
Probiotic Bifidobacterium longum BB68S Improves Cognitive Functions in Healthy Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial


Abstract
:1. Introduction
2. Methods
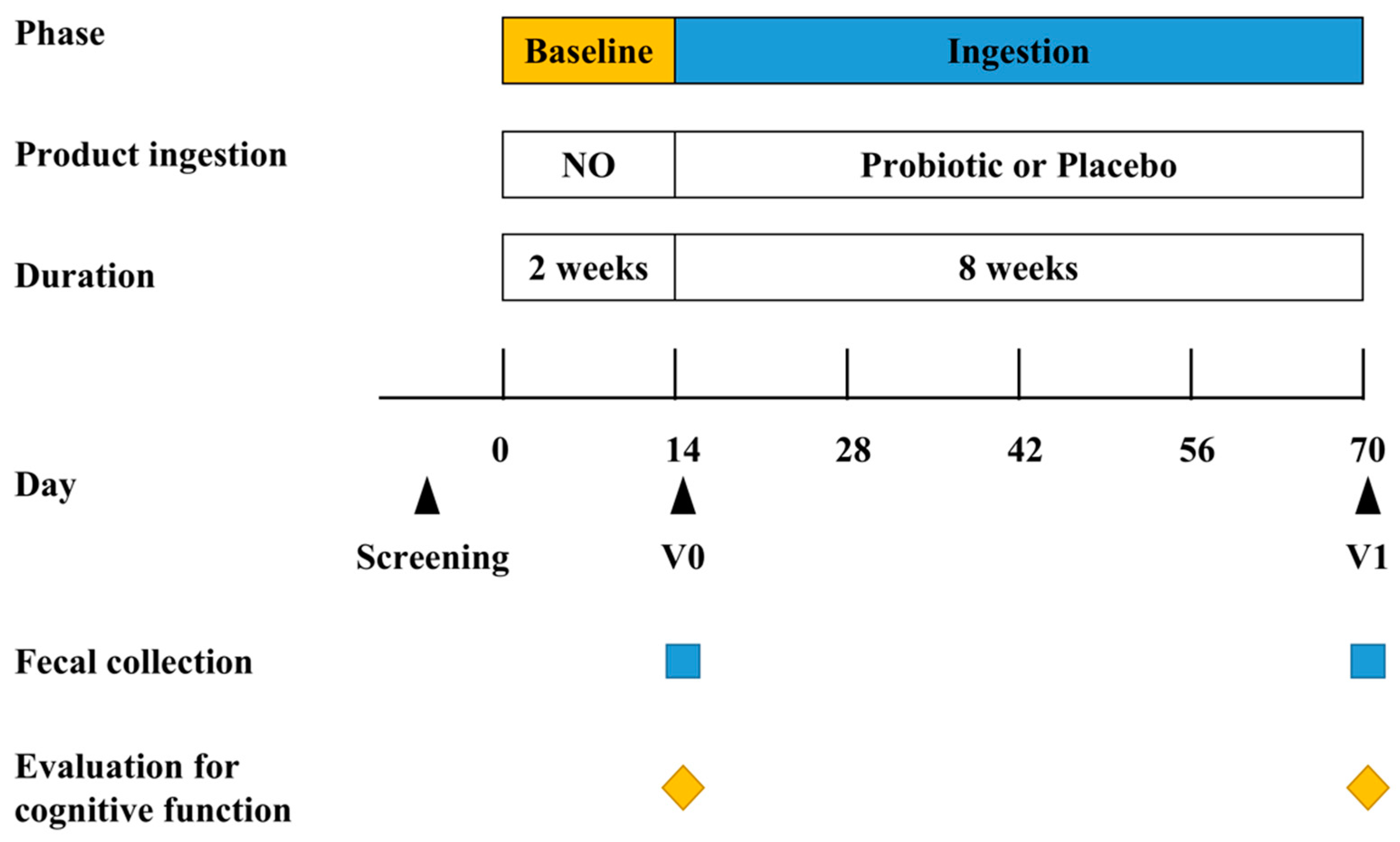
2.1. Study Design
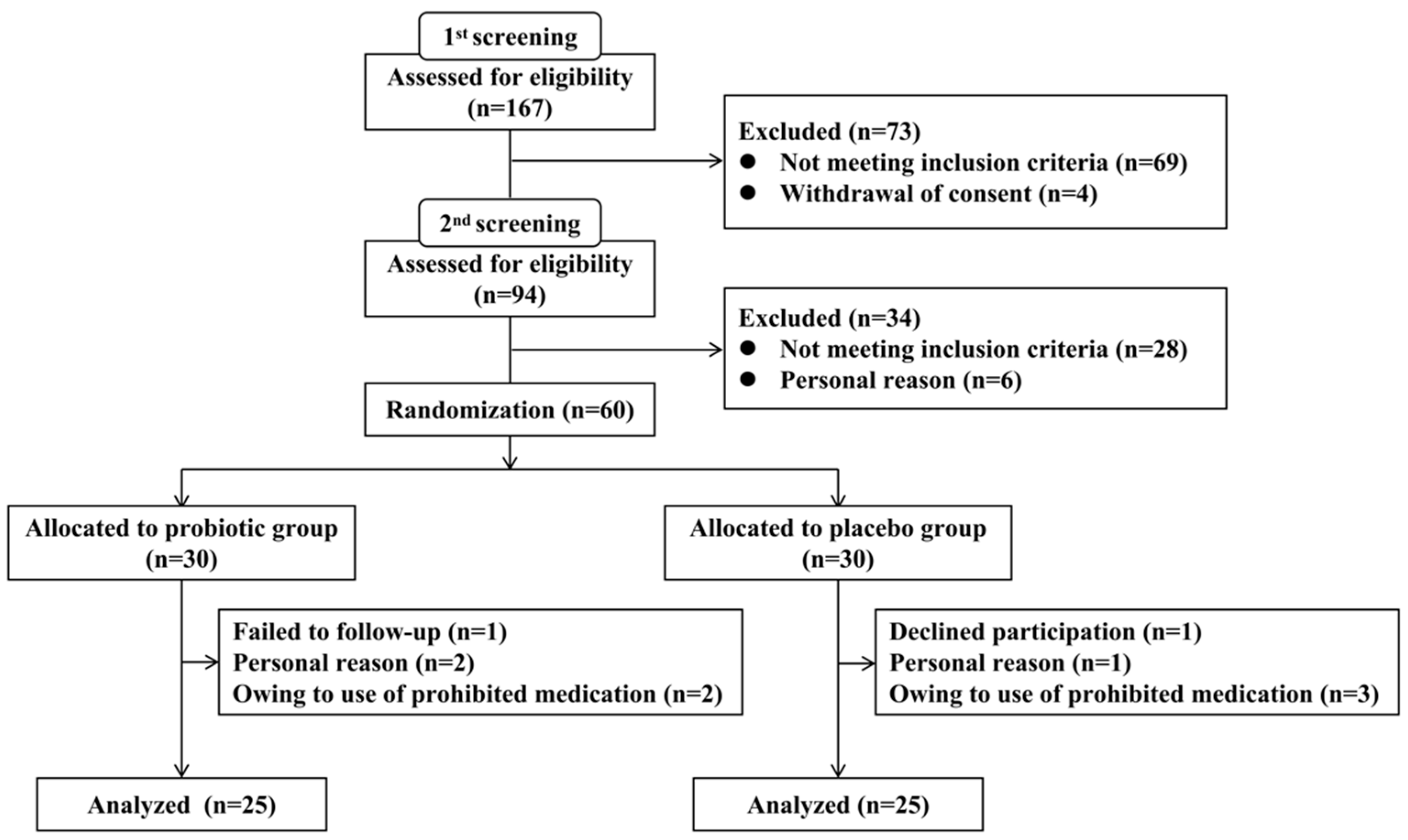
2.2. Participants
2.3. Inclusion and Exclusion Criteria
2.4. Randomization and Blinding
2.5. Fecal Sample Collection
2.6. Evaluation of Cognitive Functions
2.7. Gut Microbiota Analysis
2.7.1. Genomic DNA Extraction, Amplification, and Sequencing
2.7.2. Processing of Sequencing Data
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
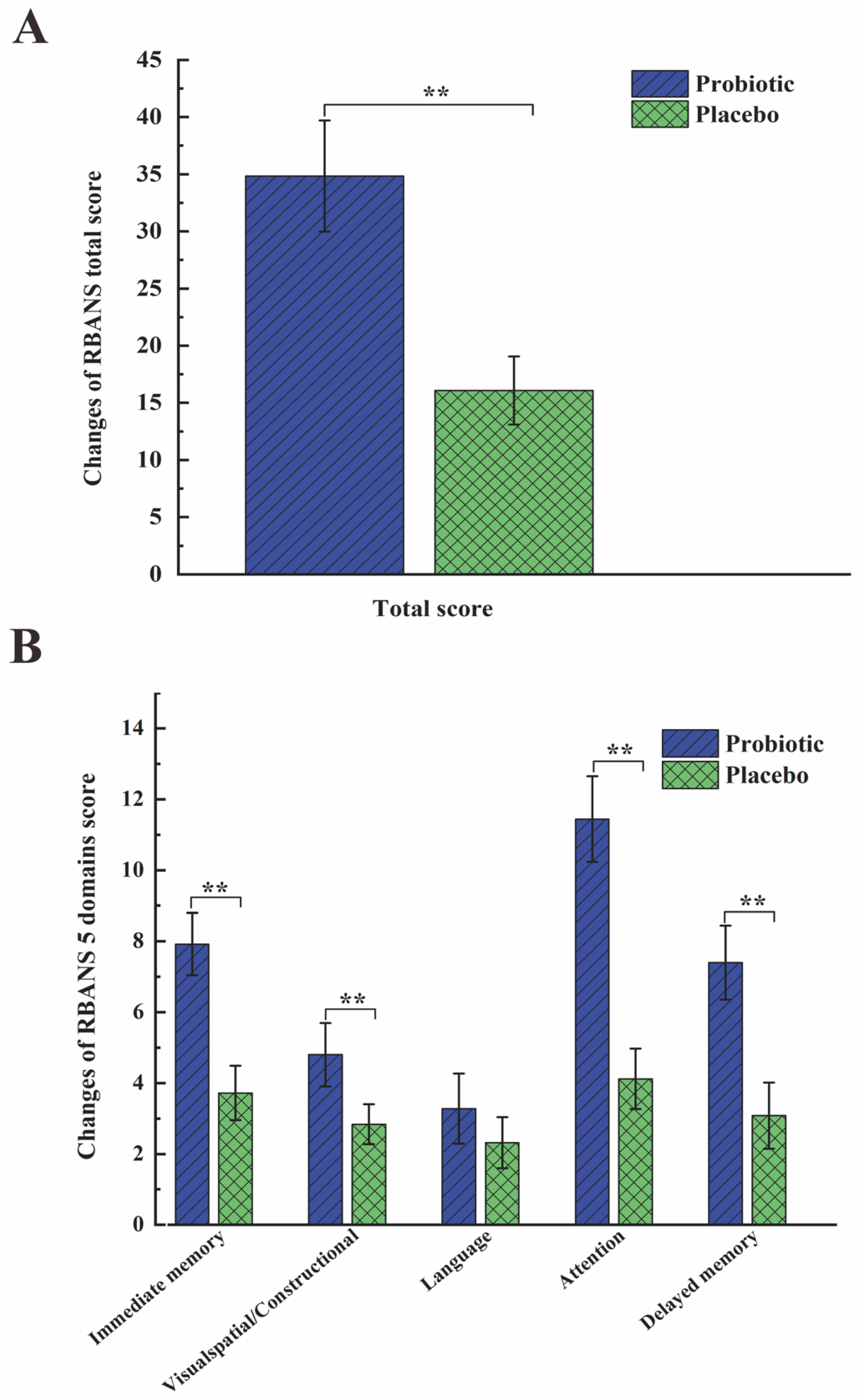
3.2. Primary Outcomes for Cognitive Function
3.3. Results of Gut Microbiota Composition
3.3.1. Results of Alpha-Diversity
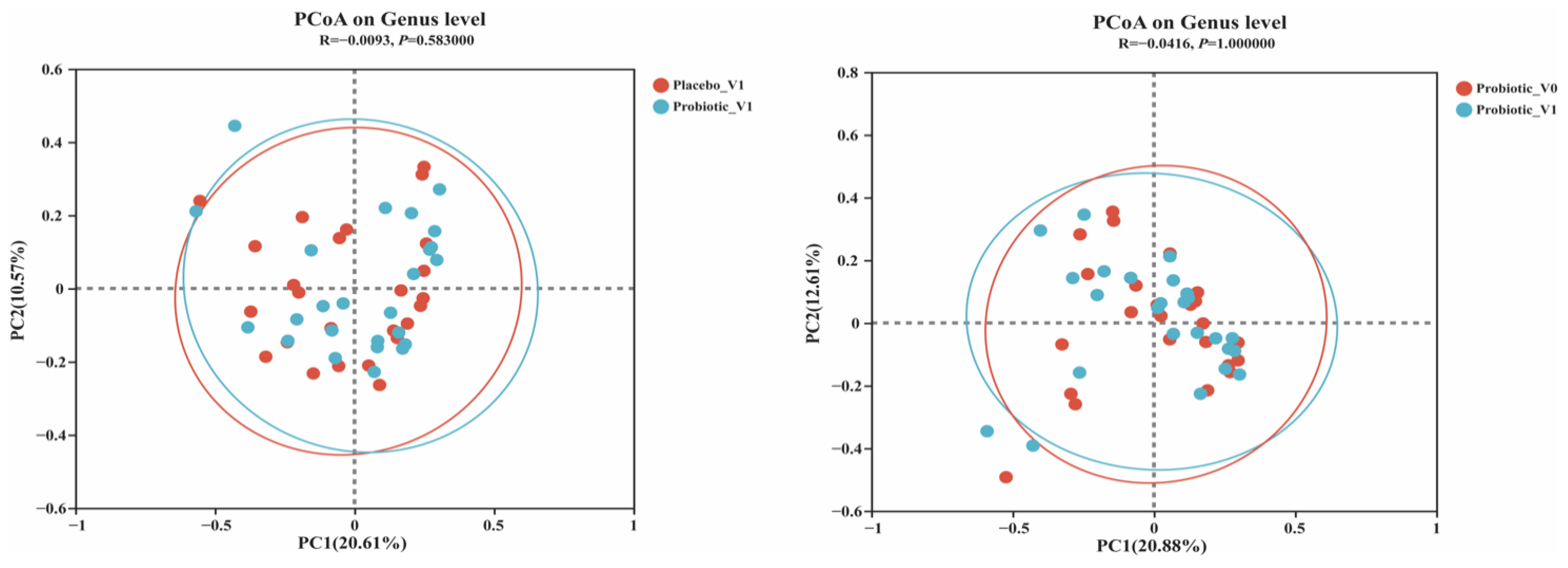
3.3.2. Results of Beta-Diversity
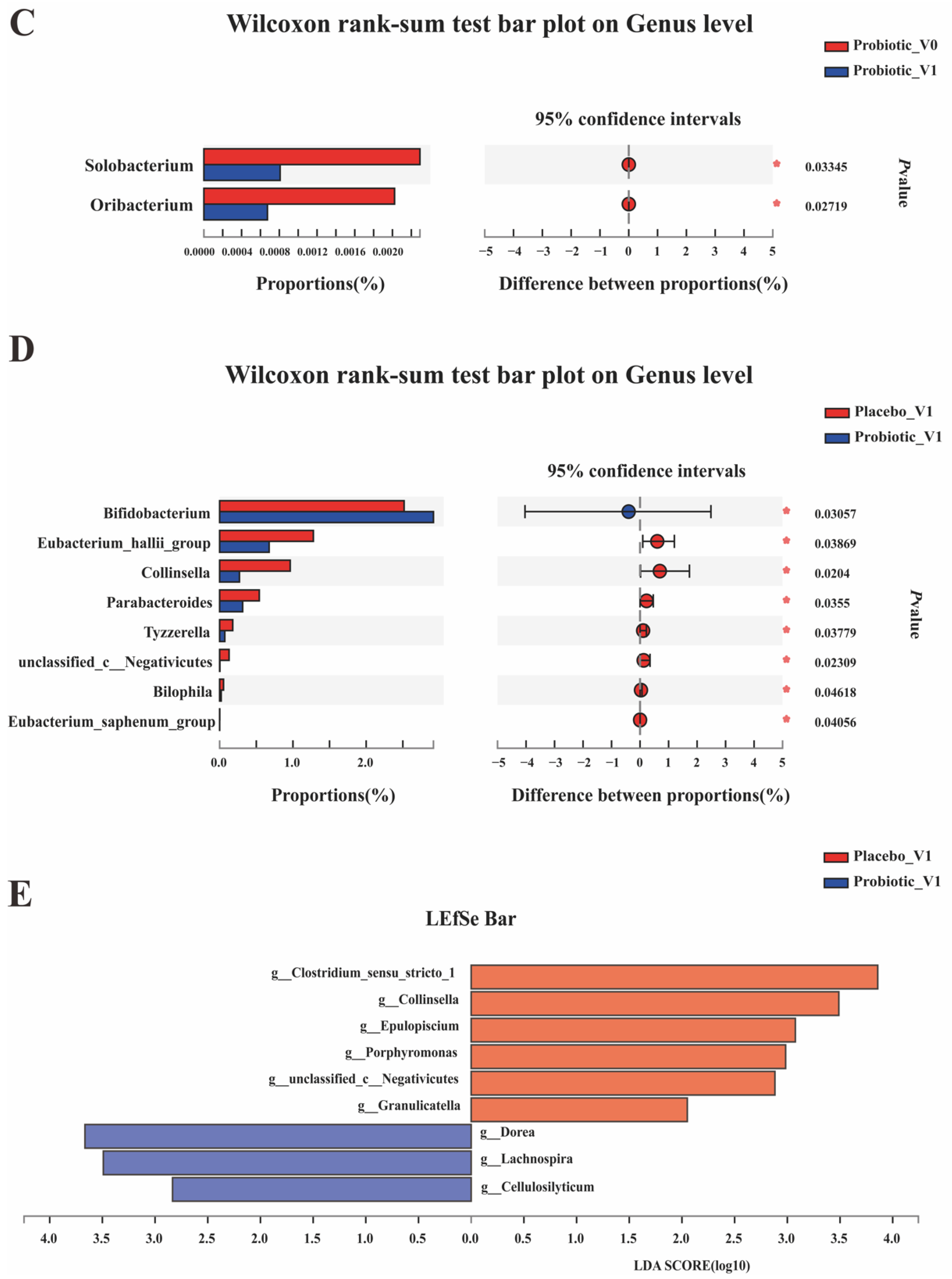
3.3.3. Results of the Species Composition Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Q.Y.; Pan, Y.C.; Shu, H.Y.; Zhang, L.J.; Li, Q.Y.; Ge, Q.M.; Shao, Y.; Zhou, Q. Brain Activity in Age-Related Macular Degeneration Patients from the Perspective of Regional Homogeneity: A Resting-State Functional Magnetic Resonance Imaging Study. Front. Aging Neurosci. 2022, 14, 865430. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.E.; Ryan, L.; Bowers, D.; Foster, T.C.; Bizon, J.L.; Geldmacher, D.S.; Glisky, E.L. Characterizing Cognitive Aging in Humans with Links to Animal Models. Front. Aging Neurosci. 2012, 4, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafto, M.A.; Tyler, L.K. Language in the Aging Brain: The Network Dynamics of Cognitive Decline and Preservation. Science 2014, 346, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Harper, S. Economic and Social Implications of Aging Societies. Science 2014, 346, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Lederberg, J.; McCray, A.T. ‘Ome Sweet’ Omics—A Genealogical Treasury of Words. Scientist 2001, 15, 8. [Google Scholar]
- Buffington, S.A.; Dooling, S.W.; Sgritta, M.; Noecker, C.; Murillo, O.D.; Felice, D.F.; Turnbaugh, P.J.; Costa-Mattioli, M. Dissecting the Contribution of Host Genetics and the Microbiome in Complex Behaviors. Cell 2021, 184, 1740–1756. [Google Scholar] [CrossRef]
- Jameson, K.G.; Hsiao, E.Y. Linking the Gut Microbiota to a Brain Neurotransmitter. Trends Neurosci. 2018, 41, 413–414. [Google Scholar] [CrossRef]
- Zhang, Z.J.; Mu, X.H.; Cao, Q.N.; Shi, Y.; Hu, X.S.; Zheng, H. Honeybee Gut Lactobacillus Modulates Host Learning and Memory Behaviors Via Regulating Tryptophan Metabolism. Nat. Commun. 2022, 13, 2037. [Google Scholar] [CrossRef]
- Costabile, A.; Bergillos-Meca, T.; Rasinkangas, P.; Korpela, K.; de Vos, W.M.; Gibson, G.R. Effects of Soluble Corn Fiber Alone or in Synbiotic Combination with Lactobacillus Rhamnosus GG and the Pilus-Deficient Derivative Gg-Pb12 on Fecal Microbiota, Metabolism, and Markers of Immune Function: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study in Healthy Elderly (Saimes Study). Front. Immunol. 2017, 8, 01443. [Google Scholar]
- Ghosh, T.S.; Shanahan, F.; O’Toole, P.W. The Gut Microbiome as a Modulator of Healthy Ageing. Nature Reviews Gastroenterol. Hepatol. 2022, 19, 565–584. [Google Scholar] [CrossRef]
- Huang, S.; Haiminen, N.; Carrieri, A.P.; Hu, R.; Jiang, L.J.; Parida, L.; Russell, B.; Allaband, C.; Zarrinpar, A.; Vazquez-Baeza, Y.; et al. Human Skin, Oral, and Gut Microbiomes Predict Chronological Age. Msystems 2020, 5, e00630-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, M.E.; Merenstein, D.J.; Reid, G.; Gibson, G.R.; Rastall, R.A. Probiotics and Prebiotics in Intestinal Health and Disease: From Biology to the Clinic. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Wieers, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; de Foy, J.M.P.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2020, 9, 00454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, F.; Polk, D.B. Probiotics and Probiotic-Derived Functional Factors-Mechanistic Insights into Applications for Intestinal Homeostasis. Front. Immunol. 2020, 11, 01428. [Google Scholar] [CrossRef] [PubMed]
- Bialecka-Debek, A.; Granda, D.; Szmidt, M.K.; Zielinska, D. Gut Microbiota, Probiotic Interventions, and Cognitive Function in the Elderly: A Review of Current Knowledge. Nutrients 2021, 13, 2514. [Google Scholar] [CrossRef]
- Tillisch, K.; Labus, J.; Kilpatrick, L.; Jiang, Z.; Stains, J.; Ebrat, B.; Guyonnet, D.; Legrain-Raspaud, S.; Trotin, B.; Naliboff, B.; et al. Consumption of Fermented Milk Product with Probiotic Modulates Brain Activity. Gastroenterology 2013, 144, 1394–1401. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.Q.; Yu, D.K.; Xue, L.; Li, H.; Du, J.R. Probiotics Modulate the Microbiota-Gut-Brain Axis and Improve Memory Deficits in Aged Samp8 Mice. Acta Pharm. Sin. B 2020, 10, 475–487. [Google Scholar] [CrossRef]
- Naomi, R.; Embong, H.; Othman, F.; Ghazi, H.F.; Maruthey, N.; Bahari, H. Probiotics for Alzheimer’s Disease: A Systematic Review. Nutrients 2022, 14, 20. [Google Scholar] [CrossRef]
- Romijn, A.R.; Rucklidge, J.J.; Kuijer, R.G.; Frampton, C. A Double-Blind, Randomized, Placebo-Controlled Trial of Lactobacillus Helveticus and Bifidobacterium Longum for the Symptoms of Depression. Aust. N. Z. J. Psychiatry 2017, 51, 810–821. [Google Scholar] [CrossRef] [Green Version]
- Abdelhamid, M.; Zhou, C.Y.; Jung, C.G.; Michikawa, M. Probiotic Bifidobacterium Breve Mcc1274 Mitigates Alzheimer’s Disease-Related Pathologies in Wild-Type Mice. Nutrients 2022, 14, 2543. [Google Scholar] [CrossRef]
- Lv, T.; Ye, M.; Luo, F.; Hu, B.; Wang, A.; Chen, J.; Yan, J.; He, Z.; Chen, F.; Qian, C.; et al. Probiotics Treatment Improves Cognitive Impairment in Patients and Animals: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2021, 120, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Toshimitsu, T.; Okada, E.; Anzai, S.; Shiraishi, I.; Inamura, N.; Kobayashi, S.; Sashihara, T.; Hisatsune, T. Effects of Lactiplantibacillus Plantarum Oll2712 on Memory Function in Older Adults with Declining Memory: A Randomized Placebo-Controlled Trial. Nutrients 2022, 14, 4300. [Google Scholar] [CrossRef]
- Thangaleela, S.; Sivamaruthi, B.S.; Kesika, P.; Chaiyasut, C. Role of Probiotics and Diet in the Management of Neurological Diseases and Mood States: A Review. Microorganisms 2022, 10, 2268. [Google Scholar] [CrossRef] [PubMed]
- Kesika, P.; Suganthy, N.; Sivamaruthi, B.S.; Chaiyasut, C. Role of Gut-Brain Axis, Gut Microbial Composition, and Probiotic Intervention in Alzheimer’s Disease. Life Sci. 2021, 264, 118627. [Google Scholar] [CrossRef] [PubMed]
- Westfall, S.; Lomis, N.; Kahouli, I.; Dia, S.Y.; Singh, S.P.; Prakash, S. Microbiome, Probiotics and Neurodegenerative Diseases: Deciphering the Gut Brain Axis. Cell. Mol. Life Sci. 2017, 74, 3769–3787. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Ge, S.Y.; Sang, Y.; Liu, Z.L. Safety Evaluation of Bifidobacteirum Longum Bb68S in vivo and vitro. In Milk and Milk Product; Springer: New York, NY, USA, 2019; pp. 43–46. [Google Scholar]
- Li, G.H.; Ge, S.Y.; Sang, Y.; Liu, Z.L.; Wang, R. Effect of Bifidobacterium Longum Bb68S on Defaecation and Intestinal Flora in Constipation People. In Milk and Milk Product; Springer: New York, NY, USA, 2019; pp. 22–25. [Google Scholar]
- Xiao, J.Z.; Katsumata, N.; Bernier, F.; Ohno, K.; Yamauchi, Y.; Odamaki, T.; Yoshikawa, K.; Ito, K.; Kaneko, T. Probiotic Bifidobacterium Breve in Improving Cognitive Functions of Older Adults with Suspected Mild Cognitive Impairment: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Alzheimers Dis. 2020, 77, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Zhou, X.; Wu, X.; Lin, S.; Ming, B.; Zhong, J.; Wang, B.; Dong, L. Gut Microbiota Aberration in Patients of Systemic Sclerosis and Bleomycin-Induced Mice Model. Front. Cell. Infect. Microbiol. 2021, 11, 647201. [Google Scholar] [CrossRef] [PubMed]
- Miao, R.; Wan, C.; Wang, Z. The Relationship of Gastric Microbiota and Helicobacter Pylori Infection in Pediatrics Population. Helicobacter 2020, 25, e12676. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, Y.; Chen, Y.; Gu, J. Fastp: An Ultra-Fast All-in-One Fastq Preprocessor. Bioinformatics 2018, 34, i884–i890. [Google Scholar] [CrossRef]
- Magoc, T.; Salzberg, S.L. Flash: Fast Length Adjustment of Short Reads to Improve Genome Assemblies. Bioinformatics 2011, 27, 2957–2963. [Google Scholar] [CrossRef] [Green Version]
- Edgar, R.C. Uparse: Highly Accurate Otu Sequences from Microbial Amplicon Reads. Nat. Methods 2013, 10, 996–998. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Garrity, G.M.; Tiedje, J.M.; Cole, J.R. Naive Bayesian Classifier for Rapid Assignment of Rrna Sequences into the New Bacterial Taxonomy. Appl. Environ. Microbiol. 2007, 73, 5261–5267. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.C.; Jin, H.M.; Cui, Y.; Kim, D.S.; Jung, J.M.; Park, J.I.; Jung, E.S.; Choi, E.K.; Chae, S.W. Fermented Milk of Lactobacillus Helveticus Idcc3801 Improves Cognitive Functioning during Cognitive Fatigue Tests in Healthy Older Adults. J. Funct. Foods 2014, 10, 465–474. [Google Scholar] [CrossRef]
- Kim, C.S.; Cha, L.N.; Sim, M.; Jung, S.; Chun, W.Y.; Baik, H.W.; Shin, D.M. Probiotic Supplementation Improves Cognitive Function and Mood with Changes in Gut Microbiota in Community-Dwelling Older Adults: A Randomized, Double-Blind, Placebo-Controlled, Multicenter Trial. J. Gerontol. Biol. Sci. Med. Sci. 2021, 76, 32–40. [Google Scholar] [CrossRef]
- Siddarth, P.; Li, Z.; Miller, K.J.; Ercoli, L.M.; Merril, D.A.; Henning, S.M.; Heber, D.; Small, G.W. Randomized Placebo-Controlled Study of the Memory Effects of Pomegranate Juice in Middle-Aged and Older Adults. Am. J. Clin. Nutr. 2020, 111, 170–177. [Google Scholar] [CrossRef]
- Gaviria, M.; Pliskin, N.; Kney, A. Cognitive Impairment in Patients with Advanced Heart Failure and Its Implications on Decision-Making Capacity. Congest. Heart Fail. 2011, 17, 175–179. [Google Scholar] [CrossRef]
- Olson, R.A.; Chhanabhai, T.; McKenzie, M. Feasibility Study of the Montreal Cognitive Assessment (Moca) in Patients with Brain Metastases. Support. Care Cancer 2008, 16, 1273–1278. [Google Scholar] [CrossRef]
- Gill, D.J.; Freshman, A.; Blender, J.A.; Ravina, B. The Montreal Cognitive Assessment as a Screening Tool for Cognitive Impairment in Parkinson’s Disease. Mov. Disord. 2008, 23, 1043–1046. [Google Scholar] [CrossRef]
- Nazem, S.; Siderowf, A.D.; Duda, J.E.; Have, T.T.; Colcher, A.; Horn, S.S.; Moberg, P.J.; Wilkinson, J.R.; Hurtig, H.I.; Stern, M.B.; et al. “Normal” Global Cognition According to Mini-Mental State Examination Score. J. Am. Geriatr. Soc. 2009, 57, 304–308. [Google Scholar] [CrossRef] [Green Version]
- Cumming, T.B.; Bernhardt, J.; Linden, T. The Montreal Cognitive Assessment: Short Cognitive Evaluation in a Large Stroke Trial. Stroke 2011, 42, 2642–2644. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.L.; Xu, Y.; Chu, A.Q.; Ding, D.; Liang, X.N.; Nasreddine, Z.S.; Dong, Q.; Hong, Z.; Zhao, Q.H.; Guo, Q.H. Validation of the Chinese Version of Montreal Cognitive Assessment Basic for Screening Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2016, 64, e285–e290. [Google Scholar] [CrossRef] [PubMed]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (Rbans): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Gontkovsky, S.T.; Mold, J.W.; Beatty, W.W. Age and Educational Influences on Rbans Index Scores in a Nondemented Geriatric Sample. Clin. Neuropsychol. 2002, 16, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Duff, K.; Patton, D.; Schoenberg, M.R.; Mold, J.; Scott, J.G.; Adams, R.L. Age- and Education-Corrected Independent Normative Data for the Rbans in a Community Dwelling Elderly Sample. Clin. Neuropsychol. 2003, 17, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Beatty, W.W.; Mold, J.W.; Gontkovsky, S.T. Rbans Performance: Influences of Sex and Education. J. Clin. Exp. Neuropsychol. 2003, 25, 1065–1069. [Google Scholar] [CrossRef] [PubMed]
- Nakatsu, D.; Fukuhara, T.; Chaytor, N.S.; Phatak, V.S.; Avellino, A.M. Repeatable Battery for the Assessment of Neuropsychological Status (Rbans) as a Cognitive Evaluation Tool for Patients with Normal Pressure Hydrocephalus. Neurol. Med. Chir. 2016, 56, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohsawa, K.; Nakamura, F.; Uchida, N.; Mizuno, S.; Yokogoshi, H. Lactobacillus Helveticus-Fermented Milk Containing Lactononadecapeptide (Nippltqtpvvvppflqpe) Improves Cognitive Function in Healthy Middle-Aged Adults: A Randomised, Double-Blind, Placebo-Controlled Trial. Int. J. Food Sci. Nutr. 2018, 69, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Marchesan, J.T.; Morelli, T.; Moss, K.; Barros, S.P.; Ward, M.; Jenkins, W.; Aspiras, M.B.; Offenbacher, S. Association of Synergistetes and Cyclodipeptides with Periodontitis. J. Dent. Res. 2015, 94, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.; Liu, F.; Liu, L.J.; Zhang, Z.Y.; Dong, W.X.; Bai, S.; Ma, L.F.; Kang, L.L. Effects of Helicobacter Pylori Infection on the Oral Microbiota of Reflux Esophagitis Patients. Front. Cell. Infect. Microbiol. 2021, 11, 10112268. [Google Scholar] [CrossRef]
- Ruiz, L.; Delgado, S.; Ruas-Madiedo, P.; Sanchez, B.; Margolles, A. Bifidobacteria and Their Molecular Communication with the Immune System. Front. Microbiol. 2017, 8, 02345. [Google Scholar] [CrossRef] [Green Version]
- van Soest, A.P.M.; Hermes, G.D.A.; Berendsen, A.A.M.; van de Rest, O.; Zoetendal, E.G.; Fuentes, S.; Santoro, A.; Franceschi, C.; de Groot, L.C.P.G.M.; de Vos, W.M. Associations between Pro- and Anti-Inflammatory Gastro-Intestinal Microbiota, Diet, and Cognitive Functioning in Dutch Healthy Older Adults: The Nu-Age Study. Nutrients 2020, 12, 3471. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Nguyen, A.; Basson, A.R.; Dark-Fleury, L.; Hsu, K.; Osme, A.; Menghini, P.; Pizarro, T.T.; Cominelli, F. Parabacteroides Distasonis Induces Depressive-Like Behavior in a Mouse Model of Crohn’s Disease. Brain Behav. Immun. 2021, 98, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.M.; Chen, C.; Yu, H.B.; Yang, Z.X. Fecal Microbiota Changes in Patients with Postpartum Depressive Disorder. Front. Cell. Infect. Microbiol. 2020, 10, 567268. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.V.; Loman, B.R.; Bailey, M.T.; Pyter, L.M. Manipulations of the Gut Microbiome Alter Chemotherapy-Induced Inflammation and Behavioral Side Effects in Female Mice. Brain Behav. Immun. 2021, 95, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Olson, C.A.; Iniguez, A.J.; Yang, G.E.; Fang, P.; Pronovost, G.N.; Jameson, K.G.; Rendon, T.K.; Paramo, J.; Barlow, J.T.; Ismagilov, R.F.; et al. Alterations in the Gut Microbiota Contribute to Cognitive Impairment Induced by the Ketogenic Diet and Hypoxia. Cell Host Microbe 2021, 29, 1378–1392. [Google Scholar] [CrossRef]
- Fleury, V.; Zekeridou, A.; Lazarevic, V.; Gaia, N.; Giannopoulou, C.; Genton, L.; Cancela, J.; Girard, M.; Goldstein, R.; Bally, J.F.; et al. Oral Dysbiosis and Inflammation in Parkinson’s Disease. J. Park. Dis. 2021, 11, 619–631. [Google Scholar] [CrossRef]
- Yi, Y.; Shen, L.; Shi, W.; Xia, F.; Zhang, H.; Wang, Y.; Zhang, J.; Wang, Y.; Sun, X.; Zhang, Z.; et al. Gut Microbiome Components Predict Response to Neoadjuvant Chemoradiotherapy in Patients with Locally Advanced Rectal Cancer: A Prospective, Longitudinal Study. Clin. Cancer Res. 2021, 27, 1329–1340. [Google Scholar] [CrossRef]
- Yuan, X.M.; Chen, B.Q.; Duan, Z.L.; Xia, Z.Q.; Ding, Y.; Chen, T.; Liu, H.Z.; Wang, B.S.; Yang, B.L.; Wang, X.Y.; et al. Depression and Anxiety in Patients with Active Ulcerative Colitis: Crosstalk of Gut Microbiota, Metabolomics and Proteomics. Gut Microbes 2021, 13, 1987775. [Google Scholar] [CrossRef]
- Sun, H.R.; Zhao, F.Y.; Liu, Y.Y.; Ma, T.; Jin, H.; Quan, K.Y.; Leng, B.; Zhao, J.W.; Yuan, X.L.; Li, Z.G.; et al. Probiotics Synergized with Conventional Regimen in Managing Parkinson’s Disease. NPJ Park. Dis. 2022, 8, 62. [Google Scholar] [CrossRef]
- Li, J.J.; Ma, Y.L.; Bao, Z.W.; Gui, X.H.; Li, A.N.; Yang, Z.L.; Li, M.D. Clostridiales Are Predominant Microbes That Mediate Psychiatric Disorders. J. Psychiatr. Res. 2020, 130, 48–56. [Google Scholar] [CrossRef]
- Miller, D.P.; Scott, D.A. Inherently and Conditionally Essential Protein Catabolism Genes of Porphyromonas Gingivalis. Trends Microbiol. 2021, 29, 54–64. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BB68S | Placebo | p-Value | |
|---|---|---|---|
| Age (years) | 64.10 ± 3.40 | 64.50 ± 3.79 | 0.67 1 |
| Sex | |||
| Male (%) | 12 (40) | 13 (43) | 0.77 2 |
| Female Male (%) | 18 (60) | 17 (57) | |
| Height (cm) | 164.79 ± 8.18 | 165.09 ± 9.05 | 0.89 1 |
| Weight (kg) | 67.13 ± 13.50 | 67.21 ± 12.50 | 0.98 1 |
| BMI (kg/m2) | 24.55 ± 3.47 | 24.49 ± 3.03 | 0.95 1 |
| Education | |||
| Elementary or less | 10 | 10 | |
| Junior-high school | 13 | 12 | |
| High school or more | 7 | 8 | |
| MoCA total score | 23.03 ± 2.50 | 22.97 ± 2.43 | 0.92 1 |
| RBANS total score | 186.90 ± 17.22 | 186.93 ± 15.62 | 0.99 1 |
| Baseline | Week 8 | |||||
|---|---|---|---|---|---|---|
| Placebo (n = 25) | BB68S (n = 25) | Placebo (n = 25) | BB68S (n = 25) | Difference (95% CI) | p-Value | |
| Total score | 185.88 ± 16.77 | 186.88 ± 18.32 | 201.96 ± 17.14 | 221.72 ± 16.20 | 18.89 (14.98 to 22.80) | <0.0001 |
| Immediate memory | 31.56 ± 5.03 | 32.20 ± 5.69 | 35.28 ± 5.09 | 40.12 ± 4.35 | 4.36 (2.95 to 5.76) | <0.0001 |
| List learning | 20.28 ± 3.03 | 20.84 ± 3.82 | 22.56 ± 3.19 | 25.52 ± 4.00 | 2.49 (1.24 to 3.74) | <0.0001 |
| Story memory | 11.28 ± 3.54 | 11.36 ± 2.93 | 12.72 ± 3.49 | 14.60 ± 2.06 | 1.82 (0.81 to 2.84) | <0.0001 |
| Visuospatial/Constructional | 30.56 ± 4.08 | 30.68 ± 5.13 | 33.40 ± 3.33 | 35.48 ± 2.35 | 2.01 (1.18 to 2.83) | <0.0001 |
| Figure copy | 16.32 ± 2.69 | 16.48 ± 2.54 | 17.64 ± 2.18 | 19.04 ± 1.02 | 1.33 (0.62 to 2.04) | <0.0001 |
| Line orientation | 14.24 ± 2.85 | 14.20 ± 2.60 | 15.76 ± 2.33 | 16.44 ± 2.22 | 0.71 (0.03 to 1.39) | 0.042 |
| Language | 29.76 ± 3.56 | 30.36 ± 4.39 | 32.08 ± 3.66 | 33.64 ± 3.87 | 1.09 (−0.38 to 2.56) | 0.141 |
| Picture naming | 9.68 ± 0.75 | 9.60 ± 0.91 | 9.92 ± 0.28 | 9.76 ± 0.60 | −0.14 (−0.36 to 0.09) | 0.233 |
| Semantic fluency | 20.08 ± 3.37 | 20.76 ± 3.48 | 22.16 ± 3.65 | 23.88 ± 3.57 | 1.23 (−0.29 to 2.74) | 0.11 |
| Attention | 55.44 ± 9.99 | 55.20 ± 9.80 | 59.56 ± 10.34 | 66.64 ± 8.68 | 7.29 (4.77 to 9.80) | <0.0001 |
| Digit span | 14.16 ± 1.95 | 14.12 ± 1.96 | 14.36 ± 1.85 | 14.44 ± 1.73 | 0.10 (−0.66 to 0.87) | 0.785 |
| Coding | 41.28 ± 9.63 | 41.08 ± 10.21 | 45.20 ± 10.11 | 52.20 ± 8.40 | 7.17 (4.62 to 9.71) | <0.0001 |
| Delayed memory | 38.56 ± 4.91 | 38.44 ± 4.54 | 41.64 ± 5.10 | 45.84 ± 4.17 | 4.28 (2.26 to 6.30) | <0.0001 |
| List recall | 4.96 ± 2.23 | 4.00 ± 2.25 | 6.00 ± 2.18 | 6.60 ± 2.08 | 1.06 (−0.03 to 2.14) | 0.056 |
| List recognition | 18.04 ± 2.17 | 18.28 ± 1.81 | 18.84 ± 1.80 | 18.72 ± 1.67 | −0.25 (−1.03 to 0.54) | 0.526 |
| Story recall | 6.84 ± 1.97 | 7.20 ± 2.10 | 7.44 ± 2.38 | 9.56 ± 2.18 | 1.96 (0.75 to 3.17) | 0.002 |
| Figure recall | 8.72 ± 2.69 | 8.96 ± 2.49 | 9.36 ± 1.91 | 10.96 ± 2.61 | 1.53 (0.29 to 2.77) | 0.017 |
| Baseline | Week 8 | a p-Value | b p-Value | |||
|---|---|---|---|---|---|---|
| Placebo | BB68S | Placebo | BB68S | |||
| Sobs | 229.44 ± 83.66 | 233.96 ± 90.34 | 236.32 ± 73.97 | 241.32 ± 91.81 | 0.76 | 0.67 |
| Ace | 282.86 ± 98.31 | 276.57 ± 106.21 | 278.72 ± 87.53 | 286.95 ± 106.95 | 0.67 | 0.63 |
| Chao | 284.75 ± 97.13 | 273.67 ± 112.03 | 280.71 ± 84.41 | 293.49 ± 114.6 | 0.56 | 0.56 |
| Shannon | 3.28 ± 0.65 | 3.22 ± 0.97 | 3.29 ± 0.59 | 3.22 ± 0.77 | 0.95 | 0.91 |
| Simpson | 0.1 ± 0.07 | 0.14 ± 0.22 | 0.11 ± 0.08 | 0.11 ± 0.09 | 0.77 | 0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, S.; Zhang, Q.; Sang, Y.; Ge, S.; Wang, Q.; Wang, R.; He, J. Probiotic Bifidobacterium longum BB68S Improves Cognitive Functions in Healthy Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2023, 15, 51. https://doi.org/10.3390/nu15010051
Shi S, Zhang Q, Sang Y, Ge S, Wang Q, Wang R, He J. Probiotic Bifidobacterium longum BB68S Improves Cognitive Functions in Healthy Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2023; 15(1):51. https://doi.org/10.3390/nu15010051
Chicago/Turabian StyleShi, Shaoqi, Qi Zhang, Yue Sang, Shaoyang Ge, Qi Wang, Ran Wang, and Jingjing He. 2023. "Probiotic Bifidobacterium longum BB68S Improves Cognitive Functions in Healthy Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 15, no. 1: 51. https://doi.org/10.3390/nu15010051
APA StyleShi, S., Zhang, Q., Sang, Y., Ge, S., Wang, Q., Wang, R., & He, J. (2023). Probiotic Bifidobacterium longum BB68S Improves Cognitive Functions in Healthy Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients, 15(1), 51. https://doi.org/10.3390/nu15010051