

The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women

 and
and
Abstract
:1. Introduction
2. Materials and Methods
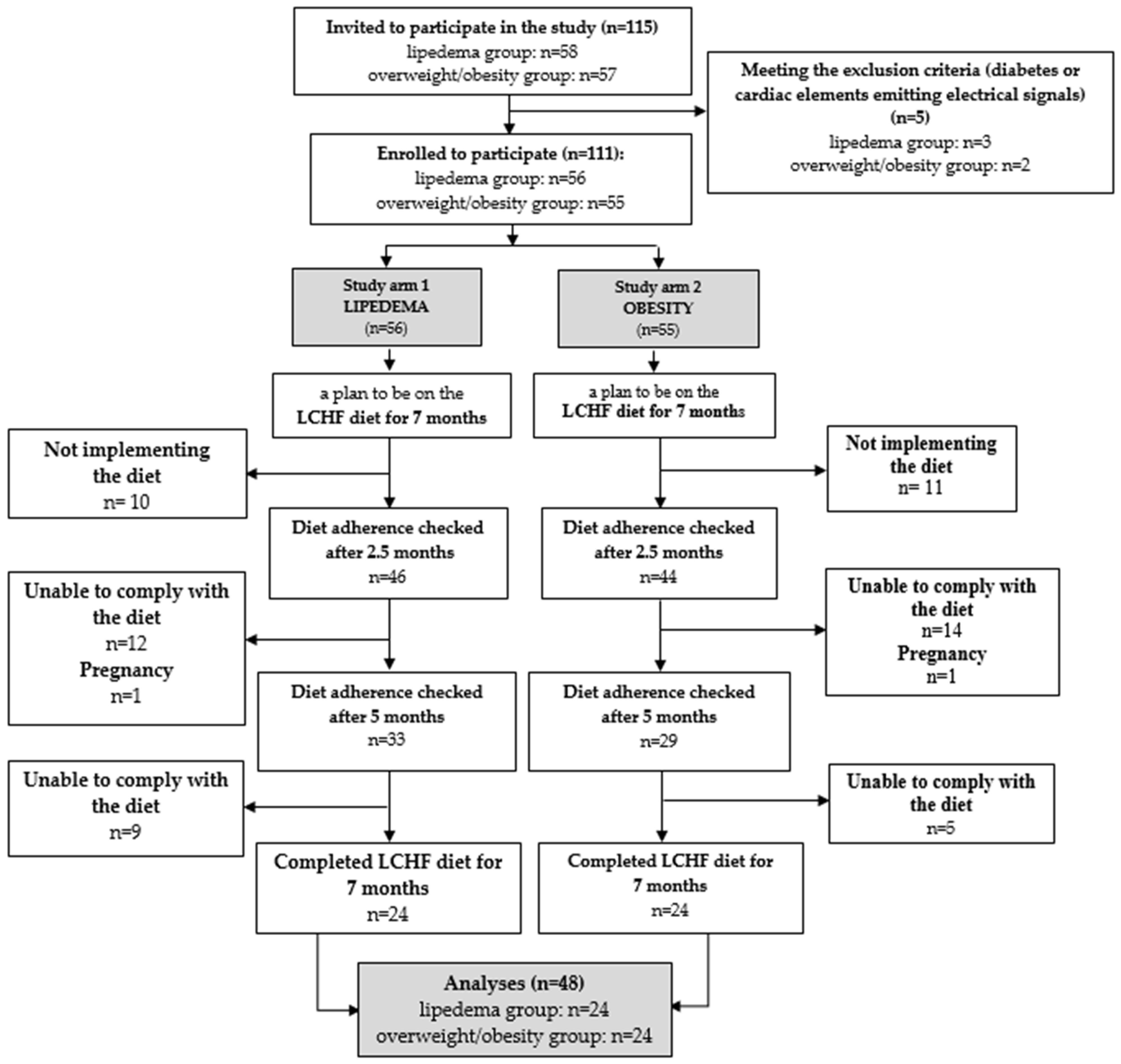
2.1. Study Design and Subjects
2.2. Measurement of Anthropometric Parameters
2.3. Blood Samples
2.4. Dietary Intervention
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Groups
3.2. Anthropometric Measurements
3.3. Diet Composition
3.4. Laboratory Blood Tests Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wounds UK. Best Practice Guidelines: The Management of Lipoedema; Wounds: London, UK, 2017. [Google Scholar]
- Dayan, E.; Kim, J.N.; Smith, M.L.; Seo, C.A.; Damstra, R.J.; Schmeller, W.; Frambach, Y.; Carmody, M.A.; Földi, E.; Rockson, S.G. Lipedema—The Disease They Call Fat; The Lipedema Project at The Friedman Center for Lymphedema Research and Treatment in Collaboration with Lymphatic Education & Research Network (LE&RN); LE&RN: New York, NY, USA, 2017. [Google Scholar]
- Foeldi, M.; Foeldi, E. Földi’s Textbook of Lymphology: For Pysicians and Lymphedema Therapists; Elsevier Urban & Fischer: München, Germany, 2012. [Google Scholar]
- AL-Ghadban, S.; Cromer, W.; Allen, M.; Ussery, C.; Badowski, M.; Harris, D.; Herbst, K.L. Dilated Blood and Lymphatic Microvessels, Angiogenesis, Increased Macrophages, and Adipocyte Hypertrophy in Lipedema Thigh Skin and Fat Tissue. J. Obes. 2019, 2019, 8747461. [Google Scholar] [CrossRef] [PubMed]
- Buck, D.W.; Herbst, K.L. Lipedema: A Relatively Common Disease with Extremely Common Misconceptions. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbst, K.L.; Kahn, L.A.; Iker, E.; Ehrlich, C.; Wright, T.; McHutchison, L.; Schwartz, J.; Sleigh, M.; Donahue, P.M.; Lisson, K.H.; et al. Standard of Care for Lipedema in the United States. Phlebology 2021, 36, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Reich-Schupke, S.; Schmeller, W.; Brauer, W.J.; Cornely, M.E.; Faerber, G.; Ludwig, M.; Lulay, G.; Miller, A.; Rapprich, S.; Richter, D.F.; et al. S1 Guidelines: Lipedema: Guidelines. JDDG J. Dtsch. Dermatol. Ges. 2017, 15, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Bertsch, T.; Erbacher, G.; Elwell, R. Lipoedema: A paradigm shift and consensus. J. Wound Care 2020, 29, 1–51. [Google Scholar] [CrossRef]
- Erbacher, G.; Bertsch, T. Lipoedema and Pain: What Is the Role of the Psyche?—Results of a Pilot Study with 150 Patients with Lipoedema. Phlebologie 2020, 49, 305–316. [Google Scholar] [CrossRef]
- Torre, Y.S.-D.L.; Wadeea, R.; Rosas, V.; Herbst, K.L. Lipedema: Friend and Foe. Horm. Mol. Biol. Clin. Investig. 2018, 33, 20170076. [Google Scholar] [CrossRef]
- Jeziorek, M.; Szuba, A.; Kujawa, K.; Regulska-Ilow, B. The Effect of a Low-Carbohydrate, High-Fat Diet versus Moderate-Carbohydrate and Fat Diet on Body Composition in Patients with Lipedema. DMSO Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 2545–2561. [Google Scholar] [CrossRef]
- Keith, L.; Seo, C.A.; Rowsemitt, C.; Pfeffer, M.; Wahi, M.; Staggs, M.; Dudek, J.; Gower, B.; Carmody, M. Ketogenic Diet as a Potential Intervention for Lipedema. Med. Hypotheses 2021, 146, 110435. [Google Scholar] [CrossRef]
- Ehrlich, C.; Iker, E.; Herbst, K.L.; Kahn, L.-A.; Sears, D.D.; Kenyon, M.; McMahon, E. Lymphedema and Lipoedema Nutrition Guide. Foods, Vitamins, Minerals, and Supplements; Lymph Notes: San Francisco, CA, USA, 2015. [Google Scholar]
- Sørlie, V.; De Soysa, A.K.; Hyldmo, Å.A.; Retterstøl, K.; Martins, C.; Nymo, S. Effect of a Ketogenic Diet on Pain and Quality of Life in Patients with Lipedema: The LIPODIET Pilot Study. Obes. Sci. Pract. 2022, 8, 483–493. [Google Scholar] [CrossRef]
- Cannataro, R.; Michelini, S.; Ricolfi, L.; Caroleo, M.; Gallelli, L.; De Sarro, G.; Onorato, A.; Cione, E. Management of Lipedema with Ketogenic Diet: 22-Month Follow-Up. Life 2021, 11, 1402. [Google Scholar] [CrossRef]
- Michalczyk, M.M.; Klonek, G.; Maszczyk, A.; Zajac, A. The Effects of a Low-Calorie Ketogenic Diet on Glycaemic Control Variables in Hyperinsulinemic Overweight/Obese Females. Nutrients 2020, 12, 1854. [Google Scholar] [CrossRef]
- Choi, Y.J.; Jeon, S.-M.; Shin, S. Impact of a Ketogenic Diet on Metabolic Parameters in Patients with Obesity or Overweight and with or without Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 2005. [Google Scholar] [CrossRef]
- Muscogiuri, G.; El Ghoch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L. Obesity Management Task Force (OMTF) of the European Association for the Study of Obesity (EASO). European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Facts 2021, 14, 222–245. [Google Scholar] [CrossRef]
- Saslow, L.R.; Daubenmier, J.J.; Moskowitz, J.T.; Kim, S.; Murphy, E.J.; Phinney, S.D.; Ploutz-Snyder, R.; Goldman, V.; Cox, R.M.; Mason, A.E.; et al. Twelve-Month Outcomes of a Randomized Trial of a Moderate-Carbohydrate versus Very Low-Carbohydrate Diet in Overweight Adults with Type 2 Diabetes Mellitus or Prediabetes. Nutr. Diabetes 2017, 7, 304. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Lin, G.; Chen, J.; Chen, Z.; Xu, F.; Zhu, F.; Zhang, J.; Yuan, S. The Effect of Periodic Ketogenic Diet on Newly Diagnosed Overweight or Obese Patients with Type 2 Diabetes. BMC Endocr. Disord. 2022, 22, 34. [Google Scholar] [CrossRef]
- D’Abbondanza, M.; Ministrini, S.; Pucci, G.; Nulli Migliola, E.; Martorelli, E.-E.; Gandolfo, V.; Siepi, D.; Lupattelli, G.; Vaudo, G. Very Low-Carbohydrate Ketogenic Diet for the Treatment of Severe Obesity and Associated Non-Alcoholic Fatty Liver Disease: The Role of Sex Differences. Nutrients 2020, 12, 2748. [Google Scholar] [CrossRef]
- Buso, G.; Depairon, M.; Tomson, D.; Raffoul, W.; Vettor, R.; Mazzolai, L. Lipedema: A Call to Action! Obesity 2019, 27, 1567–1576. [Google Scholar] [CrossRef]
- Kruppa, P.; Georgiou, I.; Biermann, N.; Prantl, L.; Klein-Weigel, P.; Ghods, M. Lipedema—Pathogenesis, Diagnosis, and Treatment Options. Dtsch. Ärztebl. Int. 2020, 117, 396–403. [Google Scholar] [CrossRef]
- Hempe, J.M.; Yang, S.; Liu, S.; Hsia, D.S. Standardizing the Haemoglobin Glycation Index. Endocrinol. Diabetes Metab. 2021, 4, e00299. [Google Scholar] [CrossRef]
- Jeziorek, M.; Szuba, A.; Kujawa, K.; Regulska-Ilow, B. Comparison of Actual and Predicted Resting Metabolic Rate in Women with Lipedema. Lymphat. Res. Biol. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- United Nations University; World Health Organization. Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation: Rome, 17–24 October 2001; Food & Agriculture Organization of the United Nations: Rome, Italy, 2004; Volume 1. [Google Scholar]
- Kunachowicz, H.; Nadolna, J.; Przygoda, B.; Iwanow, K. Tabele Składu i Wartości Odżywczej Żywności [Food Composition Tables]; PZWL: Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- U.S. Department of Agriculture, Agricultural Research Service. FoodData Central. 2019. Available online: https://Fdc.nal.usda.gov (accessed on 5 January 2021).
- Tzenios, N.; Lewis, E.D.; Crowley, D.C.; Chahine, M.; Evans, M. Examining the Efficacy of a Very-Low-Carbohydrate Ketogenic Diet on Cardiovascular Health in Adults with Mildly Elevated Low-Density Lipoprotein Cholesterol in an Open-Label Pilot Study. Metab. Syndr. Relat. Disord. 2022, 20, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Burén, J.; Ericsson, M.; Damasceno, N.; Sjödin, A. A Ketogenic Low-Carbohydrate High-Fat Diet Increases LDL Cholesterol in Healthy, Young, Normal-Weight Women: A Randomized Controlled Feeding Trial. Nutrients 2021, 13, 814. [Google Scholar] [CrossRef] [PubMed]
- Cunha, G.M.; Guzman, G.; Correa De Mello, L.L.; Trein, B.; Spina, L.; Bussade, I.; Marques Prata, J.; Sajoux, I.; Countinho, W. Efficacy of a 2-Month Very Low-Calorie Ketogenic Diet (VLCKD) Compared to a Standard Low-Calorie Diet in Reducing Visceral and Liver Fat Accumulation in Patients With Obesity. Front. Endocrinol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Rinaldi, R.; De Nucci, S.; Castellana, F.; Di Chito, M.; Giannuzzi, V.; Shahini, E.; Zupo, R.; Lampignano, L.; Piazzolla, G.; Triggiani, V.; et al. The Effects of Eight Weeks’ Very Low-Calorie Ketogenic Diet (VLCKD) on Liver Health in Subjects Affected by Overweight and Obesity. Nutrients 2023, 15, 825. [Google Scholar] [CrossRef]
- Joshi, S.; Kalantar-Zadeh, K.; Chauveau, P.; Carrero, J.J. Risks and Benefits of Different Dietary Patterns in CKD. Am. J. Kidney Dis. 2023, 81, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Goday, A.; Bellido, D.; Sajoux, I.; Crujeiras, A.B.; Burguera, B.; García-Luna, P.P.; Oleaga, A.; Moreno, B.; Casanueva, F.F. Short-Term Safety, Tolerability and Efficacy of a Very Low-Calorie-Ketogenic Diet Interventional Weight Loss Program versus Hypocaloric Diet in Patients with Type 2 Diabetes Mellitus. Nutr. Diabetes 2016, 6, e230. [Google Scholar] [CrossRef] [Green Version]
- Peeke, P.M.; Greenway, F.L.; Billes, S.K.; Zhang, D.; Fujioka, K. Effect of Time Restricted Eating on Body Weight and Fasting Glucose in Participants with Obesity: Results of a Randomized, Controlled, Virtual Clinical Trial. Nutr. Diabetes 2021, 11, 6. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Lipedema Group (n = 24) mean ± SD/Me (Q1, Q3) | Overweight/Obesity Group (n = 24) mean ± SD/Me (Q1, Q3) | t/Z | p-Values |
|---|---|---|---|---|
| Age [years] | 39.0 (34.0, 62.0) | 49.0 (41.5, 59.0) | 1.28 | NS ** |
| Height [cm] | 165.2 ± 7.5 | 164.2 ± 5.9 | −0.5 | NS * |
| Weight [kg] | 86.1 ± 17.8 | 92.0 ± 14.9 | 1.25 | NS * |
| BMI [kg/m2] | 31.6 ± 6.4 | 34.0 ± 4.6 | 1.47 | NS * |
| <25 kg/m2 | 16.7% (n = 4) | n = 0 | NS | |
| 25.0–29.9 kg/m2 | 16.7% (n = 4) | 25.0% (n = 6) | NS | |
| 30.0–34.9 kg/m2 | 41.7% (n = 10) | 41.7% (n = 10) | NS | |
| 35.0–39.9 kg/m2 | 8.3% (n = 2) | 25.0% (n = 6) | NS | |
| >40 kg/m2 | 16.7% (n = 4) | 8.3% (n = 2) | NS | |
| Waist [cm] | 98.0 ± 12.9 | 106.7 ± 10.6 | 2.57 | 0.013 * |
| Hips [cm] | 115.1 ± 12.0 | 114.6 ± 8.6 | 0.17 | NS * |
| WHR | 0.85 ± 0.1 | 0.93 ± 0.1 | −4.2 | 0.0001 * |
| Left thigh [cm] | 65.1 ± 7.5 | 64.9 ± 5.6 | 0.13 | NS * |
| Right thigh [cm] | 65.1 ± 7.4 | 64.9 ± 5.8 | 0.1 | NS * |
| Left calf [cm] | 44.3 (41.3, 47.5) | 42.0 (40.5, 44.0) | 1.97 | 0.048 ** |
| Right calf [cm] | 45.5 (40.3, 47.8) | 42.3 (39.8, 44.5) | 1.54 | NS ** |
| Left ankle [cm] | 24.8 (23.3, 26.0) | 23.0 (22.3, 24.8) | 1.92 | NS ** |
| Right ankle [cm] | 24.0 (23.0, 26.0) | 23.5 (22.5, 24.8) | 1.39 | NS ** |
| RMR [kcal] | 1651.2 ± 250.8 | 1676.4 ± 361.2 | 0.27 | NS * |
| Bilirubin [mg/dL] | 0.65 (0.5, 0.85) | 0.55 (0.4, 0.65) | 2.09 | 0.034 ** |
| ASPAT [U/L] | 21.0 (19.0, 28.5) | 25.0 (20.5, 28.0) | 1.05 | NS ** |
| ALAT [U/L] | 19.5 (15.0,25.5) | 23.5 (17.5, 29.0) | 1.53 | NS ** |
| GGTP [U/L] | 17.5 (13.0, 22.5) | 19.5 (13.5, 26.0) | 0.91 | NS ** |
| ALP [U/L] | 69.6 ± 22.7 | 67.1 ± 24.0 | 0.36 | NS * |
| TC [mg/dL] | 206.7 ± 40.2 | 232.3 ± 49.2 | 1.97 | NS * |
| LDL-C [mg/dL] | 118.0 ± 28.6 | 145.9 ± 53.5 | 2.25 | 0.029 * |
| HDL-C [mg/dL] | 67.0 (56.5, 73.0) | 64.5 (52.0, 71.0) | 0.68 | NS ** |
| TG [mg/dL] | 83.0 (61.5, 113.5) | 118.5 (70.0, 154.5) | 1.61 | NS ** |
| Creatinine [mg/dL] | 0.81 (0.71, 0.83) | 0.85 (0.8, 0.92) | 2.17 | 0.03 ** |
| GFR [ml/min/1.73 m2] | 87.5 ± 15.1 | 77.2 ± 13.6 | 2.49 | 0.016 * |
| Uric acid [mg/dL] | 4.4 (3.9, 5.6) | 5.2 (4.3, 6.0) | 1.84 | NS ** |
| TSH [uIU/mL] | 1.6 (1.3,2.2) | 1.6 (1.0, 1.9) | 0.94 | NS ** |
| HbA1c [%] | 5.3 ± 0.3 | 5.5 ± 0.3 | 2.39 | 0.021 * |
| Glucose 0 min [mg/dL] | 82.0 (79.0, 88.5) | 86.0 (78.5, 94.0) | −0.8 | NS ** |
| Glucose 60 min [mg/dL] | 125.1 ± 42.3 | 148.0 ± 47.0 | 1.71 | NS * |
| Glucose 120 min [mg/dL] | 103.5 ± 33.9 | 119.4 ± 33.5 | 1.59 | NS * |
| Insulin 0 min [uU/mL] | 5.9 (4.7, 8.7) | 7.0 (6.1, 9.0) | 1.53 | NS ** |
| Insulin 60 min [uU/mL] | 50.1 (23.1, 81.7) | 59.7 (36.9, 92.4) | 0.96 | NS ** |
| Insulin 120 min [uU/mL] | 23.8 (14.7, 49.2) | 43.1 (17.5, 101.0) | −1.6 | NS ** |
| HOMA-IR | 1.2 (0.9, 1.9) | 1.6 (1.2, 2.2) | 1.34 | NS ** |
| Stage | Description | Percentage of Lipedema Stage in the Study (n = 24) |
|---|---|---|
| 1 | skin has a smooth texture with subdermal pebble like feel due to underlying loose connective tissue fibrosis | 37.5% (n = 9) |
| 2 | the skin surface is irregular and pitted, and an orange skin phenomenon is present | 54.2% (n = 13) |
| 3 | deformation of legs with larger fat masses | 8.3% (n = 2) |
| 4 | concomitant lymphedema (lipolymphedema) | 0 |
| Type | Description | Percentage of Lipedema Types in the Study (n = 24) |
| 1 | buttocks | 0 |
| 2 | buttocks, hips, and thighs | 25.0% (n = 6) |
| 3 | buttocks, hips, thighs, and calves | 70.8% (n = 17) |
| 4 | arms | 33.3% (n = 8) |
| 5 | calves | 4.2% (n = 1) |
| Parameter | Lipedema Group (n = 24) Mean ± SD/Me (Q1, Q3) | Overweight/Obesity Group (n = 24) Mean ± SD/Me (Q1, Q3) | Differences between Baseline and 7 Months Mean ± SD/Me (Q1, Q3) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 7 Months | p-Values | Baseline | 7 Months | p-Values | Lipedema | Obesity | t/Z | p-Values | |
| Weight [kg] | 86.1 ± 17.8 | 74.1 ± 12.9 | <0.0001 * | 90.5 (81.7, 97.5) | 77.1 (69.2, 86.5) | <0.0001 ** | −11.1 (6.4, 15.9) | −11.8 (10.2, 13.1) | −0.84 | NS *** |
| BMI [kg/m2] | 31.6 ± 6.4 | 27.3 ± 5.1 | <0.0001 * | 33.9 (30.5, 36.3) | 28.0 (26.1, 33.1) | <0.0001 ** | −3.9 (2.5, 6.2) | −4.3 (3.9,4.6) | −0.96 | NS *** |
| Waist [cm] | 98.0 ± 12.9 | 85.2 ± 11.3 | <0.0001 * | 106.7 ± 10.6 | 94.4 ± 12.1 | <0.0001 * | −12.8 ± 6.4 | −12.4 ± 6.2 | 0.23 | NS * |
| Hips [cm] | 115.1 ± 12.0 | 105.4 ± 9.2 | <0.0001 * | 115.0 (109.5, 119.8) | 104.8 (101.0, 108.3) | <0.0001 ** | −8.8 (6.3, 13.0) | −8.3 (7.0, 11.3) | −0.06 | NS *** |
| WHR | 0.84 (0.78, 0.91) | 0.79 (0.74, 0.86) | 0.0001 ** | 0.93 ± 0.1 | 0.9 ± 0.1 | 0.006 * | −0.04 (0.0, 0.07) | −0.02 (0.001, 0.06) | 0.69 | NS *** |
| Left thigh [cm] | 65.1 ± 7.5 | 59.1 ± 5.9 | <0.0001 * | 64.9 ± 5.6 | 59.2 ± 5.3 | <0.0001 * | −6.0 ± 3.3 | −5.7 ± 2.2 | 0.36 | NS* |
| Right thigh [cm] | 65.1 ± 7.3 | 58.9 ± 6.0 | <0.0001 * | 64.9 ± 5.8 | 59.1 ± 5.4 | <0.0001 * | −6.2 ± 3.5 | −5.8 ± 2.4 | 0.43 | NS * |
| Left calf [cm] | 44.7 ± 5.2 | 40.7 ± 3.9 | <0.0001 * | 42.1 ± 3.9 | 39.5 ± 3.7 | <0.0001 * | −4.0 ± 2.0 | −2.7 ± 1.2 | 2.8 | 0.008 * |
| Right calf [cm] | 44.5 ± 5.3 | 40.8 ± 4.3 | <0.0001 * | 42.4 ± 4.1 | 39.9 ± 4.0 | <0.0001 * | −3.8 ± 2.0 | −2.4 ± 1.0 | 2.97 | 0.005 * |
| Left ankle [cm] | 25.0 ± 2.3 | 23.7 ± 2.1 | <0.0001 * | 23.0 (22.3, 24.8) | 23.0 (22.3, 24.5) | NS | −1.0 (0.5, 1.8) | 0.0 (0.0, 0.5) | 3.93 | <0.0001 *** |
| Right ankle [cm] | 24.0 (23.0, 26.0) | 23.0 (22.3, 24.8) | 0.0001 ** | 23.9 ± 2.5 | 23.7 ± 2.4 | NS* | −1.0 (0.5, 2.0) | −0.2 (0.0, 0.5) | 3.31 | <0.001 *** |
| Parameter | Lipedema Group (n = 24) Mean ± SD/Me (Q1, Q3) | Overweight/Obesity Group (n = 24) Mean ± SD/Me (Q1, Q3) | p- Values |
|---|---|---|---|
| Energy value [kcal] | 1680.8 ± 132.3 | 1648.7 ± 123.3 | NS * |
| Total protein [g] Total protein [% kcal] | 88.3 ± 14.4 21.0 ± 2.7 | 89.2 ± 6.5 21.7 ± 1.9 | NS * NS * |
| Total carbohydrates [g] Total carbohydrates [% kcal] | 33.9 ± 13.0 6.9 ± 2.8 | 36.5 ± 7.4 7.6 ± 1.3 | NS * NS * |
| Fiber [g] | 8.9 (7.7, 10.8) | 8.8 (8.1, 11.9) | NS ** |
| Total fat [g] Total fat [% kcal] | 133.1 (124.4, 141.1) 71.1 (70.4, 74.4) | 132.1 (120.3, 140.0) 70.7 (68.7, 72.3) | NS ** NS ** |
| SFAs [g] | 36.0 ± 7.8 | 36.9 ± 6.9 | NS * |
| MUFA [g] | 55.9 ± 8.5 | 58.5 ± 8.4 | NS * |
| PUFA [g] | 24.6 ± 5.7 | 27.0 ± 6.8 | NS * |
| n-6 to n-3 ratio | 3.1 (2.2, 4.2) | 3.3 (3.0, 3.8) | NS ** |
| Parameter | Lipedema Group (n = 24) Mean ± SD/Me (Q1, Q3) | Overweight/Obesity Group (n = 24) Mean ± SD/Me (Q1, Q3) | Differences Between Baseline and 7 Months Mean ± SD/Me (Q1, Q3) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 7 Months | p-Value | Baseline | 7 months | p-Value | Lipedema | Obesity | t/Z | p-Value | |
| Bilirubin [mg/dL] | 0.65 (0.5, 0.85) | 0.7 (0.5, 0.85) | NS ** | 0.5 (0.4, 0.7) | 0.7 (0.5, 0.9) | 0.024 ** | 0.05 (−0.2, 0.1) | 0.2 (−0.3, 0.2) | 1.51 | NS *** |
| ASPAT [U/L] | 23.3 ± 6.5 | 22.7 ± 5.6 | NS * | 25.0 (20.5, 28.0) | 19.5 (17.5, 23.0) | 0.001 ** | −0.6 ± 5.6 | −5.5 ± 7.0 | −2.57 | 0.01 *** |
| ALAT [U/l] | 20.8 ± 8.9 | 20.0 ± 7.0 | NS * | 23.5 (17.5, 29.0) | 19.5 (15.0, 21.0) | 0.008 ** | −0.8 ± 6.8 | −8.5 ± 16.0 | −2.04 | 0.04 *** |
| GGTP [U/L] | 17.5 (13.0, 22.5) | 15.0 (13.0, 20.0) | NS ** | 19.5 (13.5, 26.0) | 17.5 (14.0, 21.0) | 0.022 ** | −0.5 (−1.0, 3.0) | −2.0 (−0.5, 5.5) | −1.27 | NS *** |
| ALP [U/l] | 63.5 (52.0, 81.5) | 64.0 (56.0, 76.0) | NS ** | 67.1 ± 24.0 | 60.3 ± 20.0 | 0.001 * | −2.0 (−8.5, 26.0) | −5.5 (−0.5, 13.0) | −0.59 | NS *** |
| TC [mg/dL] | 206.7 ± 40.2 | 226.4 ± 54.7 | NS * | 223.0 (190.5, 268.5) | 215.0 (194.0, 249.0) | NS ** | 19.7 ± 50.6 | −31.9 ± 89.4 | −2.77 | 0.005 *** |
| LDL-C [mg/dL] | 118.0 ± 28.6 | 136.6 ± 44.2 | 0.046 * | 142.5 (110.0, 179.0) | 130.5 (99.0, 173.0) | NS ** | 18.6 ± 43.2 | −8.0 (−15.5, 27.0) | −2.29 | 0.022 *** |
| HDL-C [mg/dL] | 67.8 ± 18.8 | 74.2 ± 20.3 | 0.014 * | 64.5 (52.0, 71.0) | 69.0 (54.0,74.0) | NS ** | 6.4 ± 12.0 | 2.5 ± 21.7 | −1.3 | NS *** |
| TG [mg/dL] | 88.5 ± 35.9 | 77.1 ± 35.8 | 0.014 * | 122.2 ± 68.8 | 81.6 ± 36.3 | <0.0001 * | −11.5 ± 21.2 | −47.4 ± 41.7 | −3.77 | 0.0004 * |
| Creatine [mg/dL] | 0.8 ± 0.2 | 0.78 ± 0.1 | NS * | 0.9 ± 0.1 | 0.8 ± 0.1 | 0.003 * | −0.03 ± 0.08 | −0.06 ± 0.08 | −1.1 | NS * |
| GFR [mL/min/1.73 m2] | 87.5 ± 15.1 | 85.7 ± 16.0 | NS * | 77.2 ± 13.6 | 81.1 ± 11.9 | 0.049 * | −1.8 ± 9.2 | 3.9 ± 9.2 | 2.14 | 0.037 * |
| Uric acid [mg/dL] | 4.4 (3.9, 5.6) | 4.2 (3.4, 4.9) | NS ** | 5.2 (4.3, 6.0) | 4.9 (4.4, 5.7) | NS | −0.2 (−0.2, 0.9) | −0.4 (−0.3, 0.6) | 0.23 | NS *** |
| TSH [uIU/mL] | 1.6 (1.3, 2.2) | 1.3 (1.0, 1.7) | 0.009 ** | 1.6 (0.9, 1.9) | 1.4 (78.5, 94.0) | NS | −0.3 (−0.04, 0.6) | −0.05 (−0.1, 0.4) | 1.29 | NS *** |
| HbA1c [%] | 5.3 (5.1, 5.5) | 5.3 (5.1, 5.5) | NS ** | 5.5 ± 0.3 | 5.5 ± 0.3 | NS * | −0.1 (−0.1, 0.1) | −0.01 ± 0.2 | −0.31 | NS *** |
| Glucose 0 min [mg/dL] | 85.1 ± 11.9 | 87.9 ± 9.6 | NS * | 86.8 ± 10.6 | 84.4 ± 15.6 | NS * | −2.8 ± 12.8 | −2.3 ± 11.4 | −1.47 | NS * |
| Glucose 60 min [mg/dL] | 126.1 ± 39.5 | 149.8 ± 44.4 | NS * | 148.0 ± 47.0 | 125.6 ± 47.8 | 0.0004 * | −5.2 ± 83.2 | −42.4 ± 46.7 | −2.44 | 0.018 * |
| Glucose 120 min [mg/dL] | 100.0 ± 22.6 | 109.1 ± 25.0 | NS * | 115.0 (100.0, 154.0) | 96.5 (79.5, 117.0) | 0.002 ** | −1.0 (−29.0, 46.5) | −26.0 (4.0, 51.0) | −1.61 | NS *** |
| Insulin 0 min [uU/mL] | 5.9 (4.7, 8.7) | 5.8 (4.0, 9.6) | NS ** | 7.0 (6.1, 9.0) | 5.7 (3.8, 8.0) | 0.0005 ** | −0.6 (−1.3, 2.3) | −1.4 (0.4, 4.0) | −2.01 | 0.044 *** |
| Insulin 60 min [uU/mL] | 50.1 (23.1, 81.7) | 40.3 (27.7, 64.8) | NS ** | 59.7 (36.9, 92.4) | 42.8 (28.0, 70.8) | 0.008 ** | −8.1 (−15.1, 30.3) | −19.3 (1.8, 48.8) | −1.51 | NS *** |
| Insulin 120 min [uU/mL] | 33.3 ± 26.6 | 36.8 ± 21.7 | NS * | 43.1 (17.5, 100.9) | 31.8 (15.5, 44.8) | 0.016 ** | −0.7 (−11.6, 17.1) | −14.6 (0.7, 38.9) | −2.01 | 0.044 *** |
| HOMA-IR | 1.2 (0.9, 1.9) | 1.0 (−2.5, 5.0) | NS ** | 1.6 (1.2, 2.2) | 1.1 (0.5, 7.5) | 0.0007 ** | −0.1 (−0.2, 0.4) | −0.3 (0.1, 0.8) | −2.32 | 0.02 *** |
| Diagnosis | Lipedema Group n = 24 | p-Value | Overweight/Obesity Group n = 24 | p-Value | ||
|---|---|---|---|---|---|---|
| Baseline | 7 Months | Baseline | 7 Months | |||
| Hypercholesterolemia (LDL-C ≥ 115 mg/dL) | 50.0% (n = 12) | 66.7 % (n = 16) | NS | 68.2% (n = 15) | 50.0% (n = 11) | NS |
| Hypertriglyceridemia (TG ≥ 150 mg/dL) | 3.8 % (n = 1) | 3.8 % (n = 1) | NS | 31.8% (n = 7) | 4.5% (n = 1) | 0.04 |
| HDL-C < 45 mg/dL | 3.8 % (n = 1) | 3.8 % (n = 1) | NS | 9.1% (n = 2) | 4.5% (n = 1) | NS |
| IGF (100–125 mg/dL) | 3.8 % (n = 1) | 11.5% (n = 3) | NS | 9.1% (n = 2) | 13.6% (n = 3) | NS |
| IGT (140–199 mg/dL) | 7.7% (n = 2) | 7.7% (n = 2) | NS | 22.7% (n = 5) | 18.2% (n = 4) | NS |
| HOMA-IR (>2.5) | 7.7% (n = 2) | 7.7% (n = 2) | NS | 22.7% (n = 5) | 13.6% (n = 3) | NS |
| Hyperuricemia (>6 mg/dL) | 7.7% (n = 2) | 3.8 % (n = 1) | NS | 18.2% (n = 4) | 22.7% (n = 5) | NS |
| ALAT (>35 U/L) | 3.8 % (n = 1) | 3.8 % (n = 1) | NS | 18.2% (n = 4) | 0 | NS |
| ASPAT (>31 U/L) | 11.5% (n = 3) | 11.5% (n = 3) | NS | 13.6% (n = 3) | 0 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeziorek, M.; Szuba, A.; Sowicz, M.; Adaszyńska, A.; Kujawa, K.; Chachaj, A. The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women. Nutrients 2023, 15, 2619. https://doi.org/10.3390/nu15112619
Jeziorek M, Szuba A, Sowicz M, Adaszyńska A, Kujawa K, Chachaj A. The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women. Nutrients. 2023; 15(11):2619. https://doi.org/10.3390/nu15112619
Chicago/Turabian StyleJeziorek, Małgorzata, Andrzej Szuba, Monika Sowicz, Agnieszka Adaszyńska, Krzysztof Kujawa, and Angelika Chachaj. 2023. "The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women" Nutrients 15, no. 11: 2619. https://doi.org/10.3390/nu15112619
APA StyleJeziorek, M., Szuba, A., Sowicz, M., Adaszyńska, A., Kujawa, K., & Chachaj, A. (2023). The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women. Nutrients, 15(11), 2619. https://doi.org/10.3390/nu15112619