
Association between Alcohol Intake and Prostate Cancer Mortality and Survival

 ,
,  ,
,  , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
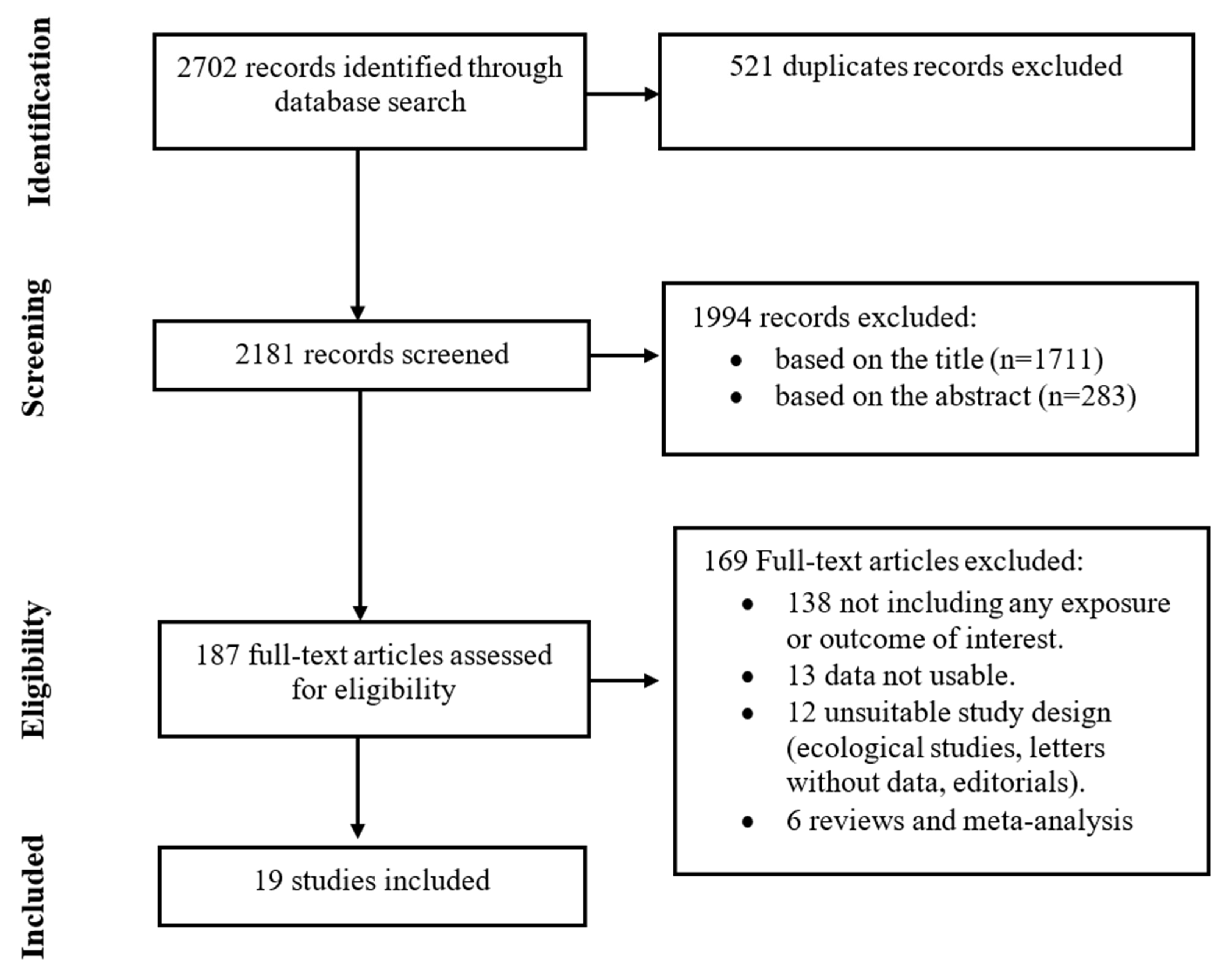
2.1. Sources of Information and Search Strategy
2.2. Eligibility Criteria, Articles Selection, and Data Extraction
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Eligible Studies
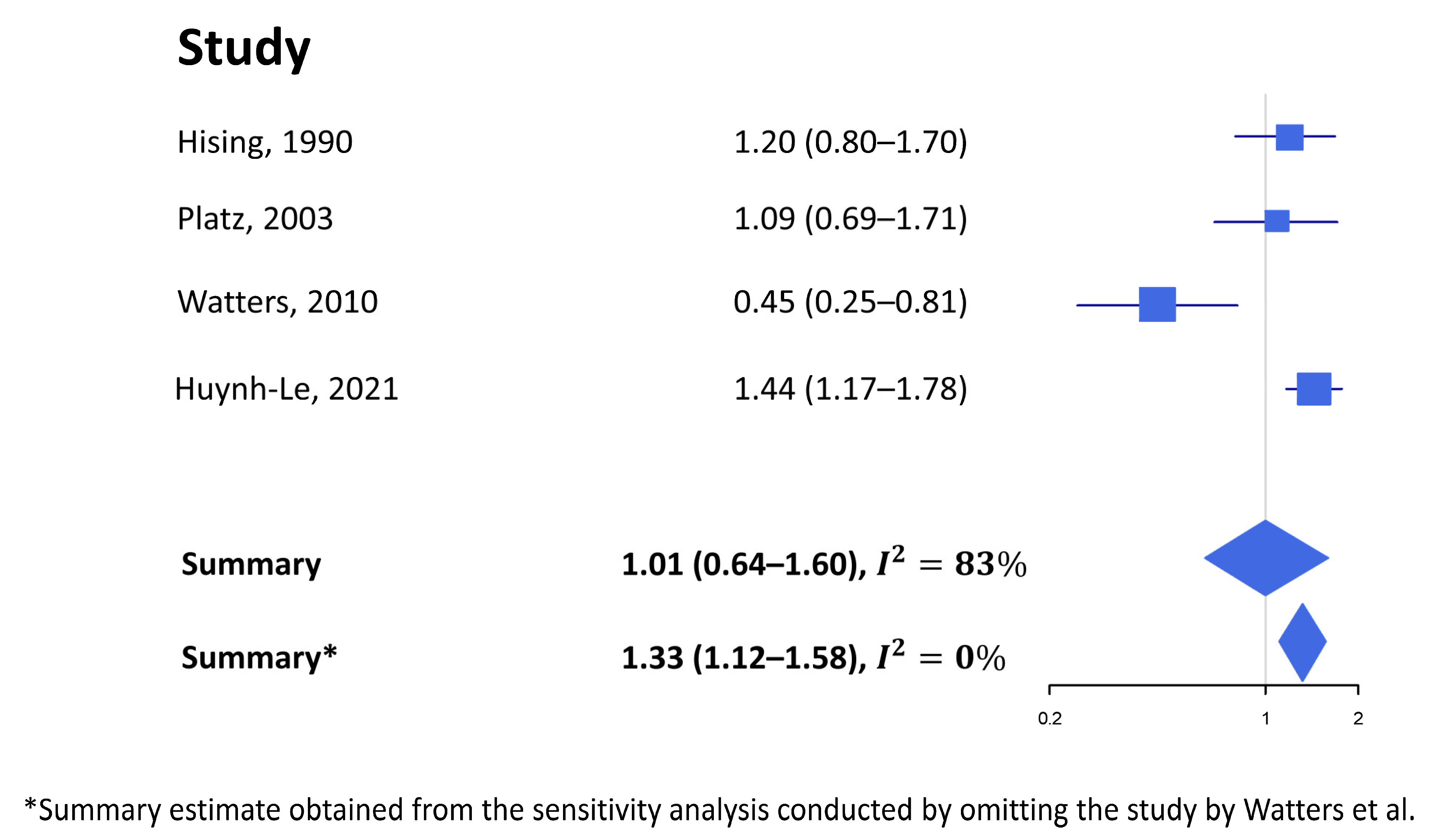
3.2. Fatal Prostate Cancer Incidence in Healthy Subjects
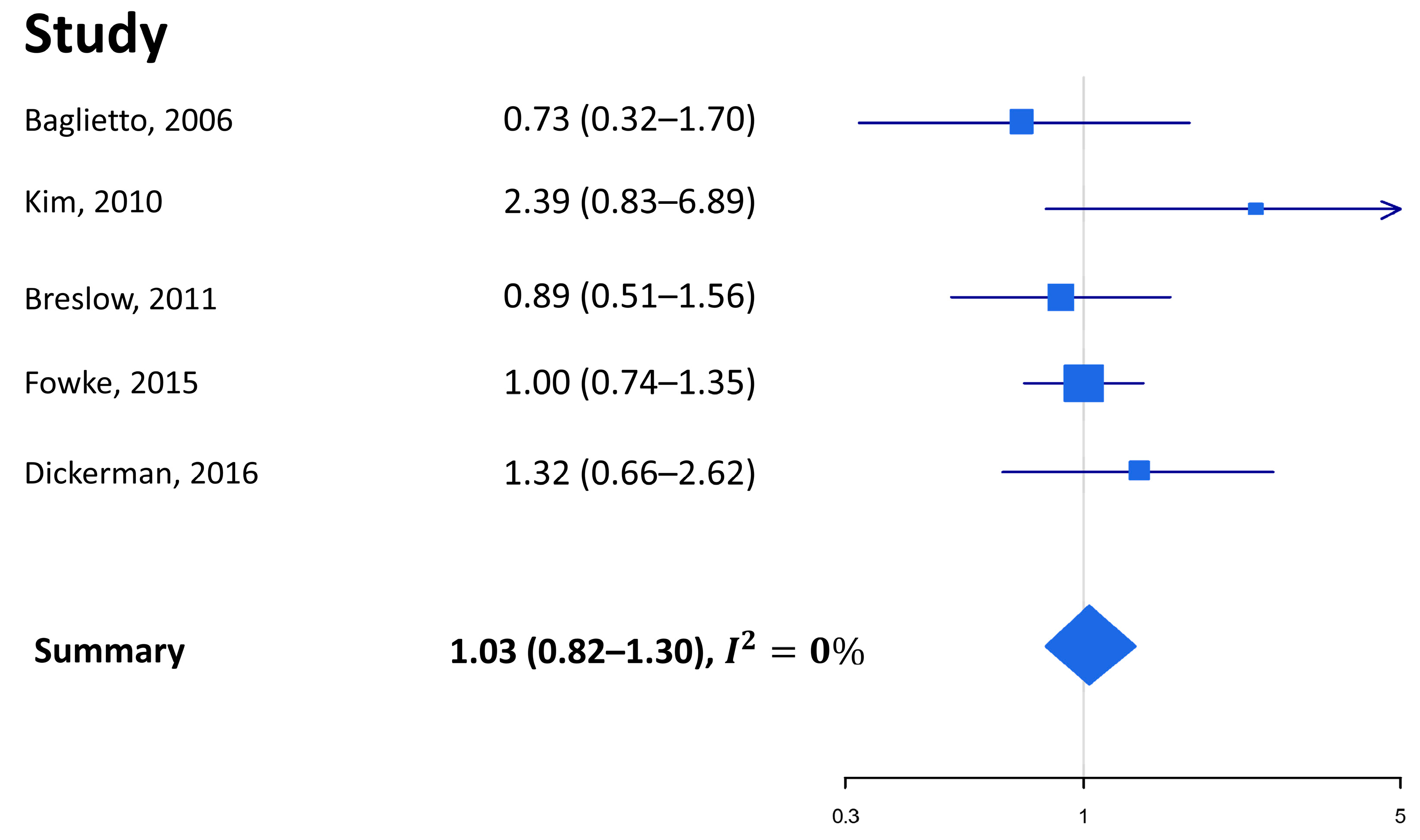
3.3. Prostate Cancer Mortality in Healthy Subjects
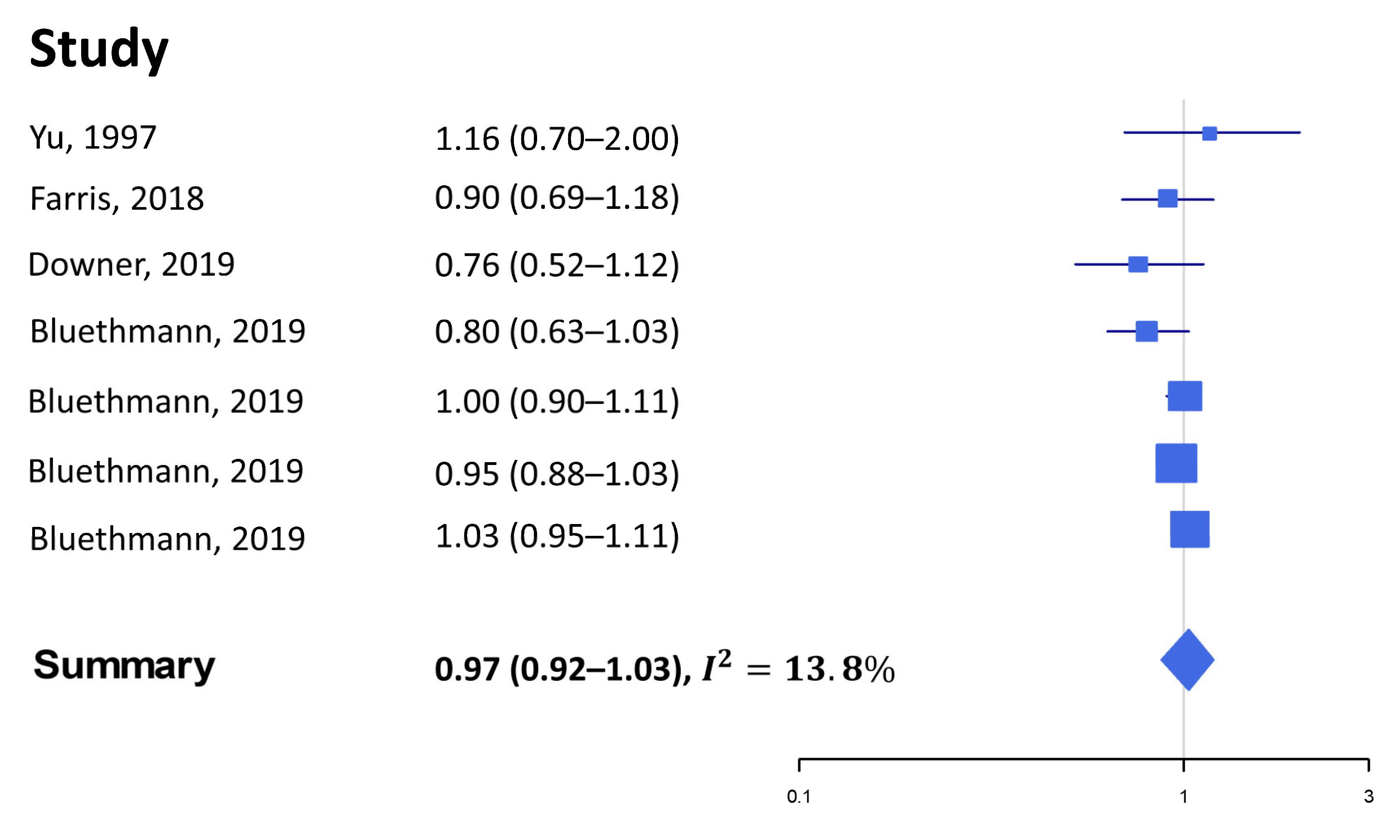
3.4. Survival (and Surrogates Thereof) among Prostate Cancer Patients
3.5. Quality Assessment and Susceptibility to Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Alcohol consumption and ethyl carbamate. IARC Monogr. Eval. Carcinog. Risks Hum. 2010, 96, 3. [Google Scholar]
- Tran, K.B.; Lang, J.J.; Compton, K.; Xu, R.; Acheson, A.R.; Henrikson, H.J.; Kocarnik, J.M.; Penberthy, L.; Aali, A.; Abbas, Q.; et al. The global burden of cancer attributable to risk factors, 2010–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar]
- Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Alcoholic-Drinks.pdf (accessed on 15 January 2023).
- Database. Available online: https://Gco.Iarc.Fr/Today/Data/Factsheets/Cancers/27-Prostate-Fact-Sheet.Pdf (accessed on 30 January 2020).
- Available online: https://www.wcrf.org/wp-content/uploads/2021/02/prostate-cancer-report.pdf (accessed on 15 January 2023).
- Sesso, H.D.; Paffenbarger, R.S.; Lee, I.-M. Alcohol consumption and risk of prostate cancer: The Harvard Alumni Health Study. Int. J. Epidemiol. 2001, 30, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Putnam, S.D.; Cerhan, J.R.; Parker, A.S.; Bianchi, G.D.; Wallace, R.B.; Cantor, K.P.; Lynch, C.F. Lifestyle and Anthropometric Risk Factors for Prostate Cancer in a Cohort of Iowa Men. Ann. Epidemiol. 2000, 10, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Crispo, A.; Talamini, R.; Gallus, S.; Negri, E.; Gallo, A.; Bosetti, C.; La Vecchia, C.; Maso, L.D.; Montella, M. Alcohol and the risk of prostate cancer and benign prostatic hyperplasia. Urology 2004, 64, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Lumey, L.H.; Pittman, B.; Wynder, E.L. Alcohol use and prostate cancer in U.S. whites: No association in a confirmatory study. Prostate 1998, 36, 250–255. [Google Scholar] [CrossRef]
- Nilsen, T.I.L.; Johnsen, R.; Vatten, L.J. Socio-economic and lifestyle factors associated with the risk of prostate cancer. Br. J. Cancer 2000, 82, 1358–1363. [Google Scholar] [CrossRef]
- Rohrmann, S.; Linseisen, J.; Key, T.J.; Jensen, M.K.; Overvad, K.; Johnsen, N.F.; Tjønneland, A.; Kaaks, R.; Bergmann, M.M.; Weikert, C.; et al. Alcohol Consumption and the Risk for Prostate Cancer in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1282–1287. [Google Scholar] [CrossRef]
- Baglietto, L.; Severi, G.; English, D.; Hopper, J.L.; Giles, G.G. Alcohol consumption and prostate cancer risk: Results from the Melbourne collaborative cohort study. Int. J. Cancer 2006, 119, 1501–1504. [Google Scholar] [CrossRef]
- Downer, M.K.; Kenfield, S.A.; Stampfer, M.J.; Wilson, K.M.; Dickerman, B.A.; Giovannucci, E.L.; Rimm, E.B.; Wang, M.; Mucci, L.A.; Willett, W.C.; et al. Alcohol Intake and Risk of Lethal Prostate Cancer in the Health Professionals Follow-Up Study. J. Clin. Oncol. 2019, 37, 1499–1511. [Google Scholar] [CrossRef]
- Zhao, J.; Stockwell, T.; Roemer, A.; Chikritzhs, T. Is alcohol consumption a risk factor for prostate cancer? A systematic review and meta–analysis. BMC Cancer 2016, 16, 1–13. [Google Scholar] [CrossRef]
- Hong, S.; Khil, H.; Lee, D.; Keum, N.; Giovannucci, E. Alcohol Consumption and the Risk of Prostate Cancer: A Dose-Response Meta-Analysis. Nutrients 2020, 12, 2188. [Google Scholar] [CrossRef]
- Penuelas, J.; Krisztin, T.; Obersteiner, M.; Huber, F.; Winner, H.; Janssens, I.; Ciais, P.; Sardans, J. Country-Level Relationships of the Human Intake of N and P, Animal and Vegetable Food, and Alcoholic Beverages with Cancer and Life Expectancy. Int. J. Environ. Res. Public Health 2020, 17, 7240. [Google Scholar] [CrossRef] [PubMed]
- Alattas, M.; Ross, C.S.; Henehan, E.R.; Naimi, T.S. Alcohol policies and alcohol-attributable cancer mortality in U.S. States. Chem. Interact. 2019, 315, 108885. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.; Chang, Y.; Kim, H.-N.; Kang, J.-H.; Shin, H.; Sung, E.; Ryu, S. Low-level alcohol consumption and cancer mortality. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Esser, M.B.; Leung, G.; Sherk, A.; Bohm, M.K.; Liu, Y.; Lu, H.; Naimi, T.S. Estimated Deaths Attributable to Excessive Alcohol Use Among US Adults Aged 20 to 64 Years, 2015 to 2019. JAMA Netw. Open 2022, 5, e2239485. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-Y.; Fisher, P.; Harris, D.; Tseng, T.-S. Alcohol intake patterns for cancer and non-cancer individuals: A population study. Transl. Cancer Res. 2019, 8, S334–S345. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Watters, J.L.; Park, Y.; Hollenbeck, A.; Schatzkin, A.; Albanes, D. Alcoholic Beverages and Prostate Cancer in a Prospective US Cohort Study. Am. J. Epidemiol. 2010, 172, 773–780. [Google Scholar] [CrossRef]
- Roach, M.; Hanks, G.; Thames, H.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Wells, G.A.; Wells, G.; Shea, B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch; Losos, M.; Tugwell, P.; Ga, S.W.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Environ. Sci. 2014. [Google Scholar]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Hsing, A.W.; McLaughlin, J.K.; Schuman, L.M.; Bjelke, E.; Gridley, G.; Wacholder, S.; Chien, H.T.; Blot, W.J. Diet, tobacco use, and fatal prostate cancer: Results from the Lutheran Brotherhood Cohort Study. Cancer Res. 1990, 50, 6836–6840. [Google Scholar]
- Platz, E.A.; Leitzmann, M.F.; Rimm, E.B.; Willett, W.C.; Giovannucci, E. Alcohol Intake, Drinking Patterns, and Risk of Prostate Cancer in a Large Prospective Cohort Study. Am. J. Epidemiol. 2004, 159, 444–453. [Google Scholar] [CrossRef]
- Huynh-Le, M.-P.; Karunamuni, R.; Fan, C.C.; Thompson, W.K.; Muir, K.; Lophatananon, A.; Tye, K.; Wolk, A.; Håkansson, N.; Mills, I.G.; et al. Common genetic and clinical risk factors: Association with fatal prostate cancer in the Cohort of Swedish Men. Prostate Cancer Prostatic Dis. 2021, 24, 845–851. [Google Scholar] [CrossRef]
- Dahlman, D.; Li, X.; Crump, C.; Sundquist, J.; Sundquist, K. Drug use disorder and risk of incident and fatal prostate cancer among Swedish men: A nationwide epidemiological study. Cancer Causes Control 2021, 33, 213–222. [Google Scholar] [CrossRef]
- Kim, M.K.; Ko, M.J.; Han, J.T. Alcohol consumption and mortality from all-cause and cancers among 1.34 million Koreans: The results from the Korea national health insurance corporation’s health examinee cohort in 2000. Cancer Causes Control 2010, 21, 2295–2302. [Google Scholar] [CrossRef]
- Breslow, R.A.; Chen, C.M.; Graubard, B.I.; Mukamal, K.J. Prospective Study of Alcohol Consumption Quantity and Frequency and Cancer-Specific Mortality in the US Population. Am. J. Epidemiol. 2011, 174, 1044–1053. [Google Scholar] [CrossRef]
- Fowke, J.H.; McLerran, D.F.; Gupta, P.C.; He, J.; Shu, X.-O.; Ramadas, K.; Tsugane, S.; Inoue, M.; Tamakoshi, A.; Koh, W.-P.; et al. Associations of Body Mass Index, Smoking, and Alcohol Consumption With Prostate Cancer Mortality in the Asia Cohort Consortium. Am. J. Epidemiol. 2015, 182, 381–389. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Markt, S.C.; Koskenvuo, M.; Pukkala, E.; Mucci, L.A.; Kaprio, J. Alcohol intake, drinking patterns, and prostate cancer risk and mortality: A 30-year prospective cohort study of Finnish twins. Cancer Causes Control 2016, 27, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.P.; Ostroff, J.S.; Zhang, Z.F.; Tang, J.; Schantz, S.P. Smoking history and cancer patient survival: A hospital cancer registry study. Cancer Detect. Prev. 1997, 21, 497–509. [Google Scholar] [PubMed]
- Chamie, K.; Daskivich, T.J.; Kwan, L.; Labo, J.; Dash, A.; Greenfield, S.; Litwin, M.S. Comorbidities, Treatment and Ensuing Survival in Men with Prostate Cancer. J. Gen. Intern. Med. 2011, 27, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Jayadevappa, R.; Chhatre, S. Association between age, substance use, and outcomes in Medicare enrollees with prostate cancer. J. Geriatr. Oncol. 2016, 7, 444–452. [Google Scholar] [CrossRef]
- Brunner, C.; Davies, N.M.; Martin, R.M.; Eeles, R.; Easton, D.; Kote-Jarai, Z.; Al Olama, A.A.; Benlloch, S.; Muir, K.; Giles, G.; et al. Alcohol consumption and prostate cancer incidence and progression: A Mendelian randomisation study. Int. J. Cancer 2016, 140, 75–85. [Google Scholar] [CrossRef]
- Farris, M.S.; Courneya, K.S.; Kopciuk, K.A.; McGregor, S.E.; Friedenreich, C.M. Post-diagnosis alcohol intake and prostate cancer survival: A population-based cohort study. Int. J. Cancer 2018, 143, 253–262. [Google Scholar] [CrossRef]
- Bluethmann, S.M.; Wang, M.; Wasserman, E.; Chen, C.; Zaorsky, N.G.; Hohl, R.J.; McDonald, A.C. Prostate cancer in Pennsylvania: The role of older age at diagnosis, aggressiveness, and environmental risk factors on treatment and mortality using data from the Pennsylvania Cancer Registry. Cancer Med. 2020, 9, 3623–3633. [Google Scholar] [CrossRef]
- Ly, D.; Reddy, C.A.; Klein, E.A.; Ciezki, J.P. Association of Body Mass Index With Prostate Cancer Biochemical Failure. J. Urol. 2010, 183, 2193–2199. [Google Scholar] [CrossRef]
- Burton, A.J.; Martin, R.M.; Donovan, J.L.; Lane, J.A.; Davis, M.; Hamdy, F.C.; Neal, D.E.; Tilling, K. Associations of Lifestyle Factors and Anthropometric Measures with Repeat PSA Levels During Active Surveillance/Monitoring. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1877–1885. [Google Scholar] [CrossRef]
- Gordon, G.G.; Altman, K.; Southren, A.L.; Rubin, E.; Lieber, C.S. Effect of Alcohol (Ethanol) Administration on Sex-Hormone Metabolism in Normal Men. N. Engl. J. Med. 1976, 295, 793–797. [Google Scholar] [CrossRef]
- Greenfield, T.K.; Kerr, W.C. Alcohol measurement methodology in epidemiology: Recent advances and opportunities. Addiction 2008, 103, 1082–1099. [Google Scholar] [CrossRef] [PubMed]
- Saieva, C.; Bardazzi, G.; Masala, G.; Quartini, A.; Ceroti, M.; Iozzi, A.; Gelain, E.; Querci, A.; Allamani, A.; Palli, D. General and Cancer Mortality in a Large Cohort of Italian Alcoholics. Alcohol. Clin. Exp. Res. 2011, 36, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Macke, A.J.; Petrosyan, A. Alcohol and Prostate Cancer: Time to Draw Conclusions. Biomolecules 2022, 12, 375. [Google Scholar] [CrossRef] [PubMed]
- Bonovas, S.; Filioussi, K.; Tsantes, A. Diabetes mellitus and risk of prostate cancer: A meta-analysis. Diabetologia 2004, 47, 1071–1078. [Google Scholar] [CrossRef]
- Beckmann, K.; Crawley, D.; Nordström, T.; Aly, M.; Olsson, H.; Lantz, A.; Jalal, N.B.A.; Garmo, H.; Adolfsson, J.; Eklund, M.; et al. Association Between Antidiabetic Medications and Prostate-Specific Antigen Levels and Biopsy Results. JAMA Netw. Open 2019, 2, e1914689. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Marvaso, G.; Jereczek-Fossa, B.A.; de Cobelli, O.; Simoncini, M.C.; Teixeira, L.F.N.; Sabbatini, A.; Pravettoni, G.; Johansson, H.; Nezi, L.; et al. Life style and interaction with microbiota in prostate cancer patients undergoing radiotherapy: Study protocol for a randomized controlled trial. BMC Cancer 2022, 22, 794. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, PY | Exposure | RR (95%CI) | Adj |
|---|---|---|---|
| Hsing A.W. et al. 1990 [29] | Age | ||
| Beer | |||
| Former vs. never | 1.7 (1.0–2.9) | ||
| Current vs. never | 1.2 (0.8–1.7) | ||
| Liquor | |||
| Former vs. never | 0.7 (0.3–1.5) | ||
| Current vs. never | 1.0 (0.7–1.4) | ||
| Platz A.E. et al. 2003 [30] | Current age, BMI at age 21, height, smoking, FHPC, major ancestry, diabetes, vasectomy, vigorous PA, intakes of total energy, calcium, fructose, tomato sauce, red meat, fish, vitamin E and α-linolenic acid | ||
| Drinking frequency (days/week) | Distant metastatic or fatal cases | ||
| 1–2 vs. 0 1 | 0.83 (0.59–1.18) | ||
| 3–4 vs. 0 1 | 1.00 (0.67–1.51) | ||
| 5–6 vs. 0 1 | 1.18 (0.80–1.75) | ||
| 7 vs. 0 1 | 0.76 (0.51–1.14) | ||
| Alcohol intake (g/day) | Distant metastatic or fatal cases | ||
| 0.1–4.9 vs. 0 1 | 0.83 (0.57–1.21) | ||
| 5.0–14.9 vs. 0 1 | 1.09 (0.78–1.57) | ||
| 15.0–29.9 vs. 0 1 | 0.85 (0.53–1.35) | ||
| 30.0 −49.9 vs. 0 1 | 1.09 (0.69–1.71) | ||
| Watters L.J. et al. 2010 [22] | Age, race, education, marital status, height, BMI, PA, FHPC, diabetes, self-reported health status, smoking, PSA screening, digital rectal examination, total energy (excluding alcohol), α-tocopherol, calcium, red meat, fish, tomato, α-linolenic acid, selenium | ||
| Alcohol (Drinks/Day) | Fatal cases | ||
| <1 vs. 0 1 | 0.86 (0.69–1.08) | ||
| 1–3 vs. 0 1 | 0.95 (0.72–1.26) | ||
| >3 and <6 vs. 0 1 | 0.81 (0.53–1.21) | ||
| ≥6 vs. 0 1 | 0.45 (0.25–0.81) | ||
| Huynh-Le M.P. et al. 2021 [31] | FHPC, Diabetes history, age | ||
| history of alcohol intake | 1.44 (1.17–1.78) 2 | ||
| Yes vs. no 1 | |||
| alcohol intake with the polygenic hazard score (PHS46): | 1.45 (1.19–1.76) 2 | FHPC, Diabetes history, age, PHS46 | |
| Yes vs. no 1 | |||
| alcohol intake with the polygenic hazard score (PHS166) | 1.52 (1.22–1.88) 2 | FHPC, Diabetes history, age, PHS166 | |
| Yes vs. no 1 | |||
| Dahlman D. et al. 2022 [32] | Alcohol use disorder | 0.90 (0.82–0.97) | age, educational attainment, social welfare, marital status, region of residence, immigrant status, comorbidities |
| First Author, PY | Exposure | RR (95%CI) | Adj |
|---|---|---|---|
| Baglietto L. et al. 2006 [12] | Total alcohol (g/day) | Country of birth | |
| 1–19 vs. Lifetime abstainers | 0.56 (0.28,1.14) | ||
| 20–39 vs. Lifetime abstainers | 0.60 (0.26,1.38) | ||
| 40+ vs. Lifetime abstainers | 0.73 (0.32,1.70) | ||
| Kim M.K. et al. 2010 [33] | Alcohol consumption, g/day: | Age, residential, smoking, regular exercise, BMI, systolic and diastolic blood pressure, fasting blood sugar | |
| 1.0–14.9 vs. Non drinker 1 | 1.32 (0.59–3.00) 2 | ||
| 15–29.9 vs. Non drinker 1 | 1.75 (0.72–4.22) 2 | ||
| 30–89.9 vs. Non drinker 1 | 2.09 (0.84–5.19) 2 | ||
| ≥90 vs. Non drinker 1 | 2.39 (0.83–6.89) 2 | ||
| Breslow R.A. et al. 2011 [34] | Former drinker 3 vs. Never drinker 4 | 1.12 (0.81–1.55) | Race/ethnicity, education, region, marital status, smoking status, BMI |
| Lifetime infrequent drinker 5 vs. Never drinker | 1.00 (0.67–1.48) | ||
| Current drinker 6: | |||
| Light 7 vs. Never drinker | 0.93 (0.66–1.30) | ||
| Moderate 8 vs. Never drinker | 1.22 (0.86–1.72) | ||
| Heavier 9 vs. Never drinker | 0.89 (0.51–1.56) | ||
| Among Current Drinkers (quantity) | |||
| Q = 2 vs. Q = 1 | 0.93 (0.61–1.41) | ||
| Q ≥ 3 vs. Q = 1 | 0.90 (0.58–1.39) | ||
| Frequency (average number of drinking days per week) | |||
| F = 1/2 vs. F < 1 | 1.70 (1.09–2.64) | ||
| F ≥ 3 vs. F < 1 | 1.55 (1.01–2.38) | ||
| Fowke J.H. et al. 2015 [35] | Age, education, population density, marital status, history of severe cancer, heart disease or stroke at baseline | ||
| Level of Alcohol Consumption | |||
| None 1 vs. 1–155 g/week | 1.02 (0.78–1.34) | ||
| ≥156 g/week vs. 1–155 g/week | 1.00 (0.74–1.35) | ||
| Dickerman B.A. et al. 2016 [36] | Alcohol consumption (continuous) | 1.06 (0.91–1.23) | BMI, smoking, social class, education, PA |
| Abstainers vs. light drinkers | 1.90 (1.04–3.47) | ||
| Moderate vs. light drinkers | 1.22 (0.76–1.97) | ||
| Heavy vs. light drinkers | 1.32 (0.66–2.62) | ||
| Binge drinking status | |||
| Yes vs. no | 0.87 (0.52–1.45) |
| First Author, PY | Exposure | HR (95%CI) | Adj |
|---|---|---|---|
| Yu G.P. et al. 1997 [37] | Alcohol use: | not specified | |
| Ever vs. never 1 | 1.16 (0.70–2.0) | ||
| Chamie K. et al. 2012 [38] | History of alcoholism | Non-prostate Cancer-related Mortality | not specified |
| Yes vs. no | 1.77 (1.07–2.93) 3 | ||
| Jayadevappa R. et al. 2016 [39] | Race, ethnicity, marital status, census tract median income, census tract proportion with college education, geographic area, disease severity, co-morbidity, prostate cancer treatment | ||
| Type of substance use disorder: | |||
| Alcohol dependence syndrome | Overall survival: | ||
| Age 66–74 | 1.4 (1.1–1.8) | ||
| Age ≥ 75 | 0.8 (0.6–1.2) | ||
| Brunner C. et al. 2016 [40] | SNPs within ALDH1A2 following a diagnosis of any prostate cancer: | Cause-specific survival: | not specified |
| rs1441817 | 0.78 (0.66–0.91) 4 | ||
| rs12910509 | 0.76 (0.64–0.91) 4 | ||
| rs8041922 | 0.76 (0.64–0.91) 4 | ||
| In ALDH1B1 following a diagnosis of low grade prostate cancer: | |||
| rs10973794 | 1.43 (1.14–1.79) 4 | ||
| Farris M.S. et al. 2018 [41] | Age, stage, PSA levels, Gleason score, smoking status and BMI at diagnosis, prostatectomy, hormone therapy, Charlson comorbidity score, lifetime total physical activity, education level and how often (on average) participants went for a general check-up in their lifetime prior to diagnosis of prostate cancer | ||
| Post-diagnosis dose intake drinks/week | Overall survival: | ||
| >0 to <0.9 vs. none 1 | 0.76 (0.58–1.00) | ||
| >0.9 to <3.7 vs. none 1 | 0.77 (0.61–0.98) | ||
| >3.7 to <8.3 vs. none 1 | 0.76 (0.58–1.01) | ||
| ≥8.3 vs. none 1 | 0.90 (0.69–1.18) | ||
| Post-diagnosis dose of alcohol intake (drinks/week) | Cause specific mortality 2 | ||
| >0 to <0.9 vs. none 1 | 0.93 (0.56–1.52) | ||
| >0.9 to <3.7 vs. none 1 | 1.06 (0.71–1.59) | ||
| >3.7 to <8.3 vs. none 1 | 0.89 (0.54–1.45) | ||
| ≥8.3 vs. none 1 | 1.31 (0.85–2.04) | ||
| Post-diagnosis dose of alcohol intake (drinks/week) | Cause specific mortality 3 | ||
| >0 to <0.9 vs. none 1 | 1.08 (0.65–1.78) | ||
| >0.9 to <3.7 vs. none 1 | 1.23 (0.80–1.87) | ||
| >3.7 to <8.3 vs. none 1 | 1.03 (0.63–1.70) | ||
| ≥8.3 vs. none 1 | 1.47 (0.91–2.37) | ||
| Bluethmann S.M. et al. 2019 [42] | Chronic drinking 5 | Race/ethnicity, insurance status, rurality, lymph node status, PC aggressiveness, serum PSA and behavioral risk factors from BRFSS (smoking, obesity, physical inactivity, chronic drinking and FV intake) | |
| Subgroup by age: | Cause-specific survival: | ||
| 40–54 | 0.80 (0.63–1.03) | ||
| 55–64 | 1.00 (0.90–1.11) | ||
| 65–74 | 0.95 (0.88–1.03) | ||
| 75+ | 1.03 (0.95–1.11) | ||
| Downer M.K. et al. 2019 [13] | Total energy intake, smoking, BMI. Vigorous physical activity, choline, coffee, lycopene, whole milk, diabetes, PSA screening, | ||
| First post-diagnostic report intake g/d | Overall survival: | ||
| >0 to <10 vs. none 1 | 0.84 (0.64–1.10) | ||
| >10 to <15 vs. none 1 | 0.77 (0.54–1.10) | ||
| 15 to <30 vs. none 1 | 0.71 (0.50–1.00) | ||
| ≥30 vs. none 1 | 0.76 (0.52–1.12) | ||
| Cause specific survival: | |||
| >0 to <10 vs. none 1 | 1.17 (0.63–2.19) | ||
| >10 to <15 vs. none 1 | 1.02 (0.45–2.29) | ||
| 15 to <30 vs. none 1 | 0.63 (0.31–1.31) | ||
| ≥30 vs. none 1 | 1.32 (0.53–3.25) |
| First Author, PY | Exposure | HR (95%CI) | Adj |
|---|---|---|---|
| Ly D. et al. 2010 [43] | Alcohol consumption: | Biochemical failure: 1.15 (0.91–1.45) | No |
| Yes vs. No | |||
| Burton A.J. et al. 2012 [44] | Alcohol (per 10 units a week) | PSA at age 50 (expressed as % difference in baseline PSA): | |
| −2.10 (−5.00–0.8) 1 | Age, height, weight, WC, HC, inside leg, occupational class, smoking status, exercise | ||
| −2.20 (−5.1–0.70) 2 | Age, height, weight, WC, HC, inside leg, occupational class, smoking status, exercise, Gleason score | ||
| Yearly increase in PSA (expressed as %change in yearly increase in PSA): | |||
| −0.20 (−0.40–0.10) 1 | Age, height, weight, WC, HC, inside leg, occupational class, smoking status, exercise | ||
| −0.20 (−0.40–0.10) | Age, height, weight, WC, HC, inside leg, occupational class, smoking status, exercise, Gleason score |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ecclesiis, O.; Pastore, E.; Gandini, S.; Caini, S.; Marvaso, G.; Jereczek-Fossa, B.A.; Corrao, G.; Raimondi, S.; Bellerba, F.; Ciceri, S.; et al. Association between Alcohol Intake and Prostate Cancer Mortality and Survival. Nutrients 2023, 15, 925. https://doi.org/10.3390/nu15040925
D’Ecclesiis O, Pastore E, Gandini S, Caini S, Marvaso G, Jereczek-Fossa BA, Corrao G, Raimondi S, Bellerba F, Ciceri S, et al. Association between Alcohol Intake and Prostate Cancer Mortality and Survival. Nutrients. 2023; 15(4):925. https://doi.org/10.3390/nu15040925
Chicago/Turabian StyleD’Ecclesiis, Oriana, Elisa Pastore, Sara Gandini, Saverio Caini, Giulia Marvaso, Barbara A. Jereczek-Fossa, Giulia Corrao, Sara Raimondi, Federica Bellerba, Silvia Ciceri, and et al. 2023. "Association between Alcohol Intake and Prostate Cancer Mortality and Survival" Nutrients 15, no. 4: 925. https://doi.org/10.3390/nu15040925
APA StyleD’Ecclesiis, O., Pastore, E., Gandini, S., Caini, S., Marvaso, G., Jereczek-Fossa, B. A., Corrao, G., Raimondi, S., Bellerba, F., Ciceri, S., Latella, M., Cavalcabò, N. d. B., Bendinelli, B., Saieva, C., Fontana, M., & Gnagnarella, P. (2023). Association between Alcohol Intake and Prostate Cancer Mortality and Survival. Nutrients, 15(4), 925. https://doi.org/10.3390/nu15040925