
Prospective Study of Diet Quality and the Risk of Dementia in the Oldest Old

 , ,
, ,
Abstract
:1. Introduction
2. Methods
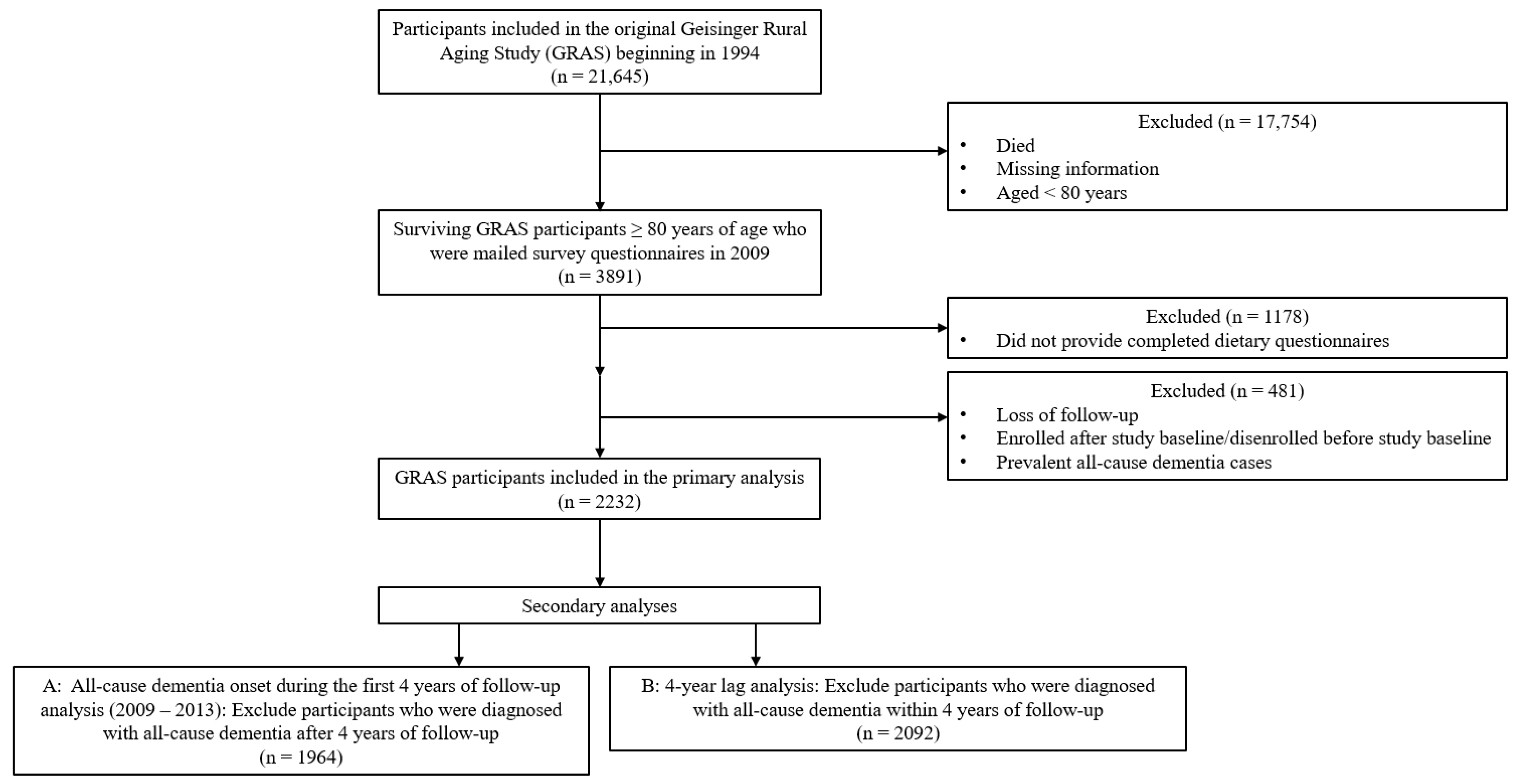
2.1. Study Population
2.2. Assessment of Diet Quality
2.3. Assessment of Incident Cases for All-Cause Dementia
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mather, M.; Jacobsen, L.; Kilduff, L.; Lee, A.; Pollard, K.; Scommegna, P.; Vonorman, A. America’s changing population. Pop. Bull. 2019, 74, 1–22. [Google Scholar]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Rajan, K.B.; Weuve, J.; Barnes, L.L.; McAninch, E.A.; Wilson, R.S.; Evans, D.A. Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020–2060). Alzheimer’s Dement. 2021, 17, 1966–1975. [Google Scholar] [CrossRef]
- Gauthier, S.; Rosa-Neto, P.; Morais, J.; Webster, C. World Alzheimer Report 2021: Journey through the Diagnosis of Dementia. Available online: https://www.alzint.org/u/World-Alzheimer-Report-2021.pdf (accessed on 4 November 2021).
- Anonymous. 2022 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.C.; Valcour, V.; Yaffe, K. Dementia in the oldest old: A multi-factorial and growing public health issue. Alzheimer’s Res. Ther. 2013, 5, 27. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. Available online: https://www.who.int/publications/i/item/9789241550543 (accessed on 26 November 2019).
- Paganini-Hill, A.; Kawas, C.H.; Corrada, M.M. Lifestyle factors and dementia in the oldest-old: The 90+ study. Alzheimer Dis. Assoc. Disord. 2016, 30, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, T.F.; Andel, R.; Small, B.J.; Borenstein, A.R.; Mortimer, J.A.; Wolk, A.; Johansson, B.; Fratiglioni, L.; Pedersen, N.L.; Gatz, M. Midlife fruit and vegetable consumption and risk of dementia in later life in Swedish twins. Am. J. Geriatr. Psychiatry 2010, 18, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Kimura, Y.; Yoshida, D.; Ohara, T.; Hata, J.; Honda, T.; Hirakawa, Y.; Shibata, M.; Oishi, E.; Sakata, S.; Furuta, Y. Long-term association of vegetable and fruit intake with risk of dementia in Japanese older adults: The Hisayama study. BMC Geriatr. 2022, 22, 257. [Google Scholar] [CrossRef]
- Zhang, H.; Greenwood, D.C.; Risch, H.A.; Bunce, D.; Hardie, L.J.; Cade, J.E. Meat consumption and risk of incident dementia: Cohort study of 493,888 UK Biobank participants. Am. J Clin. Nutr. 2021, 114, 175–184. [Google Scholar] [CrossRef]
- Wang, K.; Tang, W.; Hao, X.; Liu, H. High consumption of whole grain foods decreases the risk of dementia and Alzheimer’s disease: Framingham Offspring Cohort. Psychiatry Clin. Neurosci. 2022, 77, 141–148. [Google Scholar] [CrossRef]
- Zhao, C.; Tsapanou, A.; Manly, J.; Schupf, N.; Brickman, A.M.; Gu, Y. Vitamin D intake is associated with dementia risk in the Washington Heights-Inwood Columbia Aging Project (WHICAP). Alzheimer’s Dement. 2020, 16, 1393–1401. [Google Scholar] [CrossRef]
- Liu, S.; Luo, J.; Xiao, Z.; Wu, W.; Liang, X.; Ding, S.; Zhao, Q.; Zhao, X.; Wang, Y.; Ding, D. Low dietary vitamin E intake is associated with high risk of incident dementia among older adults: The Shanghai Aging Study. Front. Nutr. 2022, 9, 1036795. [Google Scholar] [CrossRef]
- Jacques, P.F.; Tucker, K.L. Are dietary patterns useful for understanding the role of diet in chronic disease? Am. J. Clin. Nutr. 2001, 73, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Neuhouser, M.L. The importance of healthy dietary patterns in chronic disease prevention. Nutr. Res. 2019, 70, 3–6. [Google Scholar] [CrossRef]
- Féart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Roberts, R.O.; Geda, Y.E.; Cerhan, J.R.; Knopman, D.S.; Cha, R.H.; Christianson, T.J.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; O’Connor, H.M.; et al. Vegetables, unsaturated fats, moderate alcohol intake, and mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2010, 29, 413–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, E.; Karlström, B.; Kilander, L.; Byberg, L.; Cederholm, T.; Sjögren, P. Dietary patterns and cognitive dysfunction in a 12-year follow-up study of 70 year old men. J. Alzheimer’s Dis. 2015, 43, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Haring, B.; Wu, C.; Mossavar-Rahmani, Y.; Snetselaar, L.; Brunner, R.; Wallace, R.B.; Neuhouser, M.L.; Wassertheil-Smoller, S. No Association between Dietary Patterns and Risk for Cognitive Decline in Older Women with 9-Year Follow-Up: Data from the Women’s Health Initiative Memory Study. J. Acad. Nutr. Diet. 2016, 116, 921–930.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voortman, T.; Kiefte-de Jong, J.C.; Ikram, M.A.; Stricker, B.H.; van Rooij, F.J.A.; Lahousse, L.; Tiemeier, H.; Brusselle, G.G.; Franco, O.H.; Schoufour, J.D. Adherence to the 2015 Dutch dietary guidelines and risk of non-communicable diseases and mortality in the Rotterdam Study. Eur. J. Epidemiol. 2017, 32, 993–1005. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Wolk, A. The Role of Lifestyle Factors and Sleep Duration for Late-Onset Dementia: A Cohort Study. J. Alzheimer’s Dis. 2018, 66, 579–586. [Google Scholar] [CrossRef] [Green Version]
- Akbaraly, T.N.; Singh-Manoux, A.; Dugravot, A.; Brunner, E.J.; Kivimäki, M.; Sabia, S. Association of Midlife Diet With Subsequent Risk for Dementia. JAMA 2019, 321, 957–968. [Google Scholar] [CrossRef] [Green Version]
- Scarmeas, N.; Stern, Y.; Tang, M.X.; Mayeux, R.; Luchsinger, J.A. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2006, 59, 912–921. [Google Scholar] [CrossRef] [Green Version]
- Scarmeas, N.; Luchsinger, J.A.; Schupf, N.; Brickman, A.M.; Cosentino, S.; Tang, M.X.; Stern, Y. Physical activity, diet, and risk of Alzheimer disease. JAMA 2009, 302, 627–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.; Nieves, J.W.; Stern, Y.; Luchsinger, J.A.; Scarmeas, N. Food combination and Alzheimer disease risk: A protective diet. Arch. Neurol. 2010, 67, 699–706. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.; Luchsinger, J.A.; Stern, Y.; Scarmeas, N. Mediterranean diet, inflammatory and metabolic biomarkers, and risk of Alzheimer’s disease. J. Alzheimer’s Dis. 2010, 22, 483–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskelinen, M.H.; Ngandu, T.; Tuomilehto, J.; Soininen, H.; Kivipelto, M. Midlife healthy-diet index and late-life dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Dis. Extra 2011, 1, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, M.; Ninomiya, T.; Ohara, T.; Doi, Y.; Uchida, K.; Shirota, T.; Yonemoto, K.; Kitazono, T.; Kiyohara, Y. Dietary patterns and risk of dementia in an elderly Japanese population: The Hisayama Study. Am. J. Clin. Nutr. 2013, 97, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Honkura, K.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Dietary Patterns and Incident Dementia in Elderly Japanese: The Ohsaki Cohort 2006 Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Hosking, D.E.; Eramudugolla, R.; Cherbuin, N.; Anstey, K.J. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimer’s Dement. 2019, 15, 581–589. [Google Scholar] [CrossRef]
- Hu, E.A.; Wu, A.; Dearborn, J.L.; Gottesman, R.F.; Sharrett, A.R.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Adherence to Dietary Patterns and Risk of Incident Dementia: Findings from the Atherosclerosis Risk in Communities Study. J. Alzheimer’s Dis. 2020, 78, 827–835. [Google Scholar] [CrossRef]
- Andreu-Reinón, M.E.; Chirlaque, M.D.; Gavrila, D.; Amiano, P.; Mar, J.; Tainta, M.; Ardanaz, E.; Larumbe, R.; Colorado-Yohar, S.M.; Navarro-Mateu, F.; et al. Mediterranean Diet and Risk of Dementia and Alzheimer’s Disease in the EPIC-Spain Dementia Cohort Study. Nutrients 2021, 13, 700. [Google Scholar] [CrossRef]
- Lu, Y.; Matsuyama, S.; Sugawara, Y.; Sone, T.; Tsuji, I. Changes in a specific dietary pattern and incident dementia: A prospective cohort study. Clin. Nutr. 2021, 40, 3495–3502. [Google Scholar] [CrossRef]
- Nicoli, C.; Galbussera, A.A.; Bosetti, C.; Franchi, C.; Gallus, S.; Mandelli, S.; Marcon, G.; Quadri, P.; Riso, P.; Riva, E.; et al. The role of diet on the risk of dementia in the oldest old: The Monzino 80-plus population-based study. Clin. Nutr. 2021, 40, 4783–4791. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H.; Gao, X.; Na, M.; Kris-Etherton, P.M.; Mitchell, D.C.; Jensen, G.L. Dietary Pattern, Diet Quality, and Dementia: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Alzheimer’s Dis. 2020, 78, 151–168. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Maguire, B.; Brodaty, H.; O’Leary, F. Dietary patterns and cognitive health in older adults: A systematic review. J. Alzheimer’s Dis. 2019, 67, 583–619. [Google Scholar] [CrossRef] [PubMed]
- van de Rest, O.; Berendsen, A.A.; Haveman-Nies, A.; de Groot, L.C. Dietary patterns, cognitive decline, and dementia: A systematic review. Adv. Nutr. 2015, 6, 154–168. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.H.; Gao, X.; Mitchell, D.C.; Wood, G.C.; Bailey, R.K.; Still, C.D.; Jensen, G.L. Validation of a Diet Quality Screening Tool for Use in the Oldest Old. J. Nutr. Gerontol. Geriatr. 2019, 38, 196–204. [Google Scholar] [CrossRef]
- Liu, Y.H.; Jensen, G.L.; Na, M.; Mitchell, D.C.; Wood, G.C.; Still, C.D.; Gao, X. Diet Quality and Risk of Parkinson’s Disease: A Prospective Study and Meta-Analysis. J. Parkinsons Dis. 2021, 11, 337–347. [Google Scholar] [CrossRef]
- Bailey, R.L.; Miller, P.E.; Mitchell, D.C.; Hartman, T.J.; Lawrence, F.R.; Sempos, C.T.; Smiciklas-Wright, H. Dietary screening tool identifies nutritional risk in older adults. Am. J. Clin. Nutr. 2009, 90, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Jensen, G.L.; Kita, K.; Fish, J.; Heydt, D.; Frey, C. Nutrition risk screening characteristics of rural older persons: Relation to functional limitations and health care charges. Am. J. Clin. Nutr. 1997, 66, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Mitchell, D.C.; Miller, C.K.; Still, C.D.; Jensen, G.L.; Tucker, K.L.; Smiciklas-Wright, H. A dietary screening questionnaire identifies dietary patterns in older adults. J. Nutr. 2007, 137, 421–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura Marra, M.; Thuppal, S.V.; Johnson, E.J.; Bailey, R.L. Validation of a Dietary Screening Tool in a Middle-Aged Appalachian Population. Nutrients 2018, 10, 345. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health & Human Services. Classification of Overweight and Obesity by BMI WC, and Associated Disease Risks. Available online: https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmi_dis (accessed on 29 October 2021).
- Granic, A.; Mendonça, N.; Hill, T.R.; Jagger, C.; Stevenson, E.J.; Mathers, J.C.; Sayer, A.A. Nutrition in the Very Old. Nutrients 2018, 10, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Q.; Sable, C.M.; Brooks-Wilson, A.; Murphy, R.A. Dietary patterns in the healthy oldest old in the healthy aging study and the Canadian longitudinal study of aging: A cohort study. BMC Geriatr. 2020, 20, 106. [Google Scholar] [CrossRef] [Green Version]
- Okello, E.J.; Mendonça, N.; Stephan, B.; Muniz-Terrera, G.; Wesnes, K.; Siervo, M. Tea consumption and measures of attention and psychomotor speed in the very old: The Newcastle 85+ longitudinal study. BMC Nutr. 2020, 6, 57. [Google Scholar] [CrossRef]
- Granic, A.; Davies, K.; Adamson, A.; Kirkwood, T.; Hill, T.R.; Siervo, M.; Mathers, J.C.; Jagger, C. Dietary Patterns High in Red Meat, Potato, Gravy, and Butter Are Associated with Poor Cognitive Functioning but Not with Rate of Cognitive Decline in Very Old Adults. J. Nutr. 2016, 146, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Yin, Z.; Fei, Z.; Qiu, C.; Brasher, M.S.; Kraus, V.B.; Zhao, W.; Shi, X.; Zeng, Y. Dietary Diversity and Cognitive Function among Elderly People: A Population-Based Study. J. Nutr. Health Aging 2017, 21, 1089–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolin, J.N.; Bellamy, G.R.; Ferdinand, A.O.; Vuong, A.M.; Kash, B.A.; Schulze, A.; Helduser, J.W. Rural Healthy People 2020: New Decade, Same Challenges. J. Rural Health 2015, 31, 326–333. [Google Scholar] [CrossRef]
- Cipriani, G.; Carlesi, C.; Lucetti, C.; Danti, S.; Nuti, A. Eating Behaviors and Dietary Changes in Patients With Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2016, 31, 706–716. [Google Scholar] [CrossRef]
- Fostinelli, S.; De Amicis, R.; Leone, A.; Giustizieri, V.; Binetti, G.; Bertoli, S.; Battezzati, A.; Cappa, S.F. Eating Behavior in Aging and Dementia: The Need for a Comprehensive Assessment. Front. Nutr. 2020, 7, 604488. [Google Scholar] [CrossRef]
- Slavin, M.J.; Brodaty, H.; Sachdev, P.S. Challenges of diagnosing dementia in the oldest old population. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1103–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawas, C.H.; Corrada, M.M. Alzheimer’s and dementia in the oldest-old: A century of challenges. Curr. Alzheimer Res. 2006, 3, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Brumback-Peltz, C.; Balasubramanian, A.B.; Corrada, M.M.; Kawas, C.H. Diagnosing dementia in the oldest-old. Maturitas 2011, 70, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Kawas, C.H.; Kim, R.C.; Sonnen, J.A.; Bullain, S.S.; Trieu, T.; Corrada, M.M. Multiple pathologies are common and related to dementia in the oldest-old. Neurology 2015, 85, 535–542. [Google Scholar] [CrossRef] [Green Version]
- James, B.D. Dementia From Alzheimer Disease and Mixed Pathologies in the Oldest Old. JAMA 2012, 307, 1798. [Google Scholar] [CrossRef] [Green Version]
- Schneider, J.A.; Arvanitakis, Z.; Bang, W.; Bennett, D.A. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007, 69, 2197–2204. [Google Scholar] [CrossRef] [PubMed]
- Calvin, C.M.; Wilkinson, T.; Starr, J.M.; Sudlow, C.; Hagenaars, S.P.; Harris, S.E.; Schnier, C.; Davies, G.; Fawns-Ritchie, C.; Gale, C.R.; et al. Predicting incident dementia 3-8 years after brief cognitive tests in the UK Biobank prospective study of 500,000 people. Alzheimer’s Dement. 2019, 15, 1546–1557. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Diet Quality | ||||
|---|---|---|---|---|
| Tertile 1 (DST Score < 57) (n = 766) | Tertile 2 (58 < DST Score < 68) (n = 708) | Tertile 3 (DST Score > 69) (n = 758) | p-Value a | |
| Age, mean (SD), y | 84.0 (3.5) | 84.1 (3.7) | 84.1 (3.5) | 0.95 |
| Sex No. (%) | ||||
| Men | 326 (42.6) | 288 (40.7) | 305 (40.2) | 0.62 |
| Women | 440 (57.4) | 420 (59.3) | 453 (59.8) | |
| Race No. (%) | ||||
| White | 761 (99.4) | 700 (98.9) | 753 (99.3) | 0.66 |
| Other | 2 (0.3) | 1 (0.1) | 1 (0.1) | |
| Unable to obtain or unknown | 3 (0.4) | 7 (1.0) | 4 (0.5) | |
| Body mass index No. (%), kg/m2 | ||||
| <18.5 | 17 (2.2) | 15 (2.1) | 11 (1.5) | 0.11 |
| 18.5–24.9 | 215 (28.1) | 199 (28.1) | 224 (29.6) | |
| 25.0–29.9 | 292 (38.1) | 265 (37.4) | 298 (39.3) | |
| 30.0–34.9 | 126 (16.5) | 115 (16.2) | 147 (19.4) | |
| 35 | 46 (6.0) | 44 (6.2) | 27 (3.6) | |
| Unknown | 70 (9.1) | 70 (9.9) | 51 (6.7) | |
| Educational level No. (%) | ||||
| Below college degree | 658 (85.9) | 537 (75.9) | 543 (71.6) | <0.001 |
| College degree | 62 (8.1) | 85 (12.0) | 133 (17.6) | |
| Graduate degree | 14 (1.8) | 35 (4.9) | 46 (6.1) | |
| Unknown | 32 (4.2) | 51 (7.2) | 36 (4.8) | |
| Smoking status No. (%) | ||||
| Never smoker | 393 (51.3) | 401 (56.6) | 461 (60.8) | 0.007 |
| Past or current smoker | 357 (46.6) | 294 (41.5) | 284 (37.5) | |
| Unknown | 16 (2.1) | 13 (1.8) | 13 (1.7) | |
| Physical activity No. (%) | ||||
| Everyday | 292 (38.1) | 347 (49.0) | 464 (61.2) | <0.001 |
| Some days | 428 (55.9) | 311 (43.9) | 258 (34.0) | |
| Not at all | 18 (2.4) | 7 (1.0) | 4 (0.5) | |
| Unknown | 28 (3.7) | 43 (6.1) | 32 (4.2) | |
| Diabetes/borderline diabetes No. (%) | ||||
| Yes | 184 (24.0) | 163 (23.0) | 154 (20.3) | 0.20 |
| No | 582 (76.0) | 545 (77.0) | 604 (79.7) | |
| Hypertension No. (%) | ||||
| Yes | 404 (52.7) | 375 (53.0) | 424 (55.9) | 0.38 |
| No | 362 (47.3) | 333 (47.0) | 334 (44.1) | |
| Coronary heart disease No. (%) | ||||
| Yes | 112 (14.6) | 108 (15.3) | 107 (14.1) | 0.83 |
| No | 654 (85.4) | 600 (84.8) | 651 (85.9) | |
| Living status No. (%) | ||||
| Live alone | 308 (40.2) | 276 (39.0) | 296 (39.1) | 0.02 |
| With spouse, son/daughter, other family members, or other | 441 (57.6) | 392 (55.4) | 434 (57.3) | |
| Unknown | 17 (2.2) | 40 (5.7) | 28 (3.7) | |
| Living arrangement No. (%) | ||||
| House, apartment condominium, or mobile home | 728 (95.0) | 647 (91.4) | 711 (93.8) | 0.003 |
| Assisted living apartment, care/nursing home, or other | 20 (2.6) | 15 (2.1) | 18 (2.4) | |
| Unknown | 18 (2.4) | 46 (6.5) | 29 (3.8) | |
| Antidepressant medication No. (%) | ||||
| Yes | 72 (9.4) | 80 (11.3) | 75 (9.9) | 0.46 |
| No | 694 (90.6) | 628 (88.7) | 683 (90.1) | |
| Self- or proxy-report No. (%) | ||||
| Self | 667 (87.1) | 607 (85.7) | 676 (89.2) | 0.24 |
| Proxy | 78 (10.2) | 73 (10.3) | 64 (8.4) | |
| Unknown | 21 (2.7) | 28 (4.0) | 18 (2.4) | |
| Dietary Screening Tool (DST) score, mean (SD) | 48.3 (7.3) | 63.1 (3.2) | 76.0 (5.5) | <0.001 |
| Diet Quality | ||||
|---|---|---|---|---|
| Tertile 1 (DST Score < 57) | Tertile 2 (58 < DST Score < 68) | Tertile 3 (DST Score > 69) | P-Trend a | |
| Hazard Ratio (95% CI) | ||||
| All-cause dementia onset during full follow-up years (2009–2021) | ||||
| Events/Number | 141/766 | 131/708 | 136/758 | |
| Model 1 b | 1.00 (Reference) | 1.02 (0.80, 1.29) | 0.90 (0.71, 1.13) | 0.37 |
| Model 2 c | 1.00 (Reference) | 1.05 (0.82, 1.34) | 1.01 (0.79, 1.29) | 0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores, A.C.; Jensen, G.L.; Mitchell, D.C.; Na, M.; Wood, G.C.; Still, C.D.; Gao, X. Prospective Study of Diet Quality and the Risk of Dementia in the Oldest Old. Nutrients 2023, 15, 1282. https://doi.org/10.3390/nu15051282
Flores AC, Jensen GL, Mitchell DC, Na M, Wood GC, Still CD, Gao X. Prospective Study of Diet Quality and the Risk of Dementia in the Oldest Old. Nutrients. 2023; 15(5):1282. https://doi.org/10.3390/nu15051282
Chicago/Turabian StyleFlores, Ashley C., Gordon L. Jensen, Diane C. Mitchell, Muzi Na, G. Craig Wood, Christopher D. Still, and Xiang Gao. 2023. "Prospective Study of Diet Quality and the Risk of Dementia in the Oldest Old" Nutrients 15, no. 5: 1282. https://doi.org/10.3390/nu15051282
APA StyleFlores, A. C., Jensen, G. L., Mitchell, D. C., Na, M., Wood, G. C., Still, C. D., & Gao, X. (2023). Prospective Study of Diet Quality and the Risk of Dementia in the Oldest Old. Nutrients, 15(5), 1282. https://doi.org/10.3390/nu15051282