

Chrono-Nutritional Patterns, Medical Comorbidities, and Psychological Status in Patients with Severe Obesity
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Multi-Disciplinary Assessment
2.1.1. Patients: Inclusion/Exclusion Criteria
2.1.2. Clinical Evaluation
2.1.3. Anthropometric Measurements
2.1.4. Biochemical Assessment
2.1.5. Nutritional Assessment
2.1.6. Psychometric Parameters
2.2. Statistical Analysis
2.2.1. Descriptive Analysis
2.2.2. Data Imputation
2.2.3. Chrono Nutrition Data—A Functional Data Analysis
2.2.4. Quantile and Logistic Regression
3. Results
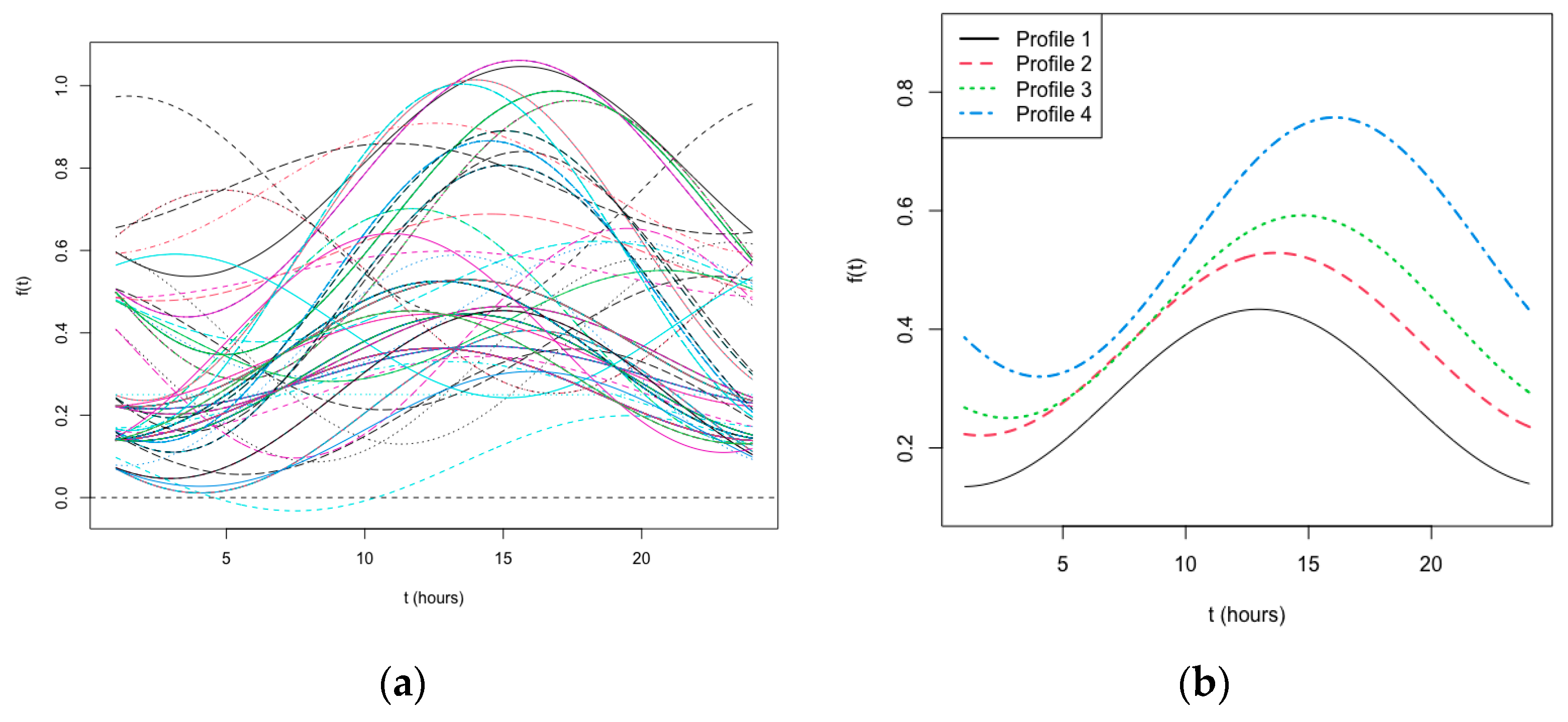
3.1. Chrono-Nutritional Profiling
3.2. Descriptive Analysis
3.3. Quantile and Logistic Regression Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 28 September 2023).
- Asher, G.; Schibler, U. Crosstalk between Components of Circadian and Metabolic Cycles in Mammals. Cell Metab. 2011, 13, 125–137. [Google Scholar] [CrossRef]
- Shi, S.; Ansari, T.S.; McGuinness, O.P.; Wasserman, D.H.; Johnson, C.H. Circadian Disruption Leads to Insulin Resistance and Obesity. Curr. Biol. 2013, 23, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Eckel-Mahan, K.; Sassone-Corsi, P. Metabolism and the Circadian Clock Converge. Physiol. Rev. 2013, 93, 107–135. [Google Scholar] [CrossRef] [PubMed]
- Baron, K.G.; Reid, K.J.; Kern, A.S.; Zee, P.C. Role of Sleep Timing in Caloric Intake and BMI. Obesity 2011, 19, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Asher, G.; Sassone-Corsi, P. Time for Food: The Intimate Interplay between Nutrition, Metabolism, and the Circadian Clock. Cell 2015, 161, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Parr, E.B.; Heilbronn, L.K.; Hawley, J.A. A Time to Eat and a Time to Exercise. Exerc. Sport Sci. Rev. 2020, 48, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Franzago, M.; Alessandrelli, E.; Notarangelo, S.; Stuppia, L.; Vitacolonna, E. Chrono-Nutrition: Circadian Rhythm and Personalized Nutrition. Int. J. Mol. Sci. 2023, 24, 2571. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, M.K. Chrononutrition—When We Eat Is of the Essence in Tackling Obesity. Nutrients 2022, 14, 5080. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S.; William, T. Friedewald.pdf. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Cooper, Z.; O’Connor, M. Eating Disorder Examination, 17.0D, ed. In Cognitive Behavior Therapy and Eating Disorders; The Guilford Press: New York, NY, USA, 2008; pp. 1–30. Available online: http://www.credo-oxford.com/pdfs/EDE_17.0D.pdf (accessed on 24 November 2023).
- Apolone, G.; Mosconi, P.; Ware, J.E. Questionario Sullo Stato Di Salute SF-36: Manuale D’uso e Guida All’interpretazione Dei Risultati; Guerini Ed Associati: Milan, Italy, 1997. [Google Scholar]
- Ware, J.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R. Symptom Checklist-90-Revised (SCL-90-R); NCS Pearson: Lyndhurst, OH, USA, 1979. [Google Scholar]
- Prunas, A.; Sarno, I.; Preti, E.; Madeddu, F.; Perugini, M. Psychometric properties of the Italian version of the SCL-90-R: A study on a large community sample. Eur. Psychiatry 2012, 27, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Dotti, A.; Lazzari, R. Validation and reliability of the Italian EAT-26. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 1998, 3, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Di Bernardo, M.; Barciulli, E.; Mannuccu, E.; Moretti, S.; Cabras, P.; Rotella, C.M. Validazione della versione italiana della Binge Eating Scale in pazienti obesi. Minerva Psichiatr. 1998, 39, 125–130. Available online: https://api.semanticscholar.org/CorpusID:151902125 (accessed on 24 November 2023).
- Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR); American Psychiatric Association: Arlington, TX, USA, 2000; Volume 1. [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef]
- Innamorati, M.; Imperatori, C.; Manzoni, G.M.; Lamis, D.A.; Castelnuovo, G.; Tamburello, A.; Tamburello, S.; Fabbricatore, M. Psychometric properties of the Italian Yale Food Addiction Scale in overweight and obese patients. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2015, 20, 119–127. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Rossi, A.; Pietrabissa, G.; Varallo, G.; Molinari, E.; Poggiogalle, E.; Donini, L.M.; Tarrini, G.; Melchionda, N.; Piccione, C.; et al. Validation of the Italian Yale Food Addiction Scale in postgraduate university students. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 167–176. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Fossati, A.; Di Ceglie, A.; Acquarini, E.; Barratt, E.S. Psychometric properties of an Italian version of the Barratt Impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J. Clin. Psychol. 2001, 57, 815–828. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Ramsay, J.O.; Silverman, B.W. Functional Data Analysis; Springer: New York, NY, USA, 2005. [Google Scholar] [CrossRef]
- Bouveyron, C.; Jacques, J. Model-based clustering of time series in group-specific functional subspaces. Adv. Data Anal. Classif. 2011, 5, 284–300. [Google Scholar] [CrossRef]
- Koenker, R.; Hallock, K.F. Quantile Regression. J. Econ. Perspect. 2001, 15, 143–156. [Google Scholar] [CrossRef]
- Sassaroli, S.; Ruggiero, G.M.; Vinai, P.; Cardetti, S.; Carpegna, G.; Ferrato, N.; Vallauri, P.; Masante, D.; Scarone, S.; Bertelli, S.; et al. Daily and Nightly Anxiety Among Patients Affected by Night Eating Syndrome and Binge Eating Disorder. Eat. Disord. 2009, 17, 140–145. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Aprano, S.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Pugliese, G.; Savastano, S.; Colao, A.; Opera Prevention Project. Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project. Nutrients 2020, 12, 1354. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Vetrani, C.; Altieri, B.; Verde, L.; Savastano, S.; Colao, A.; Muscogiuri, G. The Importance of Being a ‘Lark’ in Post-Menopausal Women with Obesity: A Ploy to Prevent Type 2 Diabetes Mellitus? Nutrients 2021, 13, 3762. [Google Scholar] [CrossRef]
- Sevinçer, G.M.; Konuk, N.; Bozkurt, S.; Coşkun, H. Food addiction and the outcome of bariatric surgery at 1-year: Prospective observational study. Psychiatry Res. 2016, 244, 159–164. [Google Scholar] [CrossRef]
- Pérez, F.G.; Sánchez-González, J.; Sánchez, I.; Jiménez-Murcia, S.; Granero, R.; Simó-Servat, A.; Ruiz, A.; Virgili, N.; López-Urdiales, R.; de Bernabe, M.M.-G.; et al. Food addiction and preoperative weight loss achievement in patients seeking bariatric surgery. Eur. Eat. Disord. Rev. 2018, 26, 645–656. [Google Scholar] [CrossRef]
- Canetti, L.; Berry, E.M.; Elizur, Y. Psychosocial predictors of weight loss and psychological adjustment following bariatric surgery and a weight-loss program: The mediating role of emotional eating. Int. J. Eat. Disord. 2009, 42, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Miller-Matero, L.R.; Bryce, K.; Saulino, C.K.; Dykhuis, K.E.; Genaw, J.; Carlin, A.M. Problematic Eating Behaviors Predict Outcomes After Bariatric Surgery. Obes. Surg. 2018, 28, 1910–1915. [Google Scholar] [CrossRef] [PubMed]
- Kinzl, J.; Schrattenecker, M.; Traweger, C.; Mattesich, M.; Fiala, M.; Biebl, W. Psychosocial Predictors of Weight Loss after Bariatric Surgery. Obes. Surg. 2006, 16, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Wedin, S.; Madan, A.; Correll, J.; Crowley, N.; Malcolm, R.; Byrne, T.K.; Borckardt, J.J. Emotional eating, marital status and history of physical abuse predict 2-year weight loss in weight loss surgery patients. Eat. Behav. 2014, 15, 619–624. [Google Scholar] [CrossRef]
- Koball, A.M.; Clark, M.M.; Collazo-Clavell, M.; Kellogg, T.; Ames, G.; Ebbert, J.; Grothe, K.B. The relationship among food addiction, negative mood, and eating-disordered behaviors in patients seeking to have bariatric surgery. Surg. Obes. Relat. Dis. 2016, 12, 165–170. [Google Scholar] [CrossRef]
- Testa, G.; Granero, R.; Siragusa, C.; Belligoli, A.; Sanna, M.; Rusconi, M.L.; Angeli, P.; Vettor, R.; Foletto, M.; Busetto, L.; et al. Psychological predictors of poor weight loss following LSG: Relevance of general psychopathology and impulsivity. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2020, 25, 1621–1629. [Google Scholar] [CrossRef]
- Assicurare La Salute E IL Benessere Per Tutti E Per Tutte le Età. Available online: https://www.istat.it/storage/rapporti-tematici/sdgs/2021/goal3.pdf (accessed on 10 October 2023).
- Olsen, A.; Møller, P.; Hausner, H. Early Origins of Overeating: Early Habit Formation and Implications for Obesity in Later Life. Curr. Obes. Rep. 2013, 2, 157–164. [Google Scholar] [CrossRef]


{kind=link}
| Chrono-Nutritional Profiles | ||||||
|---|---|---|---|---|---|---|
| Time of Food Contacts | Overall, N = 173 | 1, N = 80 1 | 2, N = 11 1 | 3, N = 55 1 | 4, N = 27 1 | p-Value 2 |
| Breakfast | 154 (89%) | 74 (92%) | 11 (100%) | 44 (80%) | 25 (93%) | 0.10 |
| Morning Nibbling | 17 (9.8%) | 0 (0%) | 0 (0%) | 8 (15%) | 9 (33%) | <0.001 |
| Morning Snack | 88 (51%) | 34 (42%) | 11 (100%) | 26 (47%) | 17 (63%) | 0.002 |
| Lunch | 168 (97%) | 80 (100%) | 11 (100%) | 52 (95%) | 25 (93%) | 0.067 |
| Afternoon Nibbling | 38 (22%) | 0 (0%) | 0 (0%) | 22 (40%) | 16 (59%) | <0.001 |
| Afternoon Snack | 108 (62%) | 44 (55%) | 11 (100%) | 32 (58%) | 21 (78%) | 0.005 |
| Dinner | 173 (100%) | 80 (100%) | 11 (100%) | 55 (100%) | 27 (100%) | - |
| Evening Nibbling | 25 (14%) | 0 (0%) | 0 (0%) | 7 (13%) | 18 (67%) | <0.001 |
| Evening Snack | 52 (30%) | 0 (0%) | 11 (100%) | 26 (47%) | 15 (56%) | <0.001 |
| Night Nibbling | 6 (3.5%) | 0 (0%) | 0 (0%) | 6 (11%) | 0 (0%) | 0.008 |
| Night Snack | 8 (4.6%) | 0 (0%) | 0 (0%) | 7 (13%) | 1 (3.7%) | 0.005 |
| Characteristics | Overall, N = 173 1 | BMI | p-Value 2 | ||
|---|---|---|---|---|---|
| [32.9, 40.2], N = 58 1 | (40.2, 46.2], N = 57 1 | (46.2, 80.3], N = 58 1 | |||
| Gender, Female | 117 (68%) | 46 (79%) | 40 (70%) | 31 (53%) | 0.011 |
| Age (years) | 46 (39, 54) | 48 (42, 55) | 48 (40, 54) | 42 (39, 52) | 0.11 |
| Educational level | 0.75 | ||||
| Middle school | 72 (42%) | 24 (41%) | 26 (46%) | 22 (38%) | |
| High school | 75 (43%) | 24 (41%) | 22 (39%) | 29 (50%) | |
| Degree or higher | 26 (15%) | 10 (17%) | 9 (16%) | 7 (12%) | |
| Physical activity | 29 (17%) | 10 (17%) | 12 (21%) | 7 (12%) | 0.43 |
| Alcohol consumption | 25 (14%) | 8 (14%) | 8 (14%) | 9 (16%) | 0.96 |
| Smoking habit | 33 (19%) | 11 (19%) | 6 (11%) | 16 (28%) | 0.067 |
| Shift work | 32 (18%) | 10 (17%) | 10 (18%) | 12 (21%) | 0.87 |
| Chrono-nutritional profile | 0.45 | ||||
| Profile 1 | 80 (46%) | 32 (55%) | 22 (39%) | 26 (45%) | |
| Profile 2 | 11 (6.4%) | 1 (1.7%) | 5 (8.8%) | 5 (8.6%) | |
| Profile 3 | 55 (32%) | 16 (28%) | 20 (35%) | 19 (33%) | |
| Profile 4 | 27 (16%) | 9 (16%) | 10 (18%) | 8 (14%) | |
| Overall, N = 173 1 | BMI | p-Value 2 | |||
|---|---|---|---|---|---|
| [32.9, 40.2], N = 58 1 | (40.2, 46.2], N = 57 1 | (46.2, 80.3], N = 58 1 | |||
| Hypertension | 76 (44%) | 28 (48%) | 25 (44%) | 23 (40%) | 0.65 |
| Diabetes | 0.16 | ||||
| No | 72 (42%) | 26 (45%) | 26 (46%) | 20 (34%) | |
| Pre-diabetes | 70 (40%) | 26 (45%) | 22 (39%) | 22 (38%) | |
| Yes | 31 (18%) | 6 (10%) | 9 (16%) | 16 (28%) | |
| Dyslipidemia | 101 (60%) | 28 (48%) | 33 (58%) | 40 (69%) | 0.077 |
| Use of Statins | 18 (10%) | 4 (6.9%) | 8 (14%) | 6 (10%) | 0.46 |
| CT (mmol/L) | 4.59 (4.06, 5.26) | 4.87 (4.36, 5.40) | 4.38 (4.01, 5.08) | 4.52 (3.93, 4.85) | 0.026 |
| HDL (mmol/L) | 1.17 (1.03, 1.41) | 1.33 (1.13, 1.68) | 1.14 (0.93, 1.34) | 1.11 (0.97, 1.29) | <0.001 |
| LDL (mmol/L) | 3.08 (2.51, 3.55) | 3.11 (2.67, 3.78) | 2.98 (2.49, 3.52) | 3.07 (2.52, 3.53) | 0.48 |
| TG (mmol/L) | 1.28 (0.93, 1.89) | 1.24 (0.86, 1.63) | 1.26 (0.91, 1.84) | 1.46 (1.14, 2.12) | 0.11 |
| HOMA | 4.0 (2.0, 6.4) | 2.5 (1.8, 4.3) | 4.1 (2.0, 5.8) | 5.9 (3.4, 9.4) | <0.001 |
| SCL90-R_GSI | 62 (50, 74) | 64 (51, 78) | 59 (49, 74) | 60 (50, 74) | 0.27 |
| SF36PH. | 52 (35, 71) | 43 (30, 62) | 60 (45, 76) | 54 (34, 70) | 0.008 |
| SF36 MH | 55 (39, 72) | 52 (31, 68) | 56 (41, 73) | 56 (44, 69) | 0.35 |
| Y-FAS score | 2 (1, 4) | 3 (2, 4) | 2 (1, 4) | 2 (1, 3) | 0.16 |
| EAT-26 score | 8 (3, 14) | 10 (5, 17) | 8 (4, 12) | 5 (2, 11) | 0.017 |
| BIS-11 score | 59 (53, 67) | 64 (57, 67) | 58 (53, 66) | 58 (52, 68) | 0.12 |
| BES score | 12 (6, 19) | 16 (7, 22) | 12 (6, 18) | 10 (4, 18) | 0.11 |
| Predictors | Hypertension | Dyslipidemia | Diabetes | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | OR | 95%CI | p | |
| (Intercept) | 0.01 | 0.00–0.06 | <0.001 | 0.77 | 0.49–1.21 | 0.265 | 0.01 | 0.00–0.10 | <0.001 |
| Age [+1 years] | 1.09 | 1.06–1.14 | <0.001 | 1.05 | 1.00–1.09 | 0.048 | |||
| Gender [Male] | 2.21 | 1.08–4.60 | 0.031 | 11.7 | 4.90–33.0 | <0.001 | 2.99 | 1.26–7.24 | 0.013 |
| Alcohol cons. [Yes] | 0.34 | 0.12–0.88 | 0.032 | ||||||
| Physical activity [Yes] | 2.07 | 0.83–5.43 | 0.127 | 0.31 | 0.05–1.20 | 0.139 | |||
| Smoking habit [Yes] | 0.48 | 0.19–1.16 | 0.108 | ||||||
| BMI cat. [41.2–46.2] | 1.61 | 0.51–5.39 | 0.425 | ||||||
| BMI cat. [47.2–80.3] | 3.12 | 1.07–10.1 | 0.044 | ||||||
| Predictors | HDL (mmol/L) | TG (mmol/L) | HOMA Index | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Est. | 95%CI | p | Est. | 95%CI | p | Est. | 95%CI | p | |
| (Intercept) | 1.15 | 0.89–1.41 | <0.001 | 0.44 | −0.08–0.96 | 0.097 | 2.31 | 1.82–2.80 | <0.001 |
| Age [+1 years] | 0.00 | −0.00–0.01 | 0.088 | 0.01 | 0.00–0.03 | 0.012 | |||
| Gender [Male] | −0.22 | −0.33–−0.11 | <0.001 | 1.86 | 0.59–3.12 | 0.005 | |||
| Smoking habit [Yes] | 0.14 | 0.02–0.27 | 0.026 | ||||||
| Alcohol consumption [Yes] | 0.16 | −0.15–0.47 | 0.299 | ||||||
| BMI cat. [41.2–46.2] | −0.16 | −0.32–−0.00 | 0.051 | 0.05 | −0.24–0.33 | 0.745 | 1.51 | 0.37–2.66 | 0.011 |
| BMI cat. [47.2–80.3] | −0.16 | −0.31–0.00 | 0.053 | 0.29 | −0.03–0.61 | 0.080 | 2.82 | 1.37–4.27 | <0.001 |
| Chrono-nutr Profile [2] | 0.01 | −1.03–1.05 | 0.989 | ||||||
| Chrono-nutr Profile [3] | 0.19 | −0.12–0.49 | 0.232 | ||||||
| Chrono-nutr Profile [4] | −0.10 | −0.44–0.23 | 0.551 | ||||||
| SF-36 Physical Health | SF-36 Mental Health | SCL-90-R_GSI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictors | Est. | 95%CI | p | Est. | 95%CI | p | Est. | 95%CI | p | |||
| (Intercept) | 69.37 | 50.98–87.75 | <0.001 | 60.07 | 48.42–71.71 | <0.001 | 65.45 | 57.07–73.82 | <0.001 | |||
| Gender [Male] | 8.47 | −2.61–19.56 | 0.136 | |||||||||
| Age [+1 years] | −0.60 | −0.93–−0.28 | <0.001 | |||||||||
| Educational level [High school] | 8.51 | 1.41–15.61 | 0.020 | |||||||||
| Educational level [Degree or high.] | 4.46 | −5.74–14.66 | 0.393 | |||||||||
| Physical Activity [Yes] | 6.15 | −1.32–13.61 | 0.109 | 8.33 | −2.67–19.34 | 0.140 | ||||||
| Alcohol cons. [Yes] | 9.59 | 3.48–15.69 | 0.002 | 6.60 | −7.30–20.50 | 0.353 | ||||||
| Smoking habit [Yes] | −11.77 | −22.52–−1.01 | 0.033 | 4.30 | −2.82–11.43 | 0.238 | ||||||
| BMI cat. [41.2–46.2] | 13.35 | 4.41–22.30 | 0.004 | −0.10 | −12.67–12.47 | 0.988 | −5.02 | −13.83–3.79 | 0.266 | |||
| BMI cat. [47.2–80.3] | 2.88 | −6.04–11.81 | 0.528 | 7.63 | −3.23–18.50 | 0.170 | −5.38 | −13.41–2.66 | 0.191 | |||
| Chrono-nutr Profile [2] | −1.27 | −9.22–6.69 | 0.756 | 0.90 | −15.32–17.12 | 0.914 | −6.81 | −17.90–4.28 | 0.230 | |||
| Chrono-nutr Profile [3] | −9.75 | −18.11–−1.40 | 0.023 | −12.87 | −24.36–−1.37 | 0.030 | 13.62 | 5.74–21.50 | 0.001 | |||
| Chrono-nutr Profile [4] | −12.40 | −23.82–−0.98 | 0.035 | −3.60 | −19.58–12.38 | 0.659 | 6.45 | −6.14–19.04 | 0.317 | |||
| Diabetes [Pre-diabetes] | 6.50 | −0.94–13.93 | 0.089 | −8.24 | −16.28–−0.21 | 0.046 | ||||||
| Diabetes [Yes] | 8.79 | −0.82–18.40 | 0.075 | −7.89 | −17.59–1.82 | 0.113 | ||||||
| Dyslipidemia [Yes] | −6.31 | −13.15–0.52 | 0.072 | −3.83 | −13.72–6.05 | 0.448 | ||||||
| Observations | 173 | 173 | 173 | |||||||||
| R2 | 0.156 | 0.008 | 0.140 | |||||||||
| EAT-26 | BIS-11 | BES | Y-FAS | |||||||||
| Predictors | Est. | 95%CI | p | Est. | 95%CI | p | Est. | 95%CI | p | Est. | 95%CI | p |
| (Intercept) | 7.00 | 4.81–9.19 | <0.001 | 61.00 | 57.66–64.34 | <0.001 | 19.83 | 12.56–27.10 | <0.001 | 2.00 | 1.39–2.61 | <0.001 |
| Gender [Male] | −3.33 | −5.82–−0.85 | 0.009 | 3.25 | −1.37–7.87 | 0.170 | ||||||
| Age [+1 years] | −0.13 | −0.27–0.02 | 0.083 | |||||||||
| Smoking habit [Yes] | 4.67 | 2.32–7.01 | <0.001 | |||||||||
| Alcohol cons. [Yes] | −1.00 | −1.73–−0.27 | 0.008 | |||||||||
| BMI cat [41.2–46.2] | −1.67 | −4.35–1.02 | 0.225 | −3.00 | −7.16–1.16 | 0.159 | −4.93 | −8.68–−1.17 | 0.011 | |||
| BMI cat [47.2–80.3] | −3.33 | −5.72–−0.94 | 0.007 | −5.50 | −9.05–−1.95 | 0.003 | −4.01 | −7.87–−0.14 | 0.044 | |||
| Chrono-nutr Profile [2] | 1.00 | −4.15–6.15 | 0.704 | 1.25 | −5.78–8.28 | 0.728 | 1.66 | −3.73–7.05 | 0.547 | 0.00 | −1.54–1.54 | 1.000 |
| Chrono-nutr Profile [3] | 2.67 | 0.33–5.00 | 0.027 | 4.00 | 0.53–7.47 | 0.025 | 5.48 | 2.10–8.87 | 0.002 | 1.00 | 0.15–1.85 | 0.023 |
| Chrono-nutr Profile [4] | 4.67 | 1.44–7.89 | 0.005 | 4.50 | −0.41–9.41 | 0.074 | 8.42 | 4.34–12.50 | <0.001 | 1.00 | −0.12–2.12 | 0.083 |
| Hypertension [Yes] | 1.67 | −0.78–4.11 | 0.183 | 3.25 | −0.22–6.72 | 0.068 | ||||||
| Dyslipidemia [Yes] | 2.00 | −0.50–4.50 | 0.119 | 1.94 | −1.27–5.16 | 0.237 | ||||||
| Physical Activity [Yes] | −3.75 | −7.09–−0.41 | 0.029 | −4.93 | −8.44–−1.42 | 0.007 | ||||||
| Diabetes [Pre-diabetes] | −2.75 | −5.99–0.49 | 0.099 | −2.93 | −6.29–0.43 | 0.089 | ||||||
| Diabetes [Yes] | −1.00 | −6.48–4.48 | 0.721 | −4.09 | −8.63–0.45 | 0.080 | ||||||
| Observations | 173 | 173 | 173 | 173 | ||||||||
| R2 | 0.123 | 0.091 | 0.141 | 0.007 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bettini, S.; Schiff, S.; Carraro, E.; Callegari, C.; Gusella, B.; Pontesilli, G.M.; D’Angelo, M.; Baldan, V.; Zattarin, A.; Romanelli, G.; et al. Chrono-Nutritional Patterns, Medical Comorbidities, and Psychological Status in Patients with Severe Obesity. Nutrients 2023, 15, 5003. https://doi.org/10.3390/nu15235003
Bettini S, Schiff S, Carraro E, Callegari C, Gusella B, Pontesilli GM, D’Angelo M, Baldan V, Zattarin A, Romanelli G, et al. Chrono-Nutritional Patterns, Medical Comorbidities, and Psychological Status in Patients with Severe Obesity. Nutrients. 2023; 15(23):5003. https://doi.org/10.3390/nu15235003
Chicago/Turabian StyleBettini, Silvia, Sami Schiff, Enrico Carraro, Chiara Callegari, Beatrice Gusella, Giulia Maria Pontesilli, Matteo D’Angelo, Valeria Baldan, Alessandra Zattarin, Giulia Romanelli, and et al. 2023. "Chrono-Nutritional Patterns, Medical Comorbidities, and Psychological Status in Patients with Severe Obesity" Nutrients 15, no. 23: 5003. https://doi.org/10.3390/nu15235003
APA StyleBettini, S., Schiff, S., Carraro, E., Callegari, C., Gusella, B., Pontesilli, G. M., D’Angelo, M., Baldan, V., Zattarin, A., Romanelli, G., Angeli, P., Girardi, P., Spinella, P., Vettor, R., & Busetto, L. (2023). Chrono-Nutritional Patterns, Medical Comorbidities, and Psychological Status in Patients with Severe Obesity. Nutrients, 15(23), 5003. https://doi.org/10.3390/nu15235003