
Changes in Tryptophan Metabolism on Serotonin and Kynurenine Pathways in Patients with Irritable Bowel Syndrome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnostic Procedures
2.3. Laboratory Tests
2.4. Nutritional Intervention
2.5. Ethical Issues
2.6. Statistical Analysis
3. Results
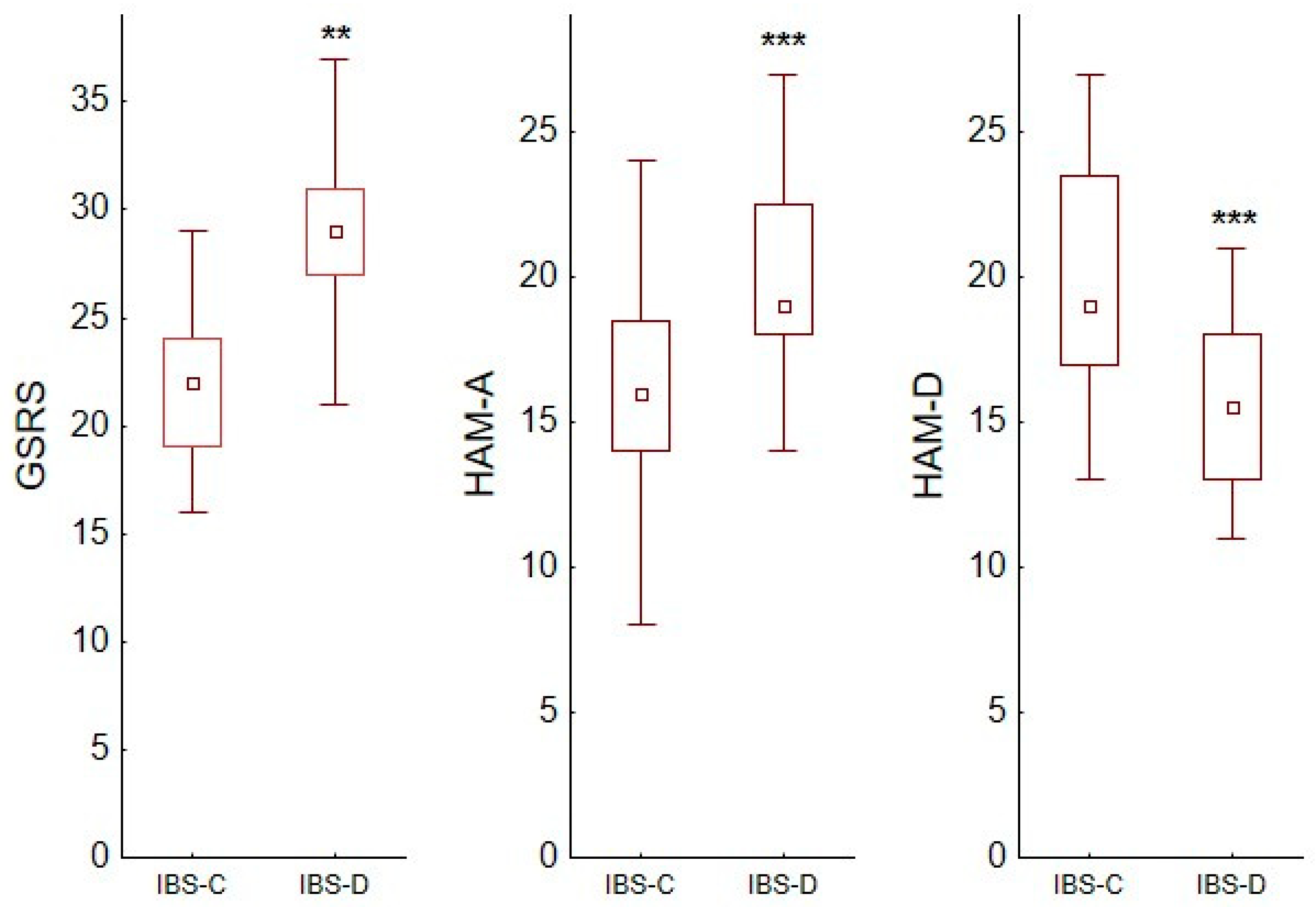
3.1. Comparison of Irritable Bowel Syndrome Patients with Controls
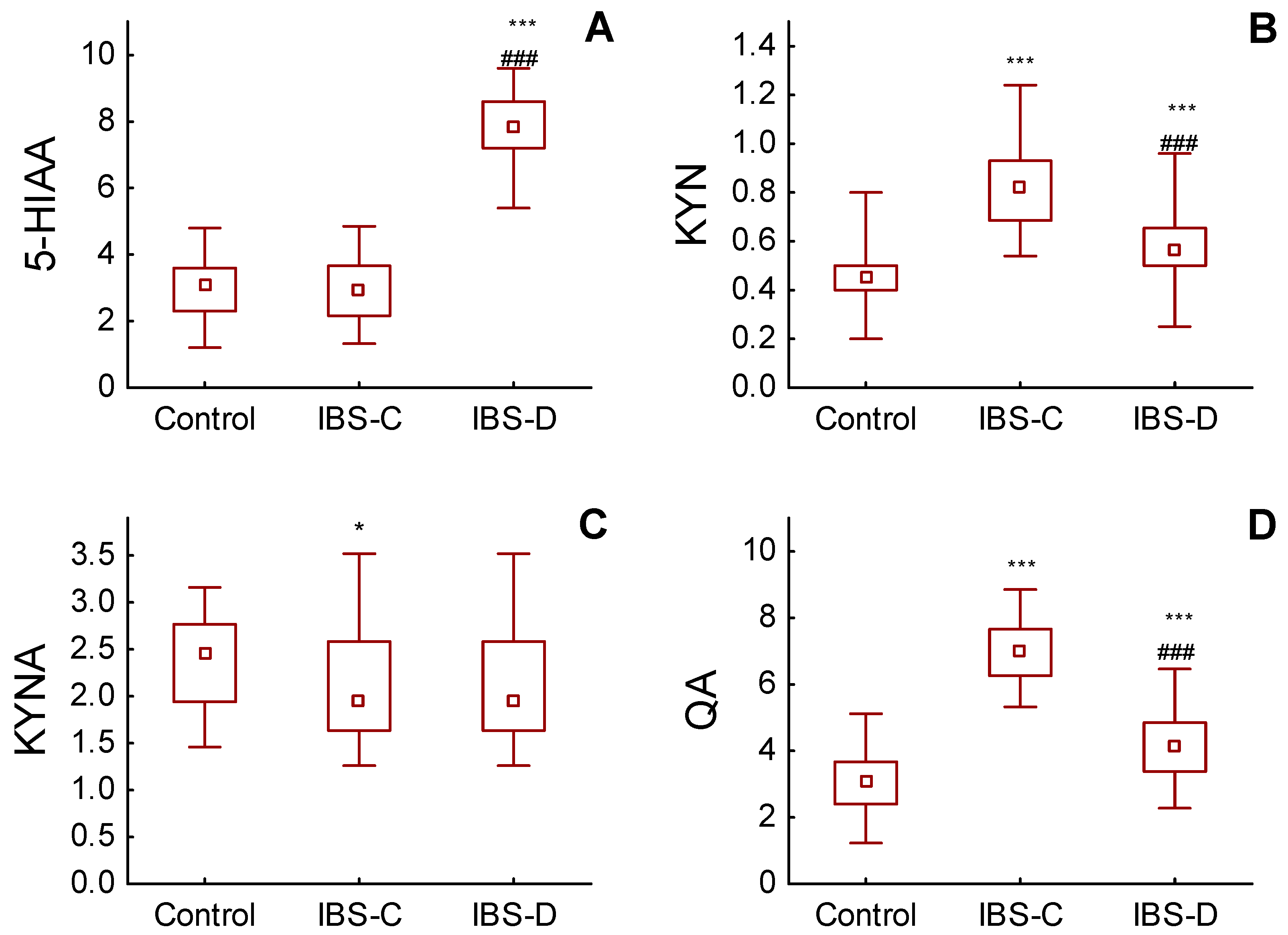
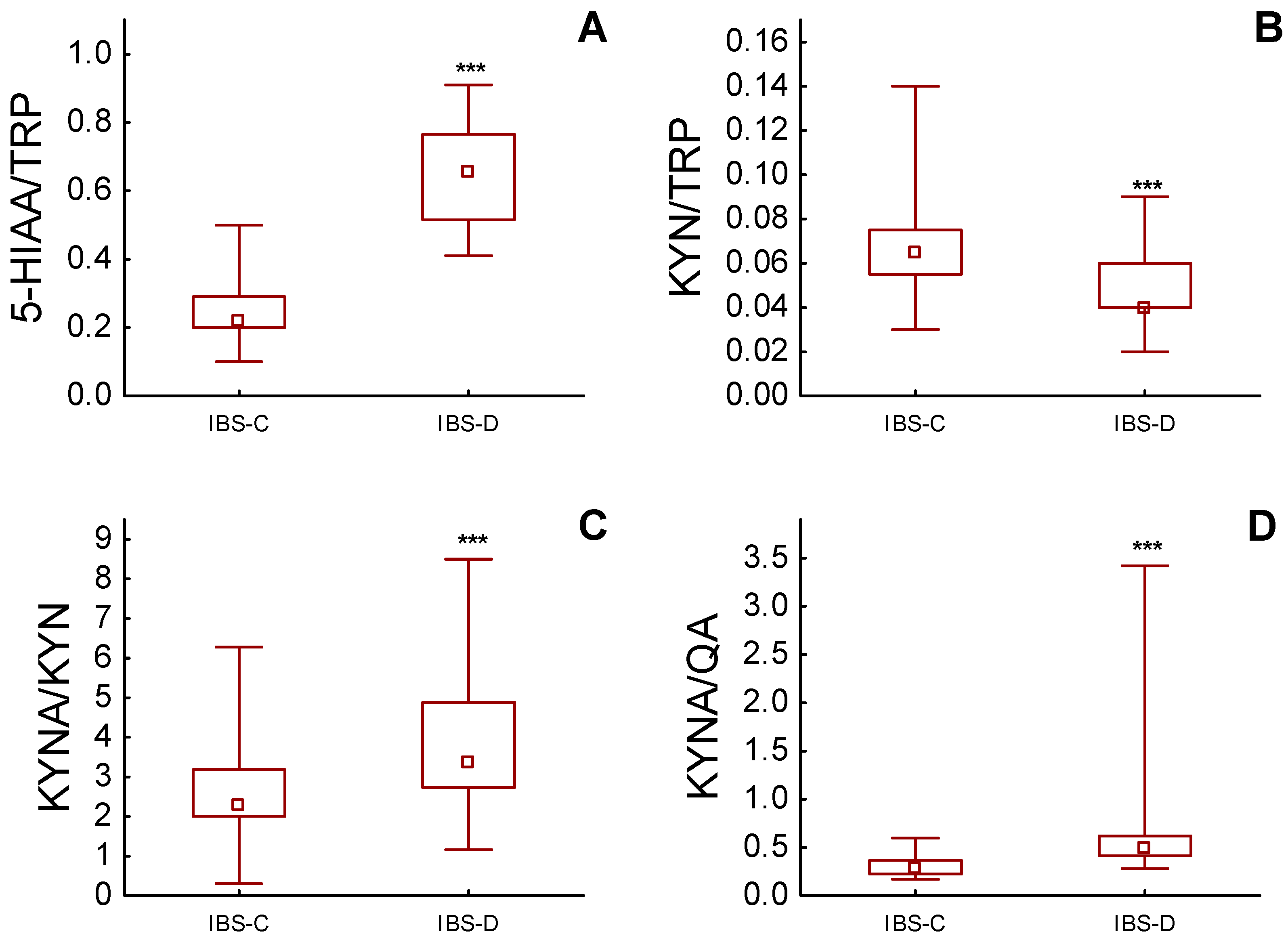
3.2. Urinary Excretion of TRP and Its Metabolites
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lacy, B.E.; Patel, N.K. Rome Criteria and a Diagnostic Approach to Irritable Bowel Syndrome. J. Clin. Med. 2017, 6, 99. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology 2016, 150, 1262–1279.e2. [Google Scholar] [CrossRef] [Green Version]
- Bassotti, G. Irritable Bowel Syndrome: A Multifaceted World Still to Discover. J. Clin. Med. 2022, 11, 4103. [Google Scholar] [CrossRef]
- Ferreira, A.I.; Garrido, M.; Castro-Pocas, F. Irritable Bowel Syndrome: News from an Old Disorders. GE Port. J. Gastroenterol. 2020, 27, 255–268. [Google Scholar] [CrossRef]
- Gros, M.; Gros, B.; Mesonero, J.E.; Latorre, E. Neurotransmitter Dysfunction in Irritable Bowel Syndrome: Emerging Approaches for Management. J. Clin. Med. 2021, 10, 3429. [Google Scholar] [CrossRef]
- Guzel, T.; Mirowska-Guzel, D. The Role of serotonin Neurotransmission in Gastrointestinal Tract. Molecules 2022, 27, 1680. [Google Scholar] [CrossRef]
- Jenkins, T.A.; Nguyen, J.C.D.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int. J. Trypt. Res. IJTR 2017, 15, 1178646917691938. [Google Scholar] [CrossRef] [Green Version]
- Palego, L.; Betti, L.; Rossi, A.; Giannaccini, G. Tryptophan Biochemistry: Structural, Nutritional, Metabolic, and Medical Aspects in Humans. J. Am. Acids 2016, 2016, 8952520. [Google Scholar] [CrossRef] [Green Version]
- Ruddick, J.P.; Evans, A.K.; Nutt, D.J.; Lightman, S.L.; Rook, G.A.; Lowry, C.A. Tryptophan Metabolism in the Central Nervous System: Medical Implications. Exp. Rev. Mol. Med. 2006, 8, 1–27. [Google Scholar] [CrossRef]
- Braidy, N.; Grant, R.; Adams, S.; Brew, B.J.; Guillemin, G.J. Mechanism for Quinolinic Acid Cytotoxicity in Human Astrocytes and Neurons. Neurotox. Res. 2009, 16, 77–86. [Google Scholar] [CrossRef]
- Colle, R.; Masson, P.; Verstuyft, C.; Feve, B.; Werner, E.; Boursier-Neyret, C.; Walther, B.; David, D.J.; Boniface, B.; Falissard, B.; et al. Peripheral tryptophan, serotonin, kynurenine, and their metabolites in major depression: A case control study. Psych. Clin. Neurosc. 2020, 74, 112–117. [Google Scholar] [CrossRef]
- Arnone, D.; Saraykar, S.; Salem, H.; Teixeira, A.L.; Dantzer, R.; Selvaraj, S. Role of Kynurenine Pathway and Its Metabolites in Mood Disorders: A Systematic Review and Meta-Analysis of Clinical Studies. Neurosc. Biobeh. Rev. 2018, 92, 477–485. [Google Scholar] [CrossRef]
- Miura, H.; Ozaki, N.; Sawada, M.; Isobe, K.; Ohta, T.; Nagatsu, T. A Link between Stress and Depression: Shifts in the Balance between the Kynurenine and Serotonin Pathways of Tryptophan Metabolism and the Etiology and Pathophysiology of Depression. Stress 2008, 11, 198–209. [Google Scholar] [CrossRef]
- Mawe, G.M.; Coates, M.D.; Moses, P.L. Review article: Intestinal serotonin signalling in irritable bowel syndrome. Alimen. Pharm. Therap. 2006, 23, 1067–1076. [Google Scholar] [CrossRef]
- Sikander, A.; Rana, S.V.; Prasad, K.K. Role of serotonin in gastrointestinal motility and irritable bowel syndrome. Clin. Chim. Acta 2009, 403, 47–55. [Google Scholar] [CrossRef]
- Gerson, M.D.; Tack, J. The serotonin signalling system: From basic understanding to drug development for functional GI disorders. Gastroenterology 2007, 132, 397–414. [Google Scholar] [CrossRef]
- Kim, D.Y.; Camilleri, M. Serotonin: A mediator of the brain-gut connection. Am. J. Gastroenterol. 2000, 95, 2698–2709. [Google Scholar] [CrossRef]
- Christmas, D.M.; Badawy, A.; Hince, D.; Davies, S.; Probert, C.S.J.; Creed, T.; Smithson, J.E.; Afzal, M.; Nutt, D.J.; Potokar, J.P. Increased Serum Free Tryptophan in Patients with Diarrhea-Predominant Irritable Bowel Syndrome. Nutr. Res. 2010, 30, 678–688. [Google Scholar] [CrossRef]
- Takakura, W.; Pimentel, M. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome–An Update. Front. Psychiatry 2020, 11, 664. [Google Scholar] [CrossRef]
- Ljotsson, B.; Jones, M.; Talley, N.J.; Kjellstrom, L.; Agreus, L.; Andreasson, A. Discriminant and convergent validity of the GSRS-IBS symptom severity measure for irritable bowel syndrome: A population study. United Eur. Gastroenterol. J. 2020, 8, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Carrozzino, D.; Patierno, C.; Fava, G.A.; Guidi, J. The Hamilton Rating Scales for Depression: A Critical Review of Clinimetric Properties of Different Versions. Psychother. Psychosom. 2020, 89, 133–150. [Google Scholar] [CrossRef]
- Beacroft, C.P.; Perrett, D.; Farthing, M.J. Postprandial plasma 5-hydroxytryptamine in diarrhoea predominant irritable bowel syndrome. Gut 1998, 42, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Houghton, L.A.; Atkinson, w.; Lockhart, C.; Whorwell, P.J.; Keevil, B. Sigmoid-colonic motility in healthy and irritable bowel syndrome: A role for 5-hydroxytryptamine. Neurogastroenterol. Motil. 2007, 19, 724–731. [Google Scholar] [CrossRef]
- Moskwa, A.; Chojnacki, J.; Wiśniewska-Jarosińska, M.; Stec-Michalska, K.; Szadkowski, K.; Śmigielski, J.; Chojnacki, C. Serum serotonin concentration and urine 5-hydroxyindole acetic acid excretion in patients with irritable bowel syndrome. Pol. Merkur. Lek. 2007, 22, 366–368. [Google Scholar] [PubMed]
- Dunlop, S.P.; Coleman, N.S.; Blackshaw, E.; Perkins, A.C.; Singh, G.; Marsden, C.A.; Spiller, R.C. Abnormalities of 5-hydroxytryptamine metabolism in irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2005, 3, 349–357. [Google Scholar] [CrossRef]
- Atkinson, W.; Lockhart, S.; Whorwell, P.J.; Keevil, B.; Houghton, L.A. Altered 5- hydroxytryptamine signalling in patients with constipation- and diarrhoea irritable bowel syndrome. Gastroenterology 2006, 130, 34–43. [Google Scholar] [CrossRef]
- Spiller, R. Recent advances in understanding the role of serotonin in gastrointestinal motility in functional bowel disorders: Alteration in 5-HT signalling and metabolism in human disease. Neurogastroenterol. Motil. 2007, 19, 25–31. [Google Scholar] [CrossRef]
- El-Salhy, M.; Wendelbo, I.H.; Gundersen, D. Reduced chromogranin A cell density in the ileum of patients with irritable bowel syndrome. Mol. Med. Rep. 2013, 7, 1241–1244. [Google Scholar] [CrossRef] [Green Version]
- Coates, M.D.; Mahoney, C.R.; Linden, D.R.; Sampson, J.E.; Chen, J.; Blaszyk, H.; Crowell, M.D.; Sharkey, K.A.; Gershon, M.D.; Mawe, G.M.; et al. Molecular defects in mucosal serotonin and decreased serotonin reuptake transporter in ulcerative colitis and irritable bowel syndrome. Gastroenterology 2004, 126, 1657–1664. [Google Scholar] [CrossRef]
- Miwa, J.; Echizen, H.; Matsueda, K.; Umeda, N. Patients with constipation-predominant irritable bowel syndrome (IBS) may have elevated serotonin concentrations in colonic mucosa as compared with diarrhoea-predominant patients and subjects with normal bowel habits. Digestion 2001, 53, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.Y.; Huang, S.G.; Zhang, H.Y.; Ye, H.; Chi, H.G.; Zou, Y.; Lv, R.X.; Zheng, X.B. Comparison of 5-hydroxytryptophan signalling pathway characteristics in diarrhoea-predominant irritable bowel syndrome and ulcerative colitis. World J. Gastroenterol. 2016, 22, 3451–3459. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Błońska, A.; Kaczka, A.; Chojnacki, J.; Stępień, A.; Gąsiorowska, A. Evaluation of serotonin and dopamine secretion and metabolism in patients with irritable bowel syndrome. Pol. Arch. Int. Med. 2018, 128, 711–713. [Google Scholar] [CrossRef] [Green Version]
- Chojnacki, C.; Popławski, T.; Gasiorowska, A.; Chojnacki, J.; Blasiak, J. Serotonin in the Pathogenesis of Lymphocytic Colitis. J. Clin. Med. 2021, 10, 285. [Google Scholar] [CrossRef]
- Thijssen, A.Y.; Mujagic, Z.; Jonkers, D.M.A.E.; Ludidi, S.; Keszthelyi, D.; Hesselink, M.A.; Clemens, C.H.M.; Conchillo, J.M.; Kruimel, J.W.; Masclee, A.A.M. Alterations in serotonin metabolism in irritable bowel syndrome. Aliment. Pharm. Therap. 2016, 43, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.; Fitzgerald, P.; Cryan, J.F.; Cassidy, E.M.; Quigley, E.M.; Dinan, T.G. Tryptophan Degradation in Irritable Bowel Syndrome: Evidence of Indoleamine 2,3-Dioxygenase Activation in a Male Cohort. BMC Gastroenterol. 2009, 9, 6. [Google Scholar] [CrossRef] [Green Version]
- Heitkemper, M.M.; Han, C.J.; Jarrett, M.E.; Gu, H.; Djukovic, D.; Shulman, R.J.; Raftery, D.; Henderson, W.A.; Cain, K.C. Serum Tryptophan Metabolite Levels During Sleep in Patients With and Without Irritable Bowel Syndrome (IBS). Biol. Res. Nurs. 2015, 18, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Keszthelyi, D.; Troost, F.J.; Jonkers, D.M.; Kruimel, J.W.; Leue, C.; Masclee, A.A. Decreased Levels of Kynurenic Acid in the Intestinal Mucosa of IBS Patients: Relation to Serotonin and Psychological State. J. Psychosom. Res. 2013, 74, 501–504. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, P.; Cassidy Eugene, M.; Clarke, G.; Scully, P.; Barry, S.; Quigley Eamonn, M.M.; Shanahan, F.; Cryan, J.; Dinan Timothy, G. Tryptophan Catabolism in Females with Irritable Bowel Syndrome: Relationship to Interferon-Gamma, Severity of Symptoms and Psychiatric Co-Morbidity. Neurogastroenterol. Motil. 2008, 20, 1291–1297. [Google Scholar] [CrossRef]
- Chojnacki, C.; Konrad, P.; Błońska, A.; Mędrek-Socha, M.; Przybyłowska-Sygut, K.; Chojnacki, J.; Popławski, T. Altered Tryptophan Metabolism on the Kynurenine Pathway I Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients 2022, 14, 3217. [Google Scholar] [CrossRef]
- Fakudo, S. Stress and visceral pain: Focusing on irritable bowel syndrome. Pain 2013, 154 (Suppl. S1), S63–S70. [Google Scholar] [CrossRef]
- Aziz, M.N.M.; Kumar, J.; Nawawi, K.N.M.; Ali, R.A.R.; Mohtar, N.M. Irritable Bowel Syndrome, Depression, and Neurodegeneration: A Bidirectional Communication from Gut to Brain. Nutrients 2021, 13, 3061. [Google Scholar] [CrossRef]
- Tran, H.; Sagi, V.; Jarrett, S.; Palzer, E.F.; Badgaiyan, R.D.; Gupta, K. Diet and companionship modulate pain via a serotonergic mechanism. Sci. Rep. 2021, 11, 2330. [Google Scholar] [CrossRef]
- Black, C.J.; Ford, A.C. Best management of irritable bowel syndrome. Frontline Gastroenterol. 2021, 12, 303–315. [Google Scholar] [CrossRef]
- O’Mahony, S.M.; Clarke, G.; Borre, Y.E.; Dinan, T.G.; Cryan, J.F. Serotonin, tryptophan metabolism and brain-gut-microbiome axis. Behav. Brain Res. 2015, 277, 32–48. [Google Scholar] [CrossRef]
- Strandwitz, P. Neurotransmitters modulation by the gut microbiota. Brain Res. 2018, 163, 128–133. [Google Scholar] [CrossRef]
- Zhang, B.; Jiang, M.; Zhao, J.; Song, Y.; Du, W.; Shi, J. The Mechanism Underlying the Influence of Indole-3-Propionic Acid: A Relevance to Metabolic Disorders. Front. Endocrinol. 2022, 13, 841703. [Google Scholar] [CrossRef]
- Lamas, B.; Richard, M.L.; Leducq, V.; Pham, H.-P.; Michel, M.-L.; Da Costa, G.; Bridonneau, C.; Jegou, S.; Hoffmann, T.W.; Natividad, J.M.; et al. CARD9 Impacts Colitis by Altering Gut Microbiota Metabolism of Tryptophan into Aryl Hydrocarbon Receptor Ligands. Nat. Med. 2016, 22, 598–605. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Feature | Controls (n = 40) | IBS-C (n = 40) | IBS-D (n = 40) |
|---|---|---|---|
| Age (years) | 42.9 ± 10.2 | 44.5 ± 10.9 | 43.7 ± 12.3 |
| Gender M/F | 8/32 | 9/31 | 10/30 |
| BMI (kg/m2) | 23.2 ± 1.2 | 24.4 ± 2.3 | 23.2 ± 3.1 |
| GFR (mL/min) | 99.2 ± 4.3 | 92.2 ± 6.9 | 96.5 ± 4.8 |
| ALT (µ/L) | 14.5 ± 2.8 | 17.8 ± 3.6 | 16.1 ± 4.2 |
| AST (µ/L) | 12.9 ± 1.9 | 13.2 ± 2.4 | 14.5 ± 2.5 |
| CRP (mg/L) | 2.54 ± 0.8 | 3.1 ± 1.7 | 4.2 ± 1.9 |
| FC (µg/g) | 19.8 ± 8.6 | 28,6 ± 18.8 | 31.9 ± 18.9 |
| TRP (mg daily) | 1329 ± 178 | 1262 ± 139 | 1286 ± 155 |
| Feature | Controls | IBS-C | IBS-D | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M | IQR | M | IQR | M | IQR | ||||
| TRP (mg/gCr) | 12.70 | 10.90 | 14.85 | 12.25 | 10.10 | 14.20 | 12.25 | 10.10 | 14.20 |
| 5HIAA (mg/gCr) | 3.10 | 2.30 | 3.60 | 2.98 | 2.16 | 3.67 | 7.85 | 7.20 | 8.60 |
| 5-HIAA/TRP | 0.22 | 0.17 | 0.28 | 0.23 | 0.20 | 0.29 | 0.66 | 0.52 | 0.77 |
| KYN (mg/gCr) | 0.45 | 0.40 | 0.50 | 0.82 | 0.69 | 0.93 | 0.57 | 0.50 | 0.66 |
| KYN/TRP | 0.03 | 0.03 | 0.04 | 0.07 | 0.06 | 0.08 | 0.04 | 0.04 | 0.06 |
| KYNA (mg/gCr) | 2.45 | 1.94 | 2.77 | 1.94 | 1.64 | 2.59 | 2.01 | 1.64 | 2.61 |
| KYNA/KYN | 5.93 | 3.96 | 6.57 | 2.31 | 2.01 | 3.19 | 3.44 | 2.76 | 4.98 |
| QA (mg/gCr) | 3.13 | 2.40 | 3.67 | 6.98 | 6.26 | 7.67 | 4.15 | 3.38 | 4.86 |
| KYNA/QA | 0.79 | 0.62 | 1.06 | 0.28 | 0.23 | 0.37 | 0.53 | 0.40 | 0.62 |
| Tryptophan Metabolites | GSRS | HAM-A | HAM-D | |||
|---|---|---|---|---|---|---|
| IBS-C | IBS-D | IBS-C | IBS-D | IBS-C | IBS-D | |
| 5-HIAA | 0.029 | 0.4498 ** | −0.0344 | 0.5064 *** | 0.2016 | 0.2545 |
| KYN | 0.0582 | 0.1829 | −0.1115 | −0.1706 | 0.0518 | −0.0525 |
| KYNA | 0.1526 | −0.2314 | 0.2004 | 0.1378 | −0.3609 * | 0.0771 |
| QA | 0.0328 | 0.0081 | −0.0326 | 0.038 | 0.8200 *** | 0.1976 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chojnacki, C.; Błońska, A.; Konrad, P.; Chojnacki, M.; Podogrocki, M.; Poplawski, T. Changes in Tryptophan Metabolism on Serotonin and Kynurenine Pathways in Patients with Irritable Bowel Syndrome. Nutrients 2023, 15, 1262. https://doi.org/10.3390/nu15051262
Chojnacki C, Błońska A, Konrad P, Chojnacki M, Podogrocki M, Poplawski T. Changes in Tryptophan Metabolism on Serotonin and Kynurenine Pathways in Patients with Irritable Bowel Syndrome. Nutrients. 2023; 15(5):1262. https://doi.org/10.3390/nu15051262
Chicago/Turabian StyleChojnacki, Cezary, Aleksandra Błońska, Paulina Konrad, Marcin Chojnacki, Marcin Podogrocki, and Tomasz Poplawski. 2023. "Changes in Tryptophan Metabolism on Serotonin and Kynurenine Pathways in Patients with Irritable Bowel Syndrome" Nutrients 15, no. 5: 1262. https://doi.org/10.3390/nu15051262
APA StyleChojnacki, C., Błońska, A., Konrad, P., Chojnacki, M., Podogrocki, M., & Poplawski, T. (2023). Changes in Tryptophan Metabolism on Serotonin and Kynurenine Pathways in Patients with Irritable Bowel Syndrome. Nutrients, 15(5), 1262. https://doi.org/10.3390/nu15051262