
Effects of Glucomannan Supplementation on Type II Diabetes Mellitus in Humans: A Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Outcomes
2.4. Statistical Analysis and Quality Assessment
2.5. Risk of Publication Bias
3. Results
3.1. Subsection
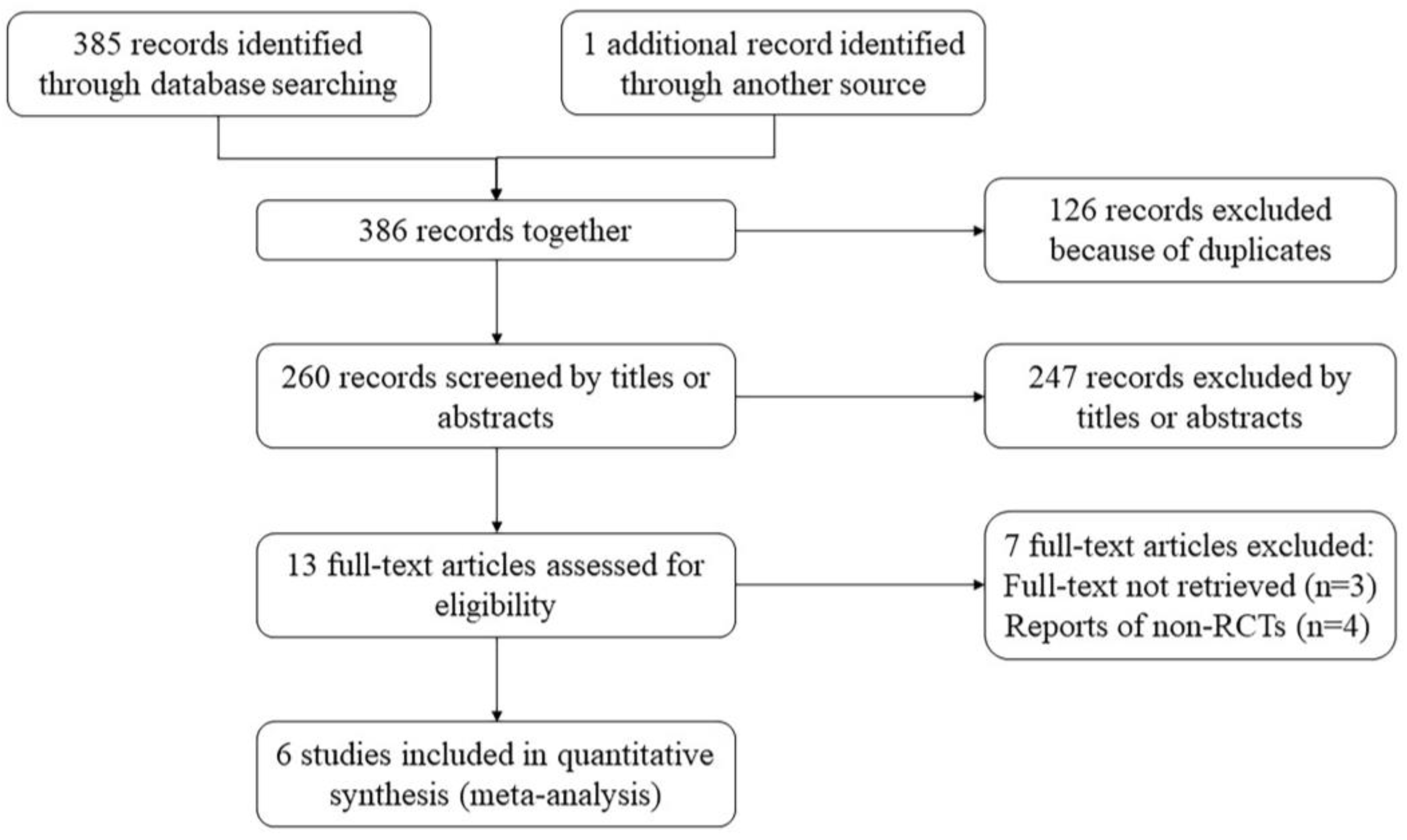
3.1.1. Search Results
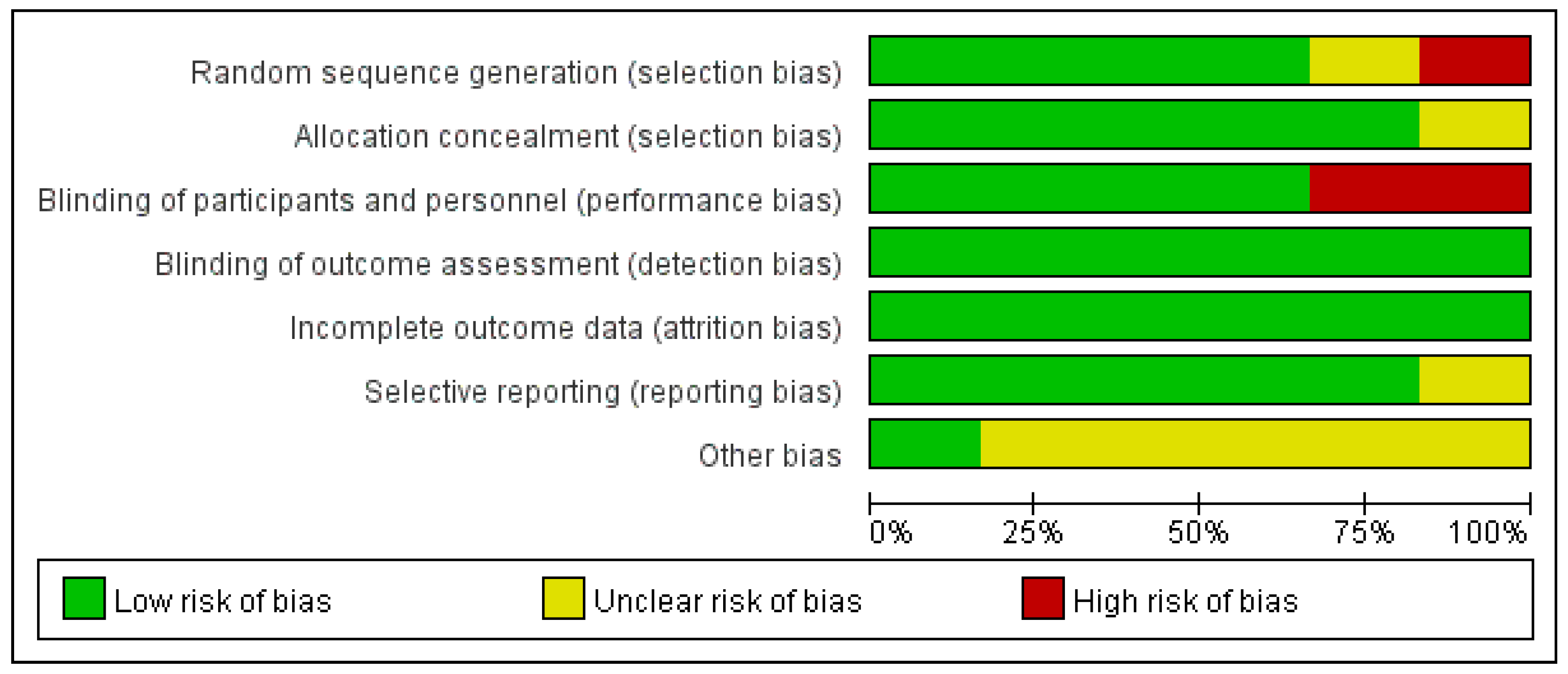
3.1.2. Study Characteristics and Quality Assessment
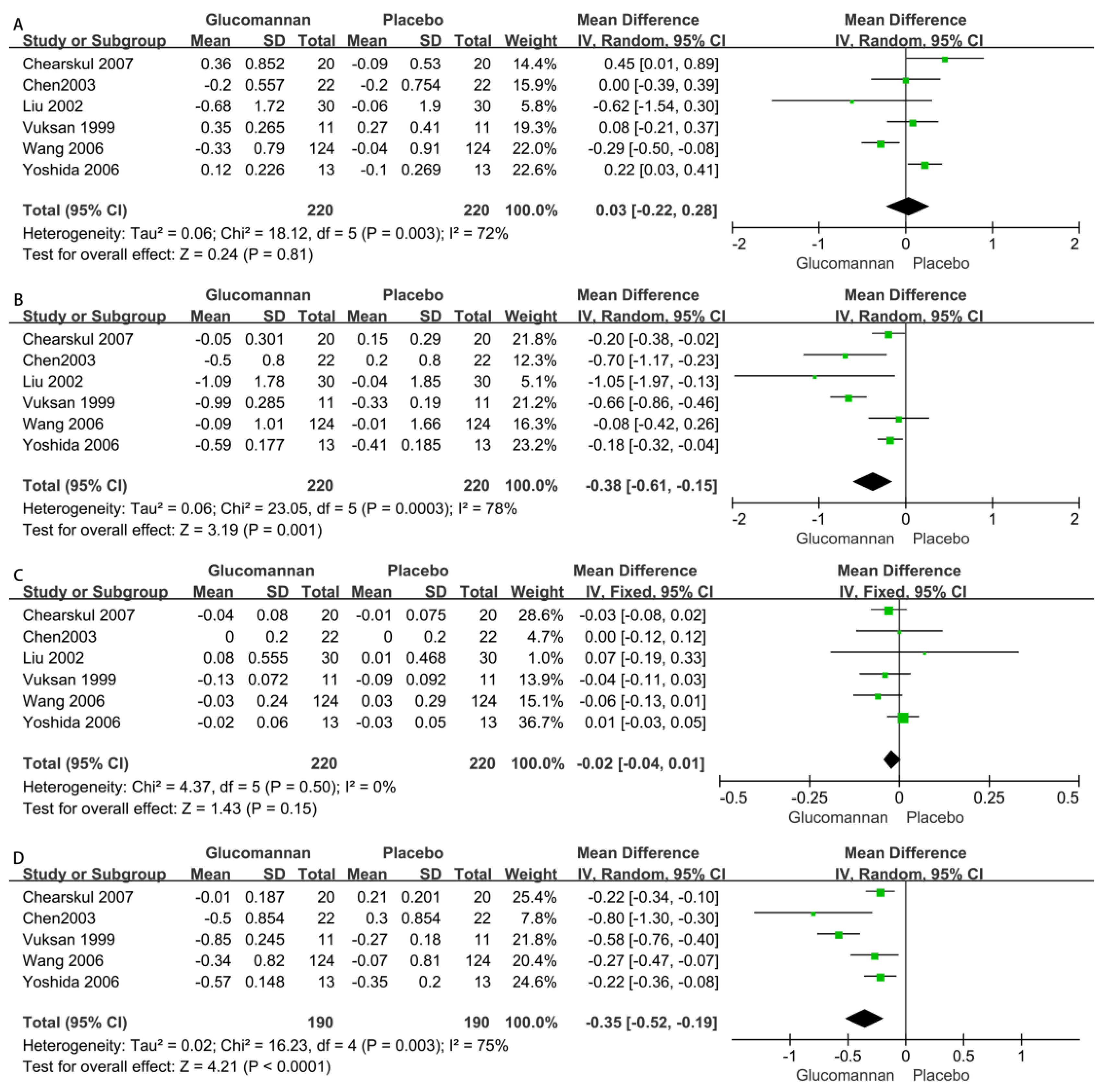
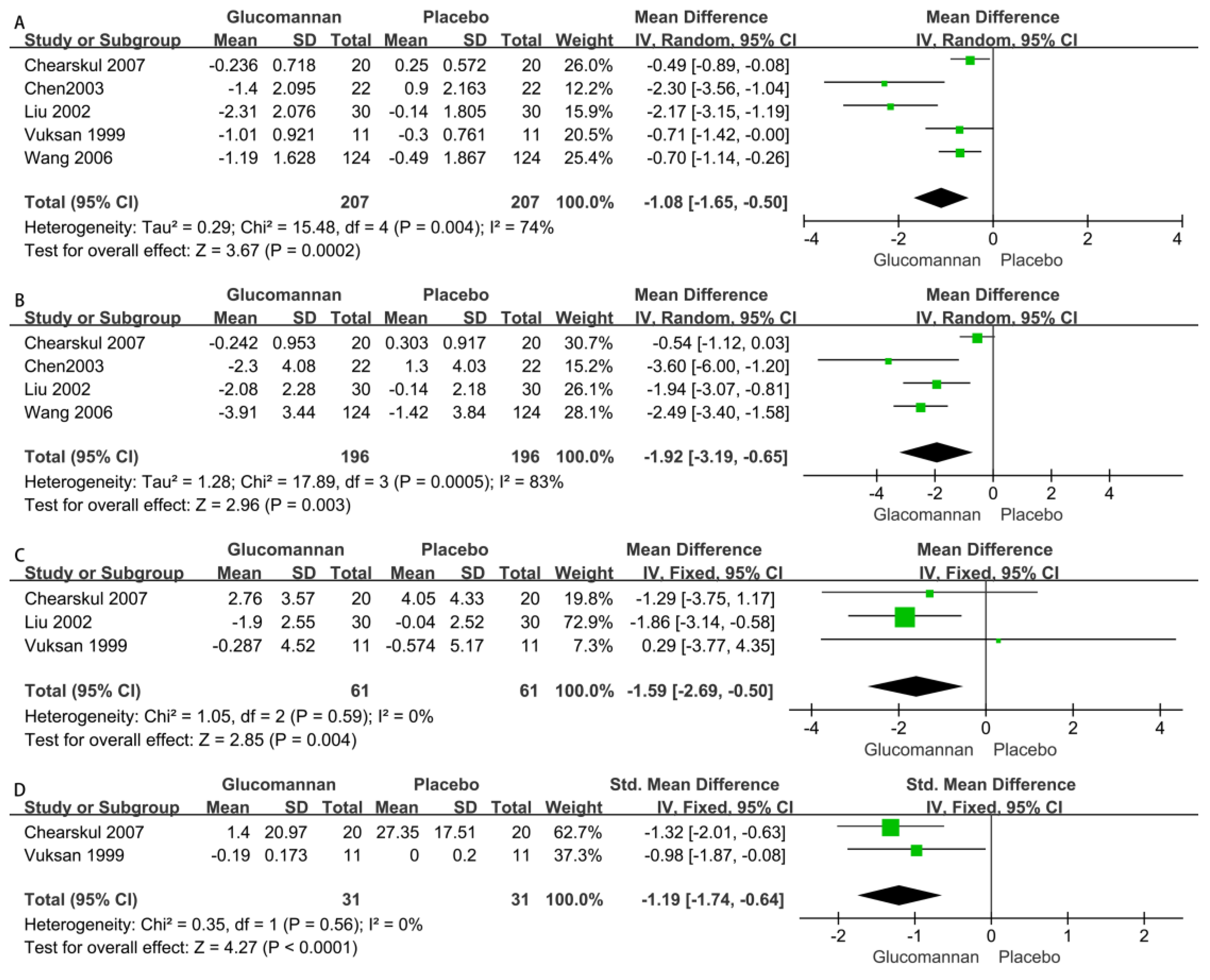
3.1.3. The Effect of Glucomannan on Blood Lipids
- 1.
- Triglyceride (TG)
- 2.
- Total Cholesterol (TC)
- 3.
- High-Density Lipoprotein (HDL)
- 4.
- Low-Density Lipoprotein (LDL)
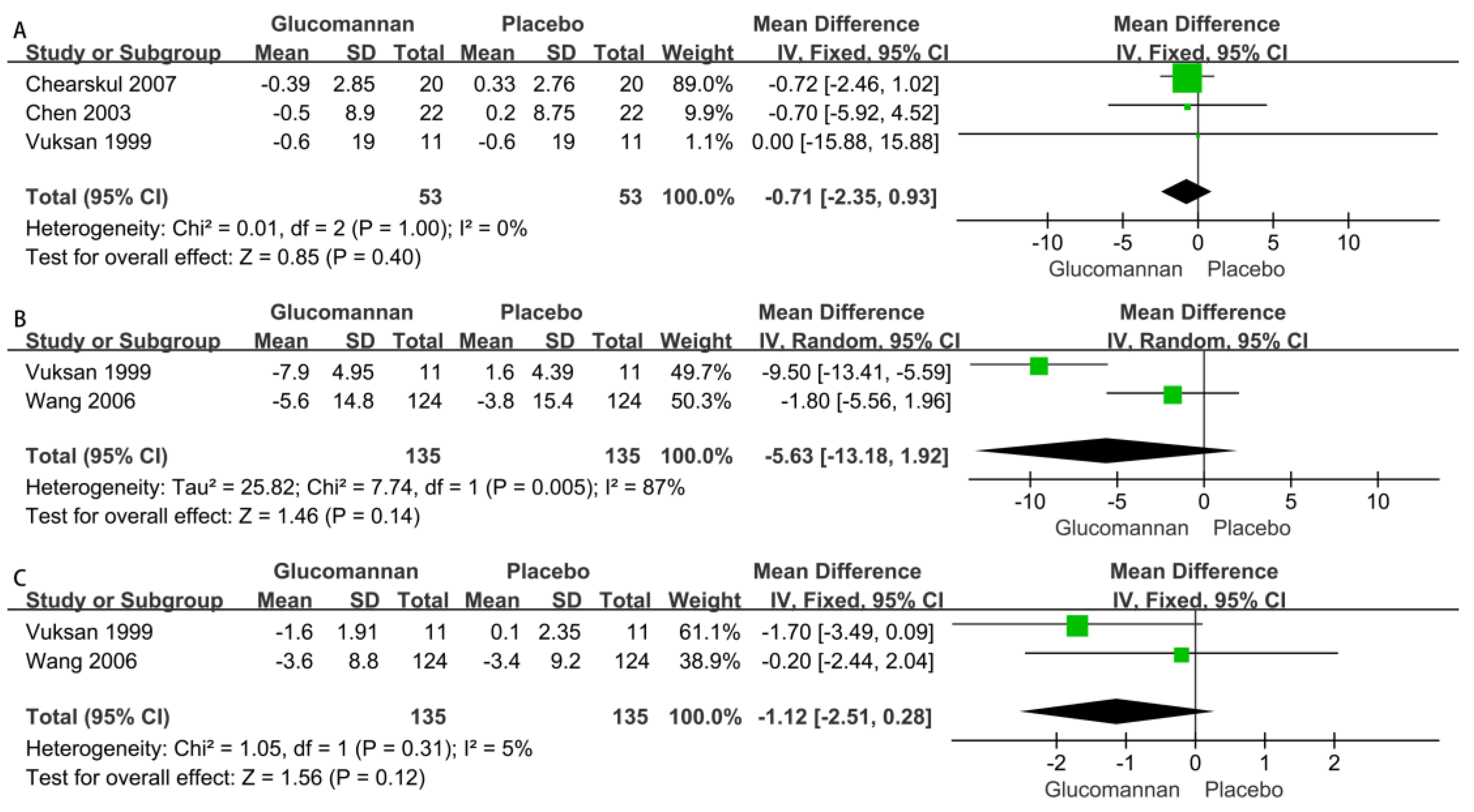
3.1.4. The Effect of Glucomannan on Glycemic Indices
- 1.
- Fasting Blood Glucose (FBG)
- 2.
- Two-hour Postprandial Blood Glucose (P2hBG)
- 3.
- Fasting Insulin (FINS)
- 4.
- Serum Fructosamine (SFRA)
3.1.5. The Effect on the Physical Examination Index
- 1.
- Body Weight (BW)
- 2.
- Systolic Blood Pressure (SBP)
- 3.
- Diastolic Blood Pressure (DBP)
3.1.6. Risk of Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, C.Y.; Zhou, J.; Long, F.; Zhang, W.; Shen, H.; Zhu, H.; Xu, J.D.; Li, S.L. Similar hypoglycemic effects of glucomannan and its enzyme degraded products from Amorphophallus albus on type 2 diabetes mellitus in mice and potential mechanisms. Food Funct. 2020, 11, 9740–9751. [Google Scholar] [CrossRef] [PubMed]
- Behera, S.S.; Ray, R.C. Konjac glucomannan, a promising polysaccharide of Amorphophallus konjac K. Koch in health care. Int. J. Biol. Macromol. 2016, 92, 942–956. [Google Scholar] [CrossRef] [PubMed]
- Lazaridou, A.; Chornick, T.; Biliaderis, C.G.; Izydorczyk, M.S. Sequential solvent extraction and structural characterization of polysaccharides from the endosperm cell walls of barley grown in different environments. Carbohydr. Polym. 2008, 73, 621–639. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Nishinari, K. Effect of degree of acetylation on gelation of konjac glucomannan. Biomacromolecules 2004, 5, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Laignier, F.; Akutsu, R.; Maldonade, I.R.; Bertoldo Pacheco, M.T.; Silva, V.S.N.; Mendonca, M.A.; Zandonadi, R.P.; Raposo, A.; Botelho, R.B.A. Amorphophallus konjac: A Novel Alternative Flour on Gluten-Free Bread. Foods 2021, 10, 1206. [Google Scholar] [CrossRef]
- Chen, J.; Liu, D.; Shi, B.; Wang, H.; Cheng, Y.; Zhang, W. Optimization of hydrolysis conditions for the production of glucomanno-oligosaccharides from konjac using β-mannanase by response surface methodology. Carbohydr. Polym. 2013, 93, 81–88. [Google Scholar] [CrossRef]
- Wu, W.T.; Chen, H.L. Effects of konjac glucomannan on putative risk factors for colon carcinogenesis in rats fed a high-fat diet. J. Agric. Food Chem. 2011, 59, 989–994. [Google Scholar] [CrossRef]
- Alves, A.; Miguel, S.P.; Araujo, A.; de Jesus Valle, M.J.; Sanchez Navarro, A.; Correia, I.J.; Ribeiro, M.P.; Coutinho, P. Xanthan Gum-Konjac Glucomannan Blend Hydrogel for Wound Healing. Polymers 2020, 12, 99. [Google Scholar] [CrossRef] [Green Version]
- Ren, W.-j.; Zhang, A.-q.; Qin, S.-y.; Li, Z.-k. Synthesis and evaluation of a novel cationic konjac glucomannan-based flocculant. Carbohydr. Polym. 2016, 144, 238–244. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, J.; Li, Q.; Wang, Y.; Wang, C. Two natural glucomannan polymers, from Konjac and Bletilla, as bioactive materials for pharmaceutical applications. Biotechnol. Lett. 2015, 37, 1–8. [Google Scholar] [CrossRef]
- Tester, R.F.; Al-Ghazzewi, F.H. Beneficial health characteristics of native and hydrolysed konjac (Amorphophallus konjac) glucomannan. J. Sci. Food Agric. 2016, 96, 3283–3291. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Effects of Two Different Dietary Patterns on Inflammatory Markers, Advanced Glycation End Products and Lipids in Subjects without Type 2 Diabetes: A Randomised Crossover Study. Nutrients 2017, 9, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, S.J.; La Gruta, N.L. A subset of immune-system T cells branded as seeds for type 1 diabetes. Nature 2022, 602, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Vanderniet, J.A.; Jenkins, A.J.; Donaghue, K.C. Epidemiology of Type 1 Diabetes. Curr. Cardiol. Rep. 2022, 24, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wang, Y.; Chen, S.; Gu, J.; Ni, Y. Insoluble and Soluble Dietary Fibers from Kiwifruit (Actinidia deliciosa) Modify Gut Microbiota to Alleviate High-Fat Diet and Streptozotocin-Induced TYPE 2 Diabetes in Rats. Nutrients 2022, 14, 3369. [Google Scholar] [CrossRef] [PubMed]
- Vuksan, V.; Sievenpiper, J.L.; Owen, R.; Swilley, J.A.; Spadafora, P.; Jenkins, D.J.; Vidgen, E.; Brighenti, F.; Josse, R.G.; Leiter, L.A.; et al. Beneficial effects of viscous dietary fiber from Konjac-mannan in subjects with the insulin resistance syndrome: Results of a controlled metabolic trial. Diabetes Care 2000, 23, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; Vuksan, V. Viscous fibers, health claims, and strategies to reduce cardiovascular disease risk. Am. J. Clin. Nutr. 2000, 71, 401–402. [Google Scholar] [CrossRef] [Green Version]
- Chua, M.; Baldwin, T.C.; Hocking, T.J.; Chan, K. Traditional uses and potential health benefits of Amorphophallus konjac K. Koch ex N.E.Br. J. Ethnopharmacol. 2010, 128, 268–278. [Google Scholar] [CrossRef]
- Ho, H.V.T.; Jovanovski, E.; Zurbau, A.; Blanco Mejia, S.; Sievenpiper, J.L.; Au-Yeung, F.; Jenkins, A.L.; Duvnjak, L.; Leiter, L.; Vuksan, V. A systematic review and meta-analysis of randomized controlled trials of the effect of konjac glucomannan, a viscous soluble fiber, on LDL cholesterol and the new lipid targets non-HDL cholesterol and apolipoprotein B. Am. J. Clin. Nutr. 2017, 105, 1239–1247. [Google Scholar] [CrossRef] [Green Version]
- Vuksan, V.; Jenkins, D.J.; Spadafora, P.; Sievenpiper, J.L.; Owen, R.; Vidgen, E.; Brighenti, F.; Josse, R.; Leiter, L.A.; Bruce-Thompson, C. Konjac-mannan (glucomannan) improves glycemia and other associated risk factors for coronary heart disease in type 2 diabetes. A randomized controlled metabolic trial. Diabetes Care 1999, 22, 913–919. [Google Scholar] [CrossRef]
- Liu, Y.M.; Yin, X.Q.; Li, X.S.; Li, R.H.; Zhang, J.C. Clinical observation of glucomannan in the treatment of type 2 diabetes. Chin. J. Prim. Med. Pharm. 2002, 9, 76. [Google Scholar]
- Chen, H.L.; Sheu, W.H.; Tai, T.S.; Liaw, Y.P.; Chen, Y.C. Konjac supplement alleviated hypercholesterolemia and hyperglycemia in type 2 diabetic subjects--a randomized double-blind trial. J. Am. Coll. Nutr. 2003, 22, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Chen, Y.N.; Huang, B.X. Analysis of curative effect of glucomannan on type 2 diabetes. J. Community Med. 2006, 4, 12–14. [Google Scholar]
- Yoshida, M.; Vanstone, C.A.; Parsons, W.D.; Zawistowski, J.; Jones, P.J.H. Effect of plant sterols and glucomannan on lipids in individuals with and without type II diabetes. Eur. J. Clin. Nutr. 2006, 60, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Chearskul, S.; Sangurai, S.; Nitiyanant, W.; Kriengsinyos, W.; Kooptiwut, S.; Harindhanavudhi, T. Glycemic and lipid responses to glucomannan in Thais with type 2 diabetes mellitus. Med. J. Med. Assoc. Thail. 2007, 90, 2150–2157. [Google Scholar]
- Lyons, T.J.; Basu, A. Biomarkers in diabetes: Hemoglobin A1c, vascular and tissue markers. Transl. Res. J. Lab. Clin. Med. 2012, 159, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Nie, Q.; Hu, J.; Huang, X.; Zhang, K.; Nie, S. Glucomannans Alleviated the Progression of Diabetic Kidney Disease by Improving Kidney Metabolic Disturbance. Mol. Nutr. Food Res. 2019, 63, e1801008. [Google Scholar] [CrossRef]
- Cohen, R.M.; Sacks, D.B. Comparing multiple measures of glycemia: How to transition from biomarker to diagnostic test? Clin. Chem. 2012, 58, 1615–1617. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Wang, Y.; He, W.; Xie, B. Studies on the antidiabetic effect of konjac glucomannan with different molecular chains on experimental diabetes mice. Zhong Yao Cai 2004, 27, 110–113. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Malmström, H.; Walldius, G.; Grill, V.; Jungner, I.; Gudbjörnsdottir, S.; Hammar, N. Fructosamine is a useful indicator of hyperglycaemia and glucose control in clinical and epidemiological studies--cross-sectional and longitudinal experience from the AMORIS cohort. PLoS ONE 2014, 9, e111463. [Google Scholar] [CrossRef]
- Koroskenyi, B.; McCarthy, S.P. Synthesis of acetylated konjac glucomannan and effect of degree of acetylation on water absorbency. Biomacromolecules 2001, 2, 824–826. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, L.; Liu, X.Q.; Zhao, Z.J.; Lv, L.X. Effect of glucomannan on functional constipation in children: A systematic review and meta-analysis of randomised controlled trials. Asia Pac. J. Clin. Nutr. 2017, 26, 471–477. [Google Scholar] [CrossRef]
- Hayeeawaema, F.; Wichienchot, S.; Khuituan, P. Amelioration of gut dysbiosis and gastrointestinal motility by konjac oligo-glucomannan on loperamide-induced constipation in mice. Nutrition 2020, 73, 110715. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, K.; Nakamura, S.; Moriyama-Hashiguchi, M.; Kitajima, M.; Ejima, H.; Imori, C.; Oku, T. Dietary Fructooligosaccharide and Glucomannan Alter Gut Microbiota and Improve Bone Metabolism in Senescence-Accelerated Mouse. J. Agric. Food Chem. 2019, 67, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Yu, Z.; Zhang, Z.; Liang, X.; Gong, P.; Yi, H.; Yang, L.; Liu, T.; Shi, H.; Zhang, L. Bifidobacterium animalis F1–7 in combination with konjac glucomannan improves constipation in mice via humoral transport. Food Funct. 2021, 12, 791–801. [Google Scholar] [CrossRef]
- Chang, X.Y.; Liu, Y.Y.; Hu, M.M.; Liu, Y.Q.; Jiang, C.H.; Wang, Q.; Jin, Q.M.; Zhang, D.J.; Yin, Z.Q.; Zhang, J. Comparative effects of different enzymatic hydrolysates of konjac glucomannan on gut flora and constipation in rats. Food Funct. 2022, 13, 8717–8729. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year (Reference) | Location | Cases | Controls | Age | Gender, Males | Dose | Duration | Comparator | Energy Balance |
|---|---|---|---|---|---|---|---|---|---|
| Vuksan, 1999 [20] | Canada | 11 | 11 | 60.4 ± 7.53 | 45.5% | 0.7 g/100 kcal | 16 weeks | Wheat bran | Isocaloric |
| Liu, 2002 [21] | China | 30 | 30 | 52.1 ± 4.89 | 43.3% | 6 g/d | 1 month | Placebo | Isocaloric |
| Chen, 2003 [22] | Taiwan | 22 | 22 | 64.2 ± 8.3 | 45.5% | 1.2–3.6 g/d | 4 weeks | Placebo | Isocaloric |
| Wang, 2006 [23] | China | 124 | 124 | 57.7 ± 9.16 | 43.0% | 15 g/d | 12 weeks | Placebo | Isocaloric |
| Yoshida, 2006 [24] | Canada | 13 | 13 | 56.8 ± 10.8 | 30.8% | 10 g/d | 3 weeks | Placebo | Isocaloric |
| Chearskul, 2007 [25] | Thailand | 20 | 20 | 51.2 ± 2.21 | 50.0% | 3 g/d | 4 weeks | Placebo | Isocaloric |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Zhang, Y.; Tao, X.; Wang, Y.; Rao, B.; Shi, H. Effects of Glucomannan Supplementation on Type II Diabetes Mellitus in Humans: A Meta-Analysis. Nutrients 2023, 15, 601. https://doi.org/10.3390/nu15030601
Zhang Z, Zhang Y, Tao X, Wang Y, Rao B, Shi H. Effects of Glucomannan Supplementation on Type II Diabetes Mellitus in Humans: A Meta-Analysis. Nutrients. 2023; 15(3):601. https://doi.org/10.3390/nu15030601
Chicago/Turabian StyleZhang, Zhanzhi, Yu Zhang, Xiaomei Tao, Yuying Wang, Benqiang Rao, and Hanping Shi. 2023. "Effects of Glucomannan Supplementation on Type II Diabetes Mellitus in Humans: A Meta-Analysis" Nutrients 15, no. 3: 601. https://doi.org/10.3390/nu15030601
APA StyleZhang, Z., Zhang, Y., Tao, X., Wang, Y., Rao, B., & Shi, H. (2023). Effects of Glucomannan Supplementation on Type II Diabetes Mellitus in Humans: A Meta-Analysis. Nutrients, 15(3), 601. https://doi.org/10.3390/nu15030601