
Pilot Study of the Applicability, Usability, and Accuracy of the Nutricate© Online Application, a New Dietary Intake Assessment Tool for Managing Infant Cow’s Milk Allergy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Participants’ Anthropometric Characteristics
2.3. Nutricate© Software
2.4. Nutricate© Web Application: Usability Metrics
2.5. 24-Hour Recall Questionnaire as a Reference
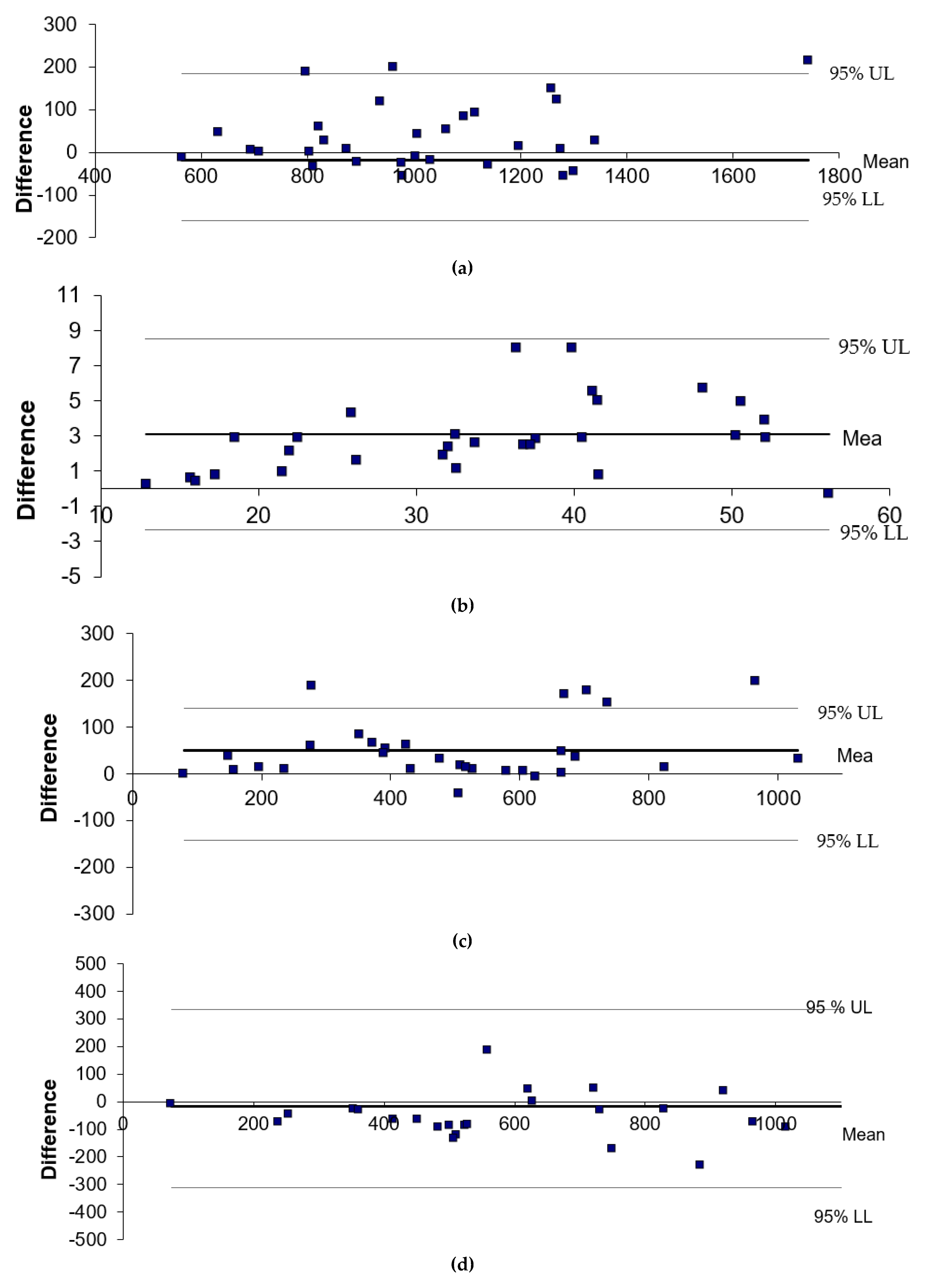
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agostoni, C.; Terracciano, L.; Varin, E.; Fiocchi, A. The Nutritional Value of Protein-hydrolyzed Formulae. Crit. Rev. Food Sci. Nutr. 2016, 56, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Tamazouzt, S.; Adel-Patient, K.; Deschildre, A.; Roduit, C.; Charles, M.A.; de Lauzon-Guillain, B.; Divaret-Chauveau, A. Prevalence of Food Allergy in France up to 5.5 Years of Age: Results from the ELFE Cohort. Nutrients 2022, 14, 3624. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Schunemann, H.J.; Brozek, J.; Restani, P.; Beyer, K.; Troncone, R.; Martelli, A.; Terracciano, L.; Bahna, S.L.; Rencé, F.; et al. Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA): A summary report. J. Allergy Clin. Immunol. 2010, 126, U1119–U1197. [Google Scholar] [CrossRef] [PubMed]
- Giannetti, A.; Vespasiani, G.T.; Ricci, G.; Miniaci, A.; di Palmo, E.; Pession, A. Cow’s Milk Protein Allergy as a Model of Food Allergies. Nutrients 2021, 13, 1525. [Google Scholar] [CrossRef] [PubMed]
- Luyt, D.; Ball, H.; Makwana, N.; Green, M.R.; Bravin, K.; Nasser, S.M.; Clark, A.T. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin. Exp. Allergy 2014, 44, 642–672. [Google Scholar] [CrossRef]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef]
- Meyer, R.; Venter, C.; Fox, A.T.; Shah, N. Practical dietary management of protein energy malnutrition in young children with cow’s milk protein allergy. Pediatr. Allergy Immunol. 2012, 23, 307–314. [Google Scholar] [CrossRef]
- Mehta, H.; Groetch, M.; Wang, J. Growth and nutritional concerns in children with food allergy. Curr. Opin. Allergy Clin. Immunol. 2013, 13, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Isolauri, E.; Sutas, Y.; Salo, M.K.; Isosomppi, R.; Kaila, M. Elimination diet in cow’s milk allergy: Risk for impaired growth in young children. J. Pediatr. 1998, 132, 1004–1009. [Google Scholar] [CrossRef]
- Ludman, S.; Shah, N.; Fox, A.T. Managing cows’ milk allergy in children. BMJ 2013, 347, f5424. [Google Scholar] [CrossRef] [Green Version]
- Muraro, A.; de Silva, D.; Halken, S.; Worm, M.; Khaleva, E.; Arasi, S.; Dunn-Galvin, A.; Nwaru, B.I.; De Jong, N.W.; Del Río, P.R.; et al. Managing food allergy: GA(2)LEN guideline 2022. World Allergy Organ. J. 2022, 15, 100687. [Google Scholar] [CrossRef] [PubMed]
- Cawood, A.L.; Meyer, R.; Grimshaw, K.E.; Sorensen, K.; Acosta-Mena, D.; Stratton, R.J. The health economic impact of cow’s milk allergy in childhood: A retrospective cohort study. Clin. Transl. Allergy 2022, 12, e12187. [Google Scholar] [CrossRef] [PubMed]
- Fong, A.T.; Ahlstedt, S.; Golding, M.A.; Protudjer, J.L.P. The Economic Burden of Food Allergy: What We Know and What We Need to Learn. Curr. Treat. Options Allergy 2022, 9, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; Meyer, R.; Grimshaw, K.E.; Cawood, A.L.; Acosta-Mena, D.; Stratton, R.J. The clinical burden of cow’s milk allergy in early childhood: A retrospective cohort study. Immun. Inflamm. Dis. 2022, 10, e572. [Google Scholar] [CrossRef]
- Warren, C.M.; Agrawal, A.; Gandhi, D.; Gupta, R.S. The US population-level burden of cow’s milk allergy. World Allergy Organ. J. 2022, 15, 100644. [Google Scholar] [CrossRef]
- Subar, A.F.; Crafts, J.; Zimmerman, T.P.; Wilson, M.; Mittl, B.; Islam, N.G.; McNutt, S.; Potischman, N.; Buday, R.; Hull, S.G.; et al. Assessment of the Accuracy of Portion Size Reports Using Computer-Based Food Photographs Aids in the Development of an Automated Self-Administered 24-Hour Recall. J. Am. Diet. Assoc. 2010, 110, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, L.A.; Erickson, D.J.; Toomey, T.L.; Wagenaar, A.C. Handheld computers—A feasible alternative to paper forms for field data collection. Eval. Rev. 2003, 27, 165–178. [Google Scholar] [CrossRef]
- Slimani, N.; Casagrande, C.; Nicolas, G.; Freisling, H.; Huybrechts, I.; Ocké, M.C.; Niekerk, E.M.; Van Rossum, C.; Bellemans, M.; De Maeyer, M.; et al. The standardized computerized 24-h dietary recall method EPIC-Soft adapted for pan-European dietary monitoring. Eur. J. Clin. Nutr. 2011, 65, S5–S15. [Google Scholar] [CrossRef] [Green Version]
- Jensen, V.B.; Jorgensen, I.M.; Rasmussen, K.B.; Molgaard, C.; Prahl, P. Bone mineral status in children with cow milk allergy. Pediatr. Allergy Immunol. 2004, 15, 562–565. [Google Scholar] [CrossRef]
- Paganus, A.; Juntunenbackman, K.; Savilahti, E. Follow-Up of Nutritional-Status and Dietary Survey in Children With Cows Milk Allergy. Acta Paediatr. 1992, 81, 518–521. [Google Scholar] [CrossRef]
- Deplanque, D.; Sénéchal-Cohen, S.; Lemaire, F. French Jardé’s law and European regulation on drug trials: Harmonization and implementation of new rules. Therapie 2017, 72, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Purnell, J.Q. Definitions, Classification, and Epidemiology of Obesity. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Myatt, M.; Guevarra, E. Zscorer: An Anthropometric Z-Score Calculator, R package version 0.3.1.; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Evenepoel, C.; Clevers, E.; Deroover, L.; Van Loo, W.; Matthys, C.; Verbeke, K. Accuracy of Nutrient Calculations Using the Consumer-Focused Online App MyFitnessPal: Validation Study. J. Med. Internet Res. 2020, 22, e18237. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Covents, M.; Matthys, C.; Maes, L. Young adolescents’ nutrition assessment on computer (YANA-C). Eur. J. Clin. Nutr. 2005, 59, 658–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 4th ed.; Coulston, A., Boushey, C., Ferruzzi, M., Eds.; Academic Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Hercberg, S.; Deheeger, M.; Preziosi, P. Portions Alimentaires Manuel Photos Pour L’estimation des Quantités; Economica: London, UK, 2002. [Google Scholar]
- Patel, S.; Vyas, A.; Custovic, A.; Murray, C.S. Estimated portion sizes in a school-aged population. Public Health Nutr. 2012, 15, 2193–2201. [Google Scholar] [CrossRef] [Green Version]
- Volatier, J. Enquête INCA Individuelle et Nationale sur les Consommations Alimentaires; CRÉDOC—AFSSA—Ministère de L’agriculture et de la Pêche: Paris, France, 2000. [Google Scholar]
- Brooke, J. SUS-aquick and dirty usability scale. In Usability Evaluation In Industry; Jordan, P.W., Thomas, B., McClelland, I.L., Weerdmeester, B., Eds.; CRC Press: Boca Raton, FL, USA, 1996; pp. 4–7. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the System Usability Scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Nutrilog. Database; Nutrilog: Marans, France, 2016. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Boaventura, R.M.; Mendonca, R.B.; Fonseca, F.A.; Mallozi, M.; Souza, F.S.; Sarni, R.O.S. Nutritional status and food intake of children with cow’s milk allergy. Allergol. Immunopathol. 2019, 47, 544–550. [Google Scholar] [CrossRef]
- Baranowski, T.; Islam, N.; Baranowski, J.; Cullen, K.W.; Myres, D.; Marsh, T.; de Moor, C. The Food Intake Recording Software System is valid among fourth-grade children. J. Am. Diet. Assoc. 2002, 102, 380–385. [Google Scholar] [CrossRef]
- Lombard, M.J.; Steyn, N.P.; Charlton, K.E.; Senekal, M. Application and interpretation of multiple statistical tests to evaluate validity of dietary intake assessment methods. Nutr. J. 2015, 14, 40. [Google Scholar] [CrossRef] [Green Version]
- Phillips, A.C.; Mackintosh, S.F.; Gibbs, C.; Ng, L.; Fryer, C.E. A comparison of electronic and paper-based clinical skills assessment: Systematic review. Med. Teach. 2019, 41, 1151–1159. [Google Scholar] [CrossRef]
- Flammarion, S.; Santos, C.; Guimber, D.; Jouannic, L.; Thumerelle, C.; Gottrand, F.; Deschildre, A. Diet and nutritional status of children with food allergies. Pediatr. Allergy Immunol. 2011, 22, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Gibson, K.; Stanley, S.; Agarwal, S.; Groetch, M.; Bunyavanich, S. Comparison of dietary intake between milk-allergic and non-food-allergic children. Pediatr. Allergy Immunol. 2021, 32, 1872–1876. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, C.; Eggesbo, M.; Halvorsen, R.; Botten, G. Nutrient intake among two-year-old children on cows’ milk-restricted diets. Acta Paediatr. 2000, 89, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Jung, C. L’alimentation de Nourrisson et du Petit Enfant; UNICEF: Florence, Italy, 2015; Volume 12, 4p. [Google Scholar]
- Timon, C.M.; Blain, R.J.; McNulty, B.; Kehoe, L.; Evans, K.; Walton, J.; Flynn, A.; Gibney, E.R. The Development, Validation, and User Evaluation of Foodbook24: A Web-Based Dietary Assessment Tool Developed for the Irish Adult Population. J. Med. Internet Res. 2017, 19, e158. [Google Scholar] [CrossRef] [Green Version]
- Motwalli, O.; Essack, M.; Salhi, A.; Hanks, J.; Mijakovic, I.; Bajic, V.B. Online dietary intake assessment using a graphical food frequency app (eNutri): Usability metrics from the EatWellUK study. PLoS ONE 2018, 13, e0202006. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD |
|---|---|
| Anthropometrics | |
| Gender M/F | 13/12 |
| Age (years) | 6.6 ± 1.6 |
| Weight (kg) | 23.8 ± 8.6 |
| Height (cm) | 122.2 ± 10.8 |
| Z-score weight-for-age | −0.40 ± 1.00 |
| Z-score height-for-age | −0.71 ± 1.43 |
| Z-score BMI-for-age | −0.05 ± 1.30 |
| Other allergies and symptoms | n |
| Other food allergies * | 5/4/1/1 |
| Asthma symptoms | 9 |
| Atopic dermatitis | 7 |
| Intake Calculation | |||||
|---|---|---|---|---|---|
| Results | |||||
| Food & Beverages | Quantity (G or mL) | Energy (kcal) | Proteins (g) | Calcium (mg) | Iron Absorbed (mg) |
| Bread (mean) | 20 g | 55 | 2 | 6 | 0.0080 |
| Meats (mean with fish, egg, ham) | 20 g | 30 | 5 | 3 | 0.0660 |
| Pasta, rice, semolina (cooked) | 70 g | 90 | 3 | 11 | 0.0112 |
| oil | 3 mL | 27 | 0 | 0 | 0.0000 |
| Vegetables raw/cooked | 50 g | 16 | 1 | 10 | 0.0050 |
| Desert with soy, flavored, enriched with ca | 90 g | 86 | 3 | 108 | 0.0347 |
| Biscuts (dry sweet) | 2 g | 9 | 0 | 1 | 0.0011 |
| Bread (mean) | 50 g | 138 | 5 | 16 | 0.0200 |
| Raw fruit, compote, and fruit puree | 100 g | 62 | 1 | 14 | 0.0060 |
| Desert with soy, flavored, enriched with ca | 90 g | 86 | 3 | 108 | 0.0347 |
| Meats (mean with fish, egg, ham) | 20 g | 30 | 5 | 3 | 0.0660 |
| Margarine (non-light, unsalted) | 5 g | 32 | 0 | 0 | 0.0018 |
| Potatoes | 80 g | 64 | 1 | 5 | 0.0080 |
| Sweet drinks, fruit juices | 90 mL | 33 | 0 | 5 | 0.0036 |
| Total | 758 | 29 | 290 | 0.2661 | |
| Beverage Categories | Mean ± SD |
|---|---|
| (g/Day) | |
| Hydrolyzed formula | 347.17 ± 263.35 |
| Vegetable beverage * | 200.36 ± 128.88 |
| Fruit juices | 98.89 ± 70.79 |
| Water ** | 256.67 ± 333.82 |
| Food Categories | Mean ± SD |
|---|---|
| (g/Day) | |
| Cereals * | 130.71 ± 89.36 |
| Bread | 40.88 ± 33.08 |
| Breakfast cereals | 25.00 ± 12.15 |
| Infant Cereal supplements | 12.00 ± 8.64 |
| Biscuits | 28.67 ± 21.95 |
| Potatoes | 72.08 ± 28.56 |
| Vegetables | 128.75 ± 89.80 |
| Meat | 65.08 ± 36.25 |
| Oils | 8.53 ± 6.28 |
| Fruits | 223.17 ± 86.05 |
| Jam/Free sugar | 12.43 ± 5.29 |
| Black chocolate | 14.14 ± 7.54 |
| Categories | R Coefficient | p |
|---|---|---|
| Energy Proteins Calcium Iron | 0.631 0.978 0.957 0.914 | 0.0001 0.0001 0.0001 0.0001 |
| Usability Item | |||
|---|---|---|---|
| Time duration for data entry | Not time-consuming (TC) 66.7% | Moderately TC 25% | Too TC 8.3% |
| Assessment of quantity for data entry | Very easy 66.7% | Moderately easy 25% | Not easy 8.3% |
| Usefulness of portion size for data entry | Very useful 83.3% | Moderately useful 25% | Not useful 0% |
| Categories | Intake | Percentage (%) |
|---|---|---|
| Energy Proteins Calcium Iron | 1038.8 ± 269.0 kcal/d 35.6 ± 12.8 g/d 527.1 ± 243.3 mg/d 709.1 ± 395.7 µg/d | 88.5 ± 26.2 264.3 ± 76.8 87.4 ± 41.0 91.5 ± 53.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzano, P.; Samier, L.; Lachaux, A.; Truc, F.V.; Béghin, L. Pilot Study of the Applicability, Usability, and Accuracy of the Nutricate© Online Application, a New Dietary Intake Assessment Tool for Managing Infant Cow’s Milk Allergy. Nutrients 2023, 15, 1045. https://doi.org/10.3390/nu15041045
Azzano P, Samier L, Lachaux A, Truc FV, Béghin L. Pilot Study of the Applicability, Usability, and Accuracy of the Nutricate© Online Application, a New Dietary Intake Assessment Tool for Managing Infant Cow’s Milk Allergy. Nutrients. 2023; 15(4):1045. https://doi.org/10.3390/nu15041045
Chicago/Turabian StyleAzzano, Pauline, Line Samier, Alain Lachaux, Florence Villard Truc, and Laurent Béghin. 2023. "Pilot Study of the Applicability, Usability, and Accuracy of the Nutricate© Online Application, a New Dietary Intake Assessment Tool for Managing Infant Cow’s Milk Allergy" Nutrients 15, no. 4: 1045. https://doi.org/10.3390/nu15041045
APA StyleAzzano, P., Samier, L., Lachaux, A., Truc, F. V., & Béghin, L. (2023). Pilot Study of the Applicability, Usability, and Accuracy of the Nutricate© Online Application, a New Dietary Intake Assessment Tool for Managing Infant Cow’s Milk Allergy. Nutrients, 15(4), 1045. https://doi.org/10.3390/nu15041045