
Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience




Abstract
:1. Introduction
2. Alzheimer’s Disease
3. Methodology
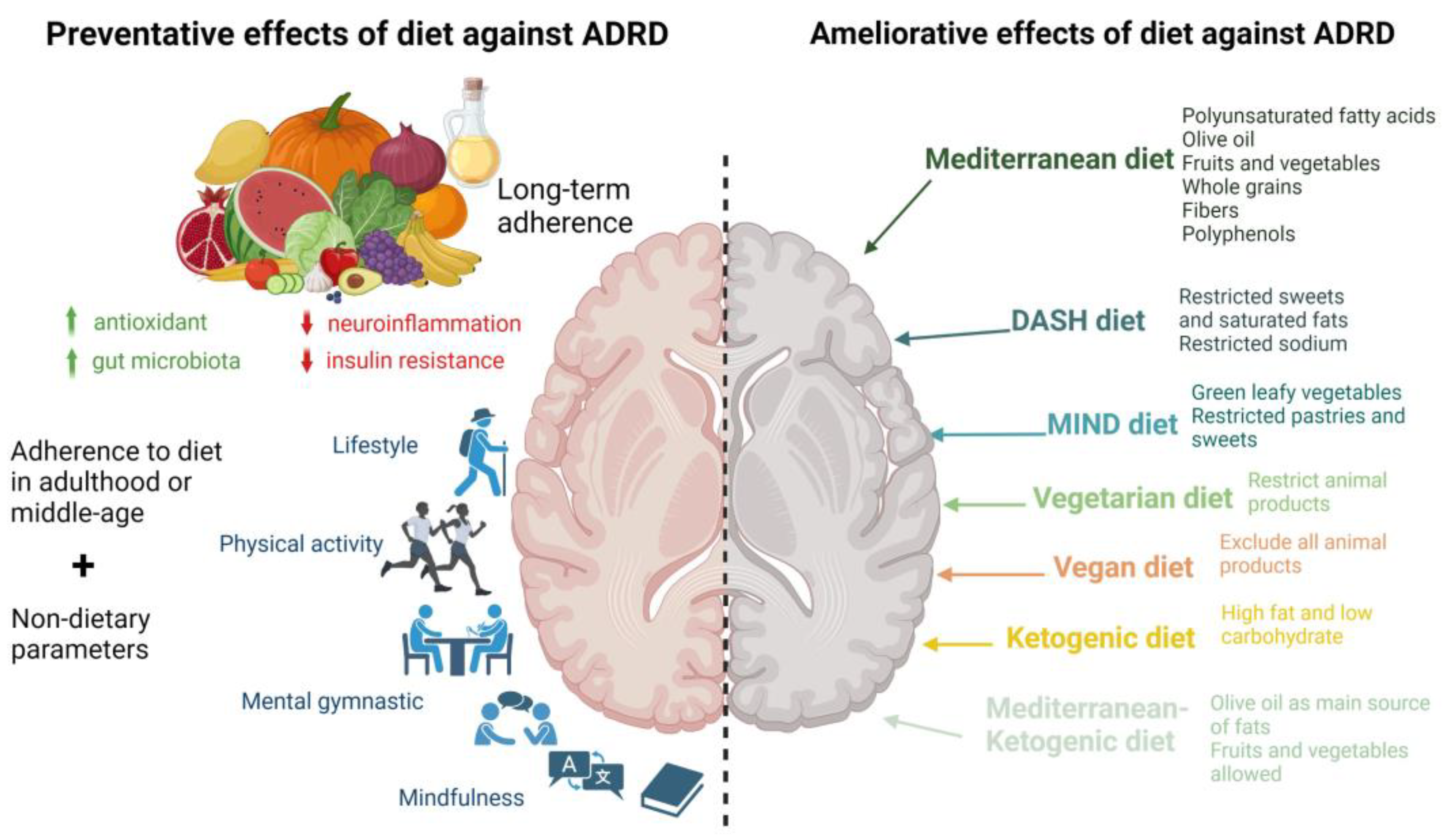
4. Impact of Specific Dietary Patterns on ADRD Progression
4.1. Impact of Mediterranean Diet on ADRD Progression


{kind=link}
{kind=link}
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults in CCMS Age: ≥65 years n = 3580 | 10.6 years | 142-item FFQ, MedD score, DASH score, global cognition (3 MS) | Associations between DASH and MedD diets and age-related cognitive change. | Higher quintile of MedD score associated with better average cognition during follow-up but not with cognitive function rate of change. | Age, gender, education, BMI, frequency of moderate physical activity, multivitamin and mineral supplement use, history of drinking and smoking, and history of diabetes, heart attack, or stroke. | [104] |
| Longitudinal | US | Participants in United States Reasons for Geographic and Racial Differences in Stroke study n = 17,478 (7548 M 9930 F) Age: 64.4 years | 4 years | 98-item block FFQ, MedD score, cognitive impairment, six-item screener (SIS) | Higher adherence to MedD and likelihood of incident cognitive impairment (ICI) and the interaction of race and vascular risk factors. | High compared with low adherence to MedD significantly associated with lower risk of ICI. Higher tertile of MedD score significantly associated with lower risk of ICI. | Age, gender, race, region, educational level, income, number of packs smoked per year, weekly exercise, diabetes mellitus, hypercholesterolemia, atrial fibrillation, history of heart disease, BMI, waist circumference, systolic and diastolic blood pressure, ACE inhibitors/angiotensin receptor blockers, β-blockers, other antihypertensive medication, depressive symptoms, and self-reported health status. | [105] |
| Longitudinal | Sweden | Senior participants in Prospective Investigation of the Vasculature in Uppsala Seniors Age: 70.1 ± 0.01 years at enrollment n = 194 (101 M 93 F) cognitive assessment at 75 years | 5 years | 7-day food diary, adapted MedD score, dietary components, global cognition (7 MS), brain volume (3D T1-weighted MRI scan) | Association between dietary habits, cognitive functioning, and brain volumes in older individuals. | Continuous MedD score not significantly associated with global cognitive function after adjustment. Continuous MedD score not associated with gray or white matter volume or total brain volume. | Gender, energy intake, education, self-reported physical activity, low-density cholesterol, BMI, systolic blood pressure, and HOMA-IR. | [99] |
| Longitudinal | US | Subset of participants from the Women’s Health study n = 6174 (0 M 6174 F) Age: 72 years | 4 years | 131-item SFFQ, adapted MedD score, dietary components, global cognition (TICS, EBMT, CF) and verbal memory (EBMT, delayed recall of TICS 10-word list) | Association of adherence to MedD with cognitive function and decline. | MedD score quintile not significantly associated with better average global cognition or verbal memory nor with change in global cognition and verbal memory. | Treatment arm, age at initial cognitive testing, Caucasian race, high education, high income, energy intake, physical activity, BMI, smoking, diabetes, hypertension, hypercholesterolemia, hormone use, and depression. | [67] |
| Longitudinal | US | Women from the Nurses’ Health Study n = 16,058 (0 M 16,058 F) Age: 74.3 years | 6 years | 116-item SFFQ, adapted MedD score, dietary components, global cognition (TICS and composite score of TICS, EBMT, CF, DST backward), and verbal memory (immediate and delayed recalls of the EBMT and TICS) | Associations between long-term adherence to MedD and subsequent cognitive function and decline. | Long-term higher quintile MedD score at older age significantly associated with better performance on TICS, global cognition, and verbal memory. Quintile of average MedD score not significantly associated with change in TICS score, global cognition, or verbal memory. | Age, education, long-term physical activity and total energy intake, BMI, smoking, multivitamin use, and history of depression, diabetes, hypertension, hypercholesterolemia, or myocardial infarction. | [54] |
| Longitudinal | US | Subset of participants from The Supplementation with Vitamins and Mineral Antioxidants study n = 3083 (1655 M 1428 F) Age: 52.0 ± 4.6 years at enrollment | 13 years | 24 h food recalls (12: each year), MedD score, Mediterranean-Style Dietary Pattern Score (MSDPS), cognitive performance (episodic memory, lexical-semantic memory, short-term memory, working memory, mental flexibility | Association between midlife MedD adherence and cognitive performance assessed 13 years later. | Higher tertile of MedD score associated only with working memory span. Higher tertile of MSDPS significantly associated with semantic fluency on the phonemic fluency task, but not with global cognition, episodic memory, short-term memory, working memory, or mental flexibility. | Age, gender, education, follow-up time, supplementation group during the trial phase, number of 24 h dietary records, total energy intake, BMI, occupational status, smoking status, physical activity, memory difficulties at baseline, depressive symptoms concomitant with the cognitive function assessment, and history of diabetes, hypertension, or CVD. | [55] |
| Longitudinal | Italy | Subset of participants in TRELONG Study n = 309 (120 M 189 F) Age: 79.1 ± 9.65 y | 7 years | FFQ, MedD yes/no (based on cereal, fish, vegetable and fruit intake), global cognition (MMSE) | Association between risk factors (body mass index (BMI), depression, chronic diseases, smoking, and lifestyles) and cognitive decline in older adults. | Adherence compared to non-adherence to MedD not significantly associated with less cognitive decline | NS | [106] |
| Longitudinal | US | Older participants from the Memory and Aging Project cognitively normal at enrollment n = 826 (26%M) Age: 81.5 ± 7.1 years | 4.1 years | 144-item FFQ, battery of cognitive tests: episodic memory, semantic memory, working memory, perceptual speed, and visuospatial ability. | Association between DASH and MedD diets and slower cognitive decline. | A 1-unit higher MedD score associated with a 0.002 slower rate of global cognitive decline standardized units, after adjustment for covariates. | Age, gender, education, participation in cognitive activities, total energy intake (kcal), time, and the interaction between time and each covariate, physical activity, presence of APOE ε4 alleles, depression, hypertension, diabetes, and stroke. | [58] |
| Longitudinal | Greece | Older adults in European Prospective Investigation into Cancer and Nutrition (EPIC) n = 401 (144 M 257 F) Age at enrollment: 74 years | 6.6 years | 150-item SFFQ, MedD score, dietary components, global cognition (MMSE) | Association between adherence to MedD in a Mediterranean country and cognitive decline in older adults. | Higher tertile of MedD scores significantly associated with less mild cognitive decline and substantial cognitive decline. | Age, gender, years of education, BMI, physical activity, smoking status, diabetes, hypertension, cohabiting, total energy intake. | [49] |
| Longitudinal | China | Older adults in China Health and Nutrition Survey n = 1650 (820 M 831 F) Age: 63.5 years | 5.3 years | 3-day 24 h recall, adapted MedD score, dietary components, decline in global cognition, composite z-scores, and verbal memory (modified TICS) | Association between cognitive changes among Chinese older adults and either an adapted Mediterranean diet score or factor-analysis-derived dietary patterns. | Higher MedD score significantly associated with slower rate of decline in global cognitive, composite z-, and verbal memory scores only in participants ≥ 65 years. Higher tertile of MedD score significantly associated with less decline in global cognitive scores and verbal memory scores only in participants ≥ 65 years | Age, gender, education, region, urbanization index, annual household income per capita, total energy intake, physical activity, current smoking, time since baseline, BMI, hypertension, and time interactions with each covariate. | [61] |
| Longitudinal | Sweden | Older adults in Uppsala longitudinal study n = 1038 (1038 M 0 F) Age at enrollment: 70 years | 12 years | 7-day food diary, adapted MedD score, AD (based on NINCDS-ADRDA and DSM-IV criteria), dementia, and cognitive impairment (MMSE) | Associations between development of cognitive dysfunctions and different diets. (Healthy Diet Indicator), a Mediterranean-like diet, and a low-carbohydrate, high-protein diet. | Continuous MedD score not associated with a lower risk of AD, dementia, or cognitive impairment. Higher tertile of MedD score not associated with AD or cognitive impairment. Highest tertile of MedD score in participants with energy intake according to the Goldberg cut-off significantly associated with a lower risk of cognitive impairment. | Energy, education, presence of APOE ε4 allele, living alone, smoking, and physical activity. | [72] |
| Longitudinal | US | Participants of the Rush Memory and Aging Project (MAP) n = 923 (±24% M) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MedD, A-DASH, and MIND scores, AD (based on NINCDS-ADRDA criteria) | Association of MIND, a hybrid Mediterranean and DASH diet, with incident Alzheimer’s disease. | Highest tertile of A-MedD adherence significantly associated with lower risk of AD diagnosis. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Older adults in Health, Aging, and Body Composition (Health ABC) n = 2326 (1109 M 1217 F) Age: 70–79 years | 7.9 years | 108-item block FFQ via interviews, A-MedD score (race-specific), global cognition (3 MS score) | Association of decreased risk of cognitive decline with MedD within a diverse population. | Among African American, but not among whites, A-MedD score significantly associated with less cognitive decline. | Age, gender, education, BMI, current smoking, physical activity, depression, diabetes, total energy intake, and socioeconomic status. | [60] |
| Longitudinal | Spain | Participants in Spanish SUN project n = 823 (597 M 223 F) Age: at enrollment, 61.9 ± 6.0 years | 6–8 years | 136-item SFFQ, MedD score, dietary components, cognitive function (TICS) | Association between adherence to MedD and cognitive function in a Spanish population. | Lower tertile of MedD score significantly associated with faster cognitive decline. | Age, gender, presence of APOE ε4 allele, follow-up time, total energy intake, BMI, smoking status, physical activity, diabetes, hypertension, hypercholesterolemia, history of CVD, and years of university education. | [59] |
| Longitudinal | US | Postmenopausal women enrolled in the Women’s Health Initiative Memory Study (WHIMS) n = 6425 (0%M) Age: 65–79 years | 9.11 years | FFQ, A-MedD score, DASH score, MCI (MMSE and battery of neuropsychological tests) | Association of dietary patterns with cognitive decline in older women and association of dietary patterns with risk of cognitive decline in women with hypertension. | A-MedD score quintile not significantly associated with reduced risk of MCI. Higher quintile of A-MedD score in a subset of white women with adjustment for APOE ε4 allele quintile significantly associated with a lower risk of MCI. | Age, race, education level, Women’s Health Initiative hormone trial randomization assignment, baseline 3 MS level, smoking status, physical activity, diabetes, hypertension, BMI, family income, depression, history of CVD, and total energy intake. | [73] |
| Longitudinal | Italy | Older adults in InCHIANTI study n = 832 (44% M) Age: 75.4 ± 7.6 y | 10.1 years | FFQ, MedD score, dietary components, global cognition (MMSE) | Association between MedD and trajectories of cognitive performance in the InCHIANTI study. | Continuous MedD score and higher tertile of MedD significantly associated lower risk of cognitive decline based on MMSE. | Age, gender, study site, chronic diseases, years of education, total energy intake, physical activity, BMI, presence of APOE ε4 allele, CRP, and IL-6. | [63] |
| Longitudinal | Sweden | Older adults in Swedish National study on Aging and Care n = 2223 (871 M 1352 F) Age: M: 69.5 ± 8.6 and F: 71.3 ± 9.1 years | 6 years | 98-item SFFQ, A-MedD, A-DASH, and MIND scores, dietary components, global cognition (MMSE) | Association between slower cognitive decline and dietary patterns: MIND, DASH, MedD, and a Nordic dietary pattern. | Higher A-MedD score significantly associated with less cognitive decline. A-MedD score not significantly associated with a lower risk of MMSE score ≤24. | Total caloric intake, age, gender, education, civil status, physical activity, smoking, BMI, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than those included in each dietary index. | [41] |
| Longitudinal | US | Male health professional participants in Health Professionals Follow-up Study n = 27,842 (27,842 M 0 F) Age at baseline: 51 y | ±26 years | FFQ, MedD score, dietary components, subjective cognitive function (SCF) | Association between long-term adherence to MedD and self-reported subjective cognitive function. | Higher quintile of MedD score associated with a lower risk of both poor SCF and moderate SCF. | Age, smoking history, diabetes, hypertension, depression, hypercholesterolemia, physical activity level, BMI. | [62] |
| Longitudinal | Australia | Older Australian adults n= 1220 (50% men) Age: 60–64 years | 12 years | CSIRO-FFQ, MedD, and MIND scores, dietary components | Cognitive impairment: MCI/dementia (Winbald criteria, NINCDS-ADRDA criteria). | Higher tertile of MedD score not significantly associated with cognitive impairment. | Energy intake, age, sex, presence of APOE ε4 allele, education, mental activity, physical activity, smoking status, depression, diabetes, BMI, hypertension, heart disease, and stroke. | [74] |
| Longitudinal | US | Participants in the Cognitive Reserve (CR) study and the Reference Ability Neural Network (RANN) study n = 183 (89 M 94 F) Age: 53.19 ± 16.52 years | 5 years | FFQ, MedD score, brain MRI | Association of greater adherence to MedD with less accumulation of white matter hyperintensities (WMHs). | MedD adherence negatively associated with an increase in WMHs, adjusting for all covariates. Association between MedD and WMH change moderated by age. | Age, gender, and race/ethnicity. | [85] |
| Cross-sectional | Greece | Older adults n = 557 (237 M 320 F) Age > 65 years | NS | 157-item EPIC-Greek SFFQ, A-MedD score, cognitive impairment (MMSE) | Association of dietary habits with cognitive function among seniors. | Continuous MedD score significantly associated with less cognitive impairment in men but more cognitive impairment in women. | Age, GDS, education, social activity, smoking, metabolic syndrome. | [107] |
| Cross-sectional | Australia | Participants from Southern Australia n = 1183 (432 M 751 F) Age: 50.6 ± 5.8 years | NS | 215-item FFQ, MedD score, dietary components Self-reported cognitive function (CFQ) on mistakes in tasks, perception, memory, and motor function | Association of level of adherence to the MedD with cognitive function and psychological well-being. | MedD score not significantly associated with self-reported cognitive function. | Age, gender, education, BMI, exercise, smoking, and total energy intake. | [108] |
| Cross-sectional | China | Chinese older adults from Hong Kong n= 3670 (1926 M 1744 F) Age: >65 years | NS | 280-item FFQ, MedD score, cognitive function (CSI-D) | Association of a priori or a posteriori diet with risk of cognitive impairment. | No significant association between MedD score and cognitive function in men and women. | Age, BMI, PASE, energy intake, education level, Hong Kong community ladder, smoking status, alcohol use, number of ADLs, GDS category, and self-reported history of diabetes, hypertension, and CVD/stroke. | [66] |
| Cross-sectional | Scotland | Participants enrolled in 1936 n = 878 (±50% M) Age: 69.5 years | NS | 168-item FFQ, MedD (22 items), cognitive function (IQ (MHT), general cognition (WAIS-III LNS, MR, BD, DS, DST backward, SS), processing speed (SS, DS, SCRT, IT), memory LM and VPA immediate and delayed recalls, SSP forward and backward, LNS, DST backward, and verbal ability (NART, WTAR)) | Association between dietary patterns and better cognitive performance in later life, taking into consideration childhood intelligence quotient (IQ) and socioeconomic status. | MedD score positively associated with verbal ability only. | Age, gender, occupational social class, IQ at age of 11 years. | [109] |
| Cross-sectional | Poland | Older adults with high risk of metabolic syndrome n = 87 (31 M 56 F) Age: 70.0 ± 6.5 years | NS | FFQ, A-MedD score (high vs. low), dietary components, MCI, global cognition (MMSE), attention (TMT), visual memory (PRM), executive function (ST, SOC, SWM, SSP) | Association between adherence to MedD and cognitive function (CF), along with selected sociodemographic (SD) and clinical indices. | High MedD score significantly associated with lower prevalence of MCI and higher global cognition, but not with attention, visual memory, or executive function. | Gender, age, education level, smoking status, family status, leisure time physical activity, and existence of metabolic syndrome. | [48] |
| Cross-sectional | US | Participants in study of aging and dementia WHICAP n = 674 (220 M 454 F) Age: 80.1 ± 5.6 years | NS | FFQ, MedD score, MRI, total brain volume (TBV); total gray matter volume (TGMV); total white matter volume (TWMV), cortical thickness | Association of higher adherence to a MedD diet with larger MRI-measured brain volume or cortical thickness. | MedD adherence associated with less brain atrophy, with an effect similar to 5 years of aging. | Age at time of scan, gender, ethnicity, education, BMI, diabetes, mean cognitive z-score, presence of APOE ε4 allele, caloric intake, hypertension, heart disease, and stroke. | [90] |
| Cross-sectional | US | Older adults n = 5907 (40% men) Age: 67.8 years | NS | Cognitive performance (global cognition score based on immediate and delayed recall, backward counting, and serial seven subtraction) | Association between the MedD and MIND diets and cognition in a nationally representative population of older U.S. adults. | Higher tertile of A-MedD score significantly associated with better cognitive performance and lower risk of poor cognitive performance. | Age, gender, race, low education attainment, current smoking, obesity, total wealth, hypertension, diabetes mellitus, physical inactivity, depression, and total energy intake. | [65] |
| Cross-sectional | US | Older Spanish adults n = 79 (36 M 41 F) Age: 81.0 years | NS | 3-day 24 h diet recalls and a face-to- face interview, 14-item Mediterranean Diet Adherence Screener (MEDAS), global cognition (MMSE) | Association of adherence to MedD and cognitive status and depressive symptoms in older adults. | Higher tertile of MEDAS score significantly associated with better cognitive status. | NS | [64] |
| Cross-sectional | Greece | Older adults in Hellenic Longitudinal Investigation of Ageing and Diet n = 1864 (757 M 1107 F) Age: 73.0 ± 6.1 years | NS | SFFQ, A-MedD score, dietary components, cognitive status (dementia (DSM-IV, NINCDS/ADRDA criteria)) and cognitive performance (memory (GVLT), language (BNT, CIMS; categories: objects and the letter A), executive functioning (TMT, verbal fluency, months forward and backward), and visuospatial perception (TMT)) | Association of adherence to an a priori defined MedD and its components with dementia and specific aspects of cognitive function in a representative population cohort in Greece. | Continuous A-MedD score and A-MedD score quartile significantly associated with lower risk of dementia. A-MedD score significantly associated with composite z-score, memory, language, and executive functioning but not with visuospatial perception. | Age, gender, education, number of clinical comorbidities, and energy intake. | [52] |
| Cross-sectional | US | Clinically and cognitively normal participants who were enrolled in observational brain imaging studies n = 116 (44 M 72 F) Age: 50 ± 6 years | NS | FFQ, MedD score, memory (immediate and delayed recall), executive function (WAIS), language (WAIS vocabulary), and MRI-based cortical thickness | Effects of lifestyle and vascular-related risk factors for Alzheimer’s disease (AD) on in vivo MRI-based brain atrophy in asymptomatic young to middle-aged adults. | Continuous MedD score significantly positively associated with MRI-based cortical thickness of the posterior cingulate cortex. MedD score not significantly associated with memory, executive function, or language. | Age, gender, presence of APOE ε4 allele. | [84] |
| Cross-sectional | US | Older participants in study focusing on healthy brain aging and cardiovascular disease risk factors n = 82 (40 M 42 F) Age: 68.8 ± 6.88 years | NS | FFQ, MedD score, cognitive assessment: information processing, executive functioning, MRI scans | Associations between MedD and cognitive and neuroimaging phenotypes in a cohort of nondemented, nondepressed older adults. | After adjustment with all covariates, a significant effect of MedD score on the volume of the dentate gyrus. | Age, gender, education, BMI, and estimated daily calorie intake. | [101] |
4.2. Impact of DASH Diet on ADRD Progression
4.3. Impact of MIND Diet on ADRD Progression
4.4. Impact of Ketogenic Diet on ADRD Progression
4.5. Impact of Modified Mediterranean-Ketogenic Diet on ADRD Progression
4.6. Impact of Vegetarian Diet on ADRD Progression
4.7. Impact of Vegan Diet on ADRD Progression
5. Impact of Specific Dietary Patterns on ADRD Prevention
5.1. Impact of Mediterranean Diet on ADRD Prevention
5.2. Impact of DASH Diet on ADRD Prevention
5.3. Impact of MIND Diet on ADRD Prevention
6. Discussion
7. Parameters Affecting Food Intake in Older Adults
8. Other Parameters Important for ADRD
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 15 March 2023).
- He, Y.; Li, C.; Yang, Y.; Li, Y.; Wang, Y.; Yang, H.; Jin, T.; Chen, S. Meta-analysis of the rs2075650 polymorphism and risk of Alzheimer disease. Aging Clin. Exp. Res. 2016, 28, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.; James, B.; Johnson, T.; Reimer, J.; Solis, M.; Weuve, J.; Buckley, R.F.; Hohman, T.J.; Alzheimer’s Association. Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar]
- Francis, P.T.; Palmer, A.M.; Snape, M.; Wilcock, G.K. The cholinergic hypothesis of Alzheimer’s disease: A review of progress. J. Neurol. Neurosurg. Psychiatry 1999, 66, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Bagyinszky, E.; Youn, Y.C.; An, S.S.; Kim, S. The genetics of Alzheimer’s disease. Clin. Interv. Aging 2014, 9, 535–551. [Google Scholar] [CrossRef] [Green Version]
- Jalbert, J.J.; Daiello, L.A.; Lapane, K.L. Dementia of the Alzheimer Type. Epidemiol. Rev. 2008, 30, 15–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farlow, M.R. Etiology and pathogenesis of Alzheimer’s disease. Am. J. Health Syst. Pharm. 1998, 55 (Suppl. S2), S5–S10. [Google Scholar] [CrossRef]
- Hersi, M.; Irvine, B.; Gupta, P.; Gomes, J.; Birkett, N.; Krewski, D. Risk factors associated with the onset and progression of Alzheimer’s disease: A systematic review of the evidence. Neurotoxicology 2017, 61, 143–187. [Google Scholar] [CrossRef]
- Solch, R.J.; Aigbogun, J.O.; Voyiadjis, A.G.; Talkington, G.M.; Darensbourg, R.M.; O’Connell, S.; Pickett, K.M.; Perez, S.R.; Maraganore, D.M. Mediterranean diet adherence, gut microbiota, and Alzheimer’s or Parkinson’s disease risk: A systematic review. J. Neurol. Sci. 2022, 434, 120166. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). 2023. Available online: https://www.cdc.gov/aging/aginginfo/alzheimers.htm (accessed on 15 March 2023).
- Tejada-Vera, B. Mortality from Alzheimer’s Disease in the United States: Data for 2000 and 2010; NCHS Data Brief, No 116; Hyattsville, M.D., Ed.; National Center for Health Statistics: Hyattsville, MD, USA, 2013.
- Chu, C.Q.; Yu, L.L.; Qi, G.Y.; Mi, Y.S.; Wu, W.Q.; Lee, Y.K.; Zhai, Q.X.; Tian, F.W.; Chen, W. Can dietary patterns prevent cognitive impairment and reduce Alzheimer’s disease risk: Exploring the underlying mechanisms of effects. Neurosci. Biobehav. Rev. 2022, 135, 104556. [Google Scholar] [CrossRef]
- James, B.D.; Wilson, R.S.; Boyle, P.A.; Trojanowski, J.Q.; Bennett, D.A.; Schneider, J.A. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain 2016, 139, 2983–2993. [Google Scholar] [CrossRef] [Green Version]
- Dodge, H.H.; Zhu, J.; Woltjer, R.; Nelson, P.T.; Bennett, D.A.; Cairns, N.J.; Fardo, D.W.; Kaye, J.A.; Lyons, D.E.; Mattek, N.; et al. SMART data consortium. Risk of incident clinical diagnosis of Alzheimer’s disease-type dementia attributable to pathology-confirmed vascular disease. Alzheimers Dement. 2017, 13, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Yu, L.; Leurgans, S.E.; Wilson, R.S.; Brookmeyer, R.; Schneider, J.A.; Bennett, D.A. Attributable risk of Alzheimer’s dementia attributed to age-related neuropathologies. Ann. Neurol. 2019, 85, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crous-Bou, M.; Minguillón, C.; Gramunt, N.; Molinuevo, J.L. Alzheimer’s disease prevention: From risk factors to early intervention. Alzheimers Res. Ther. 2017, 9, 71. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease-A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [Green Version]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Stern, Y.; Gu, Y. Modifiable lifestyle factors and cognitive reserve: A systematic review of current evidence. Ageing Res. Rev. 2022, 74, 101551. [Google Scholar] [CrossRef]
- Zainuddin, M.S.; Thuret, S. Nutrition, adult hippocampal neurogenesis and mental health. Br. Med. Bull. 2012, 103, 89–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, K.M.; Reed, B.R.; Manly, J.J.; Tommet, D.; Pietrzak, R.H.; Chelune, G.J.; Yang, F.M.; Revell, A.J.; Bennett, D.A.; Jones, R.N. Cognitive decline in the elderly: An analysis of population heterogeneity. Age Ageing 2011, 40, 684–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Boyle, P.A.; Segawa, E.; Leurgans, S.; Schneider, J.A.; Wilson, R.S.; Bennett, D.A. Residual decline in cognition after adjustment for common neuropathologic conditions. Neuropsychology 2015, 29, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, R.S.; Wang, T.; Yu, L.; Bennett, D.A.; Boyle, P.A. Normative Cognitive Decline in Old Age. Ann. Neurol. 2020, 87, 816–829. [Google Scholar] [CrossRef]
- Christ, A.; Lauterbach, M.; Latz, E. Western Diet and the Immune System: An Inflammatory Connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef] [Green Version]
- Kanehara, R.; Goto, A.; Sawada, N.; Mizoue, T.; Noda, M.; Hida, A.; Iwasaki, M.; Tsugane, S. Association between sugar and starch intakes and type 2 diabetes risk in middle-aged adults in a prospective cohort study. Eur. J. Clin. Nutr. 2022, 76, 746–755. [Google Scholar] [CrossRef]
- Chareonrungrueangchai, K.; Wongkawinwoot, K.; Anothaisintawee, T.; Reutrakul, S. Dietary Factors and Risks of Cardiovascular Diseases: An Umbrella Review. Nutrients 2020, 12, 1088. [Google Scholar] [CrossRef] [Green Version]
- Gaesser, G.A. Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies. Nutrients 2020, 12, 3756. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Moubarac, J.C.; Levy, R.B.; Canella, D.S.; Louzada, M.L.D.C.; Cannon, G. Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Crittenden, A.N.; Schnorr, S.L. Current views on hunter-gatherer nutrition and the evolution of the human diet. Am. J. Phys. Anthropol. 2017, 162 (Suppl. S63), 84–109. [Google Scholar] [CrossRef] [PubMed]
- Requena, T.; Martínez-Cuesta, M.C.; Peláez, C. Diet and microbiota linked in health and disease. Food Funct. 2018, 9, 688–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelkman, C.L. Effects of the glycemic index of foods on serum concentrations of high-density lipoprotein cholesterol and triglycerides. Curr. Atheroscler. Rep. 2001, 3, 456–461. [Google Scholar] [CrossRef] [PubMed]
- De Roos, A.; van der Grond, J.; Mitchell, G.; Westenberg, J. Magnetic Resonance Imaging of Cardiovascular Function and the Brain: Is Dementia a Cardiovascular-Driven Disease? Circulation 2017, 135, 2178–2195. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, C.M. Type 2 diabetes mellitus, dyslipidemia, and Alzheimer’s disease. J. Alzheimers Dis. 2010, 20, 711–722. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet and Lifestyle Drive the Pandemic of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [Green Version]
- Gardener, S.L.; Rainey-Smith, S.R.; Barnes, M.B.; Sohrabi, H.R.; Weinborn, M.; Lim, Y.Y.; Harrington, K.; Taddei, K.; Gu, Y.; Rembach, A.; et al. Dietary patterns and cognitive decline in an Australian study of ageing. Mol. Psychiatry 2015, 20, 860–866. [Google Scholar] [CrossRef]
- Shakersain, B.; Rizzuto, D.; Larsson, S.C.; Faxén-Irving, G.; Fratiglioni, L.; Xu, W.L. The Nordic Prudent Diet Reduces Risk of Cognitive Decline in the Swedish Older Adults: A Population-Based Cohort Study. Nutrients 2018, 10, 229. [Google Scholar] [CrossRef] [Green Version]
- Szczechowiak, K.; Diniz, B.S.; Leszek, J. Diet and Alzheimer’s dementia—Nutritional approach to modulate inflammation. Pharmacol. Biochem. Behav. 2019, 184, 172743. [Google Scholar] [CrossRef]
- Liu, X.; Morris, M.C.; Dhana, K.; Ventrelle, J.; Johnson, K.; Bishop, L.; Hollings, C.S.; Boulin, A.; Laranjo, N.; Stubbs, B.J.; et al. Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) study: Rationale, design and baseline characteristics of a randomized control trial of the MIND diet on cognitive decline. Contemp. Clin. Trials. 2021, 102, 106270. [Google Scholar] [CrossRef]
- Gutierrez, L.; Folch, A.; Rojas, M.; Cantero, J.L.; Atienza, M.; Folch, J.; Camins, A.; Ruiz, A.; Papandreou, C.; Bulló, M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients 2021, 13, 3728. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.B.; Keys, M. How to Eat Well and Stay Well the Mediterranean Way; Doubleday: New York, NY, USA, 1975. [Google Scholar]
- Scarmeas, N.; Stern, Y.; Mayeux, R.; Manly, J.J.; Schupf, N.; Luchsinger, J.A. Mediterranean diet and mild cognitive impairment. Arch. Neurol. 2009, 66, 216–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, C.; Sommerlad, A.; Lyketsos, C.G.; Livingston, G. Modifiable predictors of dementia in mild cognitive impairment: A systematic review and meta-analysis. Am. J. Psychiatry 2015, 172, 323–334. [Google Scholar] [CrossRef] [Green Version]
- Bajerska, J.; Woźniewicz, M.; Suwalska, A.; Jeszka, J. Eating patterns are associated with cognitive function in the elderly at risk of metabolic syndrome from rural areas. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3234–3245. [Google Scholar]
- Trichopoulou, A.; Kyrozis, A.; Rossi, M.; Katsoulis, M.; Trichopoulos, D.; La Vecchia, C.; Lagiou, P. Mediterranean diet and cognitive decline over time in an elderly Mediterranean population. Eur. J. Nutr. 2015, 54, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Stern, Y.; Tang, M.X.; Mayeux, R.; Luchsinger, J.A. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2006, 59, 912–921. [Google Scholar] [CrossRef] [Green Version]
- van de Rest, O.; Berendsen, A.A.; Haveman-Nies, A.; de Groot, L.C. Dietary patterns, cognitive decline, and dementia: A systematic review. Adv. Nutr. 2015, 6, 154–168. [Google Scholar] [CrossRef] [Green Version]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic Longitudinal Investigation of Ageing and Diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef] [Green Version]
- Loughrey, D.G.; Lavecchia, S.; Brennan, S.; Lawlor, B.A.; Kelly, M.E. The Impact of the Mediterranean Diet on the Cognitive Functioning of Healthy Older Adults: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 571–586. [Google Scholar] [CrossRef]
- Samieri, C.; Okereke, O.I.; EDevore, E.; Grodstein, F. Long-term adherence to the Mediterranean diet is associated with overall cognitive status, but not cognitive decline, in women. J. Nutr. 2013, 143, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Kesse-Guyot, E.; Andreeva, V.A.; Lassale, C.; Ferry, M.; Jeandel, C.; Hercberg, S.; Galan, P. SU.VI.MAX 2 Research Group. Mediterranean diet and cognitive function: A French study. Am. J. Clin. Nutr. 2013, 97, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangney, C.C.; Kwasny, M.J.; Li, H.; Wilson, R.S.; Evans, D.A.; Morris, M.C. Adherence to a Mediterranean-type dietary pattern and cognitive decline in a community population. Am. J. Clin. Nutr. 2011, 93, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SACN. SACN Statement on Diet, Cognitive Impairment and Dementia; Public Health England: London, UK, 2018.
- Tangney, C.C.; Li, H.; Wang, Y.; Barnes, L.; Schneider, J.A.; Bennett, D.A.; Morris, M.C. Relation of DASH- and Mediterranean-like dietary patterns to cognitive decline in older persons. Neurology 2014, 83, 1410–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbete, C.; Toledo, E.; Toledo, J.B.; Bes-Rastrollo, M.; Buil-Cosiales, P.; Marti, A.; Guillén-Grima, F.; Martínez-González, M.A. Mediterranean diet and cognitive function: The SUN project. J. Nutr. Health Aging 2015, 19, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Koyama, A.; Houston, D.K.; Simonsick, E.M.; Lee, J.S.; Ayonayon, H.N.; Shahar, D.R.; Rosano, C.; Satterfield, S.; Yaffe, K. Association between the Mediterranean diet and cognitive decline in a biracial population. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, B.; Adair, L.S.; Plassman, B.L.; Batis, C.; Edwards, L.J.; Popkin, B.M.; Mendez, M.A. Dietary Patterns and Cognitive Decline Among Chinese Older Adults. Epidemiology 2015, 26, 758–768. [Google Scholar] [CrossRef] [Green Version]
- Bhushan, A.; Fondell, E.; Ascherio, A.; Yuan, C.; Grodstein, F.; Willett, W. Adherence to Mediterranean diet and subjective cognitive function in men. Eur. J. Epidemiol. 2018, 33, 223–234. [Google Scholar] [CrossRef]
- Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Colpo, M.; Ferrucci, L.; Bandinelli, S. Adherence to a Mediterranean Diet Protects from Cognitive Decline in the Invecchiare in Chianti Study of Aging. Nutrients 2018, 10, 2007. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Galiot, A.; Goñi, I. Adherence to the Mediterranean diet pattern, cognitive status and depressive symptoms in an elderly non-institutionalized population. Nutr. Hosp. 2017, 34, 338–344. [Google Scholar] [CrossRef]
- McEvoy, C.T.; Guyer, H.; Langa, K.M.; Yaffe, K. Neuroprotective Diets Are Associated with Better Cognitive Function: The Health and Retirement Study. J. Am. Geriatr. Soc. 2017, 65, 1857–1862. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.; Chan, D.; Woo, J. A cross sectional study to examine the association between dietary patterns and cognitive impairment in older Chinese people in Hong Kong. J. Nutr. Health Aging 2013, 17, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Samieri, C.; Grodstein, F.; Rosner, B.A.; Kang, J.H.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Willett, W.C.; Okereke, O.I. Mediterranean diet and cognitive function in older age. Epidemiology 2013, 24, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Vercambre, M.N.; Grodstein, F.; Berr, C.; Kang, J.H. Mediterranean diet and cognitive decline in women with cardiovascular disease or risk factors. J. Acad. Nutr. Diet. 2012, 112, 816–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.O.; Geda, Y.E.; Cerhan, J.R.; Knopman, D.S.; Cha, R.H.; Christianson, T.J.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; O’Connor, H.M.; et al. Vegetables, unsaturated fats, moderate alcohol intake, and mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2010, 29, 413–423. [Google Scholar] [CrossRef] [Green Version]
- Cherbuin, N.; Anstey, K.J. The Mediterranean diet is not related to cognitive change in a large prospective investigation: The PATH Through Life study. Am. J. Geriatr. Psychiatry 2012, 20, 635–639. [Google Scholar] [CrossRef]
- Gardener, S.; Gu, Y.; Rainey-Smith, S.R.; Keogh, J.B.; Clifton, P.M.; Mathieson, S.L.; Taddei, K.; Mondal, A.; Ward, V.K.; Scarmeas, N.; et al. Adherence to a Mediterranean diet and Alzheimer’s disease risk in an Australian population. Transl. Psychiatry 2012, 2, e164. [Google Scholar] [CrossRef] [Green Version]
- Olsson, E.; Karlström, B.; Kilander, L.; Byberg, L.; Cederholm, T.; Sjögren, P. Dietary patterns and cognitive dysfunction in a 12-year follow-up study of 70 year old men. J. Alzheimers Dis. 2015, 43, 109–119. [Google Scholar] [CrossRef]
- Haring, B.; Wu, C.; Mossavar-Rahmani, Y.; Snetselaar, L.; Brunner, R.; Wallace, R.B.; Neuhouser, M.L.; Wassertheil-Smoller, S. No Association between Dietary Patterns and Risk for Cognitive Decline in Older Women with 9-Year Follow-Up: Data from the Women’s Health Initiative Memory Study. J. Acad. Nutr. Diet. 2016, 116, 921–930.e1. [Google Scholar] [CrossRef] [Green Version]
- Hosking, D.E.; Eramudugolla, R.; Cherbuin, N.; Anstey, K.J. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimers Dement. 2019, 15, 581–589. [Google Scholar] [CrossRef]
- Gregory, S.; Pullen, H.; Ritchie, C.W.; Shannon, O.M.; Stevenson, E.J.; Muniz-Terrera, G. Mediterranean diet and structural neuroimaging biomarkers of Alzheimer’s and cerebrovascular disease: A systematic review. Exp. Gerontol. 2023, 172, 112065. [Google Scholar] [CrossRef]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [Green Version]
- Hill, E.; Goodwill, A.M.; Gorelik, A.; Szoeke, C. Diet and biomarkers of Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol. Aging 2019, 76, 45–52. [Google Scholar] [CrossRef]
- Agarwal, P.; Leurgans, S.E.; Agarwal, S.; Aggarwal, N.; Cherian, L.J.; James, B.D.; Dhana, K.; Barnes, L.L.; Bennett, D.A.; Schneider, J.A. Association of Mediterranean-DASH Intervention for Neurodegenerative Delay and Mediterranean Diets with Alzheimer Disease Pathology. Neurology 2023, 10, 1212. [Google Scholar] [CrossRef]
- Cowell, O.R.; Mistry, N.; Deighton, K.; Matu, J.; Griffiths, A.; Minihane, A.M.; Mathers, J.C.; Shannon, O.M.; Siervo, M. Effects of a Mediterranean diet on blood pressure: A systematic review and meta-analysis of randomized controlled trials and observational studies. J. Hypertens. 2021, 39, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Shannon, O.M.; Ashor, A.W.; Scialo, F.; Saretzki, G.; Martin-Ruiz, C.; Lara, J.; Matu, J.; Griffiths, A.; Robinson, N.; Lillà, L.; et al. Mediterranean diet and the hallmarks of ageing. Eur. J. Clin. Nutr. 2021, 75, 1176–1192. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, A.; Barul, C.; Féart, C.; Helmer, C.; Bernard, C.; Periot, O.; Dilharreguy, B.; Dartigues, J.F.; Allard, M.; Barberger-Gateau, P.; et al. Mediterranean diet and preserved brain structural connectivity in older subjects. Alzheimers Dement. 2015, 11, 1023–1031. [Google Scholar] [CrossRef]
- Rodrigues, B.; Coelho, A.; Portugal-Nunes, C.; Magalhães, R.; Moreira, P.S.; Castanho, T.C.; Amorim, L.; Marques, P.; Soares, J.M.; Sousa, N.; et al. Higher Adherence to the Mediterranean Diet Is Associated With Preserved White Matter Integrity and Altered Structural Connectivity. Front. Neurosci. 2020, 14, 786. [Google Scholar] [CrossRef]
- Mosconi, L.; Walters, M.; Sterling, J.; Quinn, C.; McHugh, P.; Andrews, R.E.; Matthews, D.C.; Ganzer, C.; Osorio, R.S.; Isaacson, R.S.; et al. Lifestyle and vascular risk effects on MRI-based biomarkers of Alzheimer’s disease: A cross-sectional study of middle-aged adults from the broader New York City area. BMJ Open 2018, 8, e019362. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Gaynor, A.M.; Cruz, E.; Lee, S.; Gazes, Y.; Habeck, C.; Stern, Y.; Gu, Y. Mediterranean Diet and White Matter Hyperintensity Change over Time in Cognitively Intact Adults. Nutrients 2022, 14, 3664. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreu-Reinón, M.E.; Chirlaque, M.D.; Gavrila, D.; Amiano, P.; Mar, J.; Tainta, M.; Ardanaz, E.; Larumbe, R.; Colorado-Yohar, S.M.; Navarro-Mateu, F.; et al. Mediterranean Diet and Risk of Dementia and Alzheimer’s Disease in the EPIC-Spain Dementia Cohort Study. Nutrients 2021, 13, 700. [Google Scholar] [CrossRef] [PubMed]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Brickman, A.M.; Stern, Y.; Habeck, C.G.; Razlighi, Q.R.; Luchsinger, J.A.; Manly, J.J.; Schupf, N.; Mayeux, R.; Scarmeas, N. Mediterranean diet and brain structure in a multiethnic elderly cohort. Neurology 2015, 85, 1744–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croll, P.H.; Voortman, T.; Ikram, M.A.; Franco, O.H.; Schoufour, J.D.; Bos, D.; Vernooij, M.W. Better diet quality relates to larger brain tissue volumes: The Rotterdam Study. Neurology 2018, 90, e2166–e2173. [Google Scholar] [CrossRef]
- Staubo, S.C.; Aakre, J.A.; Vemuri, P.; Syrjanen, J.A.; Mielke, M.M.; Geda, Y.E.; Kremers, W.K.; Machulda, M.M.; Knopman, D.S.; Petersen, R.C.; et al. Mediterranean diet, micronutrients and macronutrients, and MRI measures of cortical thickness. Alzheimer’s Dement. 2017, 13, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Gardener, H.; Scarmeas, N.; Gu, Y.; Boden-Albala, B.; Elkind, M.S.; Sacco, R.L.; DeCarli, C.; Wright, C.B. Mediterranean diet and white matter hyperintensity volume in the Northern Manhattan Study. Arch. Neurol. 2012, 69, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Tong, T.Y.N.; Imamura, F.; Monsivais, P.; Brage, S.; Griffin, S.J.; Wareham, N.J.; Forouhi, N.G. Dietary cost associated with adherence to the Mediterranean diet, and its variation by socio-economic factors in the UK Fenland Study. Br. J. Nutr. 2018, 119, 685–694. [Google Scholar] [CrossRef] [Green Version]
- Pastor, R.; Pinilla, N.; Tur, J.A. The Economic Cost of Diet and Its Association with Adherence to the Mediterranean Diet in a Cohort of Spanish Primary Schoolchildren. Int. J. Environ. Res. Public Health 2021, 18, 1282. [Google Scholar] [CrossRef]
- Bonaccio, M.; Iacoviello, L.; de Gaetano, G.; Moli-Sani, I. The Mediterranean diet: The reasons for a success. Thromb. Res. 2012, 129, 401–404. [Google Scholar] [CrossRef]
- Gallaway, P.J.; Miyake, H.; Buchowski, M.S.; Shimada, M.; Yoshitake, Y.; Kim, A.S.; Hongu, N. Physical Activity: A Viable Way to Reduce the Risks of Mild Cognitive Impairment, Alzheimer’s Disease, and Vascular Dementia in Older Adults. Brain Sci. 2017, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommerlad, A.; Sabia, S.; Singh-Manoux, A.; Lewis, G.; Livingston, G. Association of social contact with dementia and cognition: 28-year follow-up of the Whitehall II cohort study. PLoS Med. 2019, 16, e1002862. [Google Scholar] [CrossRef] [Green Version]
- Titova, O.E.; Ax, E.; Brooks, S.J.; Sjögren, P.; Cederholm, T.; Kilander, L.; Kullberg, J.; Larsson, E.M.; Johansson, L.; Ahlström, H.; et al. Mediterranean diet habits in older individuals: Associations with cognitive functioning and brain volumes. Exp. Gerontol. 2013, 48, 1443–1448. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karstens, A.J.; Tussing-Humphreys, L.; Zhan, L.; Rajendran, N.; Cohen, J.; Dion, C.; Zhou, X.J.; Lamar, M. Associations of the Mediterranean diet with cognitive and neuroimaging phenotypes of dementia in healthy older adults. Am. J. Clin. Nutr. 2019, 109, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Smith, P.J.; Mabe, S.; Hinderliter, A.; Welsh-Bohmer, K.; Browndyke, J.N.; Lin, P.H.; Kraus, W.; Doraiswamy, P.M.; Burke, J.; et al. Lifestyle and Neurocognition in Older Adults With Cardiovascular Risk Factors and Cognitive Impairment. Psychosom. Med. 2017, 79, 719–727. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Babyak, M.A.; Craighead, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Strauman, T.A.; Sherwood, A. Effects of the dietary approaches to stop hypertension diet, exercise, and caloric restriction on neurocognition in overweight adults with high blood pressure. Hypertension 2010, 55, 1331–1338. [Google Scholar] [CrossRef] [Green Version]
- Wengreen, H.; Munger, R.G.; Cutler, A.; Quach, A.; Bowles, A.; Corcoran, C.; Tschanz, J.T.; Norton, M.C.; Welsh-Bohmer, K.A. Prospective study of Dietary Approaches to Stop Hypertension- and Mediterranean-style dietary patterns and age-related cognitive change: The Cache County Study on Memory, Health and Aging. Am. J. Clin. Nutr. 2013, 98, 1263–1271. [Google Scholar] [CrossRef] [Green Version]
- Tsivgoulis, G.; Judd, S.; Letter, A.J.; Alexandrov, A.V.; Howard, G.; Nahab, F.; Unverzagt, F.W.; Moy, C.; Howard, V.J.; Kissela, B.; et al. Adherence to a Mediterranean diet and risk of incident cognitive impairment. Neurology 2013, 80, 1684–1692. [Google Scholar] [CrossRef] [Green Version]
- Gallucci, M.; Mazzuco, S.; Ongaro, F.; Di Giorgi, E.; Mecocci, P.; Cesari, M.; Albani, D.; Forloni, G.L.; Durante, E.; Gajo, G.B.; et al. Body mass index, lifestyles, physical performance and cognitive decline: The "Treviso Longeva (TRELONG)" study. J. Nutr. Health Aging 2013, 17, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Katsiardanis, K.; Diamantaras, A.A.; Dessypris, N.; Michelakos, T.; Anastasiou, A.; Katsiardani, K.P.; Kanavidis, P.; Papadopoulos, F.C.; Stefanadis, C.; Panagiotakos, D.B.; et al. Cognitive impairment and dietary habits among elders: The Velestino Study. J. Med. Food. 2013, 16, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an Australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef]
- Corley, J.; Starr, J.M.; McNeill, G.; Deary, I.J. Do dietary patterns influence cognitive function in old age? Int. Psychogeriatr. 2013, 25, 1393–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, S.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) on serum inflammatory markers: A systematic review and meta-analysis of randomized trials. Clin. Nutr. 2018, 37, 542–550. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Russo, M.; Barbieri, M. Dietary patterns and cognition in older persons. Curr. Opini. Clini. Nutri. Metabol. Care. 2018, 21, 10–13. [Google Scholar] [CrossRef]
- Berendsen, A.A.M.; Kang, J.H.; van de Rest, O.; Feskens, E.J.M.; de Groot, L.C.P.G.M.; Grodstein, F. The Dietary Approaches to Stop Hypertension Diet, Cognitive Function, and Cognitive Decline in American Older Women. J. Am. Med. Dir. Assoc. 2017, 18, 427–432. [Google Scholar] [CrossRef]
- Nishi, S.K.; Babio, N.; Gómez-Martínez, C.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Castañer, O.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Mediterranean, DASH, and MIND Dietary Patterns and Cognitive Function: The 2-Year Longitudinal Changes in an Older Spanish Cohort. Front. Aging Neurosci. 2021, 13, 782067. [Google Scholar] [CrossRef]
- Daniel, G.D.; Chen, H.; Bertoni, A.G.; Rapp, S.R.; Fitzpatrick, A.L.; Luchsinger, J.A.; Wood, A.C.; Hughes, T.M.; Burke, G.L.; Hayden, K.M. DASH diet adherence and cognitive function: Multi-ethnic study of atherosclerosis. Clin. Nutr. ESPEN 2021, 46, 223–231. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Smith, P.J.; Mabe, S.; Hinderliter, A.; Lin, P.H.; Liao, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Kraus, W.E.; Doraiswamy, P.M.; et al. Lifestyle and neurocognition in older adults with cognitive impairments: A randomized trial. Neurology 2019, 92, e212–e223. [Google Scholar] [CrossRef] [Green Version]
- Cherian, L.; Wang, Y.; Fakuda, K.; Leurgans, S.; Aggarwal, N.; Morris, M. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) Diet Slows Cognitive Decline After Stroke. J. Prev. Alzheimers Dis. 2019, 6, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Melo van Lent, D.; O’Donnell, A.; Beiser, A.S.; Vasan, R.S.; DeCarli, C.S.; Scarmeas, N.; Wagner, M.; Jacques, P.F.; Seshadri, S.; Himali, J.J.; et al. Mind Diet Adherence and Cognitive Performance in the Framingham Heart Study. J. Alzheimers Dis. 2021, 82, 827–839. [Google Scholar] [CrossRef]
- Boumenna, T.; Scott, T.M.; Lee, J.S.; Zhang, X.; Kriebel, D.; Tucker, K.L.; Palacios, N. MIND Diet and Cognitive Function in Puerto Rican Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Tao, Y.; Chen, H.; Chen, X.; Shen, J.; Zhao, C.; Xu, X.; He, M.; Zhu, D.; Zhang, R.; et al. Mediterranean-Dietary Approaches to Stop Hypertension Intervention for Neurodegenerative Delay (MIND) Diet and Cognitive Function and its Decline: A Prospective Study and Meta-analysis of Cohort Studies. Am. J. Clin. Nutr. 2023, 118, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Berendsen, A.M.; Kang, J.H.; Feskens, E.J.M.; de Groot, C.P.G.M.; Grodstein, F.; van de Rest, O. Association of Long-Term Adherence to the MIND Diet with Cognitive Function and Cognitive Decline in American Women. J. Nutr. Health Aging 2018, 22, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Adjibade, M.; Assmann, K.E.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Prospective association between adherence to the MIND diet and subjective memory complaints in the French NutriNet-Santé cohort. J. Neurol. 2019, 266, 942–952. [Google Scholar] [CrossRef]
- Dhana, K.; James, B.D.; Agarwal, P.; Aggarwal, N.T.; Cherian, L.J.; Leurgans, S.E.; Barnes, L.L.; Bennett, D.A.; Schneider, J.A. MIND Diet, Common Brain Pathologies, and Cognition in Community-Dwelling Older Adults. J. Alzheimers Dis. 2021, 83, 683–692. [Google Scholar] [CrossRef]
- Huang, X.; Aihemaitijiang, S.; Ye, C.; Halimulati, M.; Wang, R.; Zhang, Z. Development of the cMIND Diet and Its Association with Cognitive Impairment in Older Chinese People. J. Nutr. Health Aging 2022, 26, 760–770. [Google Scholar] [CrossRef]
- Arjmand, G.; Abbas-Zadeh, M.; Eftekhari, M.H. Effect of MIND diet intervention on cognitive performance and brain structure in healthy obese women: A randomized controlled trial. Sci. Rep. 2022, 12, 2871. [Google Scholar] [CrossRef]
- Ahn, S.; Lingerfelt, C.N.; Lee, C.E.; Lee, J.A.; Raynor, H.A.; Anderson, J.G. Association of adherence to high-intensity physical activity and the Mediterranean-dietary approaches to stop hypertension intervention for neurodegenerative delay diet with cognition: A cross-sectional study. Int. J. Nurs. Stud. 2022, 131, 104243. [Google Scholar] [CrossRef]
- Wesselman, L.M.P.; van Lent, D.M.; Schröder, A.; van de Rest, O.; Peters, O.; Menne, F.; Fuentes, M.; Priller, J.; Spruth, E.J.; Altenstein, S.; et al. Dietary patterns are related to cognitive functioning in elderly enriched with individuals at increased risk for Alzheimer’s disease. Eur. J. Nutr. 2021, 60, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Calil, S.R.B.; Brucki, S.M.D.; Nitrini, R.; Yassuda, M.S. Adherence to the Mediterranean and MIND diets is associated with better cognition in healthy seniors but not in MCI or AD. Clin. Nutr. ESPEN 2018, 28, 201–207. [Google Scholar] [CrossRef]
- Munoz-Garcia, M.I.; Toledo, E.; Razquin, C.; Dominguez, L.J.; Maragarone, D.; Martinez-Gonzalez, J.; Martinez-Gonzalez, M.A. “A priori” dietary patterns and cognitive function in the SUN project. Neuroepidemiology 2020, 54, 45–57. [Google Scholar] [CrossRef]
- Nabbout, R.; Mazzuca, M.; Hubert, P.; Peudennier, S.; Allaire, C.; Flurin, V.; Aberastury, M.; Silva, W.; Dulac, O. Efficacy of ketogenic diet in severe refractory status epilepticus initiating fever induced refractory epileptic encephalopathy in school age children (FIRES). Epilepsia 2010, 51, 2033–2037. [Google Scholar] [CrossRef] [PubMed]
- Morrill, S.J.; Gibas, K.J. Ketogenic diet rescues cognition in ApoE4+ patient with mild Alzheimer’s disease: A case study. Diabetes Metab. Syndr. 2019, 13, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Goulis, D.G.; Gkiouras, K.; Theodoridis, X.; Gkouskou, K.K.; Evangeliou, A.; Dardiotis, E.; Bogdanos, D.P. To Keto or Not to Keto? A Systematic Review of Randomized Controlled Trials Assessing the Effects of Ketogenic Therapy on Alzheimer Disease. Adv. Nutr. 2020, 11, 1583–1602. [Google Scholar] [CrossRef]
- Lin, A.; Turner, Z.; Doerrer, S.C.; Stanfield, A.; Kossoff, E.H. Complications During Ketogenic Diet Initiation: Prevalence, Treatment, and Influence on Seizure Outcomes. Pediatr. Neurol. 2017, 68, 35–39. [Google Scholar] [CrossRef]
- Taylor, M.K.; Swerdlow, R.H.; Burns, J.M.; Sullivan, D.K. An Experimental Ketogenic Diet for Alzheimer Disease Was Nutritionally Dense and Rich in Vegetables and Avocado. Curr. Dev. Nutr. 2019, 3, nzz003. [Google Scholar] [CrossRef] [Green Version]
- Brinkley, T.E.; Leng, I.; Register, T.C.; Neth, B.J.; Zetterberg, H.; Blennow, K.; Craft, S. Changes in Adiposity and Cerebrospinal Fluid Biomarkers Following a Modified Mediterranean Ketogenic Diet in Older Adults at Risk for Alzheimer’s Disease. Front. Neurosci. 2022, 16, 906539. [Google Scholar] [CrossRef]
- Neth, B.J.; Mintz, A.; Whitlow, C.; Jung, Y.; Solingapuram Sai, K.; Register, T.C.; Kellar, D.; Lockhart, S.N.; Hoscheidt, S.; Maldjian, J.; et al. Modified ketogenic diet is associated with improved cerebrospinal fluid biomarker profile, cerebral perfusion, and cerebral ketone body uptake in older adults at risk for Alzheimer’s disease: A pilot study. Neurobiol. Aging 2020, 86, 54–63. [Google Scholar] [CrossRef]
- Nagpal, R.; Neth, B.J.; Wang, S.; Craft, S.; Yadav, H. Modified Mediterranean-ketogenic diet modulates gut microbiome and short-chain fatty acids in association with Alzheimer’s disease markers in subjects with mild cognitive impairment. EBioMedicine 2019, 47, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, M.C.L.; Deprez, L.M.; Mortimer, G.M.N.; Murtagh, D.K.J.; McCoy, S.; Mylchreest, R.; Gilbertson, L.J.; Clark, K.M.; Simpson, P.V.; McManus, E.J.; et al. Randomized crossover trial of a modified ketogenic diet in Alzheimer’s disease. Alzheimers Res. Ther. 2021, 13, 51. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Niu, X.; Peng, D. Eat for better cognition in older adults at risk for Alzheimer’s disease. Nutrition 2023, 109, 111969. [Google Scholar] [CrossRef]
- Fraser, G.E. Vegetarian diets: What do we know of their effects on common chronic diseases? Am. J. Clin. Nutr. 2009, 89, 1607S–1612S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satija, A.; Hu, F.B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 2018, 28, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Dhana, K.; Barnes, L.L.; Tangney, C.C.; Agarwal, P.; Aggarwal, N.; Holland, T.M.; Beck, T.; Evans, D.A.; Rajan, K.B. A healthy plant-based diet was associated with slower cognitive decline in African American older adults: A biracial community-based cohort. Am. J. Clin. Nutr. 2022, 116, 875–886. [Google Scholar] [CrossRef]
- Mottaghi, T.; Amirabdollahian, F.; Haghighatdoost, F. Fruit and vegetable intake and cognitive impairment: A systematic review and meta-analysis of observational studies. Eur. J. Clin. Nutr. 2018, 72, 1336–1344. [Google Scholar] [CrossRef]
- Gatto, N.M.; Garcia-Cano, J.; Irani, C.; Jaceldo-Siegl, K.; Liu, T.; Chen, Z.; Paul, J.; Fraser, G.; Wang, C.; Lee, G.J. Vegetarian Dietary Patterns and Cognitive Function among Older Adults: The Adventist Health Study-2. J. Nutr. Gerontol. Geriatr. 2021, 40, 197–214. [Google Scholar] [CrossRef]
- Tsai, J.H.; Huang, C.F.; Lin, M.N.; Chang, C.E.; Chang, C.C.; Lin, C.L. Taiwanese Vegetarians Are Associated with Lower Dementia Risk: A Prospective Cohort Study. Nutrients 2022, 14, 588. [Google Scholar] [CrossRef]
- Foote, J.A.; Giuliano, A.R.; Harris, R.B. Older adults need guidance to meet nutritional recommendations. J. Am. Coll. Nutr. 2000, 19, 628–640. [Google Scholar] [CrossRef] [Green Version]
- Yeh, T.S.; Yuan, C.; Ascherio, A.; Rosner, B.A.; Blacker, D.; Willett, W.C. Long-term dietary protein intake and subjective cognitive decline in US men and women. Am. J. Clin. Nutr. 2022, 115, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and adequacy of the vegan diet. A systematic review of the evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [PubMed]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Ärzteblatt Int. 2020, 117, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Katonova, A.; Sheardova, K.; Amlerova, J.; Angelucci, F.; Hort, J. Effect of a Vegan Diet on Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 23, 14924. [Google Scholar] [CrossRef] [PubMed]
- Tolppanen, A.M.; Solomon, A.; Kulmala, J.; Kåreholt, I.; Ngandu, T.; Rusanen, M.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Leisure-time physical activity from mid- to late life, body mass index, and risk of dementia. Alzheimers Dement. 2015, 11, 434–443.e6. [Google Scholar] [CrossRef] [PubMed]
- Kępka, A.; Ochocińska, A.; Borzym-Kluczyk, M.; Chojnowska, S.; Skorupa, E.; Przychodzeń, M.; Waszkiewicz, N. Healthy Food Pyramid as Well as Physical and Mental Activity in the Prevention of Alzheimer’s Disease. Nutrients 2022, 14, 1534. [Google Scholar] [CrossRef]
- Hoscheidt, S.; Sanderlin, A.H.; Baker, L.D.; Jung, Y.; Lockhart, S.; Kellar, D.; Whitlow, C.T.; Hanson, A.J.; Friedman, S.; Register, T.; et al. Mediterranean and Western diet effects on Alzheimer’s disease biomarkers, cerebral perfusion, and cognition in mid-life: A randomized trial. Alzheimers Dement. 2022, 18, 457–468. [Google Scholar] [CrossRef]
- Féart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Hu, E.A.; Wu, A.; Dearborn, J.L.; Gottesman, R.F.; Sharrett, A.R.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Adherence to Dietary Patterns and Risk of Incident Dementia: Findings from the Atherosclerosis Risk in Communities Study. J. Alzheimers Dis. 2020, 78, 827–835. [Google Scholar] [CrossRef]
- Benus, R.F.; van der Werf, T.S.; Welling, G.W.; Judd, P.A.; Taylor, M.A.; Harmsen, H.J.; Whelan, K. Association between Faecalibacterium prausnitzii and dietary fibre in colonic fermentation in healthy human subjects. Br. J. Nutr. 2010, 104, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Mantrana, I.; Selma-Royo, M.; Alcantara, C.; Collado, M.C. Shifts on Gut Microbiota Associated to Mediterranean Diet Adherence and Specific Dietary Intakes on General Adult Population. Front. Microbiol. 2018, 9, 890. [Google Scholar] [CrossRef] [Green Version]
- Cremonini, A.L.; Caffa, I.; Cea, M.; Nencioni, A.; Odetti, P.; Monacelli, F. Nutrients in the Prevention of Alzheimer’s Disease. Oxid. Med. Cell Longev. 2019, 2019, 9874159. [Google Scholar] [CrossRef] [Green Version]
- Rajaram, S.; Jones, J.; Lee, G.J. Plant-Based Dietary Patterns, Plant Foods, and Age-Related Cognitive Decline. Adv. Nutr. 2019, 10 (Suppl. S4), S422–S436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, A.; Trabelsi, K.; Boukhris, O.; Bouaziz, B.; Müller, P.; MGlenn, J.; Bott, N.T.; Müller, N.; Chtourou, H.; Driss, T.; et al. Effects of Polyphenol-Rich Interventions on Cognition and Brain Health in Healthy Young and Middle-Aged Adults: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1598. [Google Scholar] [CrossRef] [PubMed]
- Travica, N.; D’Cunha, N.M.; Naumovski, N.; Kent, K.; Mellor, D.D.; Firth, J.; Georgousopoulou, E.N.; Dean, O.M.; Loughman, A.; Jacka, F.; et al. The effect of blueberry interventions on cognitive performance and mood: A systematic review of randomized controlled trials. Brain Behav. Immun. 2020, 85, 96–105. [Google Scholar] [CrossRef]
- Holland, T.M.; Agarwal, P.; Wang, Y.; Leurgans, S.E.; Bennett, D.A.; Booth, S.L.; Morris, M.C. Dietary flavonols and risk of Alzheimer dementia. Neurology 2020, 94, e1749–e1756. [Google Scholar] [CrossRef]
- Ozawa, M.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A.; Brunner, E.J. Dietary pattern, inflammation and cognitive decline: The Whitehall II prospective cohort study. Clin. Nutr. 2017, 36, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.Y.; Chiu, C.C.; Huang, S.Y. SUKP A meta-analytic review of polyunsaturated fatty acid compositions in dementia. J. Clin. Psychiatry 2012, 73, 1245–1254. [Google Scholar] [CrossRef]
- Theodore, L.E.; Kellow, N.J.; McNeil, E.A.; Close, E.O.; Coad, E.G.; Cardoso, B.R. Nut Consumption for Cognitive Performance: A Systematic Review. Adv. Nutr. 2021, 12, 777–792. [Google Scholar] [CrossRef]
- Simonetto, M.; Infante, M.; Sacco, R.L.; Rundek, T.; Della-Morte, D. A Novel Anti-Inflammatory Role of Omega-3 PUFAs in Prevention and Treatment of Atherosclerosis and Vascular Cognitive Impairment and Dementia. Nutrients 2019, 11, 2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulose, S.M.; Miller, M.G.; Scott, T.; Shukitt-Hale, B. Nutritional Factors Affecting Adult Neurogenesis and Cognitive Function. Adv. Nutr. 2017, 8, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Farina, N.; Llewellyn, D.; Isaac, M.G.; Tabet, N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2017, 1, CD002854. [Google Scholar] [PubMed]
- An, Y.; Feng, L.; Zhang, X.; Wang, Y.; Wang, Y.; Tao, L.; Qin, Z.; Xiao, R. Dietary intakes and biomarker patterns of folate, vitamin B6, and vitamin B12 can be associated with cognitive impairment by hypermethylation of redox-related genes NUDT15 and TXNRD1. Clin. Epigenetics 2019, 11, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setola, E.; Monti, L.D.; Galluccio, E.; Palloshi, A.; Fragasso, G.; Paroni, R.; Magni, F.; Sandoli, E.P.; Lucotti, P.; Costa, S.; et al. Insulin resistance and endothelial function are improved after folate and vitamin B12 therapy in patients with metabolic syndrome: Relationship between homocysteine levels and hyperinsulinemia. Eur. J. Endocrinol. 2004, 151, 483–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Gueant-Rodriguez, R.M.; Quilliot, D.; Sirveaux, M.A.; Meyre, D.; Gueant, J.L.; Brunaud, L. Folate and vitamin B12 status is associated with insulin resistance and metabolic syndrome in morbid obesity. Clin. Nutr. 2018, 37, 1700–1706. [Google Scholar] [CrossRef]
- Wong, S.K.; Chin, K.Y.; Suhaimi, F.H.; Ahmad, F.; Ima-Nirwana, S. Vitamin E As a Potential Interventional Treatment for Metabolic Syndrome: Evidence from Animal and Human Studies. Front. Pharmacol. 2017, 8, 444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Luo, M.; Wei, S. The Bioprotective Effects of Polyphenols on Metabolic Syndrome against Oxidative Stress: Evidences and Perspectives. Oxid. Med. Cell Longev. 2019, 2019, 6713194. [Google Scholar] [CrossRef] [Green Version]
- Mak, T.N.; Caldeira, S. The Role of Nutrition in Active and Healthy Ageing. for Prevention and Treatment of Age-Related Diseases: Evidence So Far; Publications Office of the European Union: Luxembourg, 2014; Available online: https://publications.jrc.ec.europa.eu/repository/handle/JRC90454 (accessed on 1 April 2023).
- Han, Y.; Li, S.; Zheng, Y. Predictors of nutritional status among community-dwelling older adults in Wuhan, China. Public Health Nutr. 2009, 12, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Bloom, I.; Edwards, M.; Jameson, K.A.; Syddall, H.E.; Dennison, E.; Gale, C.R.; Baird, J.; Cooper, C.; Aihie Sayer, A.; Robinson, S. Influences on diet quality in older age: The importance of social factors. Age Ageing 2017, 46, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Host, A.; McMahon, A.T.; Walton, K.; Charlton, K. Factors Influencing Food Choice for Independently Living Older People-A Systematic Literature Review. J. Nutr. Gerontol. Geriatr. 2016, 35, 67–94. [Google Scholar] [CrossRef] [PubMed]
- Aravanis, C.; Corcondilas, A.; Dontas, A.S.; Lekos, D.; Keys, A. Coronary heart disease in seven countries. IX. The Greek islands of Crete and Corfu. Circulation 1970, 41 (Suppl. S4), I88–I100. [Google Scholar] [CrossRef] [PubMed]
- Parrott, M.D.; Shatenstein, B.; Ferland, G.; Payette, H.; Morais, J.A.; Belleville, S.; Kergoat, M.J.; Gaudreau, P.; Greenwood, C.E. Relationship between diet quality and cognition depends on socioeconomic position in healthy older adults. J. Nutr. 2013, 143, 1767–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, P.H.; Chen, J.H.; Chiou, J.M.; Tu, Y.K.; Chen, T.F.; Chiu, M.J.; Tang, S.C.; Yeh, S.J.; Chen, Y.C. The effect of lifestyle on late-life cognitive change under different socioeconomic status. PLoS ONE 2018, 13, e0197676. [Google Scholar] [CrossRef] [Green Version]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.D.; White, L.R.; Ross, G.W.; Masaki, K.H.; Curb, J.D.; Petrovitch, H. Walking and dementia in physically capable elderly men. JAMA 2004, 292, 1447–1453. [Google Scholar] [CrossRef] [Green Version]
- Lenart-Bugla, M.; Łuc, M.; Pawłowski, M.; Szcześniak, D.; Seifert, I.; Wiegelmann, H.; Gerhardus, A.; Wolf-Ostermann, K.; Rouwette, E.A.J.A.; Ikram, M.A.; et al. What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews. Brain Sci. 2022, 12, 1214. [Google Scholar] [CrossRef]
- Jaqua, E.; Biddy, E.; Moore, C.; Browne, G. The Impact of the Six Pillars of Lifestyle Medicine on Brain Health. Cureus 2023, 15, e34605. [Google Scholar] [CrossRef]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Laurin, D.; Verreault, R.; Lindsay, J.; MacPherson, K.; Rockwood, K. Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch. Neurol. 2001, 58, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; Macchi, C. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Mamalaki, E.; Anastasiou, C.A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Social life characteristics in relation to adherence to the Mediterranean diet in older adults: Findings from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD) study. Public Health Nutr. 2020, 23, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Corsi, M.; Di Raimo, T.; Di Lorenzo, C.; Rapp-Ricciardi, M.; Archer, T.; Ricci, S.; Businaro, R. Cognitive disability in alzheimer’s disease and its management. Clin. Ter. 2016, 167, e123–e126. [Google Scholar] [PubMed]

| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults in CCMS study aged over 65 years n = 3580 | 10.6 years | 142-item FFQ, MeDi score, DASH score Global cognition (3 MS) | Associations between DASH and Mediterranean-style dietary patterns and age-related cognitive change. | Higher quintile compared to lower one of DASH score associated with better average cognition but not significantly associated with rate of change in cognitive function. | Age, gender, education, BMI, frequency of moderate physical activity, multivitamin and mineral supplement use, history of drinking and smoking, and history of diabetes, heart attack, or stroke. | [104] |
| Longitudinal | US | Older participants of Memory and Aging Project cognitively normal at enrollment n = 826 (26% M) Age: 81.5 ± 7.1 years | 4.1 years | 144-item FFQ, battery of cognitive tests: episodic memory, semantic memory, working memory, perceptual speed, and visuospatial ability | Association between DASH and Mediterranean diets with slower cognitive decline. | In models adjusted for covariates, a 1-unit increase in DASH score associated with slower rate of global cognitive decline, with a decrease of 0.007 standardized units. | Age, gender, education, participation in cognitive activities, total energy intake (kcal), time, and the interaction between time and each covariate, physical activity, presence of APOE ε4 allele, depression, hypertension, diabetes, and stroke. | [58] |
| Longitudinal | US | Participants of the Rush Memory and Aging Project (MAP) n = 923 (±24% M) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MeDi, -DASH, and MIND scores, AD (based on NINCDS-ADRDA criteria) | Association of MIND, a hybrid Mediterranean and DASH diet, with incident AD. | The highest tertile of DASH diet adherence significantly associated with lower risk of AD. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Postmenopausal women enrolled in the Women’s Health Initiative Memory Study (WHIMS) n = 6425 (0% M) Age: 65–79 years | 9.11 years | FFQ, A-MeDi score, DASH score, MCI (MMSE and battery of neuropsychological tests) | Dietary patterns associated with cognitive decline in older women. Dietary patterns modified cognitive decline risk for women with hypertension. | Higher quintile of DASH score significantly associated with lower risk of MCI. | Age, race, education level, Women Health Initiative hormone trial randomization assignment, baseline 3 MS level, smoking status, physical activity, diabetes, hypertension, BMI, family income, depression, history of CVD, and total energy intake. | [73] |
| Longitudinal | US | Participants from Nurses’ Health Study, n = 16,144 Age: at first cognitive assessment, 74.3 ± 2.3 years | 4.1 years | 116-item SFFQ, DASH, global cognition, and verbal memory (immediate and delayed recalls) | Association between long-term adherence to DASH diet and cognitive function and decline in older American women. | Higher long-term adherence to DASH diet associated with better average global cognition, verbal memory, and TICS, but not with change in global cognition, verbal memory, or TICS score during follow-up. | Age, education, physical activity, caloric intake, alcohol intake, smoking status, multivitamin use, BMI, history of depression, high blood pressure, hypercholesterolemia, myocardial infarction, and diabetes mellitus. | [112] |
| Longitudinal | Sweden | Older community participants n = 2223 (39% men) Age: 69.5 years | 6 years | 98-item SFFQ, A-MedD, A-DASH and MIND scores, dietary components, global cognition (MMSE) | Comparison of association of the different dietary patterns with cognitive decline in an older Scandinavian population. | DASH score not associated with cognitive decline nor with risk of MMSE score ≤ 24. | Age, gender, education, civil status, total caloric intake, BMI, physical activity, smoking, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than those included in each dietary index. | [41] |
| Longitudinal | Spain | Participants in PREDIMED-Plus trial n = 6647 (52% men) Age: 65 years | 2 years | 143-item FFQ, MedD, DASH diet and MIND diet scoring, battery of cognitive tests: MMSE, visuospatial and visuo-constructive capacity, verbal ability and executive function, short-term and working memory | Relationship between baseline adherence to MedD, DASH, and MIND diets with 2-year changes in cognitive performance in older adults with overweight or obesity and high cardiovascular disease risk. | Higher adherence to DASH diet not associated with better cognitive function over 2 years. | Age, gender, education level, and civil status, physical activity, dietary intake, and smoking habit, BMI, personal history of hypertension, hypercholesterolemia, type 2 diabetes, and depression. | [113] |
| Longitudinal | US | Participants in MESA cohort from six communities n= 4169 (1965 M 2204 F) Age: 60.4 ± 9.5 years | 2 years | 120-item FFQ, cognitive function assessment by Cognitive Abilities Screening Instrument (CASI), Digit Symbol Coding (DSC), and Digit Span (DS) | Association between DASH diet and cognitive function in MESA cohort. | DASH diet adherence not associated with cognitive performance or any decline. | Age, gender, race/ethnicity, education, income, acculturation status, presence of APOE ε4 allele, total energy intake, BMI, smoking, Center for Epidemiological Studies Depression (CES-D) scale score, total intentional exercise, diabetes categories, diabetes medication use, antihypertensive medication use, Alzheimer’s medication use, stroke diagnosis, hypertension, use of antihypertensive medications, alcohol intake. | [114] |
| Cross-sectional | US | Sedentary adults with cognitive impairment and CVD risk factors n = 160 (33% men) Age: 65.4 years | NS | FFQ and 4-day food diary, A-MedD and A-DASH scores, verbal memory, visual memory, and executive function/processing speed score | The relationship of lifestyle factors and neurocognitive functioning in older adults with vascular risk factors and cognitive impairment, no dementia. | Higher adherence to DASH diet associated with better verbal memory, but not with executive function/processing speed or visual memory. | Age, education, gender, ethnicity, total caloric intake, family history of dementia, and chronic use of anti-inflammatory medications. | [102] |
| Randomized controlled trial | US | Sedentary older adults n = 160 Aerobic Exercise (AE) + DASH group, n = 40 (14 M 26 F), Age: 64.9 ± 6.2 years AE no DASH, n = 41 (12 M 29 F), Age: 65.8 ± 7.3 years DASH group, n = 41 (15 M 26 F), Age: 66.0 ± 7.1 years HE: Health Education group, n = 38 (12 M 16 F), Age: 64.7 ± 6.6 years | 6 months | FFQ, DASH diet score, battery of tests: executive function, global executive function, cognitive and functional performance | Evaluation of independent and additive effects of AE and DASH diet on executive functioning in adults with cognitive impairments with no dementia. | Participants engaged in AE but not DASH diet demonstrated significant improvements in executive function. Combined AE and DASH diet associated with the largest improvements compared to receiving HE. | NS | [115] |
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults n = 923 (±24% men) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MeDi, A-DASH, and MIND scores | AD (based on NINCDS-ADRDA criteria) | Middle and high tertiles of MIND diet score significantly associated with lower risk of AD. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Older adults n = 960 (25% men) Age: 81.4 years | 4.7 years | 144-item SFFQ, MIND diet score | Global cognition, episodic memory, semantic memory, visuospatial ability, perceptual speed, and working memory | MIND diet score significantly associated with slower ↘ in global cognition; episodic memory; semantic memory; visuospatial ability; perceptual speed; and working memory. Higher tertile of MIND diet score significantly associated with slower ↘ in global cognitive score. | Age, gender, education, participation in cognitive activities, smoking history, physical activity hours per week, total energy intake, presence of APOE ε4 allele, time, history of stroke, myocardial infarction, diabetes, hypertension, and interaction terms between each covariate and time). | [100] |
| Longitudinal | Sweden | Older-adult community residents n = 2223 (39% men) Age: 69.5 years | 6 years | 98-item SFFQ, A-MeDi, A-DASH, and MIND scores, dietary components | Global cognition (MMSE) | Higher MIND score significantly associated with less cognitive decline and lower risk of MMSE score ≤ 24. | Total caloric intake, age, gender, education, civil status, physical activity, smoking, BMI, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than main exposure in each model. | [41] |
| Longitudinal | US | Older women n = 16,058 (0% men) Age: 74.3 years | 12.9 years | 116-item FFQ, MIND score | Global cognition (TICS and composite score of TICS, EBMT) and verbal memory (immediate and delayed recalls). | Higher adherence to MIND diet not significantly associated with less ↘ in global cognition, verbal memory, or TICS score. | Age, education, physical activity, caloric intake, alcohol intake, smoking status, multivitamin use, BMI, depression, and history of hypertension, hypercholesterolemia, myocardial infarction, and diabetes mellitus. | [120] |
| Longitudinal | Australia | Older Australian adults n = 1220 (50% men) Age: 60–64 years | 12 years | CSIRO-FFQ, MeDi, A-MeDi, and MIND scores, dietary components | Cognitive impairment: MCI/dementia | Higher tertile of MIND score significantly associated with a lower risk of cognitive impairment. | Energy intake, age, gender, presence of APOE ε4 allele, education, mental activity, physical activity, smoking status, depression, diabetes, BMI, hypertension, heart disease, and stroke. | [74] |
| Longitudinal | US | Older adults with clinical history of stroke n = 106 (29 M 77 F) Age: 82.8 ± 7.1 years | 5.9 years | 144-item FFQ, neuropsychologic battery of tests/global cognitive decline: episodic memory, semantic memory, working memory, perceptual orientation, perceptual speed | Determination of whether the MIND diet is effective in preventing cognitive decline after stroke | Higher tertile compared with lowest one of MIND diet scores had slower rate of global cognitive ↘ and slower ↘ in semantic memory and perceptual speed. In continuous models, MIND diet associated with slower ↘ in cognitive function for global cognition and semantic memory. | Age, gender, education, total energy intake, presence of APOE ε4 allele, smoking, participation in cognitive and physical activities, depressive symptoms, BMI, chronic diseases. | [116] |
| Longitudinal | US | Population WRAP study n = 828 (268 M 560 F) Age: 57.7 ± 6.4 years, free of dementia and MCI at baseline | 6.3 years | 15-item questionnaire, neuropsychological battery of tests/ multidomain cognitive composite: immediate memory, delayed memory, executive function | Effect of MIND diet on multidomain cognitive composite and immediate/delayed memory and executive function composites | Higher MIND diet scores associated with slower ↘ in executive function. MIND diet not associated with PACC4, immediate memory, or delayed memory. | Age, gender, presence of APOE ε4 allele, cognitive activity, physical activity, education. | [117] |
| Longitudinal | Germany | Older adults from DELCODE study n= 389 (187 M 202 F), free of dementia Age: 69.4 ± 5.6 years Subjective Cognitive Decline group (SCD): n = 146 MCI group: n = 60 First-degree relatives of AD dementia patients: n = 35 Healthy controls: n = 148 | NS | 148-item FFQ neuropsychological battery of tests and MMSE tool/cognitive function: memory, language (verbal fluency), executive functioning, working memory, visuospatial functioning | Associations between dietary patterns and cognitive functioning in older adults free of dementia | Higher MIND diet score associated with better memory in total subjects and language functions in cognitively normal subjects. MIND diet not associated with executive functioning, working memory, or visuospatial functioning. | Age, gender, education, BMI, physical activity, smoking, total daily energy intake, presence of APOE ε4 allele. | [126] |
| Longitudinal | US | Decedent participants from Rush Memory and Aging Project (MAP) n = 569 (70% F), age at death 91 years | NS | Dietary data, cognitive testing proximate to death, and complete autopsy data at the time of the analyses | Examination of whether the association of MIND diet with cognition is independent of common brain pathologies | Higher MIND diet score associated with better global cognitive functioning proximate to death, even after adjustment for AD and other brain pathologies. MIND diet–cognition relationship remained significant when analysis restricted to individuals without MCI at baseline or postmortem diagnosed with AD. | Age at death, gender, years of education, presence of APOE ε4 allele, cognitive activities, and total energy intake. | [121] |
| Cross-sectional | US | Community-dwelling adults n = 5907 (40% men) Age: 67.8 years | NS | 163-item SFFQ, A-MeDi score, MIND diet score | Cognitive performance: immediate and delayed recall, backward counting, and serial seven subtraction | Higher MIND diet scores associated with slower ↘ in executive function. MIND diet not associated with PACC4, immediate memory, or delayed memory. | Gender, age, race, low education attainment, current smoking, obesity, total wealth, hypertension, diabetes mellitus, physical inactivity, depression, and total energy intake. | [65] |
| Cross-sectional | Brazil | Senior participants with different cognition Control: n = 36 (7 M 29 F) Age ≥ 75 years 12% MCI: n = 30 (9 M 21 F) Age ≥ 75 years 50% AD: n = 30 (11 M 19 F) Age ≥ 75 years 63.3% | NS | 98-item FFQ, neuropsychiatric battery of tests and MMSE tool/ cognitive performance: naming, incidental memory, immediate memory, learning, delayed recall and recognition | Impact of MIND diet adherence on cognitive performance for different cognitive profiles seniors | Moderate adherence to MIND diet associated with higher MMSE scores. High adherence to MIND diet associated with learning score in healthy older adults but not in MCI or AD. No association between the other cognitive variables and the MIND score. | Age, education, income, marital status, BMI, chronic diseases, having undergone nutritional care, motor or sensory impairments. | [127] |
| Cross-sectional | China | Older adults from the Chinese Longitudinal Healthy Longevity Study n = 11,245 (45.3% M) Age: 84.06 ± 11.46 years | 2 to 3 years | 12-items FFQ, Chinese MIND (cMIND)diet score | Cognitive impairment and IADL disability | Moderate and high adherence to cMIND diet associated with lower likelihood of cognitive impairment (higher MMSE score) and IADL disability, even after adjusting for covariates. Higher cMIND diet score associated with better cognitive function and IADL. | Age, gender, residence, education, BMI, diabetes, hearing impairment, hypertension, depression, smoking, drinking, exercise, and social engagement. | [123] |
| Cross-sectional | US | Data from University of Michigan Health and Retirement Study n = 3463 Age: 68.0 ± 10.0 years | NS | 163-item FFQ, MIND diet scores, episodic memory (im- mediate and delayed recall), working memory, attention/processing speed | Association of combination of high-intensity physical activity (PA) and MIND diet with better cognition compared with PA or MIND diet alone or neither | MIND diet alone associated with better global cognition and lower likelihood of cognitive decline. Combining PA and MIND diet predicted better global cognition and lower likelihood of cognitive decline, but did not predict lower odds of cognitive decline compared to PA alone. | Age, gender, race, education, annual income, smoking history, hypertension, diabetes mellitus, depression, and obesity. | [125] |
| Randomized controlled trial | Iran | Healthy obese women (MMSE = 24) n = 37 MIND group: n = 22 Age 48.95 ± 1.07 years Control group: n = 15 Age 48.86 ± 1.56 years | 3 months | 168-item FFQ and 3-day food recall, neuropsychological test battery and MMSE tool/verbal short memory, working memory, attention and visual scanning, verbal recognition memory, executive function and task switching, ability to inhibit cognitive interference | Impact of 3 months MIND diet on body composition and cognition | MIND group compared with control had improved working memory, verbal recognition memory, and attention. ↗ in the surface area of inferior frontal gyrus in MIND diet group. | Pregnancy, metabolic complications, severe untreated medical, neurological, psychiatric diseases, or gastrointestinal problems. | [124] |
| Prospective cohort | Spain | Older adults from “Seguimiento Universidad de Navarra” n= 806 (562 M 244 F) without cognitive impairment at baseline Age: 61 ± 6 years | 6 ± 3 years | 136-item FFQ, telephone-based interview of MMSE/Spanish TICS (orientation, memory, attention/calculation, and language) | Compare association of dietary patterns with cognitive function | Higher adherence to MIND diet associated with upward 6-year changes in Spanish TICS scores. Each 1-point ↗ in the MIND score ↗ Spanish TICS score by 0.27 points. In adjusted linear mixed model, MIND diet score associated with 0.038 rate of change in STICS scores over 5.6 years. | Age, gender, presence of APOE ε4 allele, smoking, education, total energy intake, physical activity, BMI, alcohol intake, depression, chronic diseases, high cholesterol, low HDL cholesterol. | [128] |
| Prospective cohort | France | Older Adults in NutriNet-Santé n = 6011 (2384 M 3627 F) without SMC at enrollment | 6 years | FFQ, SMC measured with French version of the validated self-administered cognitive difficulties scale | Impact of MIND diet adherence on SMC | MIND diet score not significantly associated with SMC in adults aged 60–69 years. Adherence to MIND diet for >70 years without depressive symptoms associated with SMC. One-point increase in MIND diet score associated with 14% ↘ in SMC risk. | Age, gender, marital status, education, occupation, smoking, income, BMI, physical activity, depressive symptoms, chronic diseases, energy intake. | [121] |
| Prospective cohort | US | Older population of Framingham Heart Study n = 2092 (956 M 1036 F) Age: 61 ± 9 years | 6.6 ± 1.1 years | FFQ, neuropsychological testing, and brain MRI scans (n = 1904). | Association between the MIND diet and measures of brain volume, silent brain infarcts (SBIs), or brain atrophy in the community-based Framingham Heart Study | Higher MIND diet scores associated with better global cognitive function, verbal memory, visual memory, processing speed, and verbal comprehension/reasoning and with larger total brain volume following adjustments. Higher MIND diet scores not associated with other brain MRI measures or cognitive decline. | Age, gender, presence of APOE ε4 allele, total energy intake, education, the time interval between completion of the FFQ and the measurement of the neuropsychological and MRI outcomes, BMI, physical activity, smoking status, cardiometabolic factors, and high level of depressive symptoms. | [117] |
| Cross-sectional and longitudinal | US | Adults from Boston Puerto Rican Health Study n= 1502 (378 M 1124 F) Age: 45–75 years at baseline | 8 years | FFQ over 5-year follow-ups, neuropsychological tests, MMSE | Association between long-term adherence to MIND diet and cognitive function in Puerto Rican adults | In cross-sectional and longitudinal analyses, the highest compared to lowest MIND quintile associated with better cognition function, but not with cognitive trajectory over 8 years. | Income-to-poverty ratio, education level, and job complexity score. | [118] |
| Longitudinal study and meta-analysis | China | Participants from the China Health and Nutrition Survey (CHNS) n = 4066 participants Meta-analysis: results from the longitudinal study and 7 other MIND diet and cognitive effect studies n = 26,103 | 3-day 24 h dietary recall, battery of cognitive tests, immediate and delayed recall memory, attention, and calculation abilities | Median 3 years | Relationship between MIND diet and cognitive function and its decline among middle-aged and older adults | Higher MIND diet scores were significantly associated with better global cognitive function. Each increment of 3 points in MIND diet score has adjusted difference in global cognitive function z-score approximately equivalent to being one year younger in age. In the meta-analysis of 26,103 participants, 1 standardized deviation MIND score increment associated with 0.042-unit higher global cognitive function z-score and 0.014-unit slower annual cognitive decline. | Age, gender, education, annual household income per capita, residence, region, smoking, alcohol drinking, BMI, total energy intake, physical activity, history of chronic diseases included self-reported hypertension, diabetes, and myocardial infarction diagnosis, and use of antihypertensive and anti-diabetic medications. | [119] |
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Randomized, double-blind, crossover single-center pilot study | US | n = 17 Age: 64.6 ± 6.4 years Participants with MCI n = 11 Participants with normal cognitive function n = 6 | 6-week interventions: MMKD and AHA diet separated by 6-week washout | Gut microbiome, fecal short-chain fatty acids, markers of AD in cerebrospinal fluid | Change in gut microbial signature, fecal short-chain fatty acids, and AD biomarkers after each diet intervention. | MMKD associated with improved metabolic indices and AD biomarkers in CSF profile. | NS | [136] |
| Randomized crossover trial | US | Participants with MCI n= 9 (3 M 6 F) Age: 63.4 ± 4.0 years Participants with SMC n= 11 (2 M 9 F) Age: 64.9 ± 7.9 years | MMKD diet and AHA diet for 6 weeks followed by 6-week washout | Immediate and delayed memory, general cognition, plasma biomarkers, CSF biomarkers, and MRI | Compare effects of MMKD and AHA diet on AD biomarkers in CSF, neuroimaging measures, peripheral metabolism, and cognition. | MMKD associated with ↗ CSF Ab42 and ↘ t-tau. | Age, presence of APOE ε4 allele, and order of diet intervention. | [135] |
| Randomized controlled trial | New Zealand | Participants with diagnosed AD n= 26 (16 M 10 F) Age: 69.8 ± 6.0 years | 12-week intervention and 10-week washout, low-fat diet and MMKD | FFQ, cognition by ACE-III, daily function by ADCS-ADL, quality of life by QOL-AD | Change in cognition, daily function, or quality of life in AD patients after 12 weeks of MMKD. | Improvement in cognitive function, everyday functioning, and quality of life for MMKD group participants compared with the low-fat diet ones. | NS | [137] |
| Crossover trial | US | Participants with MCI n = 9 (3 M 6 F) Age: 63.4 ± 4.0 Participants with SMC n = 11 (2 M 9 F) Age: 64.9 ± 7.89 years | MMKD and AHA diet for 6 weeks with a 6-week washout period | Dual-energy X-ray absorptiometry for adiposity and CSF biomarkers | Effects of MMKD compared to AHA diet on body weight, body composition, and body fat distribution and their association with AD biomarkers in CSF. | ↘ in body fat on the MMKD related to changes in Aβ biomarkers. | Age and diet order | [134] |
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| NS | US and Canada | Vegetarian, n= 72 (32 M 40 F) (62 white, 10 non-white) Age: 76.6 ± 8.3 years Non-vegetarian, n = 60 (24 M 36 F) (44 white, 16 non-white) Age: 73.5 ± 7.7 years | 10 years | FFQ, historic dietary habits survey instrument | Verbal learning, memory, attention, processing speed, executive function, visuospatial abilities, language, global cognitive functioning, MMSE, AMNART, and GDS | Vegetarian diet not associated with lower mild memory impairment likelihood. More stable diet associated with better memory/language. | Age, education | [143] |
| Prospective cohort study | Taiwan | Buddhist Tzu Chi Foundation volunteers Non-vegetarian, n = 3154 (1345 M 1809 F) Age: 57.8 ± 6.3 years Vegetarian, n = 1737 (461 M 1276 F) Age: 58.1 ± 6.5 years | Average 9.2 years | Baseline questionnaires to assess dietary pattern, overall plant-based diet index | MCI and dementia diagnosis | Vegetarians associated with less risk of dementia compared with non-vegetarians after adjusting for covariates. | Gender, age, smoking, drinking, education level, marital status, regular exercise, comorbidities | [144] |
| Longitudinal | US | n = 3337 (1200 M 2137 F) Age: 73.7 ± 5.72 years African American (AA), n = 2012; white, n = 1325 | NS | FFQ | Episodic memory, perceptual speed, and MMSE | ↗ plant-based diet associated with slower ↘ in GC, PS, and EM in AA but not in white participants. AA in the highest quintile of high plant-based diet had significantly slower rates of GC, PS, and EM than individuals in the lowest quintile. | Age, gender, presence of apolipoprotein E4 (APOE ε4) allele, lifestyle factors (education, cognitive activities, smoking, calorie intake, risk factors for cardiovascular disease, time and interaction time × each covariate) | [141] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ellouze, I.; Sheffler, J.; Nagpal, R.; Arjmandi, B. Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience. Nutrients 2023, 15, 3204. https://doi.org/10.3390/nu15143204
Ellouze I, Sheffler J, Nagpal R, Arjmandi B. Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience. Nutrients. 2023; 15(14):3204. https://doi.org/10.3390/nu15143204
Chicago/Turabian StyleEllouze, Ines, Julia Sheffler, Ravinder Nagpal, and Bahram Arjmandi. 2023. "Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience" Nutrients 15, no. 14: 3204. https://doi.org/10.3390/nu15143204
APA StyleEllouze, I., Sheffler, J., Nagpal, R., & Arjmandi, B. (2023). Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience. Nutrients, 15(14), 3204. https://doi.org/10.3390/nu15143204