

Vitamin D Deficiency Is Associated with Impaired Sensitivity to Thyroid Hormones in Euthyroid Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Populations
2.2. Clinical Variable Measurements
2.3. Calculations and Definitions
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Population
3.2. 25(OH)D Levels Were Significantly Correlated with Thyroid Hormone Sensitivity Indices
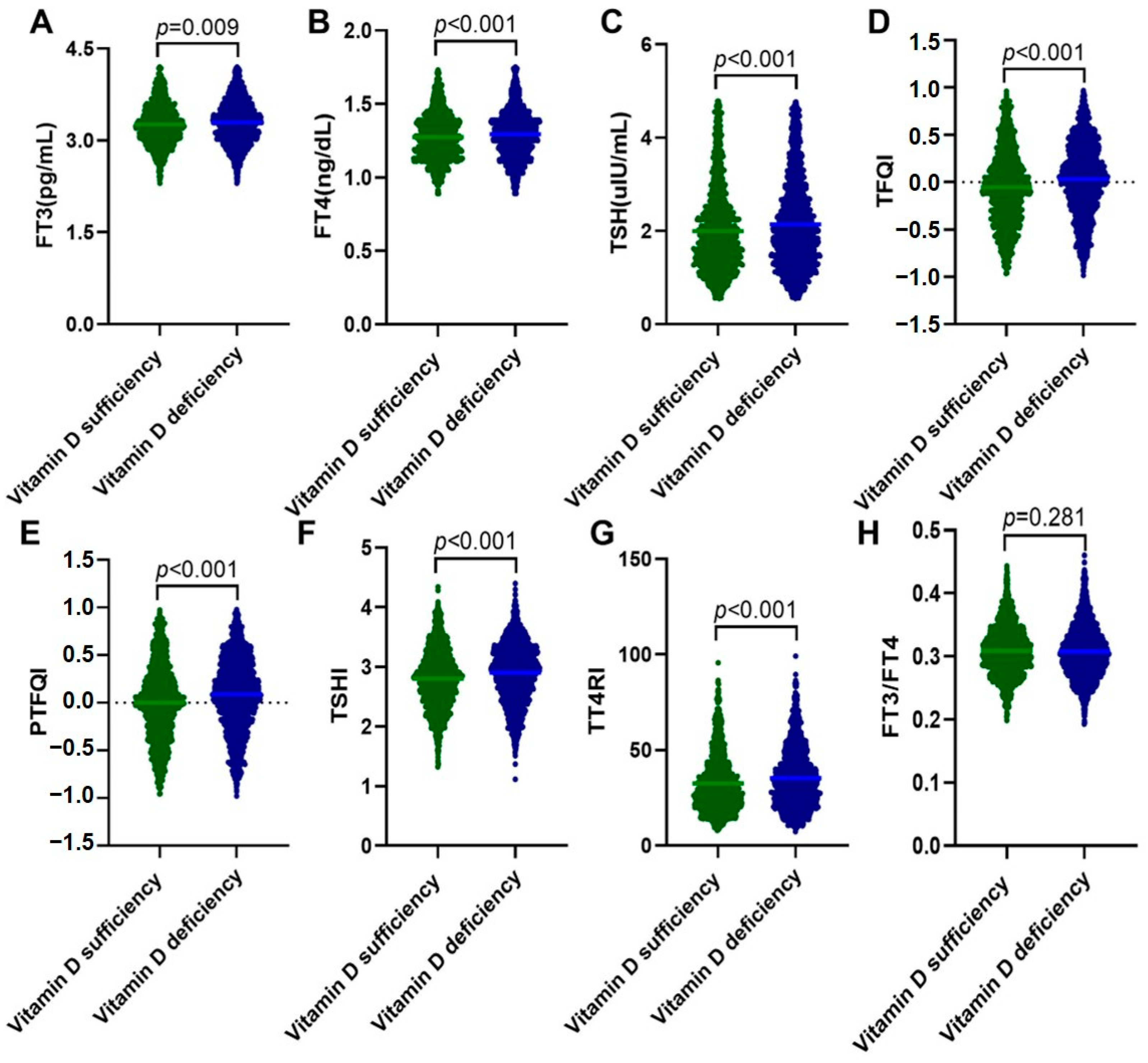
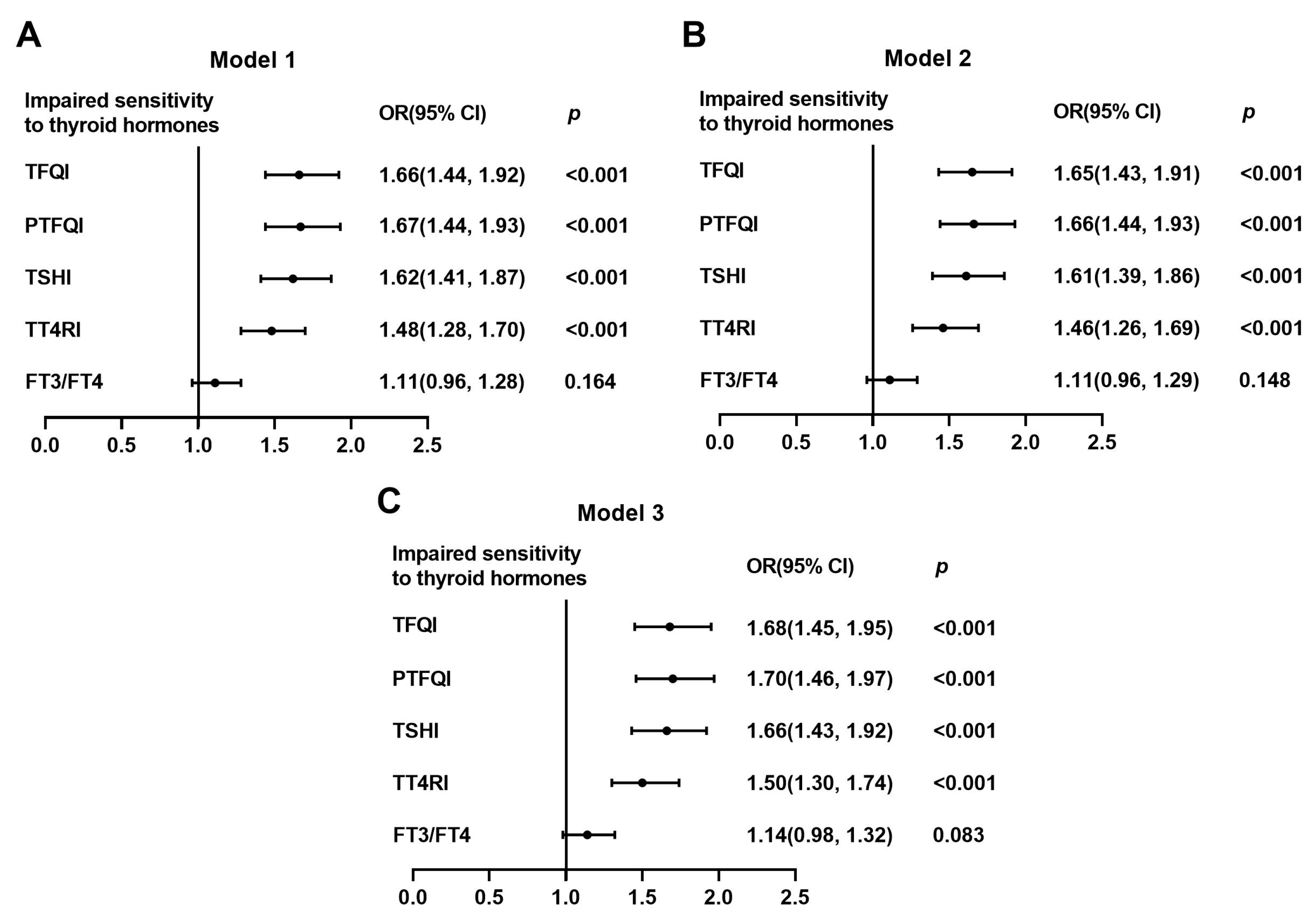
3.3. Vitamin D Deficiency Was Associated with Markedly Increased Risks of Impaired Sensitivity to Thyroid Hormones
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Guasch, A.; Bulló, M.; Rabassa, A.; Bonada, A.; Del Castillo, D.; Sabench, F.; Salas-Salvadó, J. Plasma vitamin D and parathormone are associated with obesity and atherogenic dyslipidemia: A cross-sectional study. Cardiovasc. Diabetol. 2012, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- Vieira, I.H.; Rodrigues, D.; Paiva, I. Vitamin D and Autoimmune Thyroid Disease-Cause, Consequence, or a Vicious Cycle? Nutrients 2020, 12, 2791. [Google Scholar] [CrossRef]
- Siddiqui, M.; Manansala, J.S.; Abdulrahman, H.A.; Nasrallah, G.K.; Smatti, M.K.; Younes, N.; Althani, A.A.; Yassine, H.M. Immune Modulatory Effects of Vitamin D on Viral Infections. Nutrients 2020, 12, 2879. [Google Scholar] [CrossRef]
- Mangin, M.; Sinha, R.; Fincher, K. Inflammation and vitamin D: The infection connection. Inflamm. Res. 2014, 63, 803–819. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lv, S.; Chen, G.; Gao, C.; He, J.; Zhong, H.; Xu, Y. Meta-analysis of the association between vitamin D and autoimmune thyroid disease. Nutrients 2015, 7, 2485–2498. [Google Scholar] [CrossRef]
- Grammatiki, M.; Rapti, E.; Karras, S.; Ajjan, R.A.; Kotsa, K. Vitamin D and diabetes mellitus: Causal or casual association? Rev Endocr. Metab. Disord. 2017, 18, 227–241. [Google Scholar] [CrossRef]
- Al Refaie, A.; Baldassini, L.; De Vita, M.; Gonnelli, S.; Caffarelli, C. Vitamin D and adrenal gland: Myth or reality? A systematic review. Front. Endocrinol. 2022, 13, 1001065. [Google Scholar] [CrossRef]
- He, C.; Lin, Z.; Robb, S.W.; Ezeamama, A.E. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 4555–4577. [Google Scholar] [CrossRef]
- Zhao, R.; Zhang, W.; Ma, C.; Zhao, Y.; Xiong, R.; Wang, H.; Chen, W.; Zheng, S.G. Immunomodulatory Function of Vitamin D and Its Role in Autoimmune Thyroid Disease. Front. Immunol. 2021, 12, 574967. [Google Scholar] [CrossRef] [PubMed]
- Verrusio, W.; Magro, V.M.; Renzi, A.; Casciaro, B.; Andreozzi, P.; Cacciafesta, M. Thyroid hormones, metabolic syndrome and Vitamin D in middle-aged and older euthyroid subjects: A preliminary study. Aging Clin. Exp. Res. 2019, 31, 1337–1341. [Google Scholar] [CrossRef] [PubMed]
- Mansorian, B.; Mirza-Aghazadeh Attari, M.; Vahabzadeh, D.; Mohebbi, I. Serum vitamin D level and its relation to thyroid hormone, blood sugar and lipid profiles in Iranian sedentary work staff. Nutr. Hosp. 2018, 35, 1107–1114. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, Z.; Sun, M.; Cao, M.; Zhu, Z.; Fu, Q.; Gao, Y.; Mao, J.; Li, Y.; Shi, Y.; et al. Association of high vitamin d status with low circulating thyroid-stimulating hormone independent of thyroid hormone levels in middle-aged and elderly males. Int. J. Endocrinol. 2014, 2014, 631819. [Google Scholar] [CrossRef]
- Babić Leko, M.; Jureško, I.; Rozić, I.; Pleić, N.; Gunjača, I.; Zemunik, T. Vitamin D and the Thyroid: A Critical Review of the Current Evidence. Int. J. Mol. Sci. 2023, 24, 3586. [Google Scholar] [CrossRef] [PubMed]
- Laclaustra, M.; Moreno-Franco, B.; Lou-Bonafonte, J.M.; Mateo-Gallego, R.; Casasnovas, J.A.; Guallar-Castillon, P.; Cenarro, A.; Civeira, F. Impaired Sensitivity to Thyroid Hormones Is Associated with Diabetes and Metabolic Syndrome. Diabetes Care 2019, 42, 303–310. [Google Scholar] [CrossRef]
- Ding, X.; Wang, Y.; Liu, J.; Wang, G. Impaired Sensitivity to Thyroid Hormones Is Associated with Elevated Homocysteine Levels in the Euthyroid Population. J. Clin. Endocrinol. Metab. 2022, 107, e3731–e3737. [Google Scholar] [CrossRef]
- Sun, Y.; Teng, D.; Zhao, L.; Shi, X.; Li, Y.; Shan, Z.; Teng, W. Impaired Sensitivity to Thyroid Hormones Is Associated with Hyperuricemia, Obesity, and Cardiovascular Disease Risk in Subjects with Subclinical Hypothyroidism. Thyroid Off. J. Am. Thyroid. Assoc. 2022, 32, 376–384. [Google Scholar] [CrossRef]
- Lv, F.; Cai, X.; Li, Y.; Zhang, X.; Zhou, X.; Han, X.; Ji, L. Sensitivity to thyroid hormone and risk of components of metabolic syndrome in a Chinese euthyroid population. J. Diabetes 2023. [Google Scholar] [CrossRef]
- Wan, H.; Yu, G.; Xu, S.; Chen, X.; Jiang, Y.; Duan, H.; Lin, X.; Ma, Q.; Wang, D.; Liang, Y.; et al. Central sensitivity to free triiodothyronine with MAFLD and its progression to liver fibrosis in euthyroid adults. J. Clin. Endocrinol. Metab. 2023, 108, e687–e697. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Daly, R.M.; Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Sikaris, K.A.; Zimmet, P.Z.; Ebeling, P.R.; Shaw, J.E. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: A national, population-based study. Clin. Endocrinol. 2012, 77, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef] [PubMed]
- Song, H.R.; Kweon, S.S.; Choi, J.S.; Rhee, J.A.; Lee, Y.H.; Nam, H.S.; Jeong, S.K.; Park, K.S.; Ryu, S.Y.; Choi, S.W.; et al. High prevalence of vitamin D deficiency in adults aged 50 years and older in Gwangju, Korea: The Dong-gu Study. J. Korean Med. Sci. 2014, 29, 149–152. [Google Scholar] [CrossRef]
- Liu, L.; Cao, Z.; Lu, F.; Liu, Y.; Lv, Y.; Qu, Y.; Gu, H.; Li, C.; Cai, J.; Ji, S.; et al. Vitamin D deficiency and metabolic syndrome in elderly Chinese individuals: Evidence from CLHLS. Nutr. Metab. 2020, 17, 58. [Google Scholar] [CrossRef]
- Jiang, W.; Wu, D.B.; Xiao, G.B.; Ding, B.; Chen, E.Q. An epidemiology survey of vitamin D deficiency and its influencing factors. Med. Clin. 2020, 154, 7–12. [Google Scholar] [CrossRef]
- Ren, Z.; Zhao, A.; Wang, Y.; Meng, L.; Man-Yau Szeto, I.; Yang, C.; Wang, M.; Zhang, J.; Wu, W.; Wang, P.; et al. Association of serum 25-hydroxy vitamin D with obesity-related indices in Chinese adults: A cross-sectional study. Food Sci. Nutr. 2021, 9, 2260–2268. [Google Scholar] [CrossRef]
- Zhen, D.; Liu, L.; Guan, C.; Zhao, N.; Tang, X. High prevalence of vitamin D deficiency among middle-aged and elderly individuals in northwestern China: Its relationship to osteoporosis and lifestyle factors. Bone 2015, 71, 1–6. [Google Scholar] [CrossRef]
- Gannagé-Yared, M.H.; Chedid, R.; Khalife, S.; Azzi, E.; Zoghbi, F.; Halaby, G. Vitamin D in relation to metabolic risk factors, insulin sensitivity and adiponectin in a young Middle-Eastern population. Eur. J. Endocrinol. 2009, 160, 965–971. [Google Scholar] [CrossRef]
- Chiu, K.C.; Chu, A.; Go, V.L.; Saad, M.F. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am. J. Clin. Nutr. 2004, 79, 820–825. [Google Scholar] [CrossRef]
- Carbone, L.D.; Rosenberg, E.W.; Tolley, E.A.; Holick, M.F.; Hughes, T.A.; Watsky, M.A.; Barrow, K.D.; Chen, T.C.; Wilkin, N.K.; Bhattacharya, S.K.; et al. 25-Hydroxyvitamin D, cholesterol, and ultraviolet irradiation. Metab. Clin. Exp. 2008, 57, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Yu, Z.; Pan, A.; Hu, F.B.; Franco, O.H.; Li, H.; Li, X.; Yang, X.; Chen, Y.; Lin, X. Plasma 25-hydroxyvitamin D concentration and metabolic syndrome among middle-aged and elderly Chinese individuals. Diabetes Care 2009, 32, 1278–1283. [Google Scholar] [CrossRef]
- Barchetta, I.; Baroni, M.G.; Leonetti, F.; De Bernardinis, M.; Bertoccini, L.; Fontana, M.; Mazzei, E.; Fraioli, A.; Cavallo, M.G. TSH levels are associated with vitamin D status and seasonality in an adult population of euthyroid adults. Clin. Exp. Med. 2015, 15, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Mackawy, A.M.; Al-Ayed, B.M.; Al-Rashidi, B.M. Vitamin d deficiency and its association with thyroid disease. Int. J. Health Sci. 2013, 7, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Cai, J.; Markowitz, M. Absence of a relationship between thyroid hormones and vitamin D levels. J. Pediatr. Endocrinol. Metab. JPEM 2016, 29, 703–707. [Google Scholar] [CrossRef]
- Guo, Y.; Wu, C.Y.; Deng, Y.H.; Wu, J.L. Associations Between Serum 25-Hydroxyvitamin D Levels and Thyroid Function Parameters in Previously Healthy Children Aged 6 to 24 Months. Risk Manag. Healthc. Policy 2020, 13, 1647–1653. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Brunel, L.; Muscogiuri, G.; Kimball, S. Physiological serum 25-hydroxyvitamin D concentrations are associated with improved thyroid function-observations from a community-based program. Endocrine 2017, 58, 563–573. [Google Scholar] [CrossRef]
- Ortiga-Carvalho, T.M.; Sidhaye, A.R.; Wondisford, F.E. Thyroid hormone receptors and resistance to thyroid hormone disorders. Nat. Rev. Endocrinol. 2014, 10, 582–591. [Google Scholar] [CrossRef]
- Tjørve, E.; Tjørve, K.M.; Olsen, J.O.; Senum, R.; Oftebro, H. On commonness and rarity of thyroid hormone resistance: A discussion based on mechanisms of reduced sensitivity in peripheral tissues. Med. Hypotheses 2007, 69, 913–921. [Google Scholar] [CrossRef]
- Nie, X.; Ma, X.; Xu, Y.; Shen, Y.; Wang, Y.; Bao, Y. Increased Serum Adipocyte Fatty Acid-Binding Protein Levels Are Associated with Decreased Sensitivity to Thyroid Hormones in the Euthyroid Population. Thyroid Off. J. Am. Thyroid Assoc. 2020, 30, 1718–1723. [Google Scholar] [CrossRef]
- Mehran, L.; Delbari, N.; Amouzegar, A.; Hasheminia, M.; Tohidi, M.; Azizi, F. Reduced Sensitivity to Thyroid Hormone Is Associated with Diabetes and Hypertension. J. Clin. Endocrinol. Metab. 2022, 107, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Zhu, W.; Liu, J.; An, Y.; Wang, Y.; Wang, G. Reduced Sensitivity to Thyroid Hormones Is Associated with High Remnant Cholesterol Levels in Chinese Euthyroid Adults. J. Clin. Endocrinol. Metab. 2022, 108, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Mammen, J.S.R.; Cappola, A.R. Autoimmune Thyroid Disease in Women. JAMA 2021, 325, 2392–2393. [Google Scholar] [CrossRef] [PubMed]
- Turashvili, N.; Javashvili, L.; Giorgadze, E. Vitamin D Deficiency Is More Common in Women with Autoimmune Thyroiditis: A Retrospective Study. Int. J. Endocrinol. 2021, 2021, 4465563. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Tirabassi, G.; Bizzaro, G.; Orio, F.; Paschou, S.A.; Vryonidou, A.; Balercia, G.; Shoenfeld, Y.; Colao, A. Vitamin D and thyroid disease: To D or not to D? Eur. J. Clin. Nutr. 2015, 69, 291–296. [Google Scholar] [CrossRef]
- D’Emden, M.C.; Wark, J.D. 1,25-Dihydroxyvitamin D3 enhances thyrotropin releasing hormone induced thyrotropin secretion in normal pituitary cells. Endocrinology 1987, 121, 1192–1194. [Google Scholar] [CrossRef]
- Alrefaie, Z.; Awad, H. Effect of vitamin D3 on thyroid function and de-iodinase 2 expression in diabetic rats. Arch. Physiol. Biochem. 2015, 121, 206–209. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Population | Vitamin D Sufficiency (≥20 ng/mL) | Vitamin D Deficiency (<20 ng/mL) | p |
|---|---|---|---|---|
| N | 3143 | 1294 | 1849 | NA |
| Age (years) | 47.0 ± 11.9 | 47.5 ± 11.8 | 46.8 ± 12.0 | 0.105 |
| Sex, men, n (%) | 2012 (64.0%) | 836 (64.6%) | 1176 (63.6%) | 0.571 |
| BMI (kg/m2) | 25.02 ± 3.57 | 24.92 ± 3.46 | 25.10 ± 3.65 | 0.123 |
| SBP (mmHg) | 125.36 ± 17.59 | 124.64 ± 17.86 | 125.86 ± 17.38 | 0.057 |
| DBP (mmHg) | 74.54 ± 11.71 | 74.26 ± 11.86 | 74.74 ± 11.60 | 0.264 |
| ALT (U/L) * | 21.0 (16.0–31.0) | 21.0 (16.0–30.0) | 21.0 (16.0–31.0) | 0.876 |
| AST (U/L) * | 22.0 (19.0–26.0) | 22.0 (19.0–26.0) | 22.0 (19.0–26.0) | 0.151 |
| Urea (mmol/L) | 5.32 ± 1.27 | 5.37 ± 1.26 | 5.28 ± 1.27 | 0.053 |
| Cr (umol/L) | 67.19 ± 13.33 | 68.26 ± 13.49 | 66.44 ± 13.16 | <0.001 |
| UA (umol/L) | 361.82 ± 89.64 | 366.72 ± 87.58 | 358.39 ± 90.92 | 0.010 |
| Ca (mmol/L) | 2.39 ± 0.09 | 2.40 ± 0.09 | 2.39 ± 0.09 | 0.011 |
| P (mmol/L) | 1.15 ± 0.22 | 1.15 ± 0.16 | 1.15 ± 0.25 | 0.560 |
| 25(OH)D (ng/mL) | 19.30 ± 7.39 | 26.18 ± 6.00 | 14.50 ± 3.56 | <0.001 |
| TC (mmol/L) | 5.08 ± 0.96 | 5.05 ± 0.94 | 5.10 ± 0.96 | 0.119 |
| TG (mmol/L) * | 1.38 (0.97–2.01) | 1.33 (0.96–1.89) | 1.42 (0.99–2.10) | <0.001 |
| HDL-C (mmol/L) | 1.29 ± 0.34 | 1.31 ± 0.34 | 1.28 ± 0.33 | 0.014 |
| LDL-C (mmol/L) | 3.10 ± 0.86 | 3.07 ± 0.85 | 3.12 ± 0.87 | 0.123 |
| Non-HDL-C (mmol/L) | 3.79 ± 0.92 | 3.74 ± 0.91 | 3.83 ± 0.93 | 0.012 |
| RC (mmol/L) * | 0.60 (0.39–0.86) | 0.60 (0.38–0.86) | 0.61 (0.39–0.86) | 0.729 |
| AIP | 0.063 ± 0.306 | 0.037 ± 0.295 | 0.081 ± 0.313 | <0.001 |
| Lp(a) (mmol/L) * | 12.50 (7.20–24.40) | 12.60 (7.30–24.03) | 12.40 (7.10–24.60) | 0.889 |
| Glucose (mmol/L) * | 4.94 (4.59–5.38) | 4.94 (4.59–5.38) | 4.94 (4.59–5.38) | 0.964 |
| HbA1c (%) * | 5.5 (5.3–5.8) | 5.5 (5.3–5.6) | 5.5 (5.3–5.8) | 0.349 |
| Insulin (mIU/L) * | 8.1 (5.7–11.5) | 7.7 (5.6–11.2) | 8.4 (5.8–11.7) | 0.007 |
| HOMA-IR * | 1.80 (1.22–2.73) | 1.74 (1.19–2.63) | 1.86 (1.24–2.80) | 0.018 |
| HOMA-β * | 113.51 (74.56–171.12) | 109.31 (72.30–164.09) | 116.33 (75.50–175.51) | 0.028 |
| HOMA-ISI * | 0.025 (0.017–0.036) | 0.026 (0.017–0.037) | 0.024 (0.016–0.036) | 0.018 |
| TyG (mg/dL)2 | 8.68 ± 0.63 | 8.63 ± 0.60 | 8.71 ± 0.65 | <0.001 |
| FT3 (pg/mL) | 3.28 ± 0.35 | 3.26 ± 0.34 | 3.29 ± 0.35 | 0.009 |
| FT4 (ng/dL) | 1.29 ± 0.15 | 1.27 ± 0.15 | 1.29 ± 0.16 | <0.001 |
| TSH (uIU/mL) | 2.08 ± 0.93 | 2.00 ± 0.90 | 2.14 ± 0.94 | <0.001 |
| Anti-TG positivity, n (%) | 294 (9.4%) | 109 (8.4%) | 185 (10.0%) | 0.136 |
| Anti-TPO positivity, n (%) | 284 (9.0%) | 111 (8.6%) | 173 (9.4%) | 0.487 |
| TFQI | −0.002 ± 0.382 | −0.053 ± 0.388 | 0.033 ± 0.375 | <0.001 |
| PTFQI | 0.053 ± 0.386 | 0.002 ± 0.391 | 0.088 ± 0.378 | <0.001 |
| TSHI | 2.86 ± 0.49 | 2.80 ± 0.49 | 2.90 ± 0.49 | <0.001 |
| TT4RI | 34.19 ± 15.12 | 32.58 ± 14.80 | 35.31 ± 15.23 | <0.001 |
| FT3/FT4 | 0.308 ± 0.040 | 0.309 ± 0.039 | 0.308 ± 0.041 | 0.281 |
| Variables | Unadjusted | Adjusted 1 | Adjusted 2 | |||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| FT3 (pg/mL) | −0.041 | 0.022 | −0.040 | 0.027 | −0.036 | 0.042 |
| FT4 (ng/dL) | −0.049 | 0.006 | −0.038 | 0.032 | −0.041 | 0.023 |
| TSH (uIU/mL) | −0.090 | <0.001 | −0.077 | <0.001 | −0.083 | <0.001 |
| TFQI | −0.107 | <0.001 | −0.086 | <0.001 | −0.094 | <0.001 |
| PTFQI | −0.106 | <0.001 | −0.086 | <0.001 | −0.093 | <0.001 |
| TSHI | −0.109 | <0.001 | −0.089 | <0.001 | −0.096 | <0.001 |
| TT4RI | −0.103 | <0.001 | −0.085 | <0.001 | −0.092 | <0.001 |
| FT3/FT4 | 0.012 | 0.516 | 0.005 | 0.784 | 0.009 | 0.595 |
| Impaired Sensitivity to Thyroid Hormones | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| TFQI | 1.66 (1.44, 1.92) | <0.001 | 1.65 (1.43, 1,91) | <0.001 | 1.68 (1.45, 1.95) | <0.001 |
| PTFQI | 1.67 (1.44, 1.93) | <0.001 | 1.66 (1.44, 1.93) | <0.001 | 1.70 (1.46, 1.97) | <0.001 |
| TSHI | 1.62 (1.41, 1.87) | <0.001 | 1.61 (1.39, 1.86) | <0.001 | 1.66 (1.43, 1.92) | <0.001 |
| TT4RI | 1.48 (1.28, 1.70) | <0.001 | 1.46 (1.26, 1.69) | <0.001 | 1.50 (1.30, 1.74) | <0.001 |
| FT3/FT4 | 1.11 (0.96, 1.28) | 0.164 | 1.11 (0.96, 1.29) | 0.148 | 1.14 (0.98, 1.32) | 0.083 |
| Impaired Sensitivity to Thyroid Hormone | Men (N = 2012) | Women (N = 1131) | p for Interaction | ||
|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | ||
| TFQI | 1.25 (1.04, 1.50) | 0.020 | 2.84 (2.19, 3.67) | <0.001 | <0.001 |
| PTFQI | 1.25 (1.04, 1.51) | 0.016 | 2.92 (2.25, 3.78) | <0.001 | <0.001 |
| TSHI | 1.24 (1.04, 1.49) | 0.020 | 2.86 (2.21, 3.70) | <0.001 | <0.001 |
| TT4RI | 1.18 (0.98, 1.41) | 0.083 | 2.40 (1.86, 3.10) | <0.001 | <0.001 |
| FT3/FT4 | 1.03 (0.86, 1.24) | 0.765 | 1.43 (1.11, 1.83) | 0.006 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, L.; Wang, Y.; Su, J.; An, Y.; Liu, J.; Wang, G. Vitamin D Deficiency Is Associated with Impaired Sensitivity to Thyroid Hormones in Euthyroid Adults. Nutrients 2023, 15, 3697. https://doi.org/10.3390/nu15173697
Zhou L, Wang Y, Su J, An Y, Liu J, Wang G. Vitamin D Deficiency Is Associated with Impaired Sensitivity to Thyroid Hormones in Euthyroid Adults. Nutrients. 2023; 15(17):3697. https://doi.org/10.3390/nu15173697
Chicago/Turabian StyleZhou, Liyuan, Ying Wang, Jingru Su, Yu An, Jia Liu, and Guang Wang. 2023. "Vitamin D Deficiency Is Associated with Impaired Sensitivity to Thyroid Hormones in Euthyroid Adults" Nutrients 15, no. 17: 3697. https://doi.org/10.3390/nu15173697
APA StyleZhou, L., Wang, Y., Su, J., An, Y., Liu, J., & Wang, G. (2023). Vitamin D Deficiency Is Associated with Impaired Sensitivity to Thyroid Hormones in Euthyroid Adults. Nutrients, 15(17), 3697. https://doi.org/10.3390/nu15173697