
Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Guidance
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Search Strategy
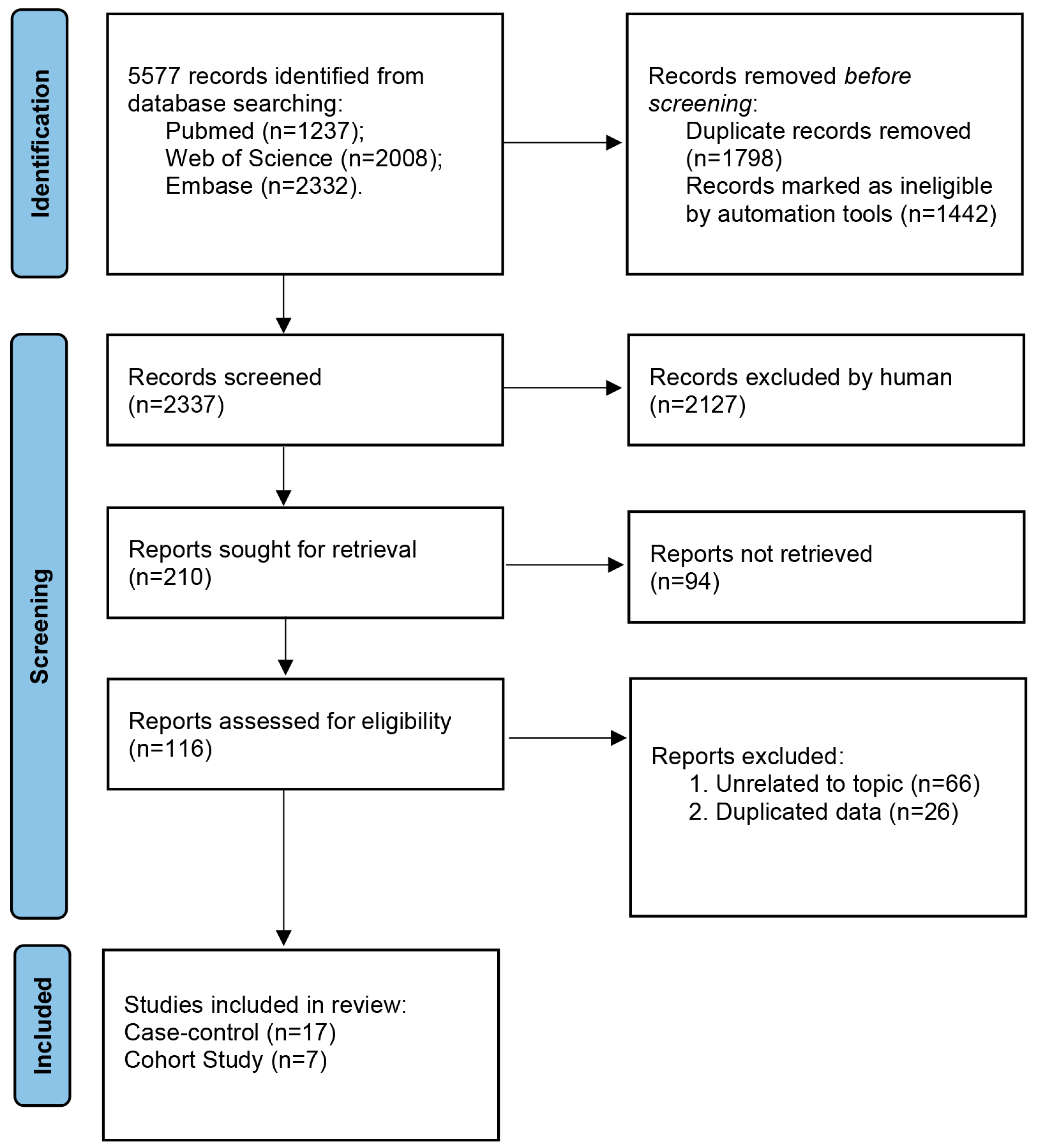
2.5. Study Selection and Data Collection
2.6. Quality Assessment of Evidence
2.7. Statistical Analysis
2.7.1. Meta-Analysis
2.7.2. Subgroup Analysis
2.7.3. Dose–Response Analysis
2.7.4. Risk of Publication Bias and Sensitivity Analysis
3. Results
3.1. Characteristics of the Studies
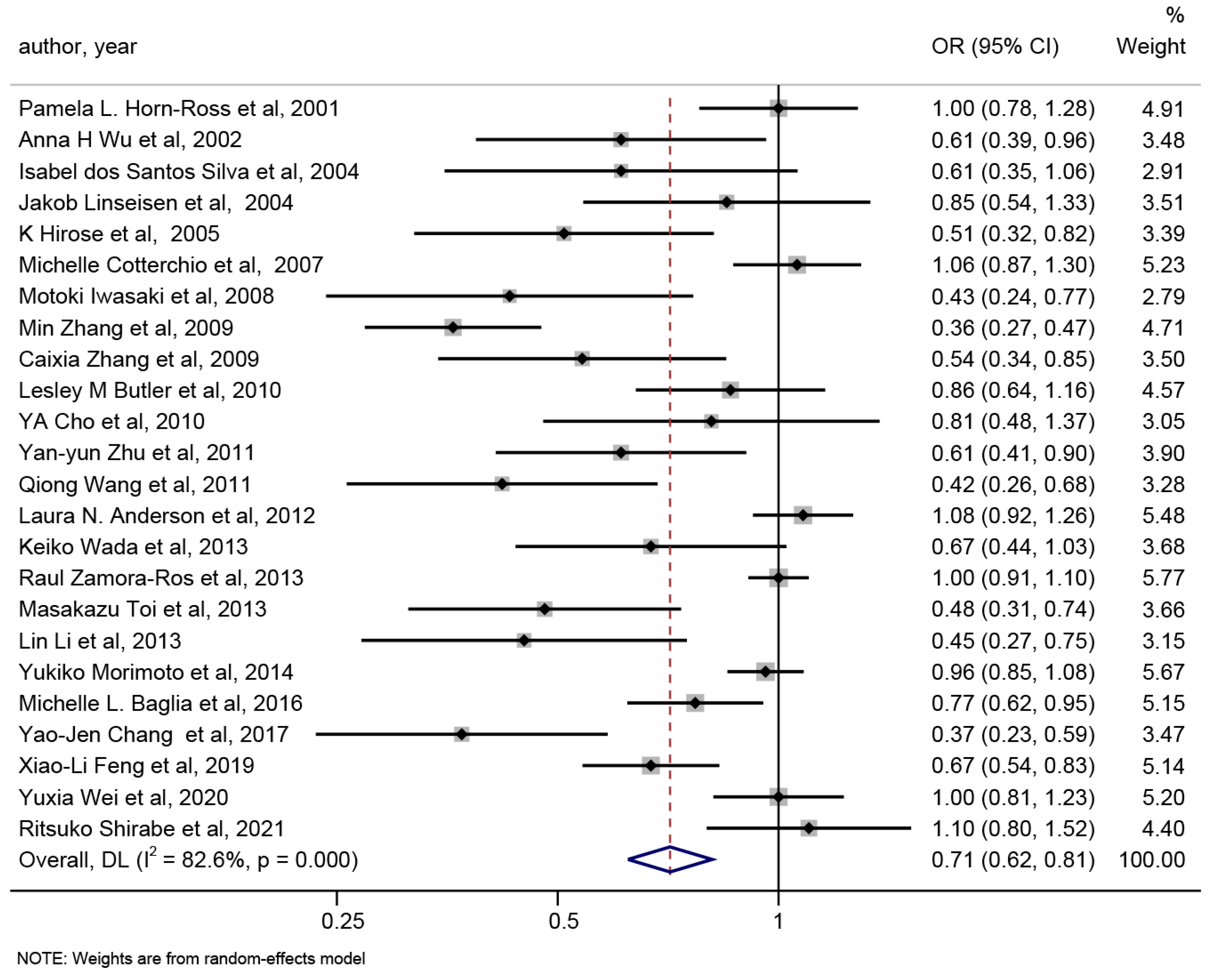
3.2. Meta-Analysis of Isoflavone Consumption and Risk of Breast Cancer
3.3. Subgroup Analysis of Isoflavone Consumption and the Risk of Breast Cancer
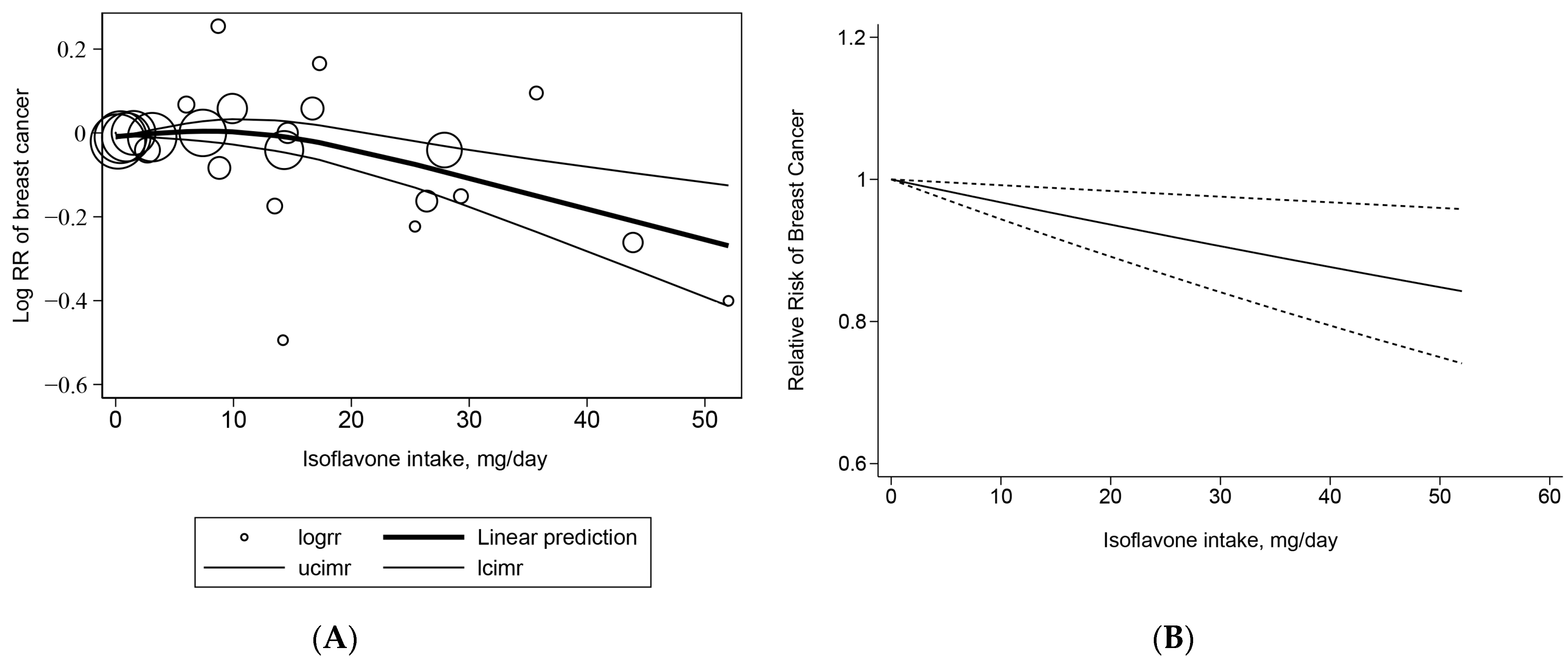
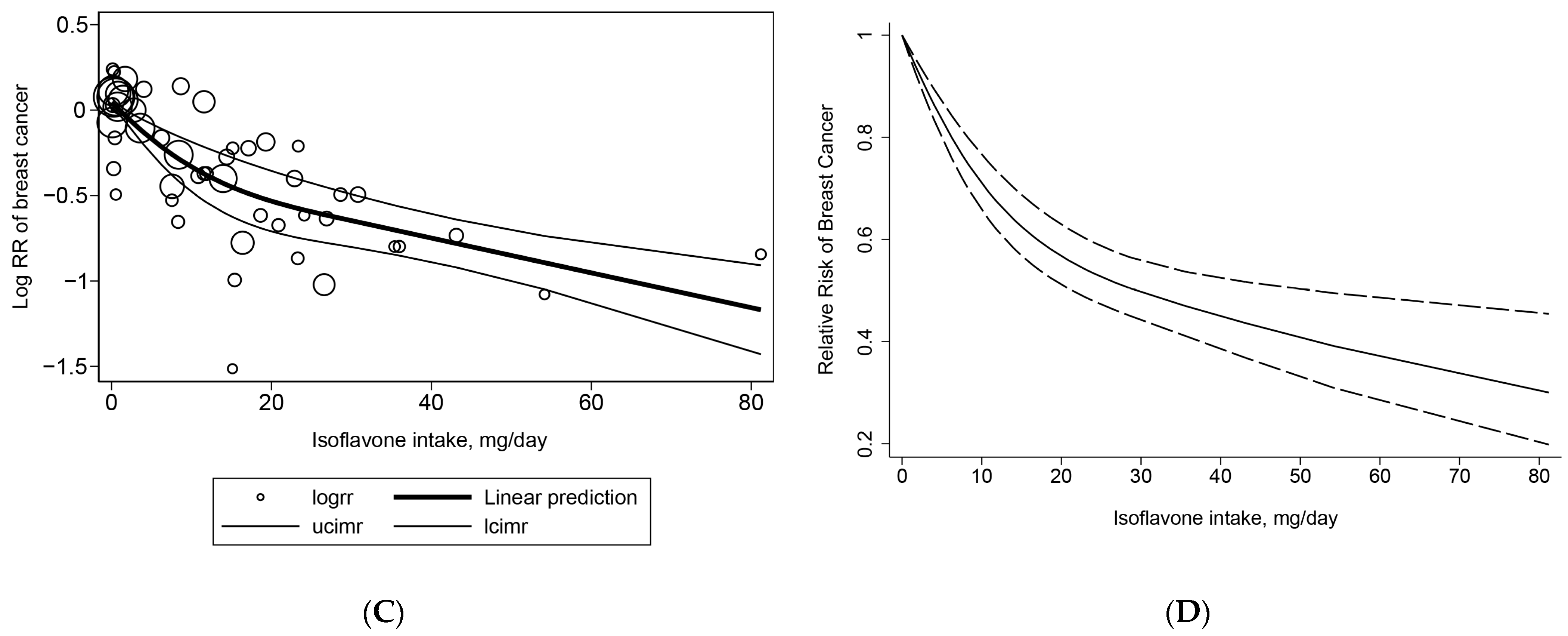
3.4. Dose–Response Meta-Analysis of Isoflavone Consumption and the Risk of Breast Cancer
3.5. Risk of Publication Bias
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Soerjomataram, I.; Bray, F. Planning for tomorrow: Global cancer incidence and the role of prevention 2020–2070. Nat. Rev. Clin. Oncol. 2021, 18, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Winters, S.; Martin, C.; Murphy, D.; Shokar, N.K. Chapter One—Breast Cancer Epidemiology, Prevention, and Screening. In Progress in Molecular Biology and Translational Science; Lakshmanaswamy, R., Ed.; Academic Press: Cambridge, MA, USA, 2017; Volume 151, pp. 1–32. [Google Scholar]
- Kim, I.S. Current Perspectives on the Beneficial Effects of Soybean Isoflavones and Their Metabolites for Humans. Antioxidants 2021, 10, 1064. [Google Scholar] [CrossRef] [PubMed]
- Cotterchio, M.; Boucher, B.A.; Kreiger, N.; Mills, C.A.; Thompson, L.U. Dietary phytoestrogen intake--lignans and isoflavones--and breast cancer risk (Canada). Cancer Causes Control 2008, 19, 259–272. [Google Scholar] [CrossRef]
- Zhu, Y.-Y.; Zhou, L.; Jiao, S.-C.; Xu, L.-Z. Relationship Between Soy Food Intake and Breast Cancer in China. Asian Pac. J. Cancer Prev. 2011, 12, 2837–2840. [Google Scholar]
- Zamora-Ros, R.; Ferrari, P.; Gonzalez, C.A.; Tjonneland, A.; Olsen, A.; Bredsdorff, L.; Overvad, K.; Touillaud, M.; Perquier, F.; Fagherazzi, G.; et al. Dietary flavonoid and lignan intake and breast cancer risk according to menopause and hormone receptor status in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. Breast Cancer Res. Treat. 2013, 139, 163–176. [Google Scholar] [CrossRef]
- Baglia, M.L.; Zheng, W.; Li, H.; Yang, G.; Gao, J.; Gao, Y.T.; Shu, X.O. The association of soy food consumption with the risk of subtype of breast cancers defined by hormone receptor and HER2 status. Int. J. Cancer 2016, 139, 742–748. [Google Scholar] [CrossRef]
- Wei, Y.; Lv, J.; Guo, Y.; Bian, Z.; Gao, M.; Du, H.; Yang, L.; Chen, Y.; Zhang, X.; Wang, T.; et al. Soy intake and breast cancer risk: A prospective study of 300,000 Chinese women and a dose-response meta-analysis. Eur. J. Epidemiol. 2020, 35, 567–578. [Google Scholar] [CrossRef]
- Zhao, T.T.; Jin, F.; Li, J.G.; Xu, Y.Y.; Dong, H.T.; Liu, Q.; Xing, P.; Zhu, G.L.; Xu, H.; Miao, Z.F. Dietary isoflavones or isoflavone-rich food intake and breast cancer risk: A meta-analysis of prospective cohort studies. Clin. Nutr. 2019, 38, 136–145. [Google Scholar] [CrossRef]
- Okekunle, A.P.; Gao, J.; Wu, X.; Feng, R.; Sun, C. Higher dietary soy intake appears inversely related to breast cancer risk independent of estrogen receptor breast cancer phenotypes. Heliyon 2020, 6, e04228. [Google Scholar] [CrossRef]
- Xie, Q.; Chen, M.L.; Qin, Y.; Zhang, Q.Y.; Xu, H.X.; Zhou, Y.; Mi, M.T.; Zhu, J.D. Isoflavone consumption and risk of breast cancer: A dose-response meta-analysis of observational studies. Asia Pac. J. Clin. Nutr. 2013, 22, 118–127. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Phillips, A.N. Meta-analysis: Principles and procedures. Bmj 1997, 315, 1533–1537. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Symp. Syst. Rev. Beyond Basics 2014. [Google Scholar]
- Ioannidis, J.P.; Patsopoulos, N.A.; Evangelou, E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ 2007, 335, 914–916. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Cook, N.R.; Bergstr?M, A.; Hsieh, C.C. A two-stage hierarchical regression model for meta-analysis of epidemiologic nonlinear dose-response data. Comput. Stat. Data Anal. 2009, 53, 4157–4167. [Google Scholar] [CrossRef]
- Xu, C.; Doi, S.A.R. The robust error meta-regression method for dose-response meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 138–144. [Google Scholar] [CrossRef]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose–response data. Stata J. 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Cro, S.; Morris, T.P.; Kenward, M.G.; Carpenter, J.R. Reference-based sensitivity analysis via multiple imputation for longitudinal trials with protocol deviation. Stata J. 2016, 16, 443–463. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Horn-Ross, P.L.; John, E.M.; Lee, M.; Stewart, S.L.; Koo, J.; Sakoda, L.C.; Shiau, A.C.; Goldstein, J.; Davis, P.; Perez-Stable, E.J. Phytoestrogen consumption and breast cancer risk in a multiethnic population: The Bay Area Breast Cancer Study. Am. J. Epidemiol. 2001, 154, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Wan, P.; Hankin, J.; Tseng, C.C.; Yu, M.C.; Pike, M.C. Adolescent and adult soy intake and risk of breast cancer in Asian-Americans. Carcinogenesis 2002, 23, 1491–1496. [Google Scholar] [CrossRef]
- dos Santos Silva, I.; Mangtani, P.; McCormack, V.; Bhakta, D.; McMichael, A.J.; Sevak, L. Phyto-oestrogen intake and breast cancer risk in South Asian women in England: Findings from a population-based case-control study. Cancer Causes Control 2004, 15, 805–818. [Google Scholar] [CrossRef]
- Linseisen, J.; Piller, R.; Hermann, S.; Chang-Claude, J.; German Case-Control, S. Dietary phytoestrogen intake and premenopausal breast cancer risk in a German case-control study. Int. J. Cancer 2004, 110, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Hirose, K.; Imaeda, N.; Tokudome, Y.; Goto, C.; Wakai, K.; Matsuo, K.; Ito, H.; Toyama, T.; Iwata, H.; Tokudome, S.; et al. Soybean products and reduction of breast cancer risk: A case-control study in Japan. Br. J. Cancer 2005, 93, 15–22. [Google Scholar] [CrossRef]
- Iwasaki, M.; Hamada, G.S.; Nishimoto, I.N.; Netto, M.M.; Motola, J., Jr.; Laginha, F.M.; Kasuga, Y.; Yokoyama, S.; Onuma, H.; Nishimura, H.; et al. Dietary isoflavone intake and breast cancer risk in case-control studies in Japanese, Japanese Brazilians, and non-Japanese Brazilians. Breast Cancer Res. Treat. 2009, 116, 401–411. [Google Scholar] [CrossRef]
- Zhang, M.; Yang, H.; Holman, C.D. Dietary intake of isoflavones and breast cancer risk by estrogen and progesterone receptor status. Breast Cancer Res. Treat. 2009, 118, 553–563. [Google Scholar] [CrossRef]
- Cho, Y.A.; Kim, J.; Park, K.S.; Lim, S.Y.; Shin, A.; Sung, M.K.; Ro, J. Effect of dietary soy intake on breast cancer risk according to menopause and hormone receptor status. Eur. J. Clin. Nutr. 2010, 64, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Ho, S.C.; Lin, F.; Cheng, S.; Fu, J.; Chen, Y. Soy product and isoflavone intake and breast cancer risk defined by hormone receptor status. Cancer Sci. 2010, 101, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, H.; Tao, P.; Wang, Y.P.; Yuan, P.; Yang, C.X.; Li, J.Y.; Yang, F.; Lee, H.; Huang, Y. Soy isoflavones, CYP1A1, CYP1B1, and COMT polymorphisms, and breast cancer: A case-control study in southwestern China. DNA Cell Biol. 2011, 30, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.N.; Cotterchio, M.; Boucher, B.A.; Kreiger, N. Phytoestrogen intake from foods, during adolescence and adulthood, and risk of breast cancer by estrogen and progesterone receptor tumor subgroup among Ontario women. Int. J. Cancer 2013, 132, 1683–1692. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, M.; Holman, C.D. Population versus hospital controls in the assessment of dietary intake of isoflavone for case-control studies on cancers in China. Nutr. Cancer 2013, 65, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Toi, M.; Hirota, S.; Tomotaki, A.; Sato, N.; Hozumi, Y.; Anan, K.; Nagashima, T.; Tokuda, Y.; Masuda, N.; Ohsumi, S.; et al. Probiotic Beverage with Soy Isoflavone Consumption for Breast Cancer Prevention: A Case-control Study. Curr. Nutr. Food Sci. 2013, 9, 194–200. [Google Scholar] [CrossRef]
- Chang, Y.J.; Hou, Y.C.; Chen, L.J.; Wu, J.H.; Wu, C.C.; Chang, Y.J.; Chung, K.P. Is vegetarian diet associated with a lower risk of breast cancer in Taiwanese women? BMC Public Health 2017, 17, 800. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Ho, S.C.; Mo, X.F.; Lin, F.Y.; Zhang, N.Q.; Luo, H.; Zhang, X.; Zhang, C.X. Association between flavonoids, flavonoid subclasses intake and breast cancer risk: A case-control study in China. Eur. J. Cancer Prev. 2020, 29, 493–500. [Google Scholar] [CrossRef]
- Butler, L.M.; Wu, A.H.; Wang, R.; Koh, W.P.; Yuan, J.M.; Yu, M.C. A vegetable-fruit-soy dietary pattern protects against breast cancer among postmenopausal Singapore Chinese women. Am. J. Clin. Nutr. 2010, 91, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Nakamura, K.; Tamai, Y.; Tsuji, M.; Kawachi, T.; Hori, A.; Takeyama, N.; Tanabashi, S.; Matsushita, S.; Tokimitsu, N.; et al. Soy isoflavone intake and breast cancer risk in Japan: From the Takayama study. Int. J. Cancer 2013, 133, 952–960. [Google Scholar] [CrossRef]
- Morimoto, Y.; Maskarinec, G.; Park, S.Y.; Ettienne, R.; Matsuno, R.K.; Long, C.; Steffen, A.D.; Henderson, B.E.; Kolonel, L.N.; Le Marchand, L.; et al. Dietary isoflavone intake is not statistically significantly associated with breast cancer risk in the Multiethnic Cohort. Br. J. Nutr. 2014, 112, 976–983. [Google Scholar] [CrossRef]
- Shirabe, R.; Saito, E.; Sawada, N.; Ishihara, J.; Takachi, R.; Abe, S.K.; Shimazu, T.; Yamaji, T.; Goto, A.; Iwasaki, M.; et al. Fermented and nonfermented soy foods and the risk of breast cancer in a Japanese population-based cohort study. Cancer Med. 2021, 10, 757–771. [Google Scholar] [CrossRef]
- You, C.P.; Tsoi, H.; Man, E.P.S.; Leung, M.H.; Khoo, U.S. Modulating the Activity of Androgen Receptor for Treating Breast Cancer. Int. J. Mol. Sci. 2022, 23, 15342. [Google Scholar] [CrossRef]
- Islam, M.S.; Afrin, S.; Jones, S.I.; Segars, J. Selective Progesterone Receptor Modulators-Mechanisms and Therapeutic Utility. Endocr. Rev. 2020, 41, bnaa012. [Google Scholar] [CrossRef]
- Khan, S.A.; Chatterton, R.T.; Michel, N.; Bryk, M.; Lee, O.; Ivancic, D.; Heinz, R.; Zalles, C.M.; Helenowski, I.B.; Jovanovic, B.D.; et al. Soy isoflavone supplementation for breast cancer risk reduction: A randomized phase II trial. Cancer Prev. Res. 2012, 5, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Lamartiniere, C.A.; Moore, J.B.; Brown, N.M.; Thompson, R.; Hardin, M.J.; Barnes, S. Genistein suppresses mammary cancer in rats. Carcinogenesis 1995, 16, 2833–2840. [Google Scholar] [CrossRef] [PubMed]
- Thanos, J.; Cotterchio, M.; Boucher, B.A.; Kreiger, N.; Thompson, L.U. Adolescent dietary phytoestrogen intake and breast cancer risk (Canada). Cancer Causes Control 2006, 17, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Touillaud, M.; Gelot, A.; Mesrine, S.; Bennetau-Pelissero, C.; Clavel-Chapelon, F.; Arveux, P.; Bonnet, F.; Gunter, M.; Boutron-Ruault, M.C.; Fournier, A. Use of dietary supplements containing soy isoflavones and breast cancer risk among women aged >50 y: A prospective study. Am. J. Clin. Nutr. 2019, 109, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Beaubernard, L.; Lamothe, V.; Bennetau-Pelissero, C. New Evaluation of Isoflavone Exposure in the French Population. Nutrients 2019, 11, 2308. [Google Scholar] [CrossRef]
- Villares, A.; Rostagno, M.A.; García-Lafuente, A.; Guillamón, E.; Martínez, J.A. Content and Profile of Isoflavones in Soy-Based Foods as a Function of the Production Process. Food Bioprocess Technol. 2011, 4, 27–38. [Google Scholar] [CrossRef]
- Messina, M.; Nagata, C.; Wu, A.H. Estimated Asian adult soy protein and isoflavone intakes. Nutr. Cancer 2006, 55, 1–12. [Google Scholar] [CrossRef]
- Jun, S.; Shin, S.; Joung, H. Estimation of dietary flavonoid intake and major food sources of Korean adults. Br. J. Nutr. 2016, 115, 480–489. [Google Scholar] [CrossRef]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Drewnowski, A. Flavonoid Intakes in the US Diet Are Linked to Higher Socioeconomic Status and to Tea Consumption: Analyses of NHANES 2011-16 Data. J. Nutr. 2020, 150, 2147–2155. [Google Scholar] [CrossRef]
- Sebastian, R.S.; Wilkinson Enns, C.; Goldman, J.D.; Martin, C.L.; Steinfeldt, L.C.; Murayi, T.; Moshfegh, A.J. A New Database Facilitates Characterization of Flavonoid Intake, Sources, and Positive Associations with Diet Quality among US Adults. J. Nutr. 2015, 145, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Jackowiak, H.; Packa, D.; Wiwart, M.; Perkowski, J. Scanning electron microscopy of Fusarium damaged kernels of spring wheat. Int. J. Food Microbiol. 2005, 98, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Constantine, G.D.; Kessler, G.; Graham, S.; Goldstein, S.R. Increased Incidence of Endometrial Cancer Following the Women’s Health Initiative: An Assessment of Risk Factors. J. Womens Health 2019, 28, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Alekel, D.L.; Van Loan, M.D.; Koehler, K.J.; Hanson, L.N.; Stewart, J.W.; Hanson, K.B.; Kurzer, M.S.; Peterson, C.T. The soy isoflavones for reducing bone loss (SIRBL) study: A 3-y randomized controlled trial in postmenopausal women. Am. J. Clin. Nutr. 2010, 91, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Unfer, V.; Casini, M.L.; Costabile, L.; Mignosa, M.; Gerli, S.; Di Renzo, G.C. Endometrial effects of long-term treatment with phytoestrogens: A randomized, double-blind, placebo-controlled study. Fertil. Steril. 2004, 82, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Tai, T.Y.; Tsai, K.S.; Tu, S.T.; Wu, J.S.; Chang, C.I.; Chen, C.L.; Shaw, N.S.; Peng, H.Y.; Wang, S.Y.; Wu, C.H. The effect of soy isoflavone on bone mineral density in postmenopausal Taiwanese women with bone loss: A 2-year randomized double-blind placebo-controlled study. Osteoporos. Int. 2012, 23, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Quaas, A.M.; Kono, N.; Mack, W.J.; Hodis, H.N.; Felix, J.C.; Paulson, R.J.; Shoupe, D. Effect of isoflavone soy protein supplementation on endometrial thickness, hyperplasia, and endometrial cancer risk in postmenopausal women: A randomized controlled trial. Menopause 2013, 20, 840–844. [Google Scholar] [CrossRef]
- Jacobsen, B.K.; Jaceldo-Siegl, K.; Knutsen, S.F.; Fan, J.; Oda, K.; Fraser, G.E. Soy isoflavone intake and the likelihood of ever becoming a mother: The Adventist Health Study-2. Int. J. Womens Health 2014, 6, 377–384. [Google Scholar] [CrossRef]
- Andrews, M.A.; Schliep, K.C.; Wactawski-Wende, J.; Stanford, J.B.; Zarek, S.M.; Radin, R.G.; Sjaarda, L.A.; Perkins, N.J.; Kalwerisky, R.A.; Hammoud, A.O.; et al. Dietary factors and luteal phase deficiency in healthy eumenorrheic women. Hum. Reprod. 2015, 30, 1942–1951. [Google Scholar] [CrossRef]
- Wiseman, H.; Casey, K.; Clarke, D.B.; Barnes, K.A.; Bowey, E. Isoflavone aglycon and glucoconjugate content of high- and low-soy U.K. foods used in nutritional studies. J. Agric. Food Chem. 2002, 50, 1404–1410. [Google Scholar] [CrossRef]
- Setchell, K.D.; Brown, N.M.; Desai, P.; Zimmer-Nechemias, L.; Wolfe, B.E.; Brashear, W.T.; Kirschner, A.S.; Cassidy, A.; Heubi, J.E. Bioavailability of pure isoflavones in healthy humans and analysis of commercial soy isoflavone supplements. J. Nutr. 2001, 131, 1362S–1375S. [Google Scholar] [CrossRef] [PubMed]
- Ju, Y.H.; Fultz, J.; Allred, K.F.; Doerge, D.R.; Helferich, W.G. Effects of dietary daidzein and its metabolite, equol, at physiological concentrations on the growth of estrogen-dependent human breast cancer (MCF-7) tumors implanted in ovariectomized athymic mice. Carcinogenesis 2006, 27, 856–863. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Publication Year | Study Design | Population | Study Period | Case/Subjects | Verification of Breast Cancer | Exposure Range (mg/day) | Variables of Adjustment | Exposure Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Keiko Wada | 2013 | Cohort | Asian | 1992–2008 | 172/15,607 | Cancer registry record | <19.9 vs. >67.4 | 2, 3, 5, 6, 7, 8, 11, 15, 22, 28 | FFQ |
| Lesley M Butler | 2010 | Cohort | Asian | 1993–2005 | 629/34,028 | Histologically confirmed | <4.6 vs. >33.9 | 2, 6, 7, 10, 12, 22, 42, 43 | FFQ |
| Michelle L. Baglia | 2016 | Cohort | Asian | 1996–2011 | 1034/70,578 | Cancer registry record | <11.1 vs. >55 | 2, 5, 7, 8, 10, 12, 22, 28, 44 | FFQ |
| Raul Zamora-Ros | 2013 | Cohort | Non-Asian | 1992–2010 | 11,576/334,850 | Histologically confirmed | <0.22 vs. >1.36 | 2, 3, 5, 7, 8, 9, 11, 12, 13, 15, 20, 22, 28, 33 | FFQ |
| Ritsuko Shirabe | 2021 | Cohort | Asian | 1990–2013 | 825/46,714 | Histologically confirmed | <9.1 vs. >44.8 | 2, 3, 6, 10, 11, 12, 13, 14, 15, 18, 19, 20, 22, 23, 28, 45 | FFQ |
| Yukiko Morimoto | 2014 | Cohort | Non-Asian | 1993–2007 | 4769/84,550 | Cancer registry record | <3.2 vs. >20.3 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16 | FFQ |
| Yuxia Wei | 2020 | Cohort | Asian | 2004–2016 | 2289/300,852 | Cancer registry record | <4.5 vs. >19.1 | 2, 3, 6, 7, 8, 9, 12, 13, 15, 17, 18, 19, 20, 28, 30 | FFQ |
| Yan-yun Zhu | 2011 | Case control | Asian | 2008~2011 | 62/108 | Histologically confirmed | <7.56 vs. >28.83 | 10, 13, 15, 21, 22, 30, 31 | FFQ |
| Min Zhang | 2009 | Case control | Asian | 2004–2005 | 158/410 | Histologically confirmed | <7.78 vs. >25.40 | 2, 3, 7, 8, 9, 10, 12, 13, 15, 22, 23, 24, 28, 31 | FFQ |
| Caixia Zhang | 2009 | Case control | Asian | 2007–2008 | 140/249 | Histologically confirmed | <3.26 vs. >16.89 | 2, 3, 10, 12, 13, 21, 28, 30 | FFQ |
| Anna H Wu | 2002 | Case control | Non-Asian | 1995–1998 | 130/278 | Cancer registry record | <1.79 mg/1000 kcal vs. >12.68 mg/1000 kcal | 2, 3, 7, 8, 10, 11, 13, 15, 22, 25, 26, 27, 28 | FFQ |
| Motoki Iwasaki | 2008 | Case control | Asian | 2001–2006 | 850/1700 | Histologically confirmed | <8.7 vs. >71.3 | 6, 8, 10, 13, 28, 32 | FFQ |
| Pamela L. Horn-Ross | 2001 | Case control | Non-Asian | 1995–1998 | 292/694 | Cancer registry record | <1.048 vs. >2.774 | 1, 2, 3, 6, 7, 8, 10, 11, 12, 19, 21, 22 | FFQ |
| K Hirose | 2005 | Case control | Asian and Non-Asian | 2001–2002 | 36/174 | Histologically confirmed | <7.61 vs. >11.87 | 2, 3, 5, 6, 12, 13, 15, 20, 22, 29, 28 | FFQ |
| Isabel dos Santos Silva | 2004 | Case control | Non-Asian | 1995–1999 | 239/714 | Cancer registry record | <0.125 mg/1862 kcal vs. >0.470 mg/1862 kcal | 3, 5, 7, 10, 19, 20, 26 | FFQ |
| Michelle Cotterchio | 2007 | Case control | Non-Asian | 2002–2003 | 3000/6370 | Histologically confirmed | <0.082 vs. >1.237 | 5, 10, 11, 21, 22, 33 | FFQ |
| Y. A. Cho | 2010 | Case control | Asian | 2007–2008 | 138/257 | Histologically confirmed | <8.5 vs. >23.7 | 2, 3, 6, 7, 8, 10, 11, 12, 13, 15, 22, 28, 34, 35 | FFQ |
| Masakazu Toi | 2013 | Case control | Asian | 2007–2009 | 101/266 | Cancer registry record | <18.76 vs. >43.75 | 3, 6, 7, 10, 11, 12, 19, 20, 21, 22, 28, 36, 46 | FFQ |
| Jakob Linseisen | 2004 | Case control | Non-Asian | 1992–1995 | 278/944 | Histologically confirmed | <0.1737 vs. >0.4147 | 2, 6, 7, 10, 12,13, 19 | FFQ |
| Lin Li | 2013 | Case control | Asian | 2009–2010 | 113/189 | Cancer registry record | <12.49 vs. >35.12 | 6, 7, 8, 9,10, 12, 13, 15, 17, 24, 28, 31, 37, 38 | FFQ |
| Xiao-Li Feng | 2019 | Case control | Asian | 2007–2008 | 456/843 | Histologically confirmed | <3.41 vs. >13.05 | 2, 7, 9, 15, 17, 22, 28, 31 | FFQ |
| Yao-Jen Chang | 2017 | Case control | Asian | 2010–2013 | 233/449 | Cancer registry record | <22 vs. >22 | 22, 28 | FFQ |
| Qiong Wang | 2011 | Case control | Asian | 2007–2009 | 181/299 | Histologically confirmed | <9.95 vs. >23.55 | 2, 5, 9, 12, 13, 19, 39, 40, 41 | FFQ |
| Laura N. Anderson | 2012 | Case control | Non-Asian | 2002–2003 | 476/1587 | Histologically confirmed | <0.122 vs. >0.497 | 5, 10, 11, 21, 22, 33 | FFQ |
| Outcome of Interest | No. of Studies | OR (95% CI) | pheterogenity | I2 (%) | p for Interaction |
|---|---|---|---|---|---|
| Study design | |||||
| Case control | 17 | 0.62 (0.50, 0.76) | 0.000 | 83.8% | 0.000 |
| Cohort | 7 | 0.94 (0.86, 1.02) | 0.178 | 32.7% | |
| Population | |||||
| Non-Asian | 8 | 0.97 (0.88, 1.06) | 0.092 | 43.0% | 0.000 |
| Asian | 18 | 0.62 (0.52, 0.74) | 0.000 | 75.6% | |
| Publication year | |||||
| Before 2010 | 11 | 0.67 (0.52, 0.87) | 0.000 | 81.5% | 0.462 |
| After 2010 | 13 | 0.75 (0.64, 0.87) | 0.000 | 82.3% | |
| Study quality | |||||
| NOS score ≤ 7 | 10 | 0.77 (0.63, 0.93) | 0.000 | 77.4% | 0.362 |
| NOS score > 7 | 14 | 0.68 (0.56, 0.82) | 0.000 | 84.2% | |
| Menopausal status | |||||
| Premenopausal | 16 | 0.76 (0.63, 0.92) | 0.000 | 66.6% | 0.897 |
| Postmenopausal | 16 | 0.75 (0.62, 0.90) | 0.000 | 78.3% | |
| Isoflavone highest intake | |||||
| <10 mg/d | 6 | 1.01 (0.94, 1.08) | 0.452 | 0.0% | 0.000 |
| ≥10 mg/d | 18 | 0.63 (0.53, 0.75) | 0.000 | 81.4% | |
| ER status | |||||
| ER+ | 7 | 0.77 (0.62, 0.95) | 0.000 | 75.7% | 0.981 |
| ER− | 7 | 0.77 (0.52, 1.15) | 0.000 | 84.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Shen, H.; Mi, M.; Qin, Y. Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies. Nutrients 2023, 15, 2402. https://doi.org/10.3390/nu15102402
Yang J, Shen H, Mi M, Qin Y. Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies. Nutrients. 2023; 15(10):2402. https://doi.org/10.3390/nu15102402
Chicago/Turabian StyleYang, Jining, Hui Shen, Mantian Mi, and Yu Qin. 2023. "Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies" Nutrients 15, no. 10: 2402. https://doi.org/10.3390/nu15102402
APA StyleYang, J., Shen, H., Mi, M., & Qin, Y. (2023). Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies. Nutrients, 15(10), 2402. https://doi.org/10.3390/nu15102402