | Anxiety Symptoms 2 | Depression Symptoms 3 | |
|---|---|---|---|
| β (95% CI) | β (95% CI) | ||
| Maternal score | Crude | −0.00 (−0.01, 0.00) | −0.04 (−0.05, −0.03) * |
| Adjusted | −0.00 (−0.01, 0.00) | −0.02 (−0.03, −0.01) * | |
| 6 months | Crude | 0.01 (−0.0, 0.01) | −0.04 (−0.06, −0.02) * |
| Adjusted | 0.01 (−0.01, 0.02) | −0.00 (−0.02, 0.02) | |
| 18 months | Crude | −0.00 (−0.01, 0.01) | −0.03 (−0.04, −0.01) * |
| Adjusted | −0.00 (−0.01, 0.01) | −0.01 (−0.02, 0.01) | |
| 3 years | Crude | −0.01 (−0.02, −0.01) * | −0.05 (−0.07, −0.03) * |
| Adjusted | −0.01 (−0.02, −0.01) * | −0.03 (−0.05, −0.01) * | |
| 7 years | Crude | −0.02 (−0.03, −0.01) * | −0.04 (−0.06, −0.03) * |
| Adjusted | −0.02 (−0.03, −0.01) * | −0.03 (−0.05, −0.02) * | |
| NND | Anxiety Symptoms 2 | Depression Symptoms 3 | |||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | ||
| maternal | Crude | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.2 (1.1, 1.2) * | 1.1 (1.0, 1.2) * | 1 |
| Adjusted | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | |
| 6 months | Crude | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.2 (1.1, 1.3) * | 1.0 (0.9, 1.1) | 1 |
| Adjusted | 0.9 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | |
| 18 months | Crude | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.1 (1.0, 1.2) * | 1.0 (0.9, 1.1) | 1 |
| Adjusted | 1.1 (0.9, 1.1) | 1.0 (0.9, 1.1) | 1 | 1.0 (0.9, 1.1) | 0.9 (0.9, 1.1) | 1 | |
| 3 years | Crude | 1.2 (1.0, 1.3) * | 1.1 (0.9, 1.2) | 1 | 1.2 (1.1, 1.3) * | 1.1 (1.0, 1.2) * | 1 |
| Adjusted | 1.1 (1.0, 1.3) * | 1.0 (0.9, 1.1) | 1 | 1.0 (0.9, 1.2) | 1.0 (0.9, 1.1) | 1 | |
| 7 years | Crude | 1.2 (1.1, 1.3) * | 1.0 (0.9, 1.1) | 1 | 1.2 (1.1, 1.3) * | 1.1 (1.0, 1.2) * | 1 |
| Adjusted | 1.2 (1.1, 1.3) * | 1.0 (0.9, 1.1) | 1 | 1.0 (1.0, 1.2) * | 1.0 (0.9, 1.1) | 1 | |
| Child Personality Trait | Extraversion | Benevolence | Neuroticism | Conscientiousness | Imagination | |
|---|---|---|---|---|---|---|
| NND Score | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | |
| Maternal score | Crude | 0.07 (0.05, 0.08) * | 0.05 (0.03, 0.07) * | −0.06 (−0.08, −0.05) * | 0.12 (0.11, 0.14) * | 0.14 (0.12, 0.16) * |
| Adjusted | 0.06 (0.04, 0.08) * | 0.05 (0.03, 0.07) * | −0.02 (−0.04, −0.01) * | 0.10 (0.08, 0.12) * | 0.12 (0.11, 0.14) * | |
| 6 months | Crude | −0.10 (−0.12, −0.07) * | 0.01 (−0.02, 0.04) | 0.02 (−0.01, 0.05) | 0.04 (0.01, 0.06) * | 0.13 (0.10, 0.15) * |
| Adjusted | −0.06 (−0.09, −0.04) * | −0.00 (−0.03, 0.03) | 0.02 (−0.00, 0.04) | 0.01 (−0.02, 0.04) | 0.09 (0.06, 0.12) * | |
| 18 months | Crude | 0.05 (0.03, 0.08) * | 0.08 (0.06, 0.10) * | −0.02 (−0.04, −0.00) * | 0.11 (0.08, 0.13) * | 0.20 (0.18, 0.22) * |
| Adjusted | 0.07 (0.04, 0.09) * | 0.07 (0.05, 0.10) * | −0.02 (−0.04, 0.00) | 0.09 (0.07, 0.11) * | 0.18 (0.16, 0.20) * | |
| 3 years | Crude | 0.09 (0.06, 0.11) * | 0.14 (0.11, 0.17) * | −0.10 (−0.12, −0.07) * | 0.18 (0.15, 0.21) * | 0.24 (0.21, 0.26) * |
| Adjusted | 0.11 (0.08, 0.14) * | 0.13 (0.10, 0.16) * | −0.09 (−0.12, −0.07) * | 0.16 (0.13, 0.19) * | 0.21 (0.19, 0.24) * | |
| 7 years | Crude | 0.04 (0.02, 0.06) * | 0.14 (0.11, 0.16) * | −0.04 (−0.05, −0.02) * | 0.14 (0.12, 0.17) * | 0.18 (0.16, 0.20) * |
| Adjusted | 0.06 (0.04, 0.09) * | 0.14 (0.11, 0.16) * | −0.06 (−0.08, −0.04) * | 0.14 (0.12, 0.16) * | 0.16 (0.14, 0.18) * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vejrup, K.; Hillesund, E.R.; Agnihotri, N.; Helle, C.; Øverby, N.C. Diet in Early Life Is Related to Child Mental Health and Personality at 8 Years: Findings from the Norwegian Mother, Father and Child Cohort Study (MoBa). Nutrients 2023, 15, 243. https://doi.org/10.3390/nu15010243
Vejrup K, Hillesund ER, Agnihotri N, Helle C, Øverby NC. Diet in Early Life Is Related to Child Mental Health and Personality at 8 Years: Findings from the Norwegian Mother, Father and Child Cohort Study (MoBa). Nutrients. 2023; 15(1):243. https://doi.org/10.3390/nu15010243
Chicago/Turabian StyleVejrup, Kristine, Elisabet R. Hillesund, Neha Agnihotri, Christine Helle, and Nina C. Øverby. 2023. "Diet in Early Life Is Related to Child Mental Health and Personality at 8 Years: Findings from the Norwegian Mother, Father and Child Cohort Study (MoBa)" Nutrients 15, no. 1: 243. https://doi.org/10.3390/nu15010243
APA StyleVejrup, K., Hillesund, E. R., Agnihotri, N., Helle, C., & Øverby, N. C. (2023). Diet in Early Life Is Related to Child Mental Health and Personality at 8 Years: Findings from the Norwegian Mother, Father and Child Cohort Study (MoBa). Nutrients, 15(1), 243. https://doi.org/10.3390/nu15010243