
Eating Attitudes of Patients with Celiac Disease in Brazil: A Nationwide Assessment with the EAT-26 Instrument

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
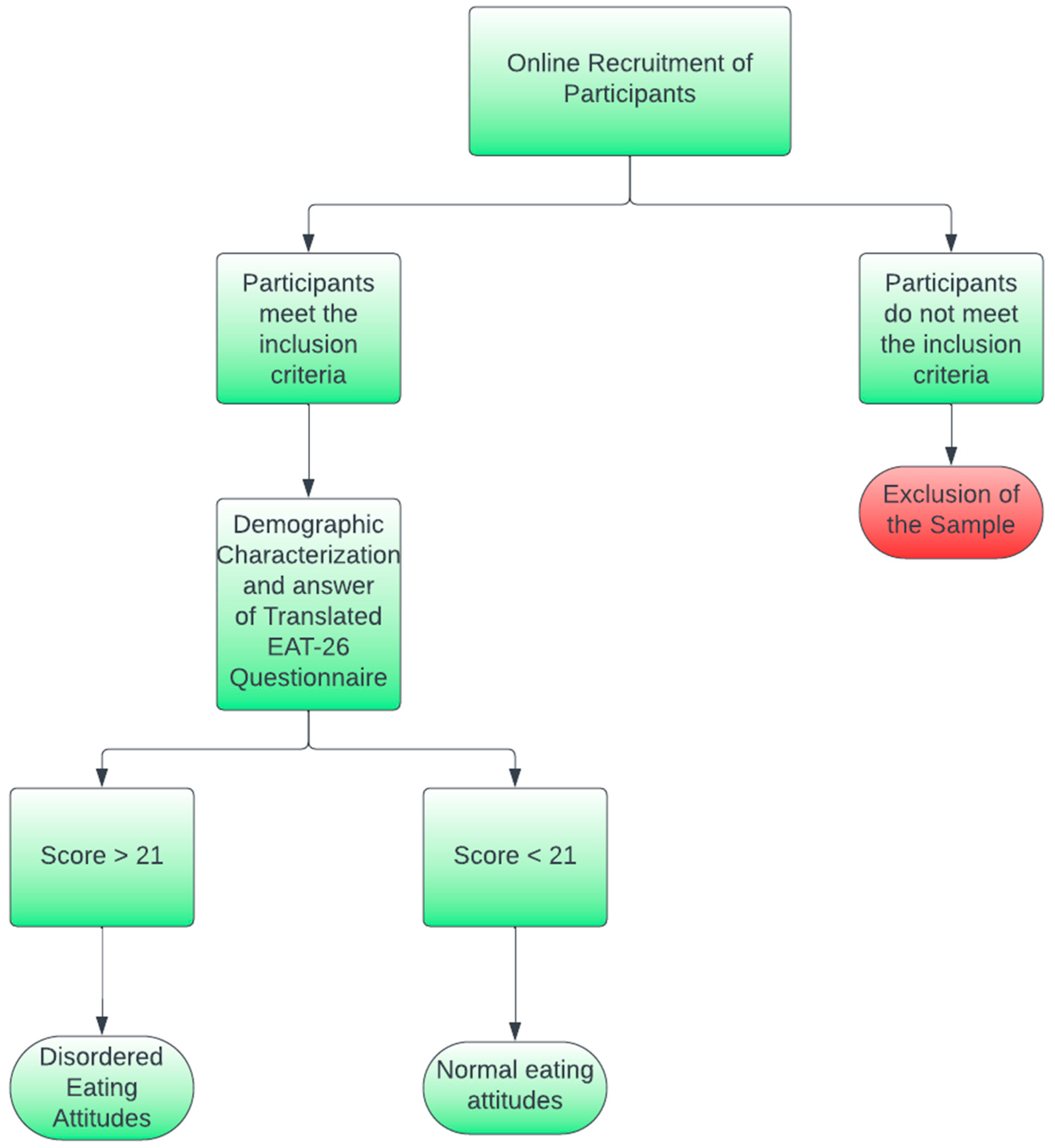
2.1. Study Design and Instrument
2.2. Recruitment of Participants and Ethics
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Included Participants
3.2. Questionnaire Internal Consistency and Obtained Scores
4. Discussion
4.1. Characteristics of the Sample
4.2. Scores Obtained from the Self-Administered Online Questionnaire
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Please Answer All the Following Items | Always | Usually | Often | Sometimes | Rarely | Never |
| 1—I’m terrified of the idea of gaining weight | ||||||
| 2—I avoid eating when I’m hungry | ||||||
| 3—I feel worried about food | ||||||
| 4—Continuing to overeat makes me feel like I can’t stop | ||||||
| 5—I cut my food into small pieces | ||||||
| 6—I pay attention to the number of calories in the food I eat | ||||||
| 7—I particularly avoid foods rich in carbohydrates (e.g., bread, rice, potatoes, etc.) | ||||||
| 8—I feel like others would like me to eat more. | ||||||
| 9—Vomiting after eating | ||||||
| 10—I feel extremely guilty after eating | ||||||
| 11—I worry about wanting to be thinner | ||||||
| 12—I think about burning extra calories when I exercise | ||||||
| 13—People think I’m too thin | ||||||
| 14—I worry about having fat on my body | ||||||
| 15—It takes me longer to eat my meals than other people | ||||||
| 16—I avoid eating foods that contain sugar | ||||||
| 17—I usually eat diet foods | ||||||
| 18—I feel like food controls my life | ||||||
| 19—I demonstrate self-control around food | ||||||
| 20—I feel like others pressure me to eat | ||||||
| 21—I spend a lot of time thinking about eating | ||||||
| 22—I feel discomfort after eating sweets | ||||||
| 23—I follow weight loss regimes | ||||||
| 24—I like feeling my stomach empty | ||||||
| 25—I like to try new high-calorie foods | ||||||
| 26—I feel like vomiting after meals |
References
- Catassi, C.; Fasano, A. Celiac Disease. Curr. Opin. Gastroenterol. 2008, 24, 687–691. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Corazza, G.R. Coeliac Disease. Lancet 2009, 373, 1480–1493. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. Diagnosis and Management of Adult Coeliac Disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef]
- Leffler, D.; Saha, S.; Farrell, R.J. Celiac Disease. Am. J. Manag. Care 2003, 9, 825–883. [Google Scholar] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Catassi, C. Celiac Disease. N. Engl. J. Med. 2012, 367, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Groll, A. Short Stature as the Primary Manifestation of Coeliac Disease. Lancet 1980, 316, 1097–1099. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, G.; Markopoulos, K.; Albertini, R.; Di Sabatino, A.; Biagi, F.; Ciccocioppo, R.; Arbustini, E.; Corazza, G.R. Anemia of Chronic Disease and Defective Erythropoietin Production in Patients with Celiac Disease. Haematologica 2008, 93, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Biel, K.; Böhm, M.; Luger, T.A.; Bonsmann, G. Long-Standing Oral Aphthae—A Clue to the Diagnosis of Coeliac Disease. Dermatology 2000, 200, 340. [Google Scholar] [CrossRef]
- Ludvigsson, J.; Montgomery, S.; Ekbom, A. Celiac Disease and Risk of Adverse Fetal Outcome: A Population-Based Cohort Study. Gastroenterology 2005, 129, 454–463. [Google Scholar] [CrossRef]
- West, J.; Logan, R.F.A.; Smith, C.J.; Hubbard, R.B.; Card, T.R. Malignancy and Mortality in People with Coeliac Disease: Population Based Cohort Study. BMJ 2004, 329, 716–719. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Logan, R.F.A.; Card, T.R.; Smith, C.; Hubbard, R. Fracture Risk in People with Celiac Disease: A Population-Based Cohort Study. Gastroenterology 2003, 125, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Pelizzaro, F.; Marsilio, I.; Fassan, M.; Piazza, F.; Barberio, B.; D’Odorico, A.; Savarino, E.V.; Farinati, F.; Zingone, F. The Risk of Malignancies in Celiac Disease—A Literature Review. Cancers 2021, 13, 5288. [Google Scholar] [CrossRef] [PubMed]
- Farage, P.; Zandonadi, R.P.; Gandolfi, L.; Pratesi, R.; Falcomer, A.L.; Araújo, L.S.; Nakano, E.Y.; Ginani, V.C. Accidental Gluten Contamination in Traditional Lunch Meals from Food Services in Brasilia, Brazil. Nutrients 2019, 11, 1924. [Google Scholar] [CrossRef]
- Falcomer, A.L.; Santos Araújo, L.; Farage, P.; Santos Monteiro, J.; Yoshio Nakano, E.; Puppin Zandonadi, R. Gluten Contamination in Food Services and Industry: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2020, 60, 479–493. [Google Scholar] [CrossRef]
- Alencar, N.M.M.; Araújo, V.A.; Faggian, L.; Silveira Araújo, M.B.; Capriles, V.D. What about Gluten-free Products? An Insight on Celiac Consumers’ Opinions and Expectations. J. Sens. Stud. 2021, 36, e12664. [Google Scholar] [CrossRef]
- Bagolin do Nascimento, A.; Medeiros Rataichesck Fiates, G.; dos Anjos, A.; Teixeira, E. Availability, Cost and Nutritional Composition of Gluten-Free Products. Br. Food J. 2014, 116, 1842–1852. [Google Scholar] [CrossRef]
- da Silva, L.A.; Tavares, I.M.d.C.; de Oliveira, C.P.; de Oliveira, J.R.; Irfan, M.; Bilal, M.; Franco, M. Nutritional Quality and Price of Regular Food versus Gluten-Free on E-Commerce Platforms. Res. Soc. Dev. 2021, 10, e137101018751. [Google Scholar] [CrossRef]
- Satherley, R.-M.; Howard, R.; Higgs, S. The Prevalence and Predictors of Disordered Eating in Women with Coeliac Disease. Appetite 2016, 107, 260–267. [Google Scholar] [CrossRef]
- Whitaker, J.K.H.; West, J.; Holmes, G.K.T.; Logan, R.F.A. Patient Perceptions of the Burden of Coeliac Disease and Its Treatment in the UK. Aliment. Pharmacol. Ther. 2009, 29, 1131–1136. [Google Scholar] [CrossRef]
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating Disorders. Lancet 2020, 395, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Nunes, L.G.; Santos, M.C.S.; Souza, A.A. Fatores de Risco Associados Ao Desenvolvimento de Bulimia e Anorexia Nervosa Em Estudantes Universitários: Uma Revisão Integrativa. HU Rev. 2017, 43, 1–13. [Google Scholar] [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of Eating Disorders over the 2000–2018 Period: A Systematic Literature Review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Moreira-Almeida, A.; Cardeña, E. Diagnóstico Diferencial Entre Experiências Espirituais e Psicóticas Não Patológicas e Transtornos Mentais: Uma Contribuição de Estudos Latino-Americanos Para o CID-11. Rev. Bras. Psiquiatr. 2011, 33, s21–s28. [Google Scholar] [CrossRef]
- Araújo, Á.C.; Neto, F.L. A Nova Classificação Americana Para Os Transtornos Mentais—O DSM-5. Rev. Bras. Ter. Comport. E Cogn. 2014, 16, 67–82. [Google Scholar] [CrossRef]
- Freitas, S.; Gorenstein, C.; Appolinario, J.C. Instrumentos Para a Avaliação Dos Transtornos Alimentares. Rev. Bras. Psiquiatr. 2002, 24, 34–38. [Google Scholar] [CrossRef]
- Bighetti, F.; Dos Santos, C.B.; Dos Santos, J.E.; Pilot Pessa, R. Translation and Validation of the Eating Attitudes Test in Female Adolescents in Ribeirão Preto, SP, Brazil. J. Bras. Psiquiatr. 2004, 53, 339–346. [Google Scholar]
- Passananti, V.; Siniscalchi, M.; Zingone, F.; Bucci, C.; Tortora, R.; Iovino, P.; Ciacci, C. Prevalence of Eating Disorders in Adults with Celiac Disease. Gastroenterol. Res. Pract. 2013, 2013, 491657. [Google Scholar] [CrossRef]
- Tokatly Latzer, I.; Lerner-Geva, L.; Stein, D.; Weiss, B.; Pinhas-Hamiel, O. Disordered Eating Behaviors in Adolescents with Celiac Disease. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2020, 25, 365–371. [Google Scholar] [CrossRef]
- Pratesi, C.P.; Häuser, W.; Uenishi, R.H.; Selleski, N.; Nakano, E.Y.; Gandolfi, L.; Pratesi, R.; Zandonadi, R.P. Quality of Life of Celiac Patients in Brazil: Questionnaire Translation, Cultural Adaptation and Validation. Nutrients 2018, 10, 1167. [Google Scholar] [CrossRef]
- White, L.E.; Bannerman, E.; Gillett, P.M. Coeliac Disease and the Gluten-Free Diet: A Review of the Burdens; Factors Associated with Adherence and Impact on Health-Related Quality of Life, with Specific Focus on Adolescence. J. Hum. Nutr. Diet. 2016, 29, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.B. Anthropometry as a Tool for Measuring Malnutrition: Impact of the New WHO Growth Standards and Reference. Int. Child Health 2013, 30, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Falcomer, A.L.; Farage, P.; Pratesi, C.B.; Pratesi, R.; Gandolfi, L.; Nakano, E.Y.; Raposo, A.; Zandonadi, R.P. Health-Related Quality of Life and Experiences of Brazilian Celiac Individuals over the Course of the SARS-CoV-2 Pandemic. Nutrients 2021, 13, 1582. [Google Scholar] [CrossRef]
- Thomas, H.J.; Ahmad, T.; Rajaguru, C.; Barnardo, M.; Warren, B.F.; Jewell, D.P. Contribution of Histological, Serological, and Genetic Factors to the Clinical Heterogeneity of Adult-Onset Coeliac Disease. Scand. J. Gastroenterol. 2009, 44, 1076–1083. [Google Scholar] [CrossRef]
- Ngo, S.T.; Steyn, F.J.; McCombe, P.A. Gender Differences in Autoimmune Disease. Front. Neuroendocrinol. 2014, 35, 347–369. [Google Scholar] [CrossRef]
- Megiorni, F.; Mora, B.; Bonamico, M.; Barbato, M.; Montuori, M.; Viola, F.; Trabace, S.; Mazzilli, M.C. HLA-DQ and Susceptibility to Celiac Disease: Evidence for Gender Differences and Parent-of-Origin Effects. Am. J. Gastroenterol. 2008, 103, 997–1003. [Google Scholar] [CrossRef]
- Jansson-Knodell, C.L.; King, K.S.; Larson, J.J.; Van Dyke, C.T.; Murray, J.A.; Rubio-Tapia, A. Gender-Based Differences in a Population-Based Cohort with Celiac Disease: More Alike than Unalike. Dig. Dis. Sci. 2018, 63, 184–192. [Google Scholar] [CrossRef]
- Pinkhasov, R.M.; Wong, J.; Kashanian, J.; Lee, M.; Samadi, D.B.; Pinkhasov, M.M.; Shabsigh, R. Are Men Shortchanged on Health? Perspective on Health Care Utilization and Health Risk Behavior in Men and Women in the United States. Int. J. Clin. Pract. 2010, 64, 475–487. [Google Scholar] [CrossRef]
- Singh, P.; Arora, S.; Singh, A.; Strand, T.A.; Makharia, G.K. Prevalence of Celiac Disease in Asia: A Systematic Review and Meta-Analysis. J. Gastroenterol. Hepatol. 2016, 31, 1095–1101. [Google Scholar] [CrossRef]
- Pratesi, R.; Gandolfi, L. Doença Celíaca: A Afecção Com Múltiplas Faces Celiac Disease: A Disease with Many Faces. J. Pediatr. Rio. J. 2005, 81, 357–358. [Google Scholar] [CrossRef]
- Machado, J.; Gandolfi, L.; Coutinho De Almeida, F.; Malta Almeida, L.; Puppin Zandonadi, R.; Pratesi, R. Gluten-Free Dietary Compliance in Brazilian Celiac Patients: Questionnaire versus Serological Test. Nutr. Clin. Y Diet. Hosp. 2013, 33, 46–49. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional Por Amostra de Domicílio; Instituto Brasileiro de Geografia e Estatística: Brasília, Brazil, 2023; pp. 1–230.
- da Costa Louzada, M.L.; Baraldi, L.G.; Steele, E.M.; Martins, A.P.B.; Canella, D.S.; Moubarac, J.C.; Levy, R.B.; Cannon, G.; Afshin, A.; Imamura, F.; et al. Consumption of Ultra-Processed Foods and Obesity in Brazilian Adolescents and Adults. Prev. Med. Baltim 2015, 81, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Leite Canhada, S.; Cristine Luft, V.; Giatti, L.; Bartholow Duncan, B.; Chor, D.; de Jesus da Fonseca, M.M.; Maria Alvim Matos, S.; del Carmen Bisi Molina, M.; Maria Barreto, S.; Bertazzi Levy, R.; et al. Ultra-Processed Foods, Incident Overweight and Obesity, and Longitudinal Changes in Weight and Waist Circumference: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Public Health Nutr. 2019, 23, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Bulik, C.M. Risk Factors for Eating Disorders. Am. Psychol. 2007, 62, 181–198. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Rosselli, F.; Perrin, N.; DeBar, L.; Wilson, G.T.; May, A.; Kraemer, H.C. Gender Difference in the Prevalence of Eating Disorder Symptoms. Int. J. Eat. Disord. 2009, 42, 471–474. [Google Scholar] [CrossRef]
- Manzato, E. Eating Disorders and Disordered Eating Behaviors in Males: A Challenging Topic. Eat. Weight. Disord. —Stud. Anorex. Bulim. Obes. 2019, 24, 651–652. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.B.; Bulik, C.M. Gender Differences in Compensatory Behaviors, Weight and Shape Salience, and Drive for Thinness. Eat. Behav. 2004, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Seeley, J.R.; Moerk, K.C.; Striegel-Moore, R.H. Gender Differences in Eating Disorder Symptoms in Young Adults. Int. J. Eat. Disord. 2002, 32, 426–440. [Google Scholar] [CrossRef] [PubMed]
- Mulders-Jones, B.; Mitchison, D.; Girosi, F.; Hay, P. Socioeconomic Correlates of Eating Disorder Symptoms in an Australian Population-Based Sample. PloS ONE 2017, 12, e0170603. [Google Scholar] [CrossRef]
- Alvarenga, M.d.S.; Scagliusi, F.B.; Philippi, S.T. Comportamento de Risco Para Transtorno Alimentar Em Universitárias Brasileiras. Arch. Clin. Psychiatry 2011, 38, 03–07. [Google Scholar] [CrossRef]
- Mitchell, J.E.; King, W.C.; Courcoulas, A.; Dakin, G.; Elder, K.; Engel, S.; Flum, D.; Kalarchian, M.; Khandelwal, S.; Pender, J.; et al. Eating Behavior and Eating Disorders in Adults before Bariatric Surgery. Int. J. Eat. Disord. 2015, 48, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Pinaquy, S.; Chabrol, H.; Simon, C.; Louvet, J.P.; Barbe, P. Emotional Eating, Alexithymia, and Binge-Eating Disorder in Obese Women. Obes. Res. 2003, 11, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Hrabosky, J.I.; Masheb, R.M.; White, M.A.; Grilo, C.M. Overvaluation of Shape and Weight in Binge Eating Disorder. J. Consult. Clin. Psychol. 2007, 75, 175–180. [Google Scholar] [CrossRef]
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered Eating and Obesity: Associations between Binge-Eating Disorder, Night-Eating Syndrome, and Weight-Related Comorbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef]
- Gowers, S.G.; Shore, A. Development of Weight and Shape Concerns in the Aetiology of Eating Disorders. Br. J. Psychiatry 2001, 179, 236–242. [Google Scholar] [CrossRef]
- Wadden, T.A.; Foster, G.D.; Sarwer, D.B.; Anderson, D.A.; Gladis, M.; Sanderson, R.S.; Letchak, R.V.; Berkowitz, R.I.; Phelan, S. Dieting and the Development of Eating Disorders in Obese Women: Results of a Randomized Controlled Trial. Am. J. Clin. Nutr. 2004, 80, 560–568. [Google Scholar] [CrossRef]
- Fassino, S.; Leombruni, P.; Pierò, A.; Abbate-Daga, G.; Rovera, G.G. Mood, Eating Attitudes, and Anger in Obese Women with and without Binge Eating Disorder. J. Psychosom. Res. 2003, 54, 559–566. [Google Scholar] [CrossRef]
- Greeno, C.G.; Wing, R.R.; Shiffman, S. Binge Antecedents in Obese Women with and without Binge Eating Disorder. J. Consult. Clin. Psychol. 2000, 68, 95–102. [Google Scholar] [CrossRef]
- Specker, S.; de Zwaan, M.; Raymond, N.; Mitchell, J. Psychopathology in Subgroups of Obese Women with and without Binge Eating Disorder. Compr. Psychiatry 1994, 35, 185–190. [Google Scholar] [CrossRef]
- Nunes, M.A.; Barras, F.C.; Anselmo Olinto, M.T.; Carney, S.; Mari, J.D.J. Prevalence of Abnormal Eating Behaviours and Inappropriate Methods of Weight Control in Young Women from Brazil: A Population-Based Study. Eat. Weight. Disord. 2003, 8, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Ciacci, C.; Zingone, F. The Perceived Social Burden in Celiac Disease. Diseases 2015, 3, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Zarkadas, M.; Dubois, S.; MacIsaac, K.; Cantin, I.; Rashid, M.; Roberts, K.C.; La Vieille, S.; Godefroy, S.; Pulido, O.M. Living with Coeliac Disease and a Gluten-Free Diet: A Canadian Perspective. J. Hum. Nutr. Diet. 2013, 26, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Gholmie, Y.; Lee, A.R.; Satherley, R.-M.; Schebendach, J.; Zybert, P.; Green, P.H.R.; Lebwohl, B.; Wolf, R. Maladaptive Food Attitudes and Behaviors in Individuals with Celiac Disease and Their Association with Quality of Life. Dig. Dis. Sci. 2023, 68, 2899–2907. [Google Scholar] [CrossRef]
- Satherley, R.-M.; Higgs, S.; Howard, R. Disordered Eating Patterns in Coeliac Disease: A Framework Analysis. J. Hum. Nutr. Diet. 2017, 30, 724–736. [Google Scholar] [CrossRef]
- Satherley, R.; Howard, R.; Higgs, S. Disordered Eating Practices in Gastrointestinal Disorders. Appetite 2015, 84, 240–250. [Google Scholar] [CrossRef]
- Leffler, D.A.; Dennis, M.; Edwards George, J.B.; Kelly, C.P. The Interaction between Eating Disorders and Celiac Disease: An Exploration of 10 Cases. Eur. J. Gastroenterol. Hepatol. 2007, 19, 251–255. [Google Scholar] [CrossRef]
- Romão, B.; Falcomer, A.L.; Palos, G.; Cavalcante, S.; Braz, R.; Botelho, A.; Nakano, E.Y.; Raposo, A.; Shakeel, F.; Alshehri, S.; et al. Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis. Foods 2021, 10, 506. [Google Scholar] [CrossRef]
- Calvo-Lerma, J.; Crespo-Escobar, P.; Martínez-Barona, S.; Fornés-Ferrer, V.; Donat, E.; Ribes-Koninckx, C. Differences in the Macronutrient and Dietary Fibre Profile of Gluten-Free Products as Compared to Their Gluten-Containing Counterparts. Eur. J. Clin. Nutr. 2019, 73, 930–936. [Google Scholar] [CrossRef]
- Do Nascimento, A.B.; Fiates, G.M.R.; Dos Anjos, A.; Teixeira, E. Analysis of Ingredient Lists of Commercially Available Gluten-Free and Gluten-Containing Food Products Using the Text Mining Technique. Int. J. Food Sci. Nutr. 2013, 64, 217–222. [Google Scholar] [CrossRef]
- Romão, B.; Botelho, R.B.A.; Alencar, E.R.; da Silva, V.S.N.; Pacheco, M.T.B.; Zandonadi, R.P. Chemical Composition and Glycemic Index of Gluten-Free Bread Commercialized in Brazil. Nutrients 2020, 12, 2234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Number | % of the Sample |
|---|---|---|
| Gender (F or M) | ||
| Female | 371 | 96.36% |
| Male | 13 | 3.37% |
| Average Monthly Income (BRL and USD) | ||
| Up to 3000.00 BRL (USD 623.00) | 76 | 19.94% |
| 3000.01 to 5000 BRL (USD 623.23 to 1038.71) | 86 | 22.33% |
| 5000.01 to 10,000.01 BRL (USD 1038.71 to 2077.43) | 112 | 29.09% |
| >10,000.01 BRL (USD 2077.43) | 111 | 28.83% |
| Age (Years) | ||
| 18 to 24 years old | 110 | 28.57% |
| 25 to 34 years old | 136 | 35.32% |
| 35 to 44 years old | 76 | 19.74% |
| 45 to 54 years old | 43 | 11.16% |
| >55 years old | 20 | 5.19% |
| Educational Level | ||
| Up to High School | 55 | 14.28% |
| Undergraduate Level (B.Sc) | 189 | 49.09% |
| Graduate Level or Above (Post-Graduation, Masters degree, or Ph.D.) | 141 | 29.61% |
| Average BMI (Kg/m2) | ||
| Underweight (<18.5 Kg/m2) | 18.7 ± 11.29 Kg/m2; n = 30 | 7.79% |
| Normal Weight (≥18.5 Kg/m2 < 25 Kg/m2) | 17.23 ± 9.13 Kg/m2; n = 231 | 60% |
| Overweight (≥25 Kg/m2 < 30 Kg/m2) | 21.44 ± 10.09 Kg/m2; n = 84 | 21.81% |
| Obesity (≥30 Kg/m2) | 24.85 ± 11.28 Kg/m2; n = 40 | 10.38% |
| Variable | Average Score | p Value |
|---|---|---|
| Gender (F or M) | ||
| Female | 19.25 ± 10.05 b | <0.001 * |
| Male | 11.85 ± 3.59 a | |
| Average Monthly Income (BRL and USD) | ||
| Up to 3000.00 BRL (USD 623.00) | 20.66 ± 11.61 a | 0.355 ** |
| 3000.01 to 5000 BRL (USD 623.23 to 1038.71) | 17.84 ± 8.57 a | |
| 5000.01 to 10,000.01 BRL (USD 1038.71 to 2077.43) | 18.83 ± 9.39 a | |
| >10,000.01 BRL (USD 2077.43) | 19.14 ± 10.61 a | |
| Age (Years) | ||
| 18 to 24 years old | 19.19 ± 10.51 a | 0.183 ** |
| 25 to 34 years old | 19.82 ± 10.82 a | |
| 35 to 44 years old | 16.70 ± 8.60 a | |
| 45 to 54 years old | 20.72 ± 9.78 a | |
| >55 years old | 18.55 ± 6.47 a | |
| Educational Level | ||
| Up to High School | 20.02 ± 10.27 b | 0.025 ** |
| Undergraduate Level (B.Sc) | 20.14 ± 10.47 b | |
| Graduate Level or Above (Post-Graduation, Masters degree, or Ph.D.) | 17.23 ± 9.18 a | |
| Average Score by BMI (Kg/m2) | ||
| Underweight (<18.5 Kg/m2) | 18.70 ± 11.23 a | <0.001 ** |
| Adequate Weight (≥18.5 Kg/m2 < 25 Kg/m2) | 17.24 ± 9.13 a | |
| Overweight (≥25 Kg/m2 < 30 Kg/m2) | 21.44 ±10.10 ab | |
| Obesity (≥30 Kg/m2) | 24.85 ± 11.28 b | |
| Item | Always | Usually | Often | Sometimes | Rarely | Never | Always | Usually | Often | Sometimes | Rarely | Never |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall Score < 21; Frequency in (%) | Overall Score > 21; Frequency in (%) | |||||||||||
| 1 | 10.6 | 16.3 | 25.6 | 12.2 | 13.8 | 21.5 | 25.5 | 51.8 | 31.7 | 9.4 | 2.2 | 1.4 |
| 2 | 0.0 | 1.2 | 8.1 | 14.6 | 28.5 | 47.6 | 0.5 | 1.4 | 13.7 | 29.5 | 9.4 | 23.0 |
| 3 | 32.5 | 39.0 | 15.9 | 6.1 | 3.7 | 2.8 | 44.4 | 65.5 | 23.0 | 8.6 | 0.7 | 1.4 |
| 4 | 1.2 | 6.1 | 13.8 | 19.9 | 19.1 | 39.8 | 10.1 | 25.9 | 21.6 | 18.7 | 12.2 | 8.6 |
| 5 | 10.2 | 17.9 | 21.1 | 15.4 | 16.3 | 19.1 | 14.0 | 20.9 | 18.0 | 23.0 | 16.5 | 8.6 |
| 6 | 1.6 | 8.1 | 14.2 | 13.0 | 17.1 | 45.9 | 6.2 | 14.4 | 24.5 | 27.3 | 7.9 | 12.9 |
| 7 | 2.0 | 3.3 | 12.2 | 14.2 | 26.4 | 41.9 | 2.6 | 3.6 | 17.3 | 33.8 | 15.8 | 12.9 |
| 8 | 4.5 | 7.7 | 13.0 | 11.0 | 18.7 | 45.1 | 7.0 | 11.5 | 12.2 | 17.3 | 12.2 | 13.7 |
| 9 | 0.0 | 0.0 | 0.0 | 1.2 | 5.3 | 93.5 | 0.0 | 0.0 | 2.2 | 5.0 | 2.9 | 9.4 |
| 10 | 0.4 | 1.6 | 11.8 | 13.0 | 23.2 | 50.0 | 6.2 | 16.5 | 20.9 | 25.2 | 11.5 | 15.1 |
| 11 | 4.5 | 8.1 | 21.1 | 13.0 | 16.7 | 36.6 | 20.5 | 48.9 | 18.7 | 16.5 | 2.9 | 5.0 |
| 12 | 3.7 | 7.7 | 18.7 | 8.5 | 19.1 | 42.3 | 17.4 | 41.7 | 17.3 | 21.6 | 6.5 | 5.0 |
| 13 | 5.7 | 10.2 | 14.6 | 15.4 | 16.7 | 37.4 | 6.8 | 8.6 | 5.8 | 15.1 | 9.4 | 12.2 |
| 14 | 5.7 | 11.0 | 22.4 | 12.6 | 23.2 | 25.2 | 18.7 | 41.7 | 30.2 | 18.0 | 2.9 | 3.6 |
| 15 | 9.3 | 9.3 | 19.9 | 15.0 | 24.4 | 22.0 | 11.7 | 15.8 | 17.3 | 18.7 | 14.4 | 15.8 |
| 16 | 2.0 | 12.6 | 17.5 | 18.3 | 24.4 | 25.2 | 4.2 | 7.9 | 25.9 | 24.5 | 12.9 | 16.5 |
| 17 | 0.8 | 3.3 | 12.2 | 11.4 | 26.4 | 45.9 | 1.3 | 2.2 | 10.8 | 25.2 | 10.1 | 22.3 |
| 18 | 5.3 | 13.8 | 17.5 | 13.8 | 13.0 | 36.6 | 13.2 | 27.3 | 25.2 | 18.7 | 12.9 | 7.2 |
| 19 | 22.8 | 41.5 | 20.7 | 8.5 | 4.5 | 2.0 | 19.0 | 12.2 | 29.5 | 28.8 | 12.2 | 13.7 |
| 20 | 2.4 | 3.3 | 14.6 | 13.8 | 24.0 | 41.9 | 4.7 | 8.6 | 12.9 | 20.1 | 12.2 | 14.4 |
| 21 | 2.4 | 13.8 | 21.1 | 21.5 | 26.4 | 14.6 | 8.1 | 18.0 | 30.2 | 25.9 | 12.9 | 7.9 |
| 22 | 0.8 | 4.1 | 21.1 | 15.0 | 18.3 | 40.7 | 4.4 | 10.8 | 23.7 | 28.8 | 11.5 | 11.5 |
| 23 | 0.0 | 2.4 | 8.5 | 11.4 | 19.9 | 57.7 | 5.7 | 15.8 | 20.9 | 22.3 | 11.5 | 15.8 |
| 24 | 0.0 | 0.4 | 6.9 | 7.7 | 13.8 | 71.1 | 0.8 | 2.2 | 15.8 | 13.7 | 10.8 | 17.3 |
| 25 | 3.7 | 9.8 | 30.1 | 21.5 | 18.3 | 16.7 | 5.5 | 8.6 | 14.4 | 27.3 | 18.0 | 23.0 |
| 26 | 0.0 | 1.2 | 1.6 | 3.7 | 7.3 | 86.2 | 1.3 | 3.6 | 3.6 | 10.1 | 5.8 | 15.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco, L.; Nakano, E.Y.; Raposo, A.; Alturki, H.A.; Alarifi, S.N.; Chaves, C.; Teixeira-Lemos, E.; Romão, B. Eating Attitudes of Patients with Celiac Disease in Brazil: A Nationwide Assessment with the EAT-26 Instrument. Nutrients 2023, 15, 4796. https://doi.org/10.3390/nu15224796
Franco L, Nakano EY, Raposo A, Alturki HA, Alarifi SN, Chaves C, Teixeira-Lemos E, Romão B. Eating Attitudes of Patients with Celiac Disease in Brazil: A Nationwide Assessment with the EAT-26 Instrument. Nutrients. 2023; 15(22):4796. https://doi.org/10.3390/nu15224796
Chicago/Turabian StyleFranco, Luiza, Eduardo Yoshio Nakano, António Raposo, Hmidan A. Alturki, Sehad N. Alarifi, Cláudia Chaves, Edite Teixeira-Lemos, and Bernardo Romão. 2023. "Eating Attitudes of Patients with Celiac Disease in Brazil: A Nationwide Assessment with the EAT-26 Instrument" Nutrients 15, no. 22: 4796. https://doi.org/10.3390/nu15224796
APA StyleFranco, L., Nakano, E. Y., Raposo, A., Alturki, H. A., Alarifi, S. N., Chaves, C., Teixeira-Lemos, E., & Romão, B. (2023). Eating Attitudes of Patients with Celiac Disease in Brazil: A Nationwide Assessment with the EAT-26 Instrument. Nutrients, 15(22), 4796. https://doi.org/10.3390/nu15224796