
Nutrients and Dementia: Prospective Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Assessment of Nutrients
2.3. Sociodemographic and Lifestyle Measurements as Covariates
2.4. Statistical Data Analysis
3. Results
3.1. Basic Baseline Data
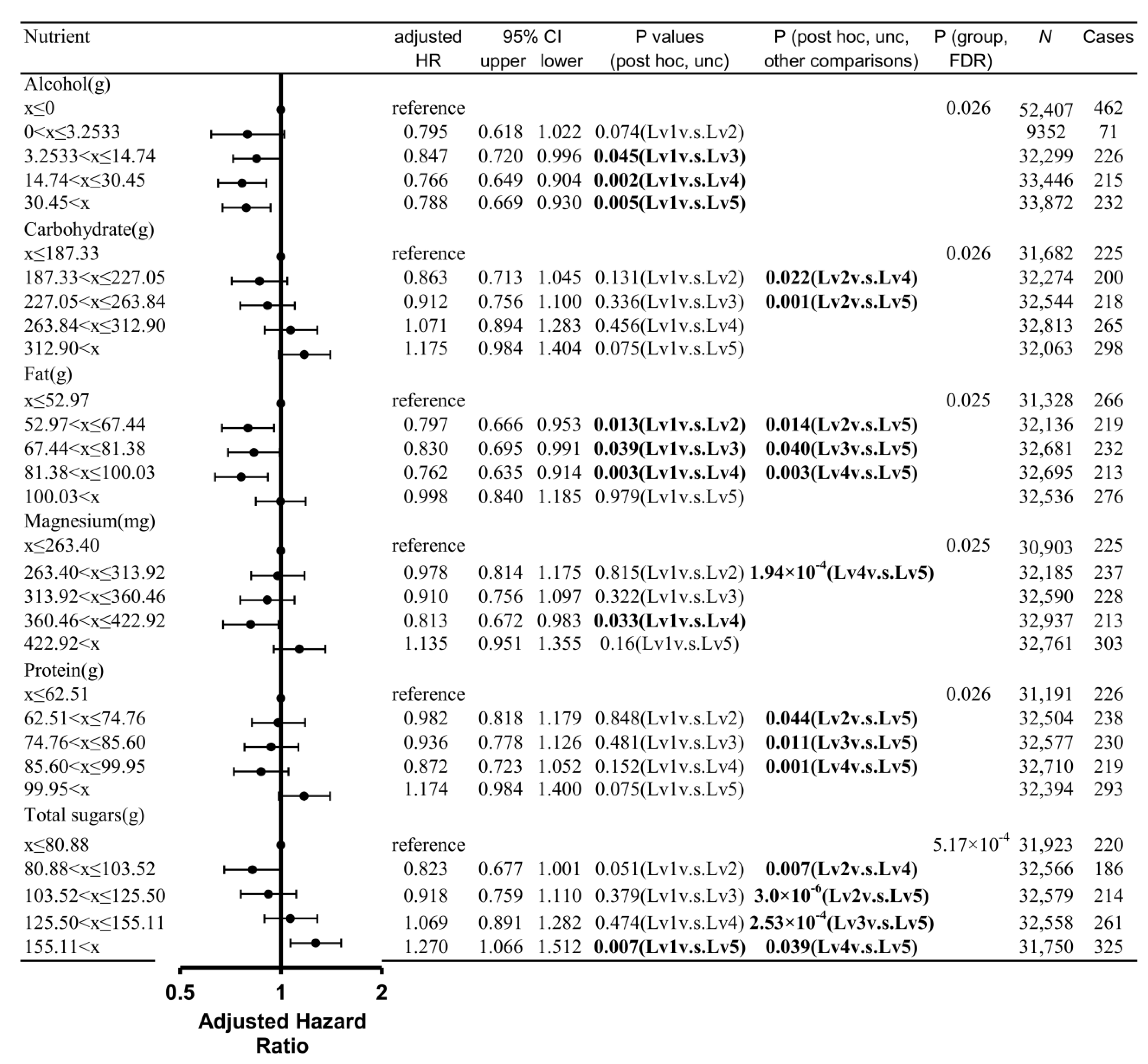
3.2. Prospective Dementia Analysis
3.3. Sensitivity Analyses Controlling for Energy Intake Quintiles
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cao, L.; Tan, L.; Wang, H.-F.; Jiang, T.; Zhu, X.-C.; Lu, H.; Tan, M.-S.; Yu, J.-T. Dietary patterns and risk of dementia: A systematic review and meta-analysis of cohort studies. Mol. Neurobiol. 2016, 53, 6144–6154. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Sun, Y.; Ji, M.; Li, X.; Wang, Z. Association of Vitamin B Status With Risk of Dementia in Cohort Studies: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2022, 23, 1826.e21–1826.e35. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Han, X.; Zhang, H.; Liu, J.; Zhang, M.; Zhao, W.; Jiang, S.; Li, R.; Cai, H.; You, H. Association of vitamin E intake in diet and supplements with risk of dementia: A meta-analysis. Front. Aging Neurosci. 2022, 14, 955878. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; Dugravot, A.; Akbaraly, T.; Britton, A.; Kivimäki, M.; Singh-Manoux, A. Alcohol consumption and risk of dementia: 23 year follow-up of Whitehall II cohort study. BMJ 2018, 362, k2927. [Google Scholar] [CrossRef]
- Wang, W.; Li, J.; Zhang, H.; Wang, X.; Zhang, X. Effects of vitamin E supplementation on the risk and progression of AD: A systematic review and meta-analysis. Nutr. Neurosci. 2021, 24, 13–22. [Google Scholar] [CrossRef]
- Stephan, B.; Wells, J.; Brayne, C.; Albanese, E.; Siervo, M. Increased fructose intake as a risk factor for dementia. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2010, 65, 809–814. [Google Scholar] [CrossRef]
- Lo, K.; Liu, Q.; Madsen, T.; Rapp, S.; Chen, J.-C.; Neuhouser, M.; Shadyab, A.; Pal, L.; Lin, X.; Shumaker, S. Relations of magnesium intake to cognitive impairment and dementia among participants in the Women’s Health Initiative Memory Study: A prospective cohort study. BMJ Open 2019, 9, e030052. [Google Scholar] [CrossRef]
- Ozawa, M.; Ninomiya, T.; Ohara, T.; Hirakawa, Y.; Doi, Y.; Hata, J.; Uchida, K.; Shirota, T.; Kitazono, T.; Kiyohara, Y. Self-Reported Dietary Intake of Potassium, Calcium, and Magnesium and Risk of Dementia in the J apanese: The H isayama Study. J. Am. Geriatr. Soc. 2012, 60. [Google Scholar]
- Roberts, R.O.; Roberts, L.A.; Geda, Y.E.; Cha, R.H.; Pankratz, V.S.; O’Connor, H.M.; Knopman, D.S.; Petersen, R.C. Relative intake of macronutrients impacts risk of mild cognitive impairment or dementia. J. Alzheimer’s Dis. 2012, 32, 329–339. [Google Scholar] [CrossRef]
- Takeuchi, H.; Kawashima, R. Effects of Body Mass Index on Brain Structures in the Elderly: Longitudinal Analyses. Front. Endocrinol. 2022, 13, 824661. [Google Scholar] [CrossRef]
- Albanese, E.; Launer, L.J.; Egger, M.; Prince, M.J.; Giannakopoulos, P.; Wolters, F.J.; Egan, K. Body mass index in midlife and dementia: Systematic review and meta-regression analysis of 589,649 men and women followed in longitudinal studies. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2017, 8, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Qizilbash, N.; Gregson, J.; Johnson, M.E.; Pearce, N.; Douglas, I.; Wing, K.; Evans, S.J.; Pocock, S.J. BMI and risk of dementia in two million people over two decades: A retrospective cohort study. Lancet Diabetes Endocrinol. 2015, 3, 431–436. [Google Scholar] [CrossRef]
- Kivimäki, M.; Singh-Manoux, A.; Shipley, M.J.; Elbaz, A. Does midlife obesity really lower dementia risk? Lancet Diabetes Endocrinol. 2015, 3, 498. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Kawashima, R. Diet and Dementia: A Prospective Study. Nutrients 2021, 13, 4500. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Young, H.; Crowe, F.L.; Benson, V.S.; Spencer, E.A.; Key, T.J.; Appleby, P.N.; Beral, V. Development and evaluation of the Oxford WebQ, a low-cost, web-based method for assessment of previous 24 h dietary intakes in large-scale prospective studies. Public Health Nutr. 2011, 14, 1998–2005. [Google Scholar] [CrossRef]
- Russ, T.C.; Kivimäki, M.; Starr, J.M.; Stamatakis, E.; Batty, G.D. Height in relation to dementia death: Individual participant meta-analysis of 18 UK prospective cohort studies. Br. J. Psychiatry 2014, 205, 348–354. [Google Scholar] [CrossRef]
- Lourida, I.; Hannon, E.; Littlejohns, T.J.; Langa, K.M.; Hyppönen, E.; Kuźma, E.; Llewellyn, D.J. Association of lifestyle and genetic risk with incidence of dementia. JAMA 2019, 322, 430–437. [Google Scholar] [CrossRef]
- Luojus, M.K.; Lehto, S.M.; Tolmunen, T.; Brem, A.-K.; Lönnroos, E.; Kauhanen, J. Self-reported sleep disturbance and incidence of dementia in ageing men. J. Epidemiol. Community Health 2017, 71, 329–335. [Google Scholar] [CrossRef]
- Benjamini, Y.; Krieger, A.M.; Yekutieli, D. Adaptive linear step-up procedures that control the false discovery rate. Biometrika 2006, 93, 491–507. [Google Scholar] [CrossRef]
- Wei, C.; Zhao, Z.; Li, B.; Sha, F. Alcohol consumption and risk of dementia: 11-year follow-up of UK Biobank cohort study. Alzheimer’s Dement. 2021, 17, e057753. [Google Scholar] [CrossRef]
- Juang, C.-L.; Yang, F.S.; Hsieh, M.S.; Tseng, H.-Y.; Chen, S.-C.; Wen, H.-C. Investigation of anti-oxidative stress in vitro and water apparent diffusion coefficient in MRI on rat after spinal cord injury in vivo with Tithonia diversifolia ethanolic extracts treatment. BMC Complement. Altern. Med. 2014, 14, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomassen, J.Q.; Tolstrup, J.S.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Frikke-Schmidt, R. Plasma Concentrations of Magnesium and Risk of Dementia: A General Population Study of 102 648 Individuals. Clin. Chem. 2021, 67, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Hynd, M.R.; Scott, H.L.; Dodd, P.R. Glutamate-mediated excitotoxicity and neurodegeneration in Alzheimer’s disease. Neurochem. Int. 2004, 45, 583–595. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.G.; Danysz, W.; Quack, G. Glutamate in CNS disorders as a target for drug development: An update. Drug News Perspect. 1998, 11, 523–569. [Google Scholar] [CrossRef]
- Simental-Mendia, L.E.; Sahebkar, A.; Rodriguez-Moran, M.; Guerrero-Romero, F. A systematic review and meta-analysis of randomized controlled trials on the effects of magnesium supplementation on insulin sensitivity and glucose control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef]
- Zheng, F.; Zhang, Y.; Xie, W.; Li, W.; Jin, C.; Mi, W.; Wang, F.; Ma, W.; Ma, C.; Yang, Y. Further evidence for genetic association of CACNA1C and schizophrenia: New risk loci in a Han Chinese population and a meta-analysis. Schizophr. Res. 2014, 152, 105–110. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in aging, health and diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef]
- Mazur, A.; Maier, J.A.; Rock, E.; Gueux, E.; Nowacki, W.; Rayssiguier, Y. Magnesium and the inflammatory response: Potential physiopathological implications. Arch. Biochem. Biophys. 2007, 458, 48–56. [Google Scholar] [CrossRef]
- Weglicki, W.; Mak, I.; Kramer, J.; Dickens, B.; Cassidy, M.; Stafford, R.; Phillips, T. Role of free radicals and substance P in magnesium deficiency. Cardiovasc. Res. 1996, 31, 677–682. [Google Scholar] [CrossRef]
- Tohidi, M.; Ghasemi, A.; Hadaegh, F.; Arbabi, S.; Hosseini Isfahani, F. Intra-erythrocyte magnesium is associated with gamma-glutamyl transferase in obese children and adolescents. Biol. Trace Elem. Res. 2011, 143, 835–843. [Google Scholar] [CrossRef]
- Weglicki, W.; Bloom, S.; Cassidy, M.; Freedman, A.; Atrakchi, A.; Dickens, B. Antioxidants and the cardiomyopathy of Mg-deficiency. Am. J. Cardiovasc. Pathol. 1992, 4, 210–215. [Google Scholar] [PubMed]
- Miao, H.; Chen, K.; Yan, X.; Chen, F. Sugar in Beverage and the Risk of Incident Dementia, Alzheimer’s disease and Stroke: A Prospective Cohort Study. J. Prev. Alzheimer’s Dis. 2021, 8, 188–193. [Google Scholar] [CrossRef]
- Orr, M.E.; Salinas, A.; Buffenstein, R.; Oddo, S. Mammalian target of rapamycin hyperactivity mediates the detrimental effects of a high sucrose diet on Alzheimer’s disease pathology. Neurobiol. Aging 2014, 35, 1233–1242. [Google Scholar] [CrossRef]
- Beilharz, J.E.; Maniam, J.; Morris, M.J. Diet-induced cognitive deficits: The role of fat and sugar, potential mechanisms and nutritional interventions. Nutrients 2015, 7, 6719–6738. [Google Scholar] [CrossRef]
- Chait, A.; Bornfeldt, K.E. Diabetes and atherosclerosis: Is there a role for hyperglycemia? J. Lipid Res. 2009, 50, S335–S339. [Google Scholar] [CrossRef] [PubMed]
- Leão, L.L.; Tangen, G.; Barca, M.L.; Engedal, K.; Santos, S.H.S.; Machado, F.S.M.; de Paula, A.M.B.; Monteiro-Junior, R.S. Does hyperglycemia downregulate glucose transporters in the brain? Med. Hypotheses 2020, 139, 109614. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.M.; Irish, M.; Kam, J.; Van Keizerswaard, J.; Bartley, L.; Samaras, K.; Hodges, J.R.; Piguet, O. Quantifying the eating abnormalities in frontotemporal dementia. JAMA Neurol. 2014, 71, 1540–1546. [Google Scholar] [CrossRef]
- Ruan, Y.; Tang, J.; Guo, X.; Li, K.; Li, D. Dietary fat intake and risk of Alzheimer’s disease and dementia: A meta-analysis of cohort studies. Curr. Alzheimer Res. 2018, 15, 869–876. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, J.; Qiu, J.; Li, Y.; Wang, J.; Jiao, J. Intakes of fish and polyunsaturated fatty acids and mild-to-severe cognitive impairment risks: A dose-response meta-analysis of 21 cohort studies–3. Am. J. Clin. Nutr. 2015, 103, 330–340. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Rimm, E.B. Fish intake, contaminants, and human health: Evaluating the risks and the benefits. JAMA 2006, 296, 1885–1899. [Google Scholar] [CrossRef]
- Wu, S.; Ding, Y.; Wu, F.; Li, R.; Hou, J.; Mao, P. Omega-3 fatty acids intake and risks of dementia and Alzheimer’s disease: A meta-analysis. Neurosci. Biobehav. Rev. 2015, 48, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Brockman, J.; Schneider, J.A.; Wang, Y.; Bennett, D.A.; Tangney, C.C.; van de Rest, O. Association of seafood consumption, brain mercury level, and APOE ε4 status with brain neuropathology in older adults. JAMA 2016, 315, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Kouvari, M.; Tyrovolas, S.; Panagiotakos, D.B. Red meat consumption and healthy ageing: A review. Maturitas 2016, 84, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Bateman, R.J.; Xiong, C.; Benzinger, T.L.; Fagan, A.M.; Goate, A.; Fox, N.C.; Marcus, D.S.; Cairns, N.J.; Xie, X.; Blazey, T.M. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 2012, 367, 795–804. [Google Scholar] [CrossRef]
- Batty, G.D.; Mcintosh, A.M.; Russ, T.C.; Deary, I.J.; Gale, C.R. Psychological distress, neuroticism, and cause-specific mortality: Early prospective evidence from UK Biobank. J. Epidemiol. Community Health 2016, 70, 1136–1139. [Google Scholar] [CrossRef]
- Cullen, B.; Newby, D.; Lee, D.; Lyall, D.M.; Nevado-Holgado, A.J.; Evans, J.J.; Pell, J.P.; Lovestone, S.; Cavanagh, J. Cross-sectional and longitudinal analyses of outdoor air pollution exposure and cognitive function in UK Biobank. Sci. Rep. 2018, 8, 1–14. [Google Scholar] [CrossRef]
- Khubchandani, J.; Brey, R.; Kotecki, J.; Kleinfelder, J.; Anderson, J. The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Arch. Psychiatr. Nurs. 2016, 30, 457–462. [Google Scholar] [CrossRef]
- Okbay, A.; Beauchamp, J.P.; Fontana, M.A.; Lee, J.J.; Pers, T.H.; Rietveld, C.A.; Turley, P.; Chen, G.B.; Emilsson, V.; Meddens, S.F.; et al. Genome-wide association study identifies 74 loci associated with educational attainment. Nature 2016, 533, 539–542. [Google Scholar] [CrossRef]
- Sarkar, S.N.; Huang, R.-Q.; Logan, S.M.; Yi, K.D.; Dillon, G.H.; Simpkins, J.W. Estrogens directly potentiate neuronal L-type Ca2+ channels. Proc. Natl. Acad. Sci. USA 2008, 105, 15148–15153. [Google Scholar] [CrossRef]
- Shen, X.; Cox, S.R.; Adams, M.J.; Howard, D.M.; Lawrie, S.M.; Ritchie, S.J.; Bastin, M.E.; Deary, I.J.; Mcintosh, A.M.; Whalley, H.C. Resting-state connectivity and its association with cognitive performance, educational attainment, and household income in the UK Biobank. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 878–886. [Google Scholar] [CrossRef]
- Townsend, P. Deprivation. J. Soc. Policy 1987, 16, 125–146. [Google Scholar] [CrossRef]
- Veldsman, M.; Kindalova, P.; Husain, M.; Kosmidis, I.; Nichols, T.E. Spatial distribution and cognitive impact of cerebrovascular risk-related white matter hyperintensities. NeuroImage: Clin. 2020, 28, 102405. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No Incident Dementia (n = 160,170) | Incident Dementia (n = 1206) | |
|---|---|---|
| Mean | ||
| Age | 58.51 (8.01) | 66.27 (5.19) |
| Townsend deprivation index | −1.62 (2.84) | −1.48 (2.94) |
| Education length | 15.49 (4.79) | 14.3 (5.07) |
| MET * | 30.27 (32.04) | 32.1 (36.08) |
| Height | 169.66 (9.17) | 169.48 (9.13) |
| Depression score | 5.42 (1.87) | 5.47 (1.94) |
| Visuospatial memory (errors) | 3.5 (2.36) | 3.93 (2.5) |
| Number | ||
| Male number | 74,596 (46.6%) | 699 (58%) |
| Household income | ||
| (a) Less than £18,000 | 22,864 (14.3%) | 359 (29.8%) |
| (b) £18,000 to £30,999 | 37,766 (23.6%) | 404 (33.5%) |
| (c) £31,000 to £5,1999 | 46,066 (28.8%) | 266 (22.1%) |
| (d) £52,000 to £100,000 | 41,033 (25.6%) | 140 (11.6%) |
| (e) Greater than £100,000 | 12,441 (7.8%) | 37 (3.1%) |
| Currently employed | 102,800 (64.2%) | 337 (27.9%) |
| BMI | ||
| Underweight (x ≤ 18.5) | 819 (0.5%) | 10 (0.8%) |
| Normal (18.5 < x ≤ 25) | 59,474 (37.1%) | 409 (33.9%) |
| Overweight (25 < x ≤ 30) | 66,943 (41.8%) | 476 (39.5%) |
| Obesity (x < 30) | 32,934 (20.6%) | 311 (25.8%) |
| Household number | ||
| (a) 1 | 28,380 (17.7%) | 281 (23.3%) |
| (b) 2 | 73,416 (45.8%) | 754 (62.5%) |
| (c) 3 | 25,180 (15.7%) | 101 (8.4%) |
| (d) 4≤ | 33,194 (20.7%) | 70 (5.8%) |
| Overall health (4 levels) | ||
| (a) Poor | 4326 (2.7%) | 88 (7.3%) |
| (b) Fair | 26,009 (16.2%) | 287 (23.8%) |
| (c) Good | 95,771 (59.8%) | 673 (55.8%) |
| (d) Excellent | 34,064 (21.3%) | 158 (13.1%) |
| Sleep duration | ||
| (a) ≤4 h, | 911 (0.6%) | 11 (0.9%) |
| (b) 5 h or 6 h, | 34,352 (21.4%) | 266 (22.1%) |
| (c) 7 h or 8 h, | 114,998 (71.8%) | 816 (67.7%) |
| (d) 9 h≤ | 9909 (6.2%) | 113 (9.4%) |
| Current smoking level (3 levels) | ||
| (a) No | 147,642 (92.2%) | 1111 (92.1%) |
| (b) Only occasionally | 4021 (2.5%) | 29 (2.4%) |
| (c) On most or all days | 8507 (5.3%) | 66 (5.5%) |
| Diastolic BP | ||
| x < 65 | 5626 (3.5%) | 47 (3.9%) |
| 65 ≤ x < 90 | 121,089 (75.6%) | 918 (76.1%) |
| 90 ≤ 30 | 33,455 (20.9%) | 241 (20%) |
| Ethnicity (non-white) | 5631 (3.5%) | 19 (1.6%) |
| Antihypertensive drug intake | 27,627 (17.2%) | 431 (35.7%) |
| Statin intake | 15,590 (9.7%) | 239 (19.8%) |
| Diabetes | 6159 (3.8%) | 120 (10%) |
| Heart attack | 2535 (1.6%) | 59 (4.9%) |
| Angina | 3270 (2%) | 95 (7.9%) |
| Stroke | 1589 (1%) | 52 (4.3%) |
| Cancer | 12,781 (8%) | 128 (10.6%) |
| Other serious medical conditions | 31,084 (19.4%) | 408 (33.8%) |
| Nutrients | Amount (Upper), Adjusted HR (Middle), Case Number/Entire Sample (%) | p (FDR) | ||||
|---|---|---|---|---|---|---|
| (Unit) | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | |
| alcohol | x ≤ 0 | 0 < x ≤ 3.2533 | 3.2533 < x ≤14.74 | 14.74 < x ≤ 30.45 | 30.45 < x | |
| (g) | reference | 0.79 (0.62,1.02) | 0.85 (0.72,1) | 0.77 (0.65,0.9) | 0.79 (0.67,0.93) | 0.026 |
| 462/52,407 (0.9%) | 71/9352 (0.8%) | 226/32,299 (0.7%) | 215/33,446 (0.6%) | 232/33,872 (0.7%) | ||
| calcium | x ≤ 688.02 | 688.02 < x ≤ 853.05 | 853.05 < x ≤ 1011.97 | 1011.97 < x ≤ 1226.67 | 1226.67 < x | |
| (mg) | reference | 1.11 (0.92,1.34) | 1.07 (0.89,1.29) | 1.01 (0.84,1.23) | 1.21 (1.01,1.45) | 0.324 |
| 200/31,483 (0.6%) | 237/32,560 (0.7%) | 241/32,671 (0.7%) | 239/32,663 (0.7%) | 289/31,999 (0.9%) | ||
| carbohydrate | x ≤ 187.33 | 187.33 < x ≤ 227.05 | 227.05 < x ≤ 263.84 | 263.84 < x ≤ 312.90 | 312.90 < x | |
| (g) | reference | 0.86 (0.71,1.04) | 0.91 (0.76,1.1) | 1.07 (0.89,1.28) | 1.18 (0.98,1.4) | 0.026 |
| 225/31,682 (0.7%) | 200/32,274 (0.6%) | 218/32,544 (0.7%) | 265/32,813 (0.8%) | 298/32,063 (0.9%) | ||
| carotene | x ≤ 991.92 | 991.92 < x ≤ 1996.76 | 1996.76 < x ≤ 3107.49 | 3107.49 < x ≤ 4748.76 | 4748.76 < x | |
| (µg) | reference | 0.93 (0.78,1.12) | 0.9 (0.75,1.08) | 0.91 (0.76,1.1) | 1.07 (0.9,1.27) | 0.328 |
| 240/31,192 (0.8%) | 225/32,817 (0.7%) | 225/32,932 (0.7%) | 231/32,641 (0.7%) | 285/31,794 (0.9%) | ||
| energy | x ≤ 6757.23 | 6757.23 < x ≤ 7976.07 | 7976.07 < x ≤ 9124.26 | 9124.26 < x ≤ 10,674.42 | 10,674.42 < x | |
| (KJ) | reference | 1.01 (0.84,1.21) | 0.96 (0.8,1.16) | 0.89 (0.73,1.07) | 1.15 (0.96,1.38) | 0.126 |
| 224/30,924 (0.7%) | 235/32,216 (0.7%) | 236/32,667 (0.7%) | 221/33,035 (0.7%) | 290/32,534 (0.9%) | ||
| Englyst dietary fibre | x ≤ 11.10 | 11.10 < x ≤ 14.22 | 14.22 < x ≤ 17.19 | 17.19 < x ≤ 21.14 | 21.14 < x | |
| (g) | reference | 0.94 (0.78,1.13) | 0.83 (0.69,1) | 0.98 (0.82,1.18) | 0.99 (0.83,1.18) | 0.336 |
| 224/31,504 (0.7%) | 227/32,513 (0.7%) | 209/32,632 (0.6%) | 263/32,718 (0.8%) | 283/32,009 (0.9%) | ||
| fat | x ≤ 52.97 | 52.97 < x ≤ 67.44 | 67.44 < x ≤ 81.38 | 81.38 < x ≤ 100.03 | 100.03 < x | |
| (g) | reference | 0.8 (0.67,0.95) | 0.83 (0.69,0.99) | 0.76 (0.64,0.91) | 1 (0.84,1.18) | 0.025 |
| 266/31,328 (0.8%) | 219/32,136 (0.7%) | 232/32,681 (0.7%) | 213/32,695 (0.7%) | 276/32,536 (0.8%) | ||
| folate | x ≤ 213.92 | 213.92 < x ≤ 265.13 | 265.13 < x ≤ 314.08 | 314.08 < x ≤ 381.53 | 381.53 < x | |
| (µg) | reference | 0.84 (0.69,1.01) | 0.8 (0.66,0.96) | 0.88 (0.74,1.06) | 0.98 (0.82,1.17) | 0.126 |
| 231/31,317 (0.7%) | 216/32,488 (0.7%) | 213/32,643 (0.7%) | 250/32,654 (0.8%) | 296/32,274 (0.9%) | ||
| food weight | x ≤ 2552.33 | 2552.33 < x ≤ 2940.00 | 2940.00 < x ≤ 3302.85 | 3302.85 < x ≤ 3782.00 | 3782.00 < x | |
| (g) | reference | 0.95 (0.79,1.14) | 0.89 (0.74,1.07) | 0.93 (0.78,1.12) | 1.07 (0.9,1.28) | 0.35 |
| 247/31,082 (0.8%) | 237/32,243 (0.7%) | 225/32,558 (0.7%) | 233/32,805 (0.7%) | 264/32,688 (0.8%) | ||
| iron | x ≤ 10.08 | 10.08 < x ≤ 12.30 | 12.30 < x ≤ 14.34 | 14.34 < x ≤ 16.96 | 16.96 < x | |
| (mg) | reference | 0.92 (0.77,1.11) | 0.85 (0.7,1.02) | 0.83 (0.69,1) | 1.02 (0.86,1.22) | 0.132 |
| 231/30,826 (0.7%) | 228/32,230 (0.7%) | 219/32,464 (0.7%) | 229/33,002 (0.7%) | 299/32,854 (0.9%) | ||
| magnesium | x ≤ 263.40 | 263.40 < x ≤ 313.92 | 313.92 < x ≤ 360.46 | 360.46 < x ≤ 422.92 | 422.92 < x | |
| (mg) | reference | 0.98 (0.81,1.18) | 0.91 (0.76,1.1) | 0.81 (0.67,0.98) | 1.14 (0.95,1.36) | 0.025 |
| 225/30,903 (0.7%) | 237/32,185 (0.7%) | 228/32,590 (0.7%) | 213/32,937 (0.6%) | 303/32,761 (0.9%) | ||
| polyunsaturated fat | x ≤ 8.32 | 8.32 < x ≤ 11.55 | 11.55 < x ≤ 14.91 | 14.91 < x ≤ 19.51 | 19.51 < x | |
| (g) | reference | 0.87 (0.73,1.04) | 0.89 (0.75,1.06) | 0.74 (0.61,0.89) | 0.89 (0.75,1.06) | 0.078 |
| 275/31,462 (0.9%) | 242/32,390 (0.7%) | 244/32,726 (0.7%) | 202/32,515 (0.6%) | 243/32,283 (0.8%) | ||
| potassium | x ≤ 2821.42 | 2821.42 < x ≤ 3377.58 | 3377.58 < x ≤ 3893.73 | 3893.73 < x ≤ 4571.70 | 4571.70 < x | |
| (mg) | reference | 0.86 (0.71,1.04) | 0.92 (0.76,1.1) | 0.87 (0.73,1.05) | 1.05 (0.88,1.26) | 0.18 |
| 222/31,075 (0.7%) | 210/32,439 (0.6%) | 233/32,666 (0.7%) | 238/32,866 (0.7%) | 303/32,330 (0.9%) | ||
| protein | x ≤ 62.51 | 62.51 < x ≤ 74.76 | 74.76 < x ≤ 85.60 | 85.60 < x ≤ 99.95 | 99.95 < x | |
| (g) | reference | 0.98 (0.82,1.18) | 0.94 (0.78,1.13) | 0.87 (0.72,1.05) | 1.17 (0.98,1.4) | 0.044 |
| 226/31,191 (0.7%) | 238/32,504 (0.7%) | 230/32,577 (0.7%) | 219/32,710 (0.7%) | 293/32,394 (0.9%) | ||
| retinol | x ≤ 176.18 | 176.18 < x ≤ 259.66 | 259.66 < x ≤ 345.04 | 345.04 < x ≤ 459.58 | 459.58 < x | |
| (µg) | reference | 0.96 (0.8,1.16) | 0.94 (0.78,1.14) | 1 (0.83,1.2) | 0.97 (0.81,1.17) | 0.814 |
| 221/31,216 (0.7%) | 224/31,751 (0.7%) | 228/31,963 (0.7%) | 251/32,225 (0.8%) | 259/32,048 (0.8%) | ||
| saturated fat | x ≤ 19.28 | 19.28 < x ≤ 25.25 | 25.25 < x ≤ 31.14 | 31.14 < x ≤ 39.24 | 39.24 < x | |
| (g) | reference | 0.9 (0.75,1.08) | 0.95 (0.79,1.14) | 1.04 (0.87,1.24) | 1.06 (0.89,1.27) | 0.393 |
| 232/31,383 (0.7%) | 218/32,302 (0.7%) | 230/32,601 (0.7%) | 257/32,611 (0.8%) | 269/32,479 (0.8%) | ||
| starch | x ≤ 84.78 | 84.78 < x ≤ 108.32 | 108.32 < x ≤ 129.57 | 129.57 < x ≤ 156.59 | 156.59 < x | |
| (g) | reference | 0.93 (0.78,1.11) | 0.97 (0.81,1.16) | 0.82 (0.68,0.99) | 0.97 (0.81,1.16) | 0.328 |
| 244/31,383 (0.8%) | 240/32,122 (0.7%) | 249/32,585 (0.8%) | 216/32,807 (0.7%) | 257/32,479 (0.8%) | ||
| total sugars | x ≤ 80.88 | 80.88 < x ≤ 103.52 | 103.52 < x ≤ 125.50 | 125.50 < x ≤ 155.11 | 155.11 < x | |
| (g) | reference | 0.82 (0.68,1) | 0.92 (0.76,1.11) | 1.07 (0.89,1.28) | 1.27 (1.07,1.51) | 0.001 |
| 220/31,923 (0.7%) | 186/32,566 (0.6%) | 214/32,579 (0.7%) | 261/32,558 (0.8%) | 325/31,750 (1%) | ||
| vitamin B6 | x ≤ 1.59 | 1.59 < x ≤ 1.95 | 1.95 < x ≤ 2.29 | 2.29 < x ≤ 2.72 | 2.72 < x | |
| (mg) | reference | 0.94 (0.77,1.13) | 0.97 (0.8,1.16) | 0.94 (0.78,1.13) | 1.1 (0.92,1.31) | 0.369 |
| 213/31,540 (0.7%) | 217/32,686 (0.7%) | 235/32,843 (0.7%) | 242/32,350 (0.7%) | 299/31,957 (0.9%) | ||
| vitamin B12 | x ≤ 3.18 | 3.18 < x ≤ 4.65 | 4.65 < x ≤ 6.31 | 6.31 < x ≤ 9.07 | 9.07 < x | |
| (µg) | reference | 1.05 (0.87,1.26) | 1 (0.83,1.2) | 0.99 (0.83,1.19) | 0.98 (0.82,1.18) | 0.814 |
| 216/31,639 (0.7%) | 247/32,359 (0.8%) | 242/32,335 (0.7%) | 244/32,617 (0.7%) | 257/32,426 (0.8%) | ||
| vitamin C | x ≤ 69.00 | 69.00 < x ≤ 109.51 | 109.51 < x ≤ 154.23 | 154.23 < x ≤ 217.06 | 217.06 < x | |
| (mg) | reference | 0.97 (0.81,1.17) | 1 (0.83,1.21) | 1.01 (0.84,1.22) | 1.12 (0.93,1.34) | 0.549 |
| 221/31,367 (0.7%) | 235/32,293 (0.7%) | 245/32,419 (0.8%) | 246/32,809 (0.7%) | 259/32,488 (0.8%) | ||
| vitamin D | x ≤ 0.97 | 0.97 < x ≤ 1.65 | 1.65 < x ≤ 2.52 | 2.52 < x ≤ 4.23 | 4.23 < x | |
| (µg) | reference | 0.91 (0.76,1.1) | 0.87 (0.73,1.04) | 0.83 (0.7,1) | 0.96 (0.81,1.14) | 0.344 |
| 238/31,738 (0.7%) | 234/32,610 (0.7%) | 232/32,269 (0.7%) | 226/32,382 (0.7%) | 276/32,377 (0.9%) | ||
| vitamin E | x ≤ 5.73 | 5.73 < x ≤ 7.64 | 7.64 < x ≤ 9.54 | 9.54 < x ≤ 12.19 | 12.19 < x | |
| (mg) | reference | 0.98 (0.82,1.17) | 1 (0.84,1.2) | 1.02 (0.85,1.22) | 1.02 (0.85,1.22) | 0.814 |
| 241/31,182 (0.8%) | 235/32,358 (0.7%) | 242/32,719 (0.7%) | 244/32,728 (0.7%) | 244/32,389 (0.8%) | ||
| Nutrients | Amount (Upper), Adjusted HR (Lower) | p (Group, FDR) | ||||
|---|---|---|---|---|---|---|
| (Unit) | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | |
| alcohol | x ≤ 0 | 0 < x ≤ 3.2533 | 3.2533 < x ≤ 14.74 | 14.74 < x ≤ 30.45 | 30.45 < x | 0.023 |
| (g) | reference | 0.79 (0.61,1.02): 0.79 (0.62,1.02) | 0.85 (0.72,1): 0.85 (0.72,1) | 0.76 (0.65,0.9): 0.77 (0.65,0.9) | 0.77 (0.65,0.91): 0.79 (0.67,0.93) | |
| calcium | x ≤ 688.02 | 688.02 < x ≤ 853.05 | 853.05 < x ≤ 1011.97 | 1011.97 < x ≤ 1226.67 | 1226.67 < x | 0.516 |
| (mg) | reference | 1.13 (0.93,1.37): 1.11 (0.92,1.34) | 1.1 (0.9,1.34): 1.07 (0.89,1.29) | 1.04 (0.84,1.28): 1.01 (0.84,1.23) | 1.19 (0.96,1.49): 1.21 (1.01,1.45) | |
| carbohydrate | x ≤ 187.33 | 187.33 < x ≤ 227.05 | 227.05 < x ≤ 263.84 | 263.84 < x ≤ 312.90 | 312.90 < x | 0.023 |
| (g) | reference | 0.9 (0.73,1.11): 0.86 (0.71,1.04) | 1.03 (0.82,1.29): 0.91 (0.76,1.1) | 1.31 (1.03,1.68): 1.07 (0.89,1.28) | 1.44 (1.09,1.91): 1.18 (0.98,1.4) | |
| carotene | x ≤ 991.92 | 991.92 < x ≤ 1996.76 | 1996.76 < x ≤ 3107.49 | 3107.49 < x ≤ 4748.76 | 4748.76 < x | 0.440 |
| (ug) | reference | 0.93 (0.77,1.12): 0.93 (0.78,1.12) | 0.89 (0.74,1.08): 0.9 (0.75,1.08) | 0.91 (0.75,1.09): 0.91 (0.76,1.1) | 1.05 (0.88,1.25): 1.07 (0.9,1.27) | |
| Englyst diet fiber | x ≤ 11.10 | 11.10 < x ≤ 14.22 | 14.22 < x ≤ 17.19 | 17.19 < x ≤ 21.14 | 21.14 < x | 0.440 |
| (g) | reference | 0.94 (0.78,1.13): 0.94 (0.78,1.13) | 0.82 (0.68,1): 0.83 (0.69,1) | 0.97 (0.8,1.17): 0.98 (0.82,1.18) | 0.94 (0.77,1.15): 0.99 (0.83,1.18) | |
| fat | x ≤ 52.97 | 52.97 < x ≤ 67.44 | 67.44 < x ≤ 81.38 | 81.38 < x ≤ 100.03 | 100.03 < x | 0.032 |
| (g) | reference | 0.75 (0.61,0.91): 0.8 (0.67,0.95) | 0.76 (0.61,0.94): 0.83 (0.69,0.99) | 0.68 (0.53,0.87): 0.76 (0.64,0.91) | 0.81 (0.62,1.07): 1 (0.84,1.18) | |
| folate | x ≤ 213.92 | 213.92 < x ≤ 265.13 | 265.13 < x ≤ 314.08 | 314.08 < x ≤ 381.53 | 381.53 < x | 0.248 |
| (µg) | reference | 0.83 (0.69,1.01): 0.84 (0.69,1.01) | 0.79 (0.65,0.96): 0.8 (0.66,0.96) | 0.87 (0.71,1.05): 0.88 (0.74,1.06) | 0.93 (0.76,1.14): 0.98 (0.82,1.17) | |
| food weight | x ≤ 2552.33 | 2552.33 < x ≤ 2940.00 | 2940.00 < x ≤ 3302.85 | 3302.85 < x ≤ 3782.00 | 3782.00 < x | 0.614 |
| (g) | reference | 0.95 (0.79,1.14): 0.95 (0.79,1.14) | 0.89 (0.74,1.08): 0.89 (0.74,1.07) | 0.92 (0.76,1.12): 0.93 (0.78,1.12) | 1.02 (0.84,1.25): 1.07 (0.9,1.28) | |
| iron | x ≤ 10.08 | 10.08 < x ≤ 12.30 | 12.30 < x ≤ 14.34 | 14.34 < x ≤ 16.96 | 16.96 < x | 0.328 |
| (mg) | reference | 0.9 (0.75,1.1): 0.92 (0.77,1.11) | 0.82 (0.67,1.01): 0.85 (0.7,1.02) | 0.8 (0.64,1): 0.83 (0.69,1) | 0.93 (0.74,1.17): 1.02 (0.86,1.22) | |
| magnesium | x ≤ 263.40 | 263.40 < x ≤ 313.92 | 313.92 < x ≤ 360.46 | 360.46 < x ≤ 422.92 | 422.92 < x | 0.111 |
| (mg) | reference | 0.97 (0.8,1.18): 0.98 (0.81,1.18) | 0.9 (0.73,1.12): 0.91 (0.76,1.1) | 0.8 (0.64,1.01): 0.81 (0.67,0.98) | 1.07 (0.84,1.37): 1.14 (0.95,1.36) | |
| polyunsaturated fat | x ≤ 8.32 | 8.32 < x ≤ 11.55 | 11.55 < x ≤ 14.91 | 14.91 < x ≤ 19.51 | 19.51 < x | 0.023 |
| (g) | reference | 0.84 (0.7,1.01): 0.87 (0.73,1.04) | 0.84 (0.7,1.02): 0.89 (0.75,1.06) | 0.67 (0.55,0.83): 0.74 (0.61,0.89) | 0.75 (0.6,0.93): 0.89 (0.75,1.06) | |
| potassium | x ≤ 2821.42 | 2821.42 < x ≤ 3377.58 | 3377.58 < x ≤ 3893.73 | 3893.73 < x ≤ 4571.70 | 4571.70 < x | 0.440 |
| (mg) | reference | 0.86 (0.71,1.05): 0.86 (0.71,1.04) | 0.92 (0.75,1.13): 0.92 (0.76,1.1) | 0.87 (0.7,1.09): 0.87 (0.73,1.05) | 1.01 (0.8,1.27): 1.05 (0.88,1.26) | |
| protein | x ≤ 62.51 | 62.51 < x ≤ 74.76 | 74.76 < x ≤ 85.60 | 85.60 < x ≤ 99.95 | 99.95 < x | 0.248 |
| (g) | reference | 0.99 (0.82,1.2): 0.98 (0.82,1.18) | 0.95 (0.78,1.17): 0.94 (0.78,1.13) | 0.89 (0.71,1.11): 0.87 (0.72,1.05) | 1.15 (0.91,1.45): 1.17 (0.98,1.4) | |
| retinol | X ≤ 176.18 | 176.18 < x ≤ 259.66 | 259.66 < x ≤ 345.04 | 345.04 < x ≤ 459.58 | 459.58 < x | 0.790 |
| (µg) | reference | 0.96 (0.8,1.16): 0.96 (0.8,1.16) | 0.94 (0.77,1.14): 0.94 (0.78,1.14) | 0.99 (0.81,1.2): 1 (0.83,1.2) | 0.92 (0.75,1.13): 0.97 (0.81,1.17) | |
| saturated fat | X ≤ 19.28 | 19.28 < x ≤ 25.25 | 25.25 < x ≤ 31.14 | 31.14 < x ≤ 39.24 | 39.24 < x | 0.629 |
| (g) | reference | 0.92 (0.76,1.12): 0.9 (0.75,1.08) | 0.99 (0.8,1.21): 0.95 (0.79,1.14) | 1.08 (0.87,1.35): 1.04 (0.87,1.24) | 1.03 (0.81,1.32): 1.06 (0.89,1.27) | |
| starch | X ≤ 84.78 | 84.78 < x ≤ 108.32 | 108.32 < x ≤ 129.57 | 129.57 < x ≤ 156.59 | 156.59 < x | 0.328 |
| (g) | reference | 0.91 (0.76,1.1): 0.93 (0.78,1.11) | 0.94 (0.77,1.14): 0.97 (0.81,1.16) | 0.78 (0.63,0.96): 0.82 (0.68,0.99) | 0.85 (0.68,1.06): 0.97 (0.81,1.16) | |
| total sugars | X ≤ 80.88 | 80.88 < x ≤ 103.52 | 103.52 < x ≤ 125.50 | 125.50 < x ≤ 155.11 | 155.11 < x | 0.001 |
| (g) | reference | 0.85 (0.7,1.04): 0.82 (0.68,1) | 0.98 (0.8,1.19): 0.92 (0.76,1.11) | 1.17 (0.96,1.43): 1.07 (0.89,1.28) | 1.4 (1.13,1.73): 1.27 (1.07,1.51) | |
| vitamin B6 | X ≤ 3.18 | 3.18 < x ≤ 4.65 | 4.65 < x ≤ 6.31 | 6.31 < x ≤ 9.07 | 9.07 < x | 0.666 |
| (mg) | reference | 0.94 (0.78,1.15): 0.94 (0.77,1.13) | 0.98 (0.8,1.19): 0.97 (0.8,1.16) | 0.95 (0.78,1.16): 0.94 (0.78,1.13) | 1.07 (0.87,1.31): 1.1 (0.92,1.31) | |
| vitamin B12 | X ≤ 1.59 | 1.59 < x ≤ 1.95 | 1.95 < x ≤ 2.29 | 2.29 < x ≤ 2.72 | 2.72 < x | 0.790 |
| (µg) | reference | 1.04 (0.87,1.26): 1.05 (0.87,1.26) | 0.99 (0.82,1.2): 1 (0.83,1.2) | 0.98 (0.81,1.18): 0.99 (0.83,1.19) | 0.96 (0.8,1.16): 0.98 (0.82,1.18) | |
| vitamin C | X ≤ 69.00 | 69.00 < x ≤ 109.51 | 109.51 < x ≤ 154.23 | 154.23 < x ≤ 217.06 | 217.06 < x | 0.666 |
| (mg) | reference | 0.97 (0.81,1.17): 0.97 (0.81,1.17) | 1 (0.83,1.21): 1 (0.83,1.21) | 1.01 (0.84,1.22): 1.01 (0.84,1.22) | 1.1 (0.91,1.33): 1.12 (0.93,1.34) | |
| vitamin D | X ≤ 0.97 | 0.97 < x ≤ 1.65 | 1.65 < x ≤ 2.52 | 2.52 < x ≤ 4.23 | 4.23 < x | 0.398 |
| (µg) | reference | 0.91 (0.76,1.09): 0.91 (0.76,1.1) | 0.86 (0.71,1.03): 0.87 (0.73,1.04) | 0.82 (0.68,0.99): 0.83 (0.7,1) | 0.94 (0.78,1.12): 0.96 (0.81,1.14) | |
| Vitamin E | X ≤ 5.73 | 5.73 < x ≤ 7.64 | 7.64 < x ≤ 9.54 | 9.54 < x ≤ 12.19 | 12.19 < x | 0.800 |
| (mg) | reference | 0.98 (0.81,1.18): 0.98 (0.82,1.17) | 1 (0.82,1.21): 1 (0.84,1.2) | 1 (0.82,1.23): 1.02 (0.85,1.22) | 0.95 (0.76,1.18): 1.02 (0.85,1.22) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeuchi, H.; Kawashima, R. Nutrients and Dementia: Prospective Study. Nutrients 2023, 15, 842. https://doi.org/10.3390/nu15040842
Takeuchi H, Kawashima R. Nutrients and Dementia: Prospective Study. Nutrients. 2023; 15(4):842. https://doi.org/10.3390/nu15040842
Chicago/Turabian StyleTakeuchi, Hikaru, and Ryuta Kawashima. 2023. "Nutrients and Dementia: Prospective Study" Nutrients 15, no. 4: 842. https://doi.org/10.3390/nu15040842
APA StyleTakeuchi, H., & Kawashima, R. (2023). Nutrients and Dementia: Prospective Study. Nutrients, 15(4), 842. https://doi.org/10.3390/nu15040842