
Benefits of Probiotic Pretreatment on the Gut Microbiota and Minor Complications after Bowel Preparation for Colonoscopy: A Randomized Double-Blind, Placebo-Controlled Pilot Trial

 ,
,
Abstract
:1. Introduction
2. Methods
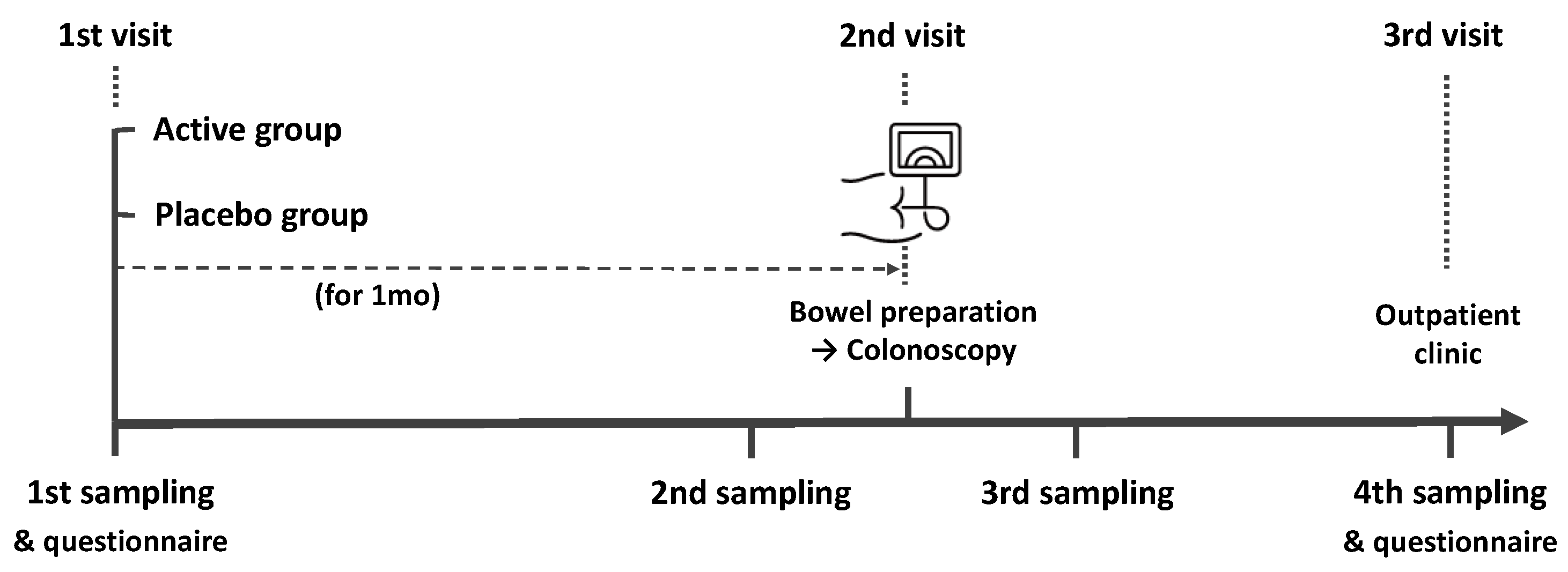
2.1. Study Design and Participants
2.2. Randomization
2.3. Endpoints
2.4. Sample Preparation and Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Colonoscopy Outcomes
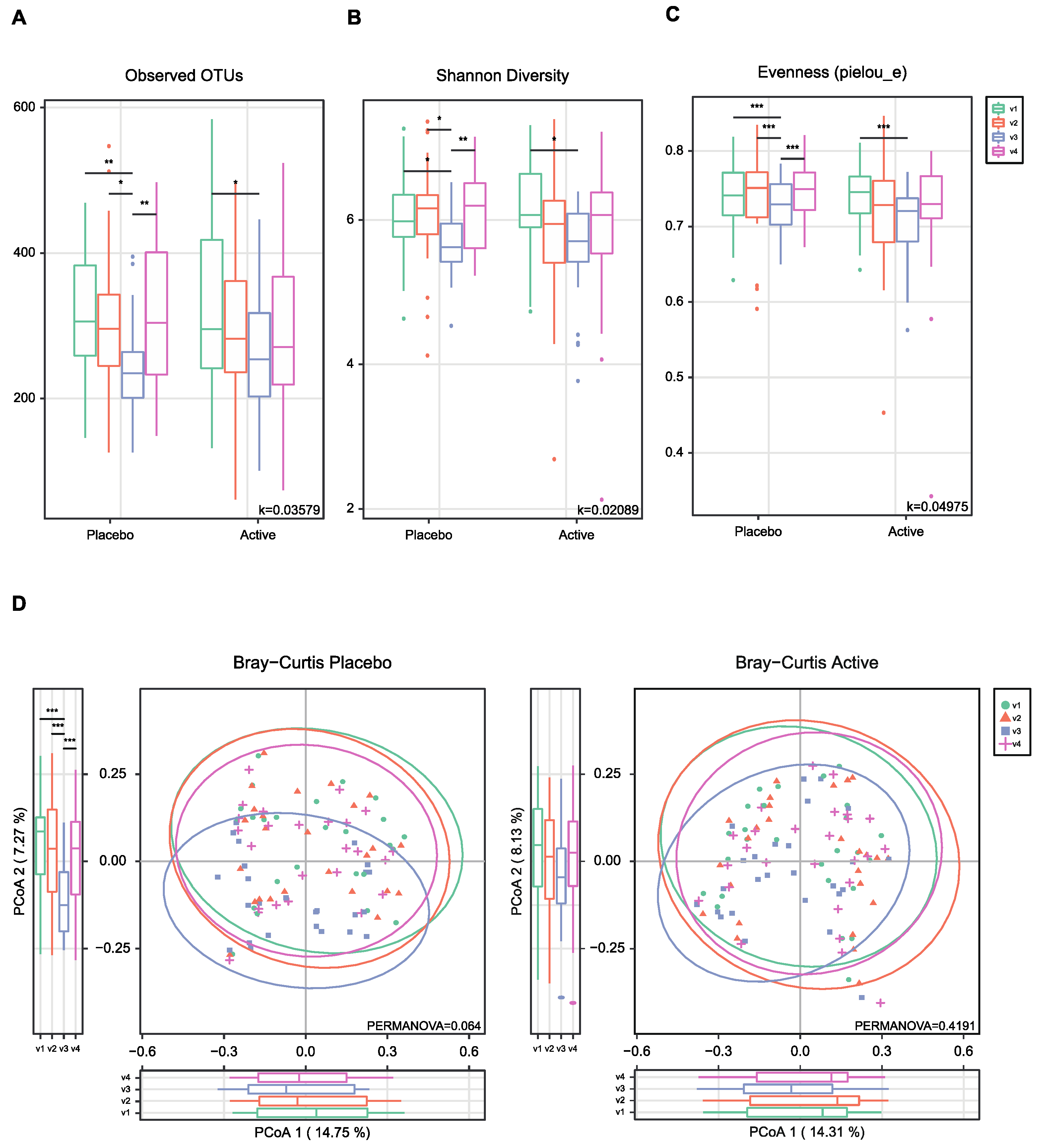
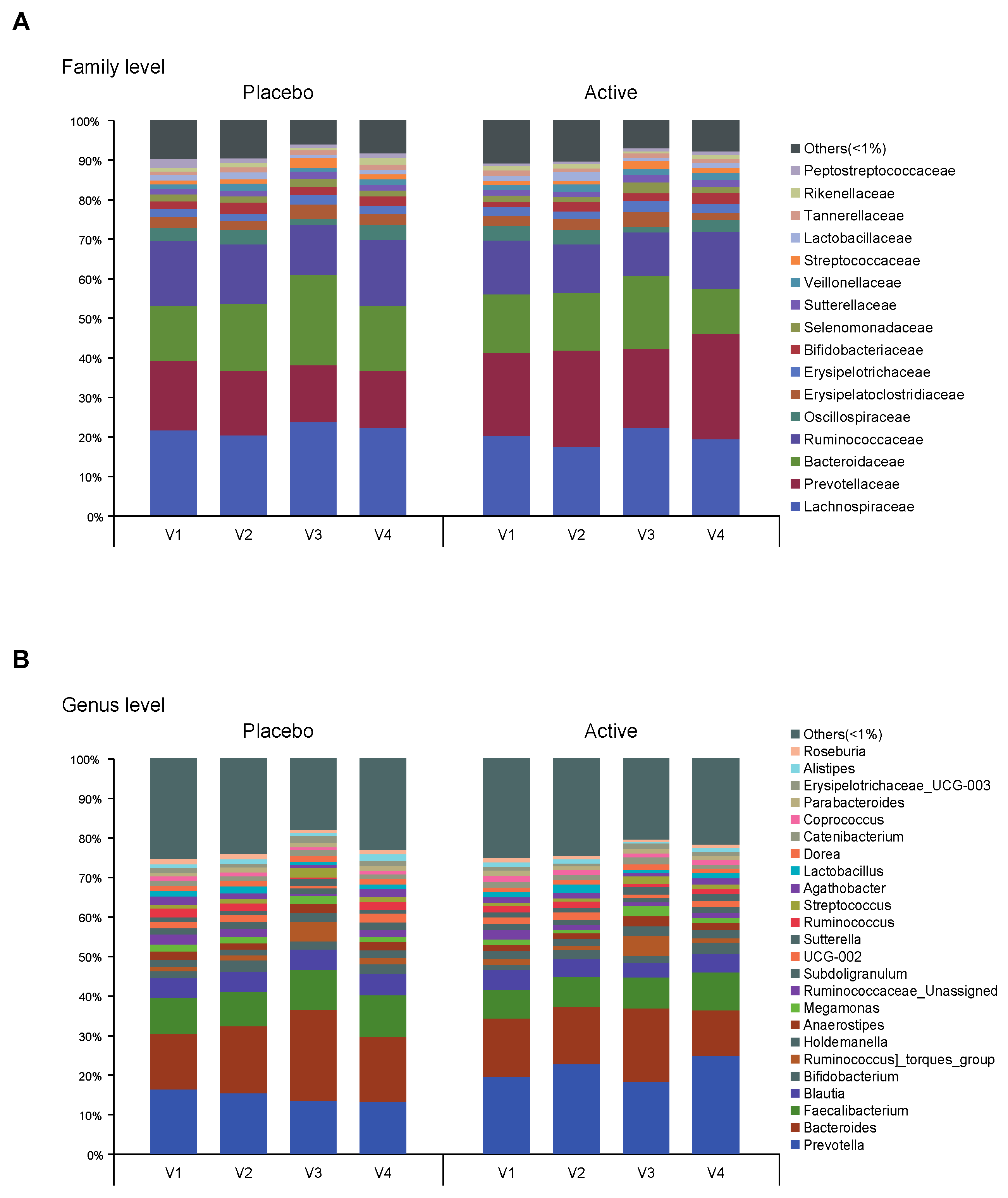
3.2. Alteration and Restoration of Gut Microbiota after Bowel Preparation
3.3. Complications after Bowel Preparation and Factors Associated with Complications
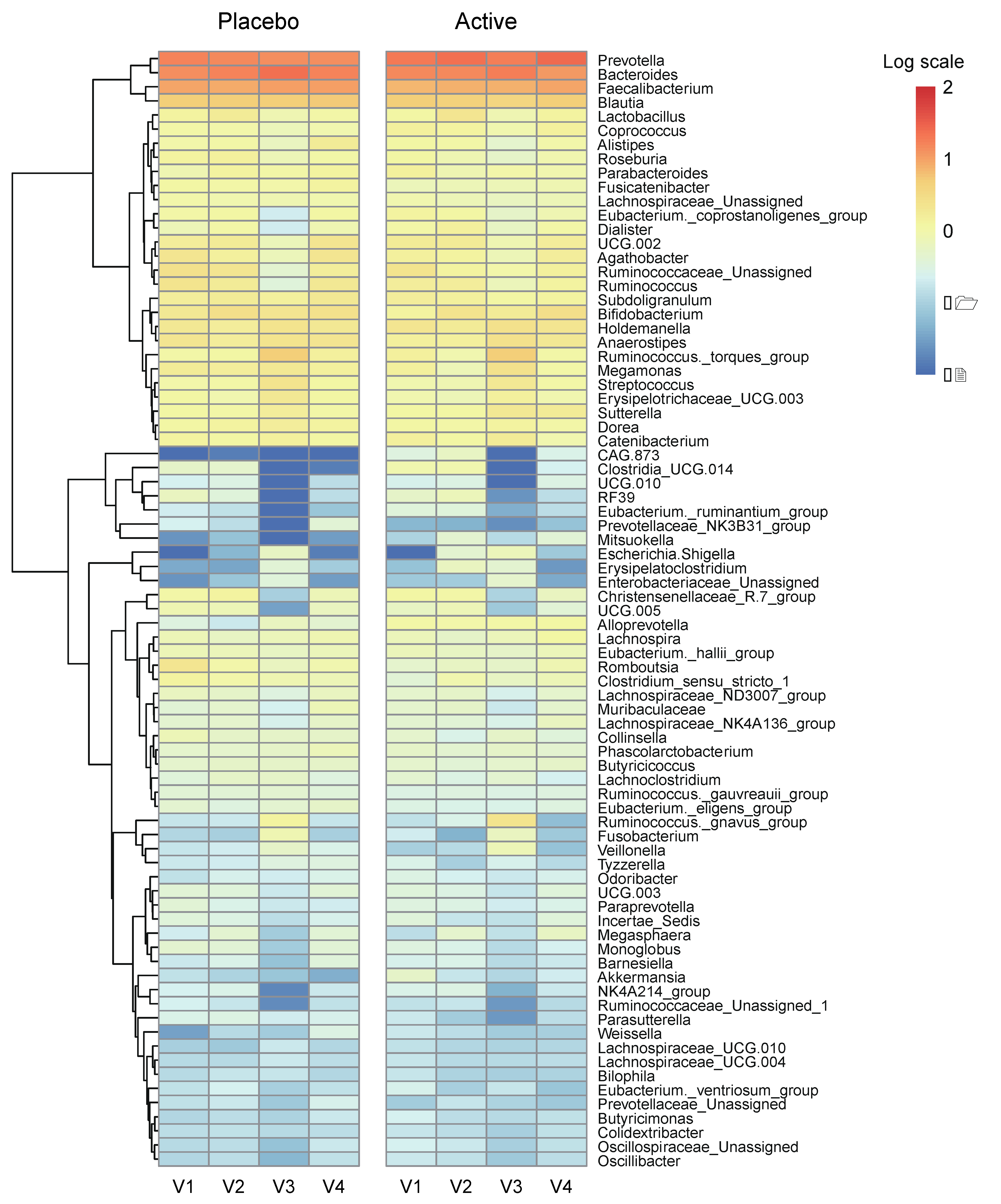
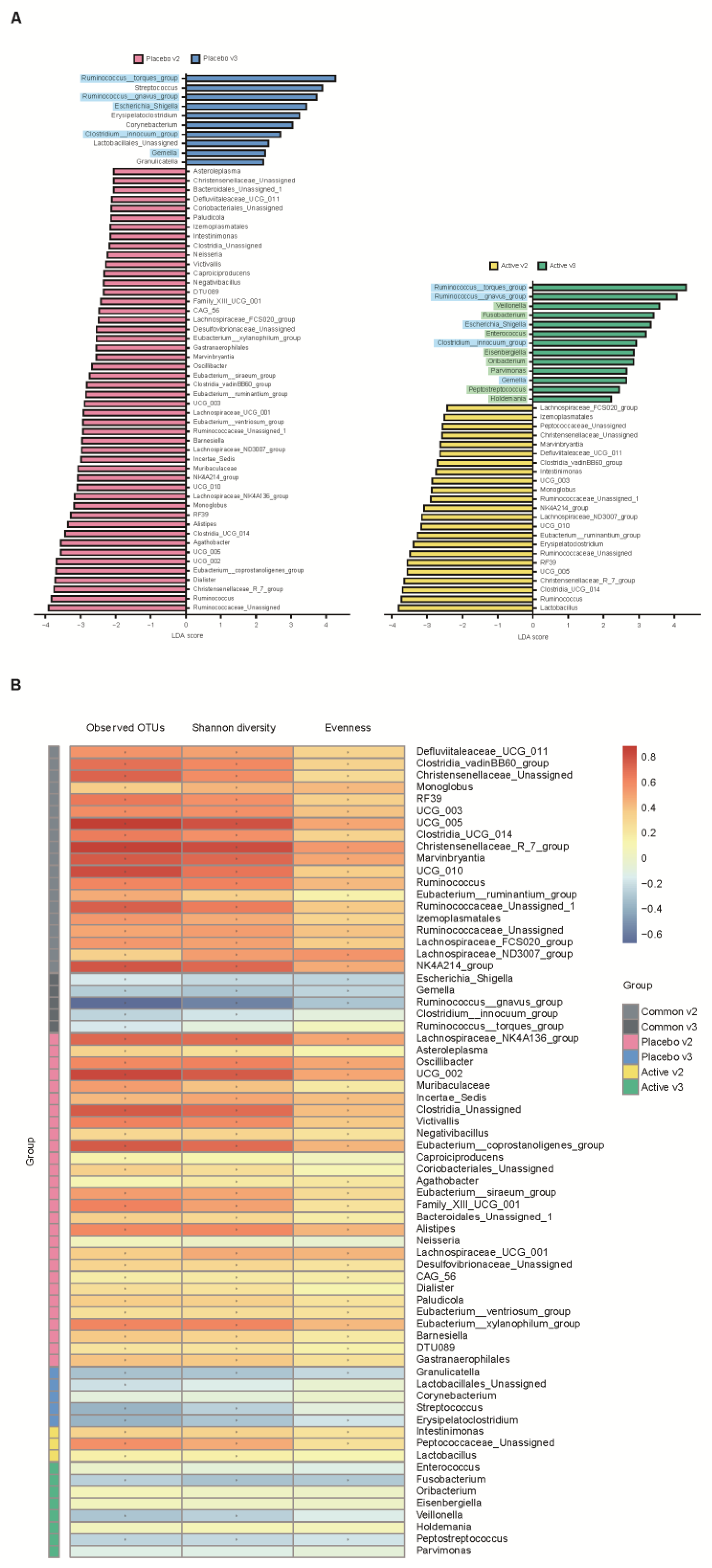
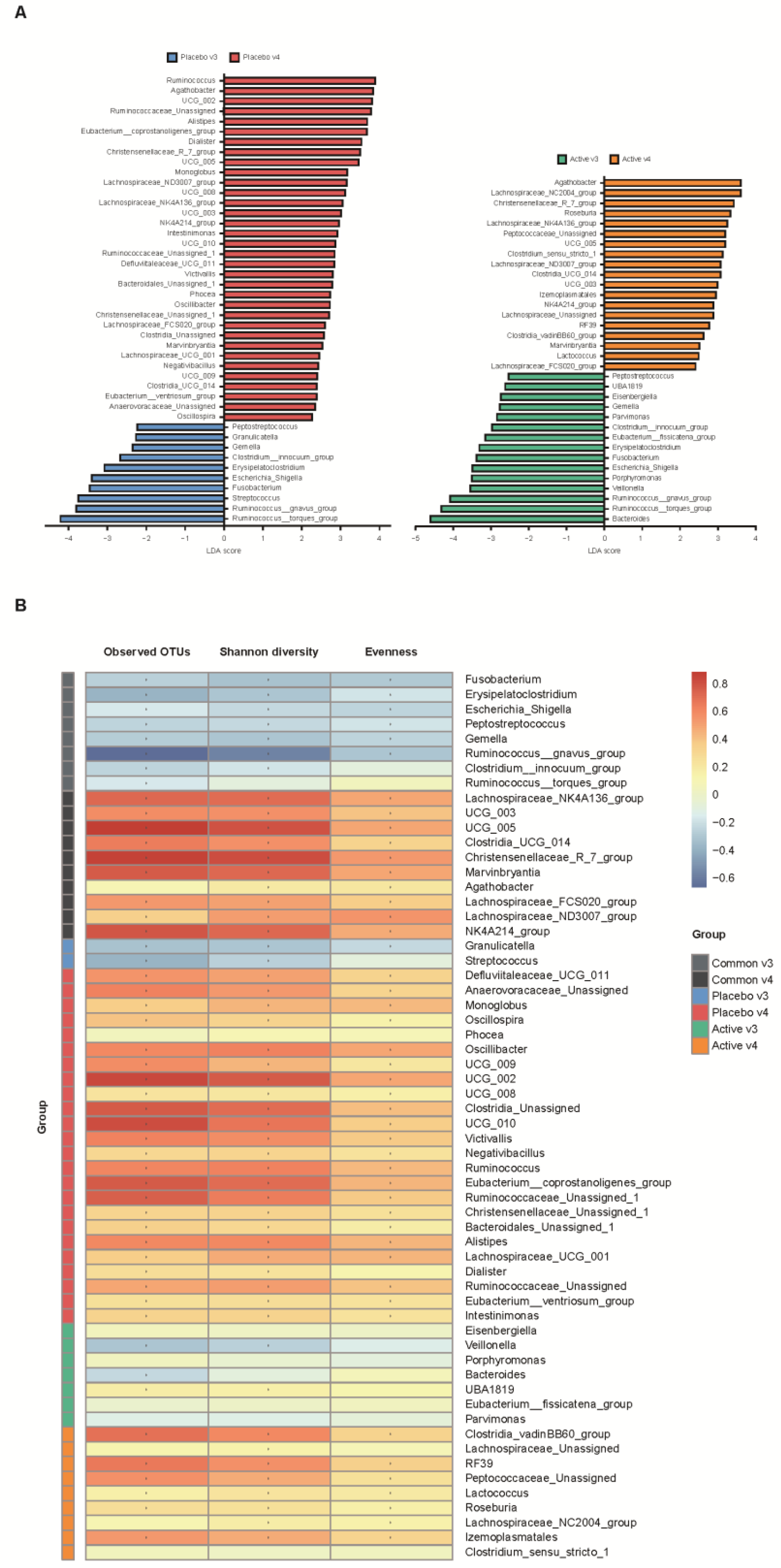
3.4. Specific Gut Microbiota Observed in the Early Stage after Bowel Preparation and Correlation with Microbial Diversity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Inadomi, J.M.; Vijan, S.; Janz, N.K.; Fagerlin, A.; Thomas, J.P.; Lin, Y.V.; Munoz, R.; Lau, C.; Somsouk, M.; El-Nachef, N.; et al. Adherence to colorectal cancer screening: A randomized clinical trial of competing strategies. Arch. Intern. Med. 2012, 172, 575–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Vlugt, M.; Grobbee, E.J.; Bossuyt, P.M.; Bongers, E.; Spijker, W.; Kuipers, E.J.; Lansdorp-Vogelaar, I.; Essink-Bot, M.L.; Spaander, M.C.; Dekker, E. Adherence to colorectal cancer screening: Four rounds of faecal immunochemical test-based screening. Br. J. Cancer 2017, 116, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Denberg, T.D.; Melhado, T.V.; Coombes, J.M.; Beaty, B.L.; Berman, K.; Byers, T.E.; Marcus, A.C.; Steiner, J.F.; Ahnen, D.J. Predictors of nonadherence to screening colonoscopy. J. Gen. Intern. Med. 2005, 20, 989–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, D.A.; Maple, J.T.; Ben-Menachem, T.; Cash, B.D.; Decker, G.A.; Early, D.S.; Evans, J.A.; Fanelli, R.D.; Fukami, N.; Hwang, J.H.; et al. Complications of colonoscopy. Gastrointest. Endosc. 2011, 74, 745–752. [Google Scholar] [CrossRef]
- Ko, C.W.; Riffle, S.; Shapiro, J.A.; Saunders, M.D.; Lee, S.D.; Tung, B.Y.; Kuver, R.; Larson, A.M.; Kowdley, K.V.; Kimmey, M.B. Incidence of minor complications and time lost from normal activities after screening or surveillance colonoscopy. Gastrointest. Endosc. 2007, 65, 648–656. [Google Scholar] [CrossRef]
- Cho, H.S.; Han, D.S.; Park, H.S.; Ahn, S.B.; Byun, T.J.; Kim, T.Y.; Eun, C.S.; Jeon, Y.C.; Sohn, J.H. The incidence of minor complications and patients’ time requirements for colonoscopy. Korean J. Gastrointest. Endosc. 2009, 39, 205–211. [Google Scholar]
- Collatuzzo, G.; Boffetta, P.; Radaelli, F.; Cadoni, S.; Hassan, C.; Frazzoni, L.; Anderloni, A.; Laterza, L.; La Marca, M.; Rogai, F.; et al. Incidence, risk and protective factors of symptoms after colonoscopy. Dig. Liver Dis. 2022, 54, 1698–1705. [Google Scholar] [CrossRef]
- Drago, L.; Toscano, M.; De Grandi, R.; Casini, V.; Pace, F. Persisting changes of intestinal microbiota after bowel lavage and colonoscopy. Eur. J. Gastroenterol. Hepatol. 2016, 28, 532–537. [Google Scholar] [CrossRef]
- Harrell, L.; Wang, Y.; Antonopoulos, D.; Young, V.; Lichtenstein, L.; Huang, Y.; Hanauer, S.; Chang, E. Standard colonic lavage alters the natural state of mucosal-associated microbiota in the human colon. PLoS ONE 2012, 7, e32545. [Google Scholar] [CrossRef]
- Nagata, N.; Tohya, M.; Fukuda, S.; Suda, W.; Nishijima, S.; Takeuchi, F.; Ohsugi, M.; Tsujimoto, T.; Nakamura, T.; Shimomura, A.; et al. Effects of bowel preparation on the human gut microbiome and metabolome. Sci. Rep. 2019, 9, 4042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, C.L.; Allison, G.E.; Grimpen, F.; Pavli, P. Impact of colonoscopy bowel preparation on intestinal microbiota. PLoS ONE 2013, 8, e62815. [Google Scholar] [CrossRef] [Green Version]
- Jalanka, J.; Salonen, A.; Salojarvi, J.; Ritari, J.; Immonen, O.; Marciani, L.; Gowland, P.; Hoad, C.; Garsed, K.; Lam, C.; et al. Effects of bowel cleansing on the intestinal microbiota. Gut 2015, 64, 1562–1568. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, Y.J.; Kwon, H.J.; Jung, K.; Kim, S.E.; Moon, W.; Park, M.I.; Park, S.J. Effect of gut microbiome on minor complications after a colonoscopy. Intest. Res. 2021, 19, 341–348. [Google Scholar] [CrossRef]
- Kim, J.H. The Change of Gut Microbiota after Bowel Preparation and the Effect of Probiotics: A Randomized Controlled, Open-Label Trial. Identifier: NCT03760133. Updated 20 February 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT03760133 (accessed on 9 June 2022).
- Hotel, A.C.P.; Cordoba, A. Health and nutritional properties of probiotics in food including powder milk with live lactic acid bacteria. Prevention 2001, 5, 1–10. [Google Scholar]
- Bermudez-Brito, M.; Plaza-Díaz, J.; Muñoz-Quezada, S.; Gómez-Llorente, C.; Gil, A. Probiotic mechanisms of action. Ann. Nutr. Metab. 2012, 61, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Wieërs, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; Philippart de Foy, J.M.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell Infect. Microbiol. 2019, 9, 454. [Google Scholar] [CrossRef] [Green Version]
- Sanders, M.E.; Lenoir-Wijnkoop, I.; Salminen, S.; Merenstein, D.J.; Gibson, G.R.; Petschow, B.W.; Nieuwdorp, M.; Tancredi, D.J.; Cifelli, C.J.; Jacques, P.; et al. Probiotics and prebiotics: Prospects for public health and nutritional recommendations. Ann. N. Y. Acad. Sci. 2014, 1309, 19–29. [Google Scholar] [CrossRef]
- Hungin, A.P.S.; Mitchell, C.R.; Whorwell, P.; Mulligan, C.; Cole, O.; Agréus, L.; Fracasso, P.; Lionis, C.; Mendive, J.; Philippart de Foy, J.M.; et al. Systematic review: Probiotics in the management of lower gastrointestinal symptoms—An updated evidence-based international consensus. Aliment. Pharmacol. Ther. 2018, 47, 1054–1070. [Google Scholar] [CrossRef] [Green Version]
- Su, G.L.; Ko, C.W.; Bercik, P.; Falck-Ytter, Y.; Sultan, S.; Weizman, A.V.; Morgan, R.L. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 697–705. [Google Scholar] [CrossRef]
- Labenz, J.; Borkenstein, D.P.; Heil, F.J.; Madisch, A.; Tappe, U.; Schmidt, H.; Terjung, B.; Klymiuk, I.; Horvath, A.; Gross, M.; et al. Application of a multispecies probiotic reduces gastro-intestinal discomfort and induces microbial changes after colonoscopy. Front. Oncol. 2023, 12, 1078315. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Murakami, M.; Nakao, K.; Asahara, T.; Nomoto, K.; Tsunoda, A. Randomized clinical trial of the influence of mechanical bowel preparation on faecal microflora in patients undergoing colonic cancer resection. Br. J. Surg. 2010, 97, 1791–1797. [Google Scholar] [CrossRef]
- Ringel, Y.; Maharshak, N.; Ringel-Kulka, T.; Wolber, E.A.; Sartor, R.B.; Carroll, I.M. High throughput sequencing reveals distinct microbial populations within the mucosal and luminal niches in healthy individuals. Gut Microbes 2015, 6, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Tong, C.; Qian, X.; Wang, H.; Wang, Y. Mechanical Bowel Preparation Is a Risk Factor for Postoperative Delirium as It Alters the Gut Microbiota Composition: A Prospective Randomized Single-Center Study. Front. Aging Neurosci. 2022, 14, 847610. [Google Scholar] [CrossRef] [PubMed]
- Scheiman, J.; Luber, J.M.; Chavkin, T.A.; MacDonald, T.; Tung, A.; Pham, L.-D.; Wibowo, M.C.; Wurth, R.C.; Punthambaker, S.; Tierney, B.T. Meta-omics analysis of elite athletes identifies a performance-enhancing microbe that functions via lactate metabolism. Nat. Med. 2019, 25, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Torres-Maravilla, E.; Boucard, A.-S.; Mohseni, A.H.; Taghinezhad-S, S.; Cortes-Perez, N.G.; Bermúdez-Humarán, L.G. Role of gut microbiota and probiotics in colorectal cancer: Onset and progression. Microorganisms 2021, 9, 1021. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 51) | Active (n = 26) | Placebo (n = 25) | p-Value | |
|---|---|---|---|---|
| Age (years) | 53.9 ± 8.0 | 54.4 ± 7.8 | 53.1 ± 8.3 | 0.589 |
| Sex | 0.773 | |||
| Male | 19 (37.3) | 9 (34.6) | 10 (40.0) | |
| Female | 32 (62.7) | 17 (65.4) | 15 (60.0) | |
| Height (cm) | 163.1 ± 9.0 | 162.7 ± 8.9 | 163.5 ± 9.3 | 0.771 |
| Weight (kg) | 66.6 ± 14.1 | 66.6 ± 13.1 | 66.7 ± 15.3 | 0.989 |
| BMI (kg/m2) | 24.9 ± 4.0 | 25.0 ± 3.7 | 24.8 ± 4.3 | 0.798 |
| Alcohol history | 15 (29.4) | 7 (26.9) | 8 (32.0) | 0.894 |
| Current smoker | 6 (11.8) | 4 (15.3) | 2 (8.0) | 0.674 |
| Co-morbidities | 0.450 | |||
| Diabetes mellitus | 3 (5.9) | 1 (3.8) | 2 (8.0) | |
| Hypertension | 11 (21.6) | 6 (23.2) | 5 (20.0) | |
| Dyslipidemia | 3 (5.9) | 0 (0.0) | 3 (12.0) | |
| Ischemic heart disease | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| Dietary habits | 0.892 | |||
| Vegetarian | 10 (19.6) | 6 (23.2) | 4 (16.0) | |
| Meat eater † | 4 (7.8) | 2 (7.7) | 2 (8.0) | |
| Eat evenly ¶ | 37 (72.6) | 18 (69.1) | 19 (76.0) | |
| Stool frequency | 0.740 | |||
| Low (≤2 times/week) | 2 (3.9) | 2 (7.7) | 0 (0.0) | |
| Normal (1–2 times/1–2 days) | 47 (92.2) | 23 (88.5) | 24 (96.0) | |
| High (≥3 times/day) | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| Stool consistency (Bristol stool scale) | 1.0 | |||
| 1–2 | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| 3–5 | 47 (92.2) | 24 (92.4) | 23 (92.0) | |
| 6–7 | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| Reason for colonoscopy | 1.0 | |||
| Screening | 48 (94.1) | 24 (92.3) | 24 (96.0) | |
| Post-polypectomy surveillance | 3 (5.9) | 2 (7.7) | 1 (4.0) | |
| Previous experience of colonoscopy | 20 (39.2) | 10 (38.5) | 10 (40.0) | 0.910 |
| Previous experience of polypectomy | 43 (84.3) | 22 (84.6) | 21 (84.0) | 1.0 |
| Bowel preparation | 1.0 | |||
| Good/fair | 48 (94.1) | 24 (92.3) | 24 (96.0) | |
| Poor | 3 (5.9) | 2 (7.7) | 1 (4.0) | |
| Findings of colonoscopy | 0.902 | |||
| Normal | 12 (23.5) | 6 (23.1) | 6 (20.0) | |
| Polyp | 32 (62.8) | 17 (65.4) | 15 (60.0) | |
| Cancer | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Diverticulosis | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| Hemorrhoid | 5 (9.8) | 2 (7.7) | 3 (12.0) | |
| Colon polyp | ||||
| Size (≥1 cm) | 2 (3.9) | 0 (0.0) | 2 (11.8) | 0.485 |
| Resection | 0.776 | |||
| Cold forceps polypectomy | 23 (45.1) | 13 (50.0) | 11 (44.0) | |
| Cold snare polypectomy | 8 (15.7) | 4 (15.4) | 4 (16.0) |
| Overall (n = 51) | Active (n = 26) | Placebo (n = 25) | p-Value | |
|---|---|---|---|---|
| Decreased body weight after bowel preparation (≥2 kg) | 11 (21.6) | 7 (26.9) | 4 (16.0) | 0.499 |
| Post-colonoscopy complications | 17 (33.3) | 9 (34.6) | 8 (32.0) | 0.843 |
| Type | 0.783 | |||
| Abdominal pain | 4 (7.8) | 2 (7.7) | 2 (8.0) | |
| Abdominal pain/Bloating | 2 (3.9) | 1 (3.8) | 1 (4.0) | |
| Bloating | 8 (15.7) | 5 (19.2) | 3 (12.0) | |
| Bloating/Constipation | 1 (2.0) | 1 (3.8) | 0 (0.0) | |
| Constipation | 0 (3.9) | 0 (0.0) | 2 (8.0) | |
| Hemorrhage | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Perforation | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Onset timing | 0.694 | |||
| Day of colonoscopy | 12 (23.5) | 6 (23.1) | 6 (24.0) | |
| 1st day after colonoscopy | 4 (7.8) | 3 (11.5) | 1 (4.0) | |
| 2nd day after colonoscopy | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 3rd day after colonoscopy | 1 (2.0) | 0 (0.0) | 1 (4.0) | |
| Frequency | 0.835 | |||
| 1 time/day | 6 (11.8) | 3 (11.5) | 3 (12.0) | |
| 2 times/day | 6 (11.8) | 4 (15.4) | 2 (8.0) | |
| ≥3 times/day | 5 (9.8) | 2 (7.7) | 3 (12.0) | |
| Duration | 0.025 | |||
| <30 min | 8 (15.7) | 7 (26.9) | 1 (4.0) | |
| 1–2 h | 4 (7.8) | 1 (3.8) | 3 (12.0) | |
| ≥24 h | 5 (9.8) | 1 (3.8) | 4 (16.0) | |
| Severity score (VAS) | 3.6 ± 2.2 | 3.1 ± 1.6 | 4.1 ± 2.6 | 0.349 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Factor | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age | ||||||
| <55 years | 1 | |||||
| ≥55 years | 0.57 | 0.13–2.43 | 0.444 | |||
| Sex | ||||||
| Male | 1 | |||||
| Female | 1.15 | 0.25–5.30 | 0.854 | |||
| BMI | ||||||
| <25 | 1 | |||||
| ≥25 | 0.27 | 0.05–1.47 | 0.130 | |||
| Dietary habit | ||||||
| Eat evenly | 1 | |||||
| Vegetarian | 1.48 | 0.24–8.92 | 0.671 | |||
| Meat eater | 1.72 | 0.15–19.49 | 0.661 | |||
| Co-morbidities | ||||||
| None | 1 | |||||
| Present | 0.30 | 0.56–1.62 | 0.162 | |||
| Polyp removal | 0.72 | 0.17–3.11 | 0.661 | |||
| Group | ||||||
| Placebo | 1 | |||||
| Active | 0.22 | 0.04–1.21 | 0.082 | 0.13 | 0.02–0.69 | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, D.; Choi, Y.J.; Son, M.Y.; Moon, W.; Park, S.J.; Lim, S.; Kim, J.H. Benefits of Probiotic Pretreatment on the Gut Microbiota and Minor Complications after Bowel Preparation for Colonoscopy: A Randomized Double-Blind, Placebo-Controlled Pilot Trial. Nutrients 2023, 15, 1141. https://doi.org/10.3390/nu15051141
Son D, Choi YJ, Son MY, Moon W, Park SJ, Lim S, Kim JH. Benefits of Probiotic Pretreatment on the Gut Microbiota and Minor Complications after Bowel Preparation for Colonoscopy: A Randomized Double-Blind, Placebo-Controlled Pilot Trial. Nutrients. 2023; 15(5):1141. https://doi.org/10.3390/nu15051141
Chicago/Turabian StyleSon, Dooheon, Youn Jung Choi, Min Young Son, Won Moon, Seun Ja Park, Sanghyun Lim, and Jae Hyun Kim. 2023. "Benefits of Probiotic Pretreatment on the Gut Microbiota and Minor Complications after Bowel Preparation for Colonoscopy: A Randomized Double-Blind, Placebo-Controlled Pilot Trial" Nutrients 15, no. 5: 1141. https://doi.org/10.3390/nu15051141
APA StyleSon, D., Choi, Y. J., Son, M. Y., Moon, W., Park, S. J., Lim, S., & Kim, J. H. (2023). Benefits of Probiotic Pretreatment on the Gut Microbiota and Minor Complications after Bowel Preparation for Colonoscopy: A Randomized Double-Blind, Placebo-Controlled Pilot Trial. Nutrients, 15(5), 1141. https://doi.org/10.3390/nu15051141