
The Impact of Kiwifruit Consumption on the Sleep and Recovery of Elite Athletes
 , ,
, ,
Abstract
:1. Introduction
- To characterise the baseline sleep and recovery levels of elite athletes;
- To assess the impact of kiwifruit supplementation on the sleep and sleep health of elite athletes;
- To reassess the sleep and recovery levels of elite athletes after the 4-week intervention.
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Measures
2.5. The Recovery Stress Questionnaire for Athletes (RESTQ Sport)
2.6. Pittsburgh Sleep Quality Index (PSQI)
2.7. Consensus Sleep Dairy-Core (CSD-C)
2.8. The Regulatory, Satisfaction, Alertness, Timing, Efficiency and Duration (RU-SATED)
2.8.1. Questionnaire
- Regulation: consistent sleep–wake schedule (within 1 h)
- Satisfaction/quality: subjective assessment of ‘good’ or ‘poor’ sleep
- Alertness/sleepiness: ability to maintain waking
- Timing: placement of sleep within the 24 h
- Efficiency: ease of falling asleep and returning to sleep
- Duration: total amount of sleep per 24 h [8].
2.8.2. Kiwifruit Intervention
2.9. Data Analysis
3. Results
3.1. Baseline vs. Post-Intervention (PSQI and RESTQ)
3.1.1. Sleep Quality
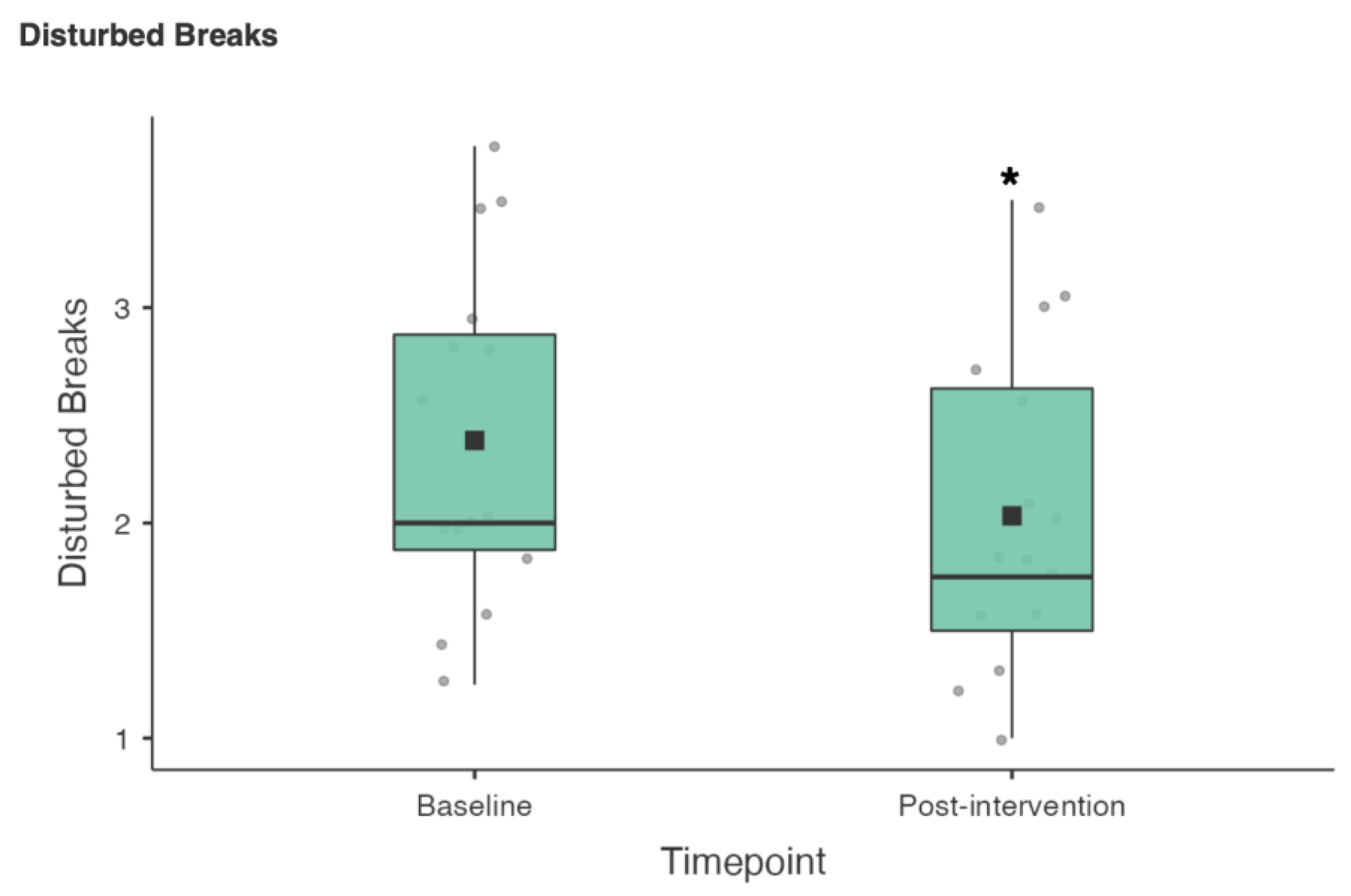
3.1.2. Recovery
3.2. Intervention (Weeks 2–5)
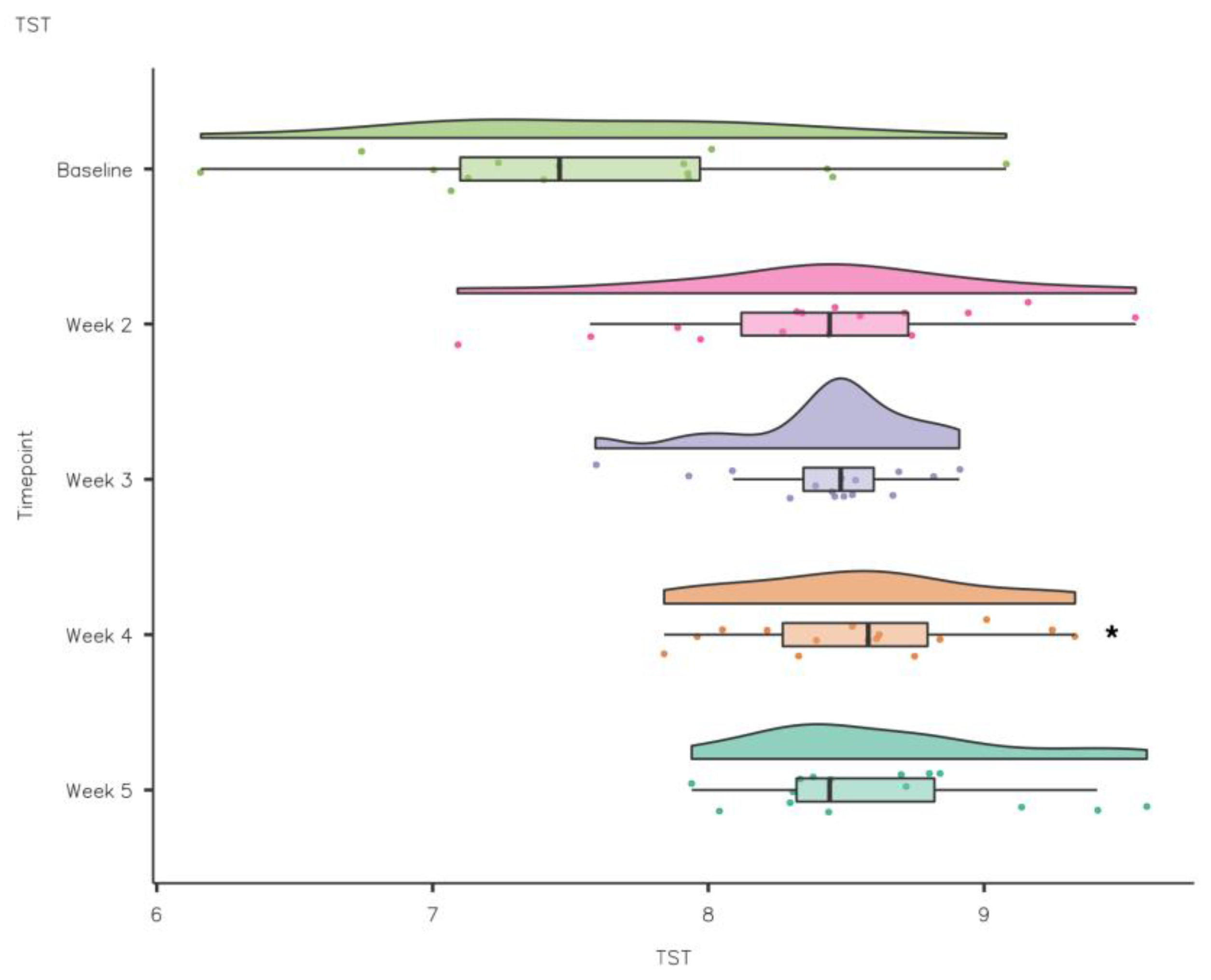
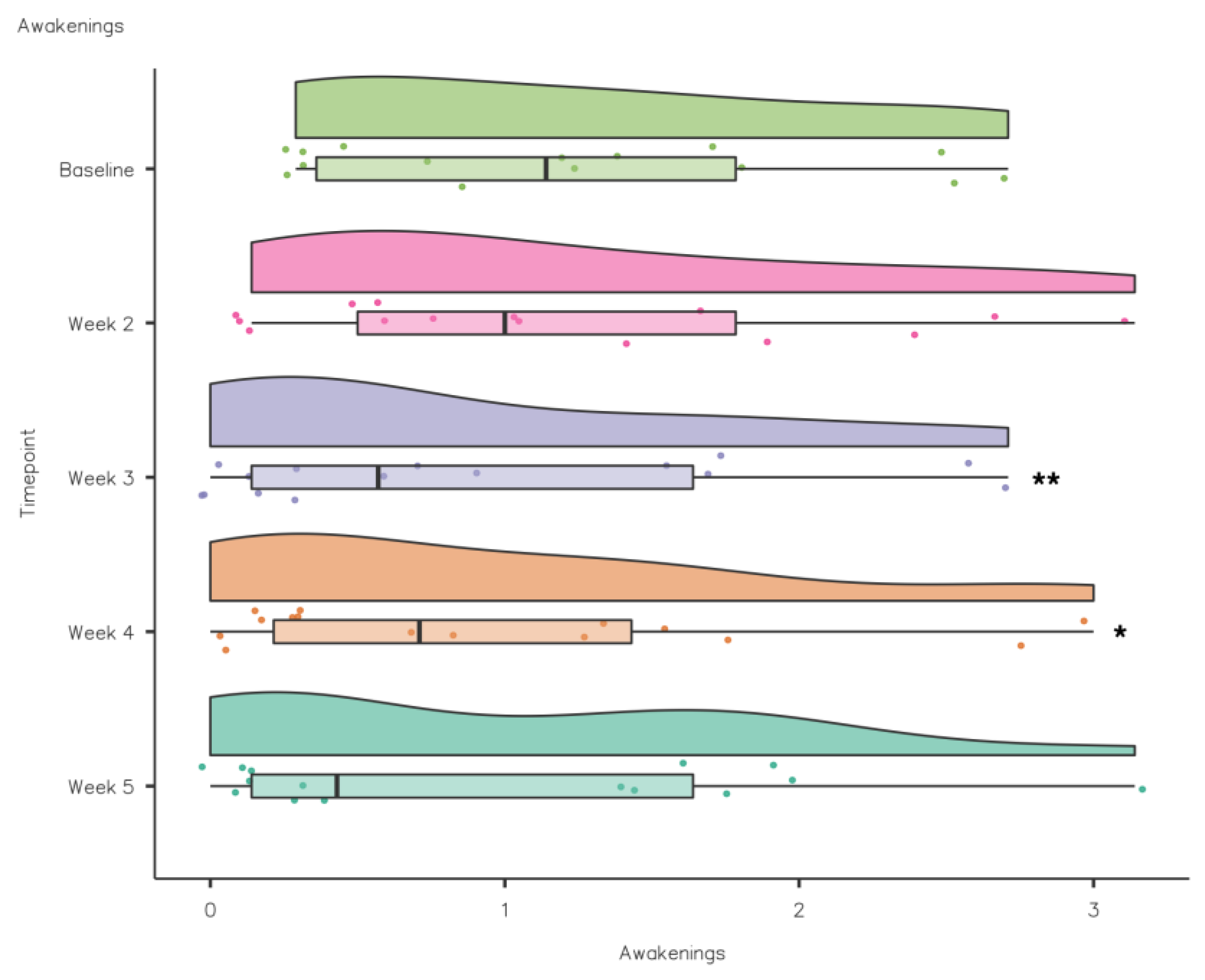
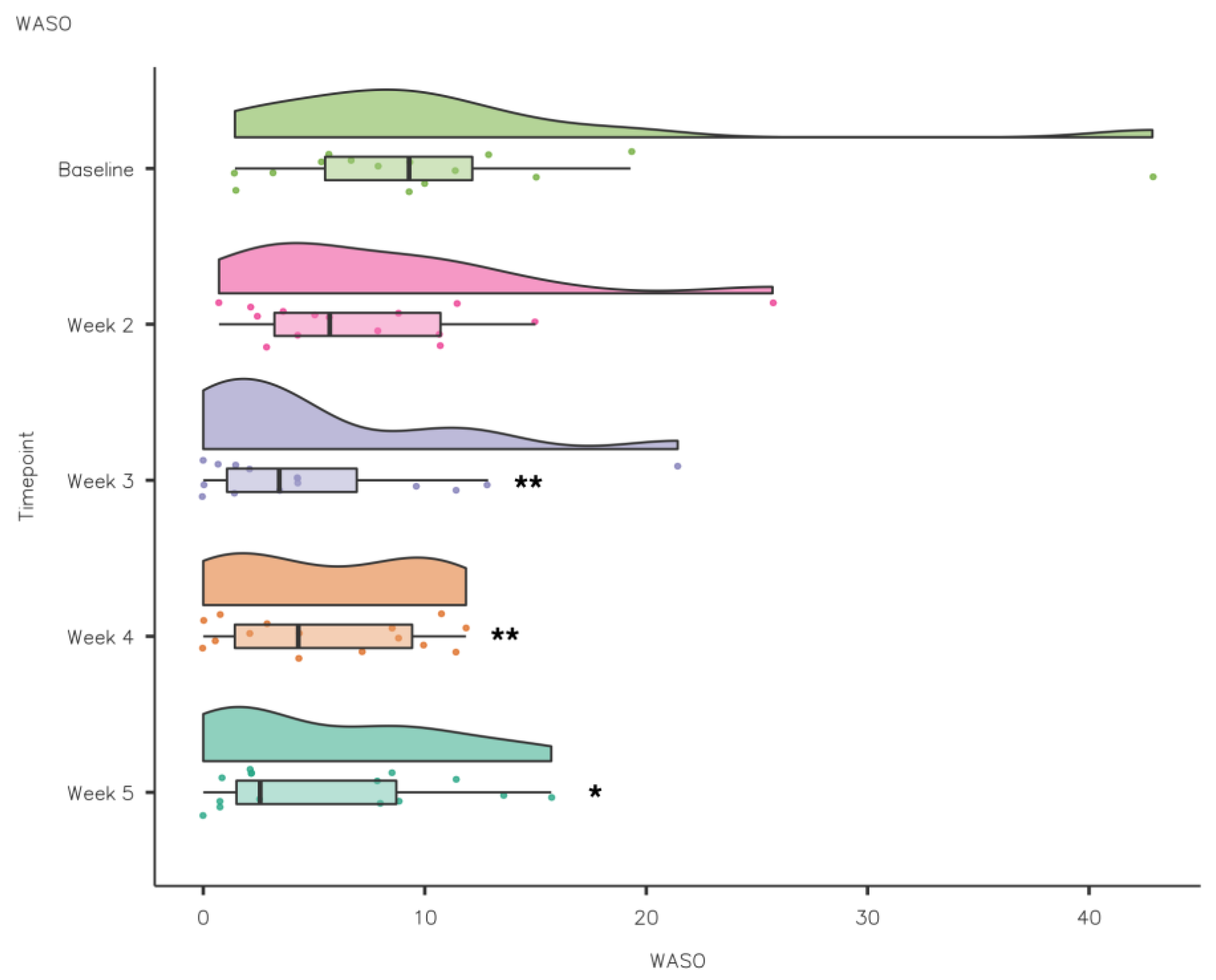
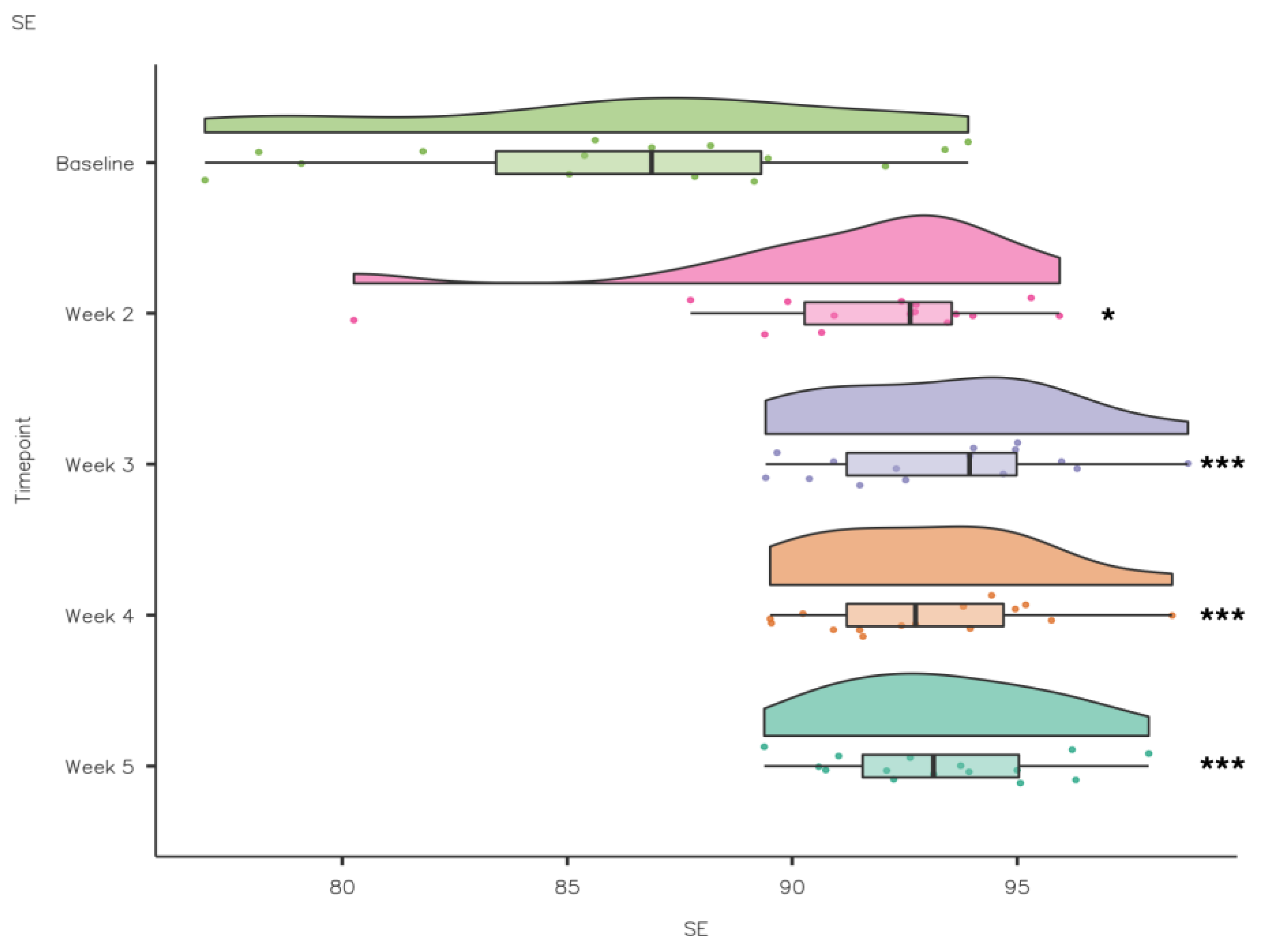
3.2.1. Sleep Diary
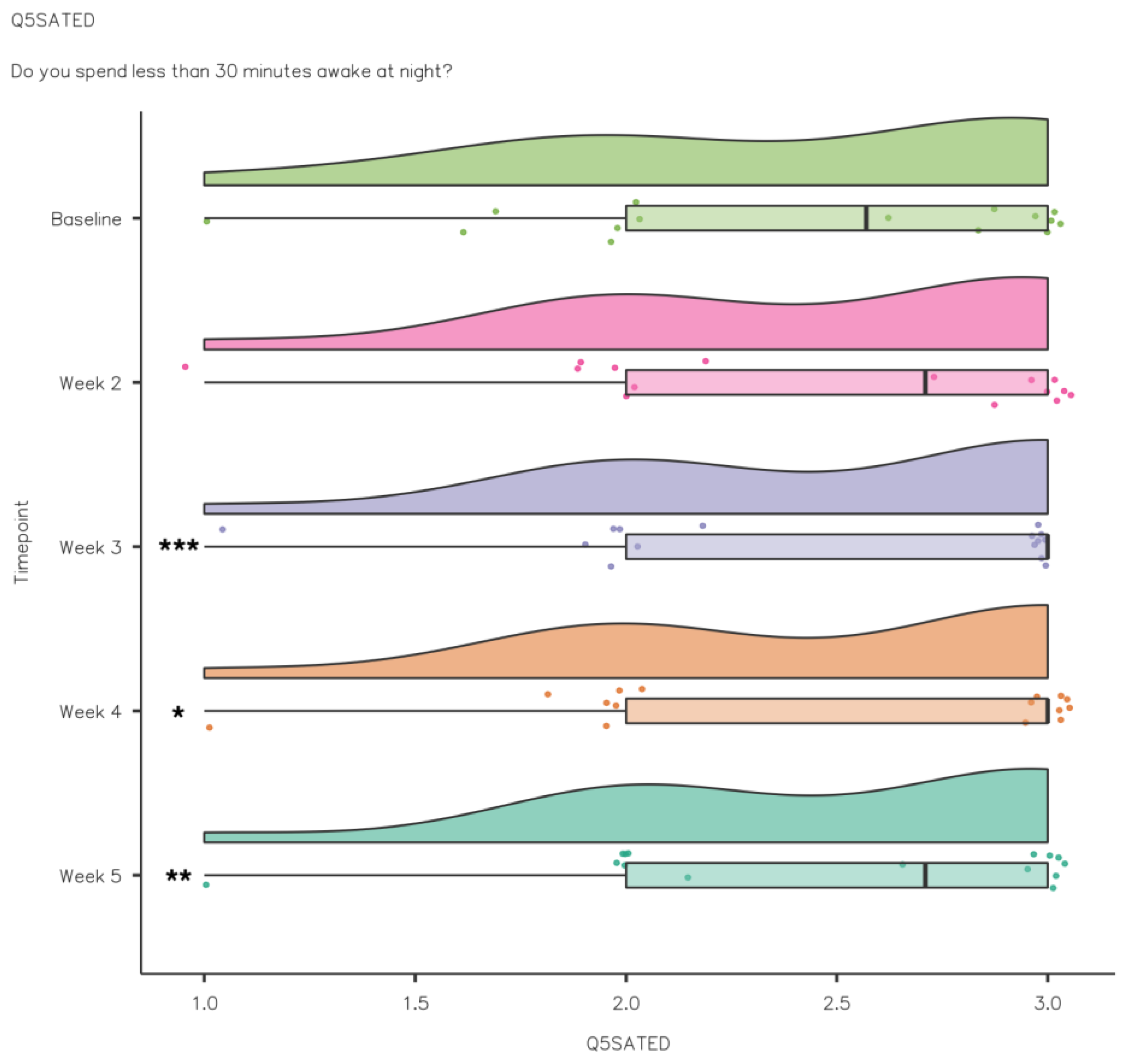
3.2.2. Sleep Health
4. Discussion
4.1. Baseline vs. Post-Intervention Measures
4.1.1. Over the Course of the Intervention—Sleep Diary
4.1.2. Over the Course of the Intervention—Sleep Health
4.2. Limitations
4.3. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, N.P.; Halson, S.L.; Sargent, C.; Roach, G.D.; Nédélec, M.; Gupta, L.; Leeder, J.; Fullagar, H.H.; Coutts, A.J.; Edwards, B.J.; et al. Sleep and the athlete: Narrative review and 2021 expert consensus recommendations. Br. J. Sports Med. 2021, 55, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L. Sleep Monitoring in Athletes: Motivation, methods, miscalculations and why it matters. Sports Med. 2019, 49, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Sargent, C.; Lastella, M.; Halson, S.L.; Roach, G.D. The impact of training schedules on the sleep and fatigue of elite athletes. Chronobiol. Int. 2014, 31, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- Juliff, L.E.; Halson, S.L.; Peiffer, J.J. Understanding sleep disturbance in athletes prior to important competitions. J. Sci. Med. Sport 2015, 18, 13–18. [Google Scholar] [CrossRef]
- Erlacher, D.; Ehrlenspiel, F.; Adegbesan, O.A.; El-Din, H.G. Sleep habits in German athletes before important competitions or games. J. Sports Sci. 2011, 29, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Biggins, M.; Purtill, H.; Fowler, P.; Bender, A.; Sullivan, K.O.; Samuels, C.; Cahalan, R. Sleep, health, and well-being in elite athletes from different sports, before, during, and after international competition. Physician Sports Med. 2021, 49, 437. [Google Scholar] [CrossRef]
- Fowler, P.M.; Duffield, R.; Morrow, I.; Roach, G.; Vaile, J. Effects of sleep hygiene and artificial bright light interventions on recovery from simulated international air travel. Eur. J. Appl. Physiol. 2015, 115, 541–553. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef]
- Hale, L.; Troxel, W.; Buysse, D.J. Sleep Health: An Opportunity for Public Health to Address Health Equity. Annu. Rev. Public Health 2020, 41, 81–89. [Google Scholar] [CrossRef]
- Gupta, L.; Morgan, K.; Gilchrist, S. Does elite sport degrade sleep quality? A systematic review. Sports Med. 2017, 47, 1317–1333. [Google Scholar] [CrossRef]
- Lewis, N.A.; Collins, D.; Pedlar, C.R.; Rogers, J.P. Can clinicians and scientists explain and prevent unexplained underperformance syndrome in elite athletes: An interdisciplinary perspective and 2016 update. BMJ Open Sport Exerc. Med. 2015, 1, e000063. [Google Scholar] [CrossRef]
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Ordóñez, F.M.; Oliver, A.J.S.; Bastos, P.C.; Guillén, L.S.; Domínguez, R. Sleep improvement in athletes: Use of nutritional supplements. Am. J. Sports Med. 2017, 34, 93–99. [Google Scholar]
- Close, G.L.; Hamilton, D.L.; Philip, A.; Burke, L.M.; Morton, J.P. New strategies in sport nutrition to increase exercise performance. Free Radic. Biol. Med. 2016, 98, 144–158. [Google Scholar] [CrossRef]
- Morin, C.M.; Benca, R. Chronic insomnia. Lancet 2012, 379, 1129–1141. [Google Scholar] [CrossRef]
- Lin, H.H.; Tsai, P.S.; Fang, S.C.; Liu, J.F. Effect of Kiwifruit consumption on sleep quality in adults with sleep problems. Asia Pac. J. Clin. Nutr. 2011, 20, 169–174. [Google Scholar] [PubMed]
- Collins, A.R.; Harrington, V.; Drew, J.; Melvin, R. Nutritional modulation of DNA repair in a human intervention study. Carcinogenesis 2003, 24, 511–515. [Google Scholar] [CrossRef]
- Nødtvedt, Ø.O.; Hansen, A.L.; Bjorvatn, B.; Pallesen, S. The effects of kiwi fruit consumption in students with chronic insomnia symptoms: A randomized controlled trial. Sleep Biol. Rhythm. 2017, 15, 159–166. [Google Scholar] [CrossRef]
- Sedgwick, P. What is an open label trial? Br. Med. J. 2014, 23, 348. [Google Scholar] [CrossRef]
- Swann, C.; Moran, A.; Piggott, D. Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychol. Sport Exerc. 2015, 16, 3–14. [Google Scholar] [CrossRef]
- Kellmann, M.; Kallus, K.W. Recovery-Stress Questionnaire for Athletes: User Manual; Human Kinetics: Champaign, IL, USA, 2001. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Venter, R.E. Perceptions of team athletes on the importance of recovery modalities. Eur. J. Sport Sci. 2014, 14, 69–76. [Google Scholar] [CrossRef]
- Maich, K.H.; Lachowski, A.M.; Carney, C.E. Psychometric Properties of the Consensus Sleep Diary in Those with Insomnia Disorder. Behav. Sleep Med. 2018, 16, 117–134. [Google Scholar] [CrossRef]
- Ravyts, S.G.; Dzierzewski, J.M.; Perez, E.; Donovan, E.K.; Dautovich, N.D. Sleep health as measured by RU SATED: A psychometric evaluation. Behav. Sleep Med. 2021, 19, 48–56. [Google Scholar] [CrossRef]
- Thomas, J.R.; Silverman, S.; Nelson, J. Research Methods in Physical Activity, 7th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Knufinke, M.; Nieuwenhuys, A.; Geurts, S.A.; Coenen, A.M.; Kompier, M.A. Self-reported sleep quantity, quality and sleep hygiene in elite athletes. J. Sleep Res. 2018, 27, 78–85. [Google Scholar] [CrossRef]
- Swinbourne, R.; Gill, N.; Vaile, J.; Smart, D. Prevalence of poor sleep quality, sleepiness and obstructive sleep apnoea risk factors in athletes. Eur. J. Sport Sci. 2016, 16, 850–858. [Google Scholar] [CrossRef]
- Samuels, C. Sleep, recovery, and performance: The new frontier in high-performance athletics. Phys. Med. Rehabil. Clin. N. Am. 2008, 20, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Dunican, I.C.; Walsh, J.; Higgins, C.C.; Jones, M.J.; Maddison, K.; Caldwell, J.A.; David, H.; Eastwood, P.R. Prevalence of sleep disorders and sleep problems in an elite super Rugby union team. J. Sports Sci. 2019, 37, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Bender, A.M.; Van Dongen, H.; Samuels, C.H. Sleep Quality and Chronotype Differences between Elite Athletes and Non-Athlete Controls. Clocks Sleep 2019, 1, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Leeder, J.; Glaister, M.; Pizzoferro, K.; Dawson, J.; Pedlar, C. Sleep duration and quality in elite athletes measured using wristwatch actigraphy. J. Sports Sci. 2012, 30, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Jarraya, S.; Jarraya, M.; Chtourou, H.; Souissi, N. Effect of time of day and partial sleep deprivation on the reaction time and the attentional capacities of the handball goalkeeper. Biol. Rhythm Res. 2014, 45, 183–191. [Google Scholar] [CrossRef]
- Reyner, L.A.; Horne, J.A. Sleep restriction and serving accuracy in performance tennis players, and effects of caffeine. Physiol. Behav. 2013, 120, 93–96. [Google Scholar] [CrossRef]
- Edwards, B.J.; Waterhouse, J. Effects of one night of partial sleep deprivation upon diurnal rhythms of accuracy and consistency in throwing darts. Chronobiol. Int. 2009, 26, 756–768. [Google Scholar] [CrossRef]
- Penttilä, E.; Vuorinen, V.P.; Kivimäki, M.; Ahlberg, J.; Airaksinen, O.; Tuomilehto, H. Comparison of sleep between youth elite amateur athletes and professional athletes. Sport Sci. Health 2022, 18, 107–113. [Google Scholar] [CrossRef]
- Rexroat, R. NCAA National Study of Substance Use Habits of College Student-Athletes; National Collegiate Athletic Association (NCAA): Indianapolis, IN, USA, 2014; pp. 1–101. [Google Scholar]
- Grobbelaar, H.W.; Malan, D.D.; Steyn, B.J.; Ellis, S.M. Factors affecting the recovery-stress, burnout and mood state scores of elite student Rugby players. S. Afr. J. Res. Sport Phys. Educ. Recreat. 2010, 32, 41–54. [Google Scholar] [CrossRef]
- Laux, P.; Krumm, B.; Diers, M.; Flor, H. Recovery–stress balance and injury risk in professional football players: A prospective study. J. Sports Sci. 2015, 33, 2140–2148. [Google Scholar] [CrossRef]
- Mougin, F.; Bourdin, H.; Simon-Rigaud, M.L.; Didier, J.M.; Toubin, G.; Kantelip, J.P. Effects of a selective sleep deprivation on subsequent anaerobic performance. Int. J. Sports Med. 1996, 17, 115–119. [Google Scholar] [CrossRef]
- Roberts, S.S.; Teo, W.P.; Warmington, S.A. Effects of training and competition on the sleep of elite athletes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 513–522. [Google Scholar] [CrossRef]
- Martin, B.J. Effect of sleep deprivation on tolerance of prolonged exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1981, 47, 345–354. [Google Scholar] [CrossRef]
- Sargent, C.; Lastella, M.; Halson, S.L.; Roach, G.D. How Much Sleep Does an Elite Athlete Need? Int. J. Sports Physiol. Perform. 2021, 16, 1746–1757. [Google Scholar] [CrossRef] [PubMed]
- Chennaoui, M.; Léger, D.; Gomez-Merino, D. Sleep and the GH/IGF-1 axis: Consequences and countermeasures of sleep loss/disorders. Sleep Med. Rev. 2020, 49, 101–112. [Google Scholar] [CrossRef]
- Simim, M.A.M.; Souza, H.S.; Cardoso Filho, C.A.; Gianoni, R.L.D.S.; Bezerra, R.R.; Affonso, H.O.; Amadio, A.C.; D’Almeida, V.; Serrão, J.C.; Claudino, J.G. Sleep quality monitoring in individual sports athletes: Parameters and definitions by systematic review. Sleep Sci. 2020, 13, 267–285. [Google Scholar] [PubMed]
- Claudino, J.G.; Gabbett, T.J.; de Sá Souza, H.; Simim, M.; Fowler, P.; de Alcantara Borba, D.; Melo, M.; Bottino, A.; Loturco, I.; D’Almeida, V.; et al. Which parameters to use for sleep quality monitoring in team sport athletes? A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000475. [Google Scholar] [CrossRef]
- Lastella, M.; Roach, G.D.; Halson, S.L.; Martin, D.T.; West, N.P.; Sargent, C. Sleep/wake behaviour of endurance cyclists before and during competition. J. Sports Sci. 2015, 33, 293–299. [Google Scholar] [CrossRef]
- Ohayon, M.; Wickwire, E.M.; Hirshkowitz, M.; Albert, S.M.; Avidan, A.; Daly, F.J.; Dauvilliers, Y.; Ferri, R.; Fung, C.; Gozal, D.; et al. National Sleep Foundation’s sleep quality recommendations: First report. Sleep Health 2017, 3, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ortuño, M.M.; Edinger, J.D.; Means, M.K.; Almirall, D. Home is where sleep is: An ecological approach to test the validity of actigraphy for the assessment of insomnia. J. Clin. Sleep Med. 2010, 6, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Simpson, N.S.; Gibbs, E.L.; Matheson, G.O. Optimizing sleep to maximize performance: Implications and recommendations for elite athletes. Scand. J. Med. Sci. Sports 2017, 27, 266–274. [Google Scholar] [CrossRef]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Hammes, D.; Coutts, A.J.; Meyer, T. Sleep and athletic performance: The effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise. Sports Med. 2015, 45, 161–186. [Google Scholar] [CrossRef]
- Shearer, D.A.; Jones, R.M.; Kilduff, L.P.; Cook, C.J. Effects of competition on the sleep patterns of elite Rugby union players. Eur. J. Sport Sci. 2015, 15, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L. Starting at the beginning: An introduction to coefficient alpha and internal consistency. J. Personal. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Benham, G. The Sleep Health Index: Correlations with standardized stress and sleep measures in a predominantly Hispanic college student population. Sleep Health 2019, 5, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2015, 66, 143–172. [Google Scholar] [CrossRef]
- Haugen, T. Key success factors for merging sport science and best practice. Int. J. Sports Physiol. Perform. 2020, 15, 297. [Google Scholar] [CrossRef]
- Caia, J.; Thornton, H.R.; Kelly, V.G.; Scott, T.J.; Halson, S.L.; Cupples, B.; Driller, M.W. Does self-perceived sleep reflect sleep estimated via activity monitors in professional Rugby league athletes? J. Sports Sci. 2018, 36, 1492–1496. [Google Scholar] [CrossRef]
- Dunican, I.C.; Martin, D.T.; Halson, S.L.; Reale, R.J.; Dawson, B.T.; Caldwell, J.A.; Jones, M.J.; Eastwood, P.R. The effects of the removal of electronic devices for 48 hours on sleep in elite judo athletes. J. Strength Cond. Res. 2017, 31, 2832–2839. [Google Scholar] [CrossRef]
- Halson, S.L. Monitoring fatigue and recovery. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef]
- Weiner, D.L.; Balasubramaniam, V.; Shah, S.I.; Javier, J.R. COVID-19 impact on research, lessons learned from COVID-19 research, implications for pediatric research. Pediatr. Res. 2020, 88, 148–150. [Google Scholar] [CrossRef]
- Zehra, A.; Naik, H.R.; Nayik, G.A.; Kour, J.; Bobis, O.; Wani, S.A.; Gull, A.; Pandita, D.; Ganaie, T.A.; Nanda, V.K. Antioxidants in Fruits: Properties and Health Benefits; Nayik, G.A., Gull, A., Eds.; Springer: Singapore, 2020; pp. 547–561. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Sailing | Athletics | |
|---|---|---|---|
| Gender | 15 (M = 9/F = 6) | 9 (M = 7/F = 2) | 6 (M = 2/F = 4) |
| Age (Y) | 23.2 ± 3.9 | 24.56 ± 4 | 21.17 ± 2.93 |
| Body mass (kg) | 70.39 ± 13.34 | 78.89 ± 7.42 *** | 57.65 ± 9.25 |
| Height (cm) | 175.37 ± 8.99 | 179.22 ± 7.31 * | 169.58 ± 8.58 |
| Phase of season | Pre-season n = 10 Competition n = 2 Off-season n = 3 | Pre-season n = 6 Competition n = 1 Off-season n = 2 | Pre-season n = 4 Competition n = 1 Off-season n = 1 |
| Normal training time | 8 a.m. to 5 p.m. n = 14 After 5 p.m. n = 1 | 8 a.m. to 5 p.m. n = 9 | 8 a.m. to 5 p.m. n = 5 After 5 p.m. n = 1 |
| Training/competition duration per week (mins) | 912 ± 359.19 | 636.67 ± 237.8 ** | 1095.56 ± 309.32 |
| Baseline | Post-Intervention | Mean Difference | 95% CI | Effect Size | p-Value | |
|---|---|---|---|---|---|---|
| Sleep Quality | 1.53 ± 0.84 | 0.27 ± 0.46 | 1.27 | 1–2 | 1 | 0.002 ** |
| Sleep Latency | 1.67 ± 0.49 | 1.33 ± 0.62 | 1 | −1.79–1 | 0.46 | 0.18 |
| Sleep duration | 0.34 ± 0.49 | 0.14 ± 0.35 | 1 | −0.02–0.43 | 1 | 0.15 |
| Sleep Efficiency | 0.6 ± 0.91 | 0.2 ± 0.42 | 1.5 | 1–2 | 1 | 0.09 |
| Sleep Disturbance | 1.2 ± 0.56 | 1.2 ± 0.56 | 0 | 0 | 0 | 1 |
| Medication | 0 | 0 | 0 | 0 | 0 | 0 |
| Daytime Dysfunction | 1.13 ± 0.74 | 1 ± 0.54 | 4.31 | −1.98–1 | 0.33 | 0.48 |
| PSQI Global Score | 6.47 ± 2.17 | 4.13 ± 1.19 | 2.5 | 1.5–3.5 | 1 | 0.002 ** |
| Baseline | Post-Intervention | Mean Difference | 95% CI | Effect Size | p-Value | |
|---|---|---|---|---|---|---|
| General Stress | 2.83 ± 1.54 | 2.37 ± 1.01 | 0.5 | −0.13–1.06 | 0.48 | 0.16 |
| Emotional Stress | 2.9 ± 0.95 | 2.47 ± 0.61 | 0.5 | −2.71–1.25 | 0.44 | 0.17 |
| Social Stress | 3.03 ± 1.03 | 2.57 ± 0.84 | 0.75 | −0.5–1.75 | 0.64 | 0.95 |
| Conflicts/Pressure | 3.43 ± 1.31 | 3.17 ± 0.92 | 0.75 | −0.5–1.75 | 0.5 | 0.3 |
| Fatigue | 3.4 ± 1.42 | 2.8 ± 1.21 | 1 | 0.5–1.5 | 0.84 | 0.02 * |
| Lack of Energy | 3.07 ± 1.18 | 2.87 ± 1.09 | 0.5 | −4.26–1 | 0.56 | 0.15 |
| Physical Complaints | 2.37 ± 0.92 | 1.8 ± 0.6 | 0.75 | 0.5–1.25 | 1 | 0.005 ** |
| Success | 3.47 ± 0.9 | 3.73 ± 0.93 | −0.5 | −1.5–0.5 | −0.43 | 0.4 |
| Social Recovery | 4.13 ± 1.1 | 4.43 ± 1.1 | −0.68 | −1.25–0.5 | −0.61 | 0.14 |
| Physical Recovery | 3.53 ± 1.19 | 3.83 ± 1.18 | −0.5 | −1–0.25 | −0.5 | 0.17 |
| General Wellbeing | 4.47 ± 1.27 | 4.5 ± 0.95 | −2.7 | −1.5–1.25 | −0.02 | 1 |
| Sleep Quality | 3.57 ± 1.22 | 4.07 ± 1.35 | −1 | −1.75–0.5 | −0.64 | 0.1 |
| Disturbed Breaks | 2.38 ± 0.8 | 2.03 ± 0.75 | 0.5 | 5.9–0.88 | 0.73 | 0.04 * |
| Emotional Exhaustion | 2.7 ± 1.14 | 2.33 ± 0.98 | 0.5 | −2.3–1 | 0.67 | 0.051 |
| Injury | 3.08 ± 0.68 | 2.8 ± 0.94 | 0.38 | −0.13–0.75 | 0.42 | 0.2 |
| Being in Shape | 4.23 ± 1.25 | 4.4 ± 1.1 | −0.25 | −1–0.5 | −0.37 | 0.33 |
| Personal Accomplishment | 3.58 ± 1.08 | 3.7 ± 1.13 | −0.16 | −0.5–0.38 | −0.35 | 0.3 |
| Self-Efficacy | 3.95 ± 1.27 | 3.93 ± 1.09 | 6.01 | −0.75–0.75 | 0.03 | 0.96 |
| Self-Regulation | 4.33 ± 1.15 | 4.32 ± 0.84 | 0.13 | −0.75–0.88 | 0.13 | 0.77 |
| Baseline | Week 2 | Week 3 | Week 4 | Week 5 | |
|---|---|---|---|---|---|
| SOL (mins) | 24.6 ± 15.9 | 18.8 ± 11 | 14.9 ± 9.51 | 16.1 ± 10.3 | 13.9 ± 8.4 |
| Awakenings | 1.22 ± 0.87 | 1.2 ± 0.98 | 0.89 ± 0.94 ** | 0.95 ± 0.96 * | 0.98 ± 0.96 |
| WASO (mins) | 10.8 ± 10.2 | 7.8 ± 6.45 | 5.15 ± 6.12 ** | 5.56 ± 4.43 ** | 5.68 ± 5.19 * |
| TIB (h) | 8.84 ± 0.75 | 9.18 ± 0.5 | 9.02 ± 0.41 | 9.2 ± 0.54 | 9.24 ± 0.47 |
| TST (h) | 7.6 ± 0.75 | 8.4 ± 0.62 | 8.42 ± 0.34 | 8.55 ± 0.44 * | 8.63 ± 0.47 |
| SE (%) | 86.2 ± 5.31 | 91.5 ± 3.8 * | 93.4 ± 2.7 *** | 93 ± 2.54 *** | 93.3 ± 2.43 *** |
| Fatigue (Bed) | 3.23 ± 0.78 | 3.1 ± 0.58 | 3.28 ± 0.57 | 3.24 ± 0.49 | 3.16 ± 0.69 |
| Fatigue (Morning) | 3.85 ± 1.15 | 3.67 ± 1.08 | 4.03 ± 1.31 | 4.1 ± 1.3 | 3.7 ± 1.24 * |
| Sleep Quality | 3.45 ± 0.74 | 3.48 ± 0.78 | 3.76 ± 0.7 | 3.76 ± 0.68 | 3.58 ± 0.83 |
| Baseline | Week 2 | Week 3 | Week 4 | Week 5 | |
|---|---|---|---|---|---|
| Regulation | 2.6 ± 0.46 | 2.56 ± 0.47 | 2.58 ± 0.48 | 2.62 ± 0.46 | 2.59 ± 0.52 |
| Satisfaction/Quality | 2.33 ± 0.51 | 2.27 ± 0.61 | 2.25 ± 0.68 | 2.3 ± 0.62 | 2.31 ± 0.62 |
| Alertness/Sleepiness | 2.78 ± 0.36 | 2.83 ± 0.31 | 2.88 ± 0.28 | 2.9 ± 0.26 | 2.9 ± 0.27 |
| Timing | 2.98 ± 0.08 | 2.97 ± 0.08 | 2.99 ± 0.04 | 2.98 ± 0.07 | 2.99 ± 0.04 |
| Efficiency | 2.37 ± 0.66 | 2.43 ± 0.63 | 2.47 ± 0.65 *** | 2.46 ± 0.65 * | 2.46 ± 0.62 ** |
| Duration | 2.81 ± 0.36 | 2.75 ± 0.43 | 2.74 ± 0.43 | 2.74 ± 0.45 | 2.74 ± 0.44 |
| Sleep Health Score | 9.88 ± 1.63 | 9.81 ± 1.75 | 9.9 ± 1.65 | 9.97 ± 1.68 | 9.98 ± 1.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doherty, R.; Madigan, S.; Nevill, A.; Warrington, G.; Ellis, J.G. The Impact of Kiwifruit Consumption on the Sleep and Recovery of Elite Athletes. Nutrients 2023, 15, 2274. https://doi.org/10.3390/nu15102274
Doherty R, Madigan S, Nevill A, Warrington G, Ellis JG. The Impact of Kiwifruit Consumption on the Sleep and Recovery of Elite Athletes. Nutrients. 2023; 15(10):2274. https://doi.org/10.3390/nu15102274
Chicago/Turabian StyleDoherty, Rónán, Sharon Madigan, Alan Nevill, Giles Warrington, and Jason Gordon Ellis. 2023. "The Impact of Kiwifruit Consumption on the Sleep and Recovery of Elite Athletes" Nutrients 15, no. 10: 2274. https://doi.org/10.3390/nu15102274
APA StyleDoherty, R., Madigan, S., Nevill, A., Warrington, G., & Ellis, J. G. (2023). The Impact of Kiwifruit Consumption on the Sleep and Recovery of Elite Athletes. Nutrients, 15(10), 2274. https://doi.org/10.3390/nu15102274