
Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment




Abstract
:
1. Introduction
2. Materials and Methods
2.1. Micronutrients’ Health Claims Approved in the European Union (EU)
2.2. Spanish Market Research and Sample Selection
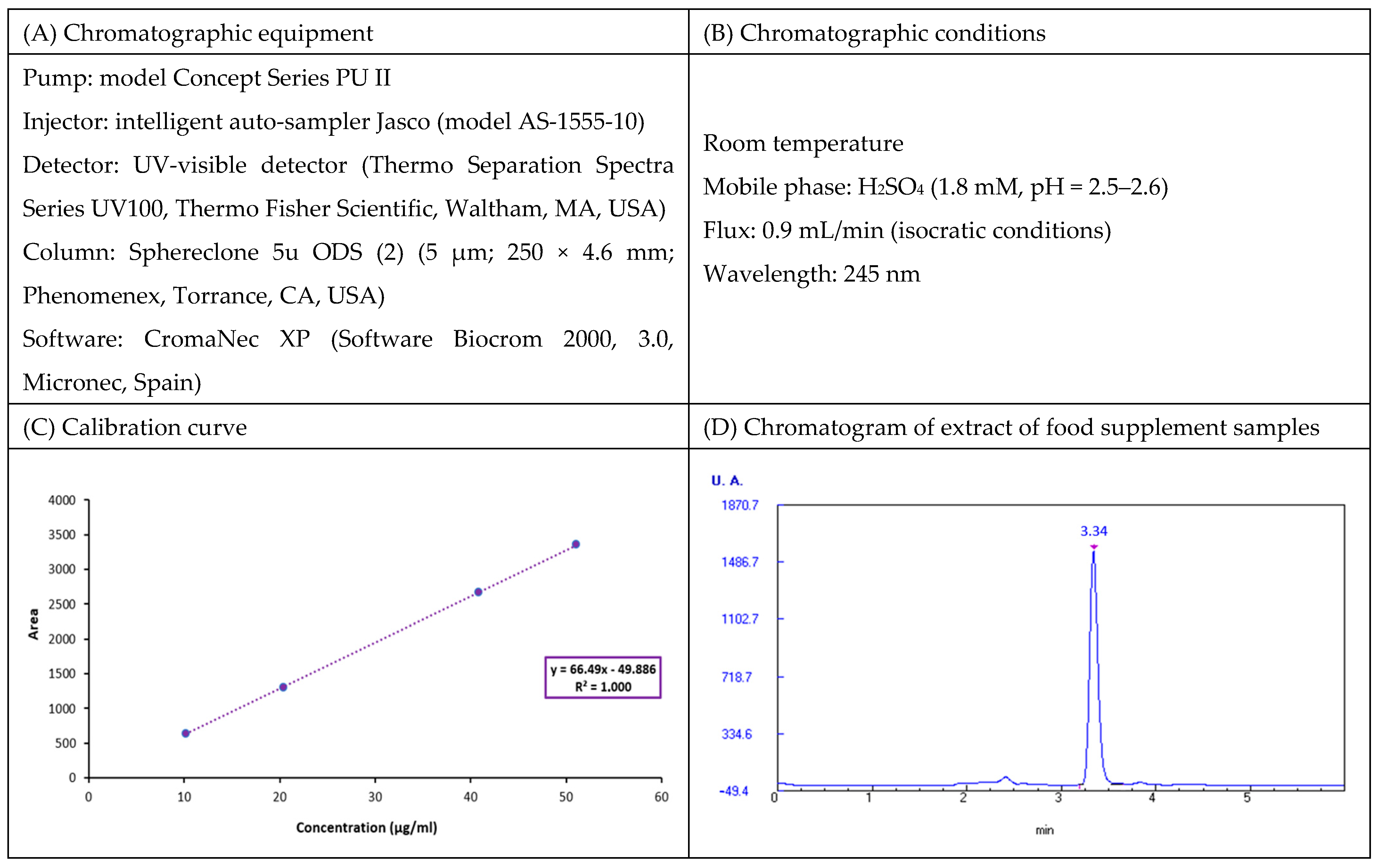
2.3. Chemical Analysis of Micronutrient Contents in Samples
2.3.1. Vitamin C: L-Ascorbic Acid
2.3.2. Vitamin B9 (Folic Acid)
2.3.3. Micro- and Macrominerals
2.3.4. Statistical Analysis
3. Results and Discussion
3.1. Health Claims Approved in the EU for Analyzed Micronutrients
3.2. Spanish Market Search and Samples Selection
3.3. Micronutrients Content and Assessment of the Application of Health Claims in Selected Samples
3.3.1. Vitamin C
3.3.2. Vitamin B9 (Folic Acid)
3.3.3. Micro- and Macro-Elements
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Food Safety Authority (EFSA). Food Supplements—Introduction. Available online: https://www.efsa.europa.eu/en/topics/topic/food-supplements (accessed on 26 June 2023).
- European Commission. Food Supplements. Available online: https://ec.europa.eu/food/safety/labelling_nutrition/supplements_en (accessed on 20 June 2023).
- European Parliament and Council of the European Union. Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the approximation of the laws of the Member States relating to food supplements. Off. J. Eur. Union 2002, L183, 51. Available online: http://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:32002L0046 (accessed on 21 June 2023).
- Cámara, M.; Fernández-Ruiz, V.; Domínguez, L.; Cámara, R.M.; Sánchez-Mata, M.C. Global Concepts and Regulations in Functional Foods. In Functional Foods, Series of Bioprocessing in Food Science; Chhikara, N., Panghal, A., Chaudhary, G., Eds.; Wiley, Scrivener Publishing LLC: Beverly, MA, USA, 2022; pp. 511–554. [Google Scholar]
- Domínguez, L.; Fernández-Ruiz, V.; Cámara, M. The frontier between nutrition and pharma: The international regulatory framework of functional foods, food supplements and nutraceuticals. Crit. Rev. Food Sci. Nutr. 2019, 60, 1738–1746. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, L.; Fernández-Ruiz, V.; Morales, P.; Sánchez-Mata, M.C.; Cámara, M. Assessment of Health Claims Related to Folic Acid in Food Supplements for Pregnant Women According to the European Regulation. Nutrients 2021, 13, 937. [Google Scholar] [CrossRef]
- Ipsos. Europeans’ Attitudes towards Food Supplements. Available online: https://www.ipsos.com/en/nutrition-pill-europeans-attitudes-towards-food-supplements (accessed on 25 June 2023).
- Baladia, E.; Moñino, M.; Martínez-Rodríguez, R.; Miserachs, M.; Picazo, O.; Fernández, T.; Morte, V.; Russolillo, G. Uso de Suplementos Nutricionales en la Población Española. Uso de Complementos Alimenticios, Alimentos para Grupos Específicos (Usos Médicos Especiales y Deportivos) y Productos a Base de Extractos de Plantas en Población Española: Un Estudio Transversal; Fundación MAPFRE: Madrid, Spain, 2021; ISBN 978-84-9844-782-8. [Google Scholar]
- Koletzko, B.; Cremer, M.; Flothkötter, M.; Graf, C.; Hauner, H.; Hellmers, C.; Kersting, M.; Krawinkel, M.; Przyrembel, H.; Röbl-Mathieu, M.; et al. Diet and Lifestyle Before and During Pregnancy—Practical Recommendations of the Germany-wide Healthy Start—Young Family Network. Geburtsh Frauenheilk 2018, 78, 1262–1282. [Google Scholar] [CrossRef] [PubMed]
- Meija, L.; Rezeberga, D. Proper Maternal Nutrition during Pregnancy Planning and Pregnancy: A Healthy Start in Life Recommendations for Health Care Professionals—The Experience from Latvia. Recommendations for Health Care Specialists. 2017. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/publications/2017/propermaternal-nutrition-during-pregnancy-planning-and-pregnancy-a-healthy-start-in-life-2017 (accessed on 17 June 2023).
- United Nations International Children’s Emergency Fund (UNICEF). UNICEF Programming Guidance. Maternal Nutrition Prevention of Malnutrition in Women before and during Pregnancy and while Breastfeeding; Nutrition Guidance Series; UNICEF: New York, NY, USA, 2022. [Google Scholar]
- U.S. Department of Health and Human Services. Nutrition During Pregnancy to Support a Healthy Mom and Baby. Available online: https://health.gov/news/202202/nutrition-during-pregnancy-support-healthy-mom-and-baby (accessed on 20 October 2023).
- World Health Organization (WHO). Good Maternal Nutrition. The Best Start in Life; WHO Regional Office for Europe: Copenhagen, Denmark, 2016; ISBN 978-92-890-5154-5. [Google Scholar]
- World Health Organization (WHO). WHO Antenatal Care Recommendations for a Positive Pregnancy Experience. Nutritional Interventions Update: Multiple Micronutrient Supplements during Pregnancy; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000778-9. [Google Scholar]
- Brown, B.; Wright, C. Safety and efficacy of supplements in pregnancy. Nutr. Rev. 2019, 78, 813–826. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Daily Iron and Folic Acid Supplementation during Pregnancy. Available online: https://www.who.int/tools/elena/interventions/daily-iron-pregnancy (accessed on 21 October 2023).
- Michael, K.; Georgieff, M.D. Iron Deficiency in Pregnancy. Am. J. Obstet. Gynecol. 2020, 223, 516–524. [Google Scholar] [CrossRef]
- Omotayo, M.O.; Dickin, K.L.; O’Brien, K.O.; Neufeld, L.M.; De Regil, L.M.; Stoltzfus, R.J. Calcium supplementation to prevent preeclampsia: Translating guidelines into practice in low-income countries. Adv. Nutr. 2016, 7, 275–278. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Calcium Supplementation during Pregnancy to Reduce the Risk of Pre-Eclampsia. Available online: https://www.who.int/tools/elena/interventions/calcium-pregnancy (accessed on 21 October 2023).
- Iqbal, S.; Ali, I. Effect of maternal zinc supplementation or zinc status on pregnancy complications and perinatal outcomes: An umbrella review of meta-analyses. Heliyon 2021, 7, e07540. [Google Scholar] [CrossRef]
- Gohari, H.; Khajavian, N.; Mahmoudian, A.; Bilandi, R.R. Copper and zinc deficiency to the risk of preterm labor in pregnant women: A case control study. BMC Pregnancy Childbirth 2023, 23, 366. [Google Scholar] [CrossRef]
- Turan, K.; Arslan, A.; Uçkan, K.; Demir, H.; Demir, C. Change of the levels of trace elements and heavy metals in threatened abortion. J. Chin. Med. Assoc. 2019, 82, 554–557. [Google Scholar] [CrossRef]
- Parisi, F.; Di Bartolo, I.; Savasi, V.M.; Cetin, I. Micronutrient supplementation in pregnancy: Who, what and how much? Obstet. Med. 2019, 12, 5–13. [Google Scholar] [CrossRef]
- Rumbold, A.; Ota, E.; Nagata, C.; Shahrook, S.; Crowther, C.A. Vitamin C supplementation in pregnancy. CDSR 2015, 9, CD004072. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Vitamin C Supplementation in Pregnancy. Systematic Review Summary. Available online: https://www.who.int/tools/elena/review-summaries/vitaminsec-pregnancy--vitamin-c-supplementation-in-pregnancy (accessed on 21 October 2023).
- Prabhu, K.; Dastidar, R.G.; Aroor, A.R.; Rao, M.; Poojari, V.G.; Varashree, B.S. Micronutrients in Adverse Pregnancy Outcomes. F1000Research 2022, 11, 1369. [Google Scholar] [CrossRef]
- WHO. Guideline: Vitamin D Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization (WHO). Vitamin D Supplementation during Pregnancy. Available online: https://www.who.int/tools/elena/interventions/vitamind-supp-pregnancy (accessed on 21 October 2023).
- American Pregnancy Association. Roles of Vitamin B in Pregnancy. Available online: https://americanpregnancy.org/healthy-pregnancy/pregnancy-health-wellness/vitamin-b-pregnancy/ (accessed on 15 September 2023).
- Ballestín, S.S.; Campos, M.I.G.; Ballestín, J.B.; Bartolomé, M.J.L. Is Supplementation with Micronutrients Still Necessary during Pregnancy? A Review. Nutrients 2021, 13, 3134. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Vitamin B6 Supplementation during Pregnancy. Available online: https://www.who.int/tools/elena/interventions/vitaminb6-pregnancy (accessed on 21 October 2023).
- Domínguez, L.; Fernández-Ruiz, V.; Cámara, M. An international regulatory review of food health-related claims in functional food products labeling. J. Funct. Foods 2020, 68, 103896. [Google Scholar] [CrossRef]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Informes del Sistema Coordinado de Intercambio de Información (SCIRI). Available online: https://www.aesan.gob.es/AECOSAN/web/seguridad_alimentaria/subseccion/SCIRI.htm (accessed on 13 July 2023).
- European Commission. EU Register of Nutrition and Health Claims Made on Food. Available online: http://ec.europa.eu/food/safety/labelling_nutrition/claims/register/public/?event=register.home (accessed on 18 June 2023).
- Sánchez-Mata, M.C.; Cabrera Loera, R.D.; Morales, P.; Fernández-Ruiz, V.; Cámara, M.; Díez Marqués, C.; Pardo-de-Santayana, M.; Tardío, J. Wild vegetables of the Mediterranean area as valuable sources of bioactive compounds. Genet. Resour. Crop Evol. 2012, 59, 431–443. [Google Scholar] [CrossRef]
- Domínguez, L.; Dorta, E.; Maher, S.; Morales, P.; Fernández-Ruiz, V.; Cámara, M.; Sánchez-Mata, M.C. Potential Nutrition and Health Claims in Deastringed Persimmon Fruits (Diospyros kaki L.), Variety ‘Rojo Brillante’, PDO ‘Ribera del Xúquer’. Nutrients 2020, 12, 1397. [Google Scholar] [CrossRef]
- Kaur, R.; Nayyar, H. Ascorbic Acid: A Potent Defender Against Environmental Stresses. Antioxid. Redox Signal. 2014, 235–287. [Google Scholar] [CrossRef]
- Sánchez-Mata, M.C.; Cámara-Hurtado, M.; Diez-Marques, C.; Torija-Isasa, M.E. Comparison of HPLC and spectrofluorimetry for vitamin C analysis of green beans. Eur. Food Res. Technol. 2000, 210, 220–225. [Google Scholar] [CrossRef]
- Latimer, G.W. Official Methods of Analysis of AOAC International, 21st ed.; AOAC International: Gaithersburg, MD, USA, 2019. [Google Scholar]
- Fernández-Ruiz, V.; Olives, A.I.; Cámara, M.; Sánchez-Mata, M.C.; Torija, M.E. Mineral and trace elements content in 30 accessions of tomato fruits (Solanum lycopersicum L.) and wild relatives (Solanum pimpinellifolium L., Solanum cheesmaniae L. Riley, and Solanum habrochaites S. Knapp & D.M. Spooner). Biol. Trace Elem. Res. 2010, 141, 329–339. [Google Scholar] [CrossRef]
- European Parliament and Council of the European Union. Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on food. Off. J. Eur. Union 2006, L404, 9. Available online: http://eurlex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A02006R1924-20121129 (accessed on 21 June 2023).
- European Parliament and Council of the European Union. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004. Off. J. Eur. Union 2011, L304, 18. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32011R1169 (accessed on 19 June 2023).
- European Commission. Guidance Document for Competent Authorities for the Control of Compliance with EU Legislation on Regulation (EU) No 1169/2011, Council Directive 90/496/EEC and Directive 2002/46/EC with Regard to the Setting of Tolerances for Nutrient Values Declared on a Label. Available online: https://ec.europa.eu/food/safety/labelling_nutrition/labelling_legislation/nutrition-labelling_en (accessed on 17 June 2023).
- European Food Safety Authority (EFSA). Tolerable Upper Intake Levels for Vitamins and Minerals. Scientific Committee on Food Scientific Panel on Dietetic Products, Nutrition and Allergies. 2006. Available online: https://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/ndatolerableuil.pdf (accessed on 21 June 2023).
- European Food Safety Authority (EFSA). Scientific Opinion on the Tolerable Upper Intake Level of Calcium. EFSA J. 2012, 10, 2814. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Overview on Tolerable Upper Intake Levels as derived by the Scientific Committee on Food (SCF) and the EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Summary of Tolerable Upper Intake Levels. 2018. Available online: https://www.efsa.europa.eu/sites/default/files/assets/UL_Summary_tables.pdf (accessed on 21 June 2023).



{kind=link}
{kind=link}
{kind=link}
| Micronutrients | Health Claims (N°) | Approved Claims |
|---|---|---|
| Vitamin C | 15 | Vitamin C contributes to maintaining the normal functions of the immune system during and after intense physical exercise; normal collagen formation for the normal function of blood vessels, bones, cartilage, gums, skin, teeth; normal energy-yielding metabolism; functioning of the nervous system; psychological function; function of the immune system; protection of cells from oxidative stress; reduction of tiredness and fatigue; regeneration of the reduced form of vitamin E. Vitamin C increases iron absorption. |
| Vitamin B9 | 8 | Folate contributes to maternal tissue growth during pregnancy, normal amino acid synthesis, blood formation, homocysteine metabolism, psychological function, function of the immune system, reduction of tiredness and fatigue. Folate has a role in the process of cell division. |
| Iron | 7 | Iron contributes to normal cognitive function, energy-yielding metabolism, formation of red blood cells and hemoglobin, oxygen transport in the body, function of the immune system, reduction of tiredness and fatigue. Iron has a role in the process of cell division. |
| Copper | 8 | Copper contributes to maintenance of normal connective tissues, energy-yielding metabolism, functioning of the nervous system, hair pigmentation, iron transport in the body, skin pigmentation, function of the immune system, protection of cells from oxidative stress. |
| Manganese | 4 | Manganese contributes to normal energy-yielding metabolism, formation of connective tissue, maintenance of normal bones, protection of cells from oxidative stress. |
| Zinc | 18 | Zinc contributes to normal acid–base metabolism, carbohydrate metabolism, cognitive function, DNA synthesis, fertility and reproduction, macronutrient metabolism, metabolism of fatty acids, metabolism of vitamin A, protein synthesis. Zinc contributes to the maintenance of normal bones, hair, nails, skin, testosterone levels in the blood, vision, function of the immune system. Zinc contributes to the protection of cells from oxidative stress. Zinc has a role in the process of cell division. |
| Calcium | 8 | Calcium contributes to normal blood clotting, energy-yielding metabolism, muscle function, neurotransmission, function of digestive enzymes. Calcium is needed for the maintenance of normal bones and teeth. Calcium has a role in the process of cell division and specialization. |
| Magnesium | 10 | Magnesium contributes to reduction of tiredness and fatigue, electrolyte balance, normal energy-yielding metabolism, functioning of the nervous system, muscle function, protein synthesis, psychological function, maintenance of normal bones and teeth. Magnesium has a role in the process of cell division. |
| Micronutrients | NRV | Required Amount to Use the Claim (15% NRV) |
|---|---|---|
| Vitamin C | 80 mg | 12 mg/100 g |
| Vitamin B9 | 200 µg | 30 µg/100 g |
| Fe | 14 mg | 2.1 mg/100 g |
| Cu | 1 mg | 0.15 mg/100 g |
| Mn | 2 mg | 0.3 mg/100 g |
| Zn | 10 mg | 1.5 mg/100 g |
| Ca | 800 mg | 120 mg/100 g |
| Mg | 375 mg | 56.25 mg/100 g |
| Sample | Analytical Value (mg/sachet) | Declared Value (mg/sachet) | Range of Tolerances (RT) (mg/sachet) |
|---|---|---|---|
| S1 | 127.385 ± 6.179 a 111.804 ± 7.347 a = 119.595 ± 11.017 | 110 | 87.600–165.600 |
| S4 | 217.856 ± 7.307 a 233.815 ± 7.451 a = 225.836 ± 11.285 | 225 | 179.600–338.100 |
| Sample | Analytical Value Range (mg/sachet) | Declared Value (mg/sachet) | Range of Tolerances (RT) (mg/sachet) |
|---|---|---|---|
| S1 | 499.63–519.47 | 500 | 399.60–750.60 |
| S2 | 399.12–418.06 | 400 | 390.03–600.60 |
| S3 | 426.27–432.77 | 400 | 396.25–600.60 |
| S4 | 211.60–229.78 | 200 | 159.60–300.60 |
| Fe | Cu | Mn | Zn | Ca | Mg | |
|---|---|---|---|---|---|---|
| S1 sample | ||||||
| Batch 1 | 4.856 ± 0.017 a | 0.954 ± 0.003 a | 0.070 ± 0.007 a | 5.205 ± 0.019 a | 393.016 ± 5.528 a | 182.486 ± 3.213 a |
| Batch 2 | 4.864 ± 0.021 a | 0.931 ± 0.004 a | 0.072 ± 0.007 a | 5.227 ± 0.019 a | 387.441 ± 3.835 a | 177.360 ± 2.145 a |
| Mean | 4.860 ± 0.005 | 0.942 ± 0.017 | 0.071 ± 0.001 | 5.216 ± 0.016 | 390.228 ± 3.942 | 179.923 ± 3.625 |
| S2 sample | ||||||
| Batch 1 | 0.047 ± 0.005 a | 0.026 ± 0.000 a | 0.025 ± 0.002 a | 0.038 ± 0.003 a | 1.285 ± 0.038 a | 0.036 ± 0.003 a |
| Batch 2 | 0.049 ± 0.002 a | 0.024 ± 0.002 a | 0.025 ± 0.002 a | 0.039 ± 0.002 a | 1.396 ± 0.136 a | 0.039 ± 0.002 a |
| Mean | 0.048 ± 0.002 | 0.025 ± 0.001 | 0.025 ± 0.000 | 0.038 ± 0.000 | 1.340 ± 0.079 | 0.038 ± 0.002 |
| S3 sample | ||||||
| Batch 1 | 0.017 ± 0.000 a | 0.014 ± 0.001 a | 2.009 ± 0.130 a | 10.791 ± 0.524 a | 1.010 ± 0.100 a | 0.090 ± 0.006 a |
| Batch 2 | 0.015 ± 0.000 a | 0.015 ± 0.001 a | 2.032 ± 0.096 a | 10.560 ± 0.393 a | 1.053 ± 0.103 a | 0.078 ± 0.001 a |
| Mean | 0.705 ± 0.066 | 0.014 ± 0.000 | 2.020 ± 0.016 | 10.675 ± 0.163 | 1.031 ± 0.030 | 0.084 ± 0.008 |
| S4 sample | ||||||
| Batch 1 | 6.123 ± 0.060 a | 0.555 ± 0.012 a | 0.989 ± 0.030 a | 6.033 ± 0.224 a | 200.358 ± 1.456 a | 153.869 ± 6.987 a |
| Batch 2 | 6.153 ± 0.096 a | 0.550 ± 0.009 a | 1.000 ± 0.037 a | 6.011 ± 0.210 a | 200.213 ± 6.087 a | 148.602 ± 8.524 a |
| Mean | 6.138 ± 0.021 | 0.553 ± 0.003 | 0.995 ± 0.008 | 6.022 ± 0.016 | 200.286 ± 0.102 | 151.236 ± 3.724 |
| Mineral | Analytical Value (mg/sachet) | Declared Value (mg/sachet) | Range of Tolerances (RT) (mg/sachet) |
|---|---|---|---|
| Fe | |||
| S1 sample | 4.855–4.865 | 5 | 4–7.25 |
| S4 sample | 6.117–6.159 | 6 | 4.8–8.7 |
| Cu | |||
| S1 sample | 0.925–0.959 | 1 | 0.8–1.45 |
| S4 sample | 0.550–0.555 | 0.5 | 0.4–0.725 |
| Mn | |||
| S3 sample | 2.004–2.036 | 2 | 1.6–2.9 |
| S4 sample | 0.987–1.003 | 1 | 0.8–1.45 |
| Zn | |||
| S1 sample | 5.200–5.232 | 5 | 4–7.25 |
| S3 sample | 10.512–10.838 | 10 | 8–14.5 |
| S4 sample | 6.006–6.038 | 6 | 4.8–8.7 |
| Ca | |||
| S1 sample | 386.286–394.17 | 400 | 320–580 |
| S4 sample | 200.184–200.388 | 200 | 160–290 |
| Mg | |||
| S1 sample | 176.298–183.548 | 180 | 144–261 |
| S4 sample | 147.512–154.960 | 150 | 120–217.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez, L.; Fernández-Ruiz, V.; Cámara, M. Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment. Nutrients 2023, 15, 4592. https://doi.org/10.3390/nu15214592
Domínguez L, Fernández-Ruiz V, Cámara M. Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment. Nutrients. 2023; 15(21):4592. https://doi.org/10.3390/nu15214592
Chicago/Turabian StyleDomínguez, Laura, Virginia Fernández-Ruiz, and Montaña Cámara. 2023. "Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment" Nutrients 15, no. 21: 4592. https://doi.org/10.3390/nu15214592
APA StyleDomínguez, L., Fernández-Ruiz, V., & Cámara, M. (2023). Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment. Nutrients, 15(21), 4592. https://doi.org/10.3390/nu15214592