

Systematic Literature Review of the Nutrient Status, Intake, and Diet Quality of Chinese Children across Different Age Groups

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Guidelines and Registration
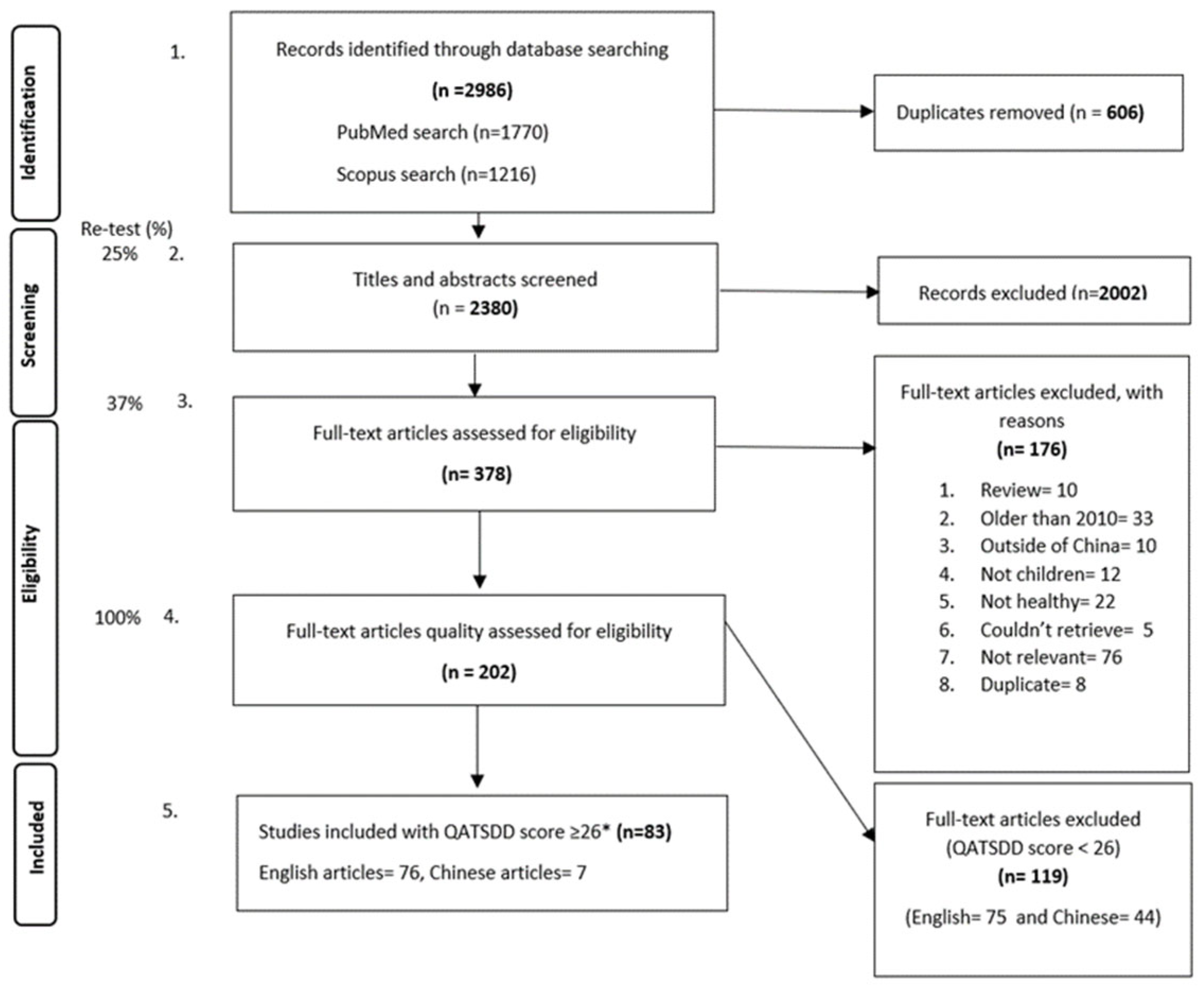
2.2. Data Sources and Study Selection
2.3. Data Extraction
2.4. Quality and Bias Assessment
2.5. Data Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Outcome Indicator | Biomarker/Assessment Method | Outcome Indicator Measure (Units) | Cutoffs for Deficiency, Insufficiency, or Inadequacy |
|---|---|---|---|---|
| Nutrient Status | Iron status | Hemoglobin concentration (Hb) | Mean (g/L), SE 1 | Prevalence of anemia: as per WHO guidelines, age-specific groups: for children <5 years <110 g/L anemia, for children aged 5–11 years <115 g/L anemia, for children aged 12–14 years <120 g/L anemia, for non-pregnant women (15 years and above) <120 g/L anemia, and for men (15 years and above) <130 g/L [16] |
| Serum ferritin | Mean (μg/L), SE 1 | % Iron deficiency: as per WHO guidelines, <12 μg/L for non-infected children or <30 μg/L for infected children (%, n) [17] | ||
| Vitamin A status | Serum retinol concentration | Mean (μmol/L), SE 1 | Vitamin A deficient (VAD): as per WHO guidelines, 0.7 μmol/L (<20 µg/dL), % Vitamin A Insufficient (VAI): 1.05 μmol/L (<30 µg/dL) [18] | |
| Vitamin D status | 25(OH)D concentration | Mean (nmol/L), SE 1 | Vitamin D deficiency (VAD): the clinical practice guidelines of the Endocrine Society Task Force on Vitamin D have defined a cutoff level of <20 ng/mL (50 nmol/L) as Vitamin D deficient, % Vitamin D insufficient: levels between 20 and 30 ng/mL (50–75 nmol/L) as ‘insufficient’ [19]. More recent recommendations justify a cutoff of 12 ng/mL (30 nmol/L) for deficiency | |
| Iodine status | Urinary iodine Presence of goiter | Median (ng/mL), SE 1 | % Iodine deficient: as per WHO guidelines, <100 μg/L as deficient, 100–300 μg/L as sufficient, and >300 μg/L as excess [20] % children with goiter | |
| Zinc status | Serum zinc concentration | Mean (μg/L), SE 1 | % Zinc deficient: <700 μg/L as deficient [21] | |
| Selenium status | Serum selenium concentration | Mean (μg/L), SE 1 | % Selenium deficient: <45 μg/L as very low, % Low selenium: <60 μg/L as low and 60–120 μg/L as normal [22] | |
| Vitamin B12 status | Plasma Vitamin B12 | Mean (pmol/L), SE 1 | % Vitamin B12 deficient: as per WHO guidelines: <150 pmol/L (203 pg/mL) [23,24] | |
| Folate status | Serum/plasma folate level | Mean (nmol/L), SE 1 | % Folate deficient: as per WHO guidelines, 4 ng/mL (<10 nmol/L) as deficient [23] | |
| Nutrient (and Energy) Intake | Energy intake | Self-reported from 24 h recalls (24 h). In most cases, multiple 24 h | Mean (Kcal/day), SE 1 | EER cutoff method using Chinese estimated energy requirement (EER) [13] |
| Macronutrients (carbohydrates, fat, and protein) and micronutrients (iron; zinc; selenium; calcium; iodine; sodium; Vitamins A, B1, B2, B3, B9, B12, D) | Self-reported from 24 h recalls (24 h). In most cases, multiple 24 h | Mean (g mg, μg)/day, SE 1 | % inadequacy: % population that consumed below the EAR. Calculated using the EAR cutoff method using Chinese-specific estimated average requirement (EAR) and Upper Limit (UL) [13]. Adequate Intakes (AI) were used when EAR was not possible | |
| Food Intake | Food group intake | Self-reported from 24 h recalls (24 h). In most cases, multiple 24 h | Mean (g/day) | Food group inadequacy; % below recommended; recommendations based on the Chinese Nutrition Society’s Food Guide Pagoda [14] |
| Diet Quality | Diet quality | Assessment method varies by study; see Appendix B | Diet diversity score | Scoring system varies by study; see Appendix B |
3. Results
3.1. Study Characteristics
3.2. Energy and Macronutrient Intake
3.2.1. Energy Intake
3.2.2. Fat Intake
3.2.3. Carbohydrate Intake
3.2.4. Protein Intake
3.3. Mineral Intake and Status
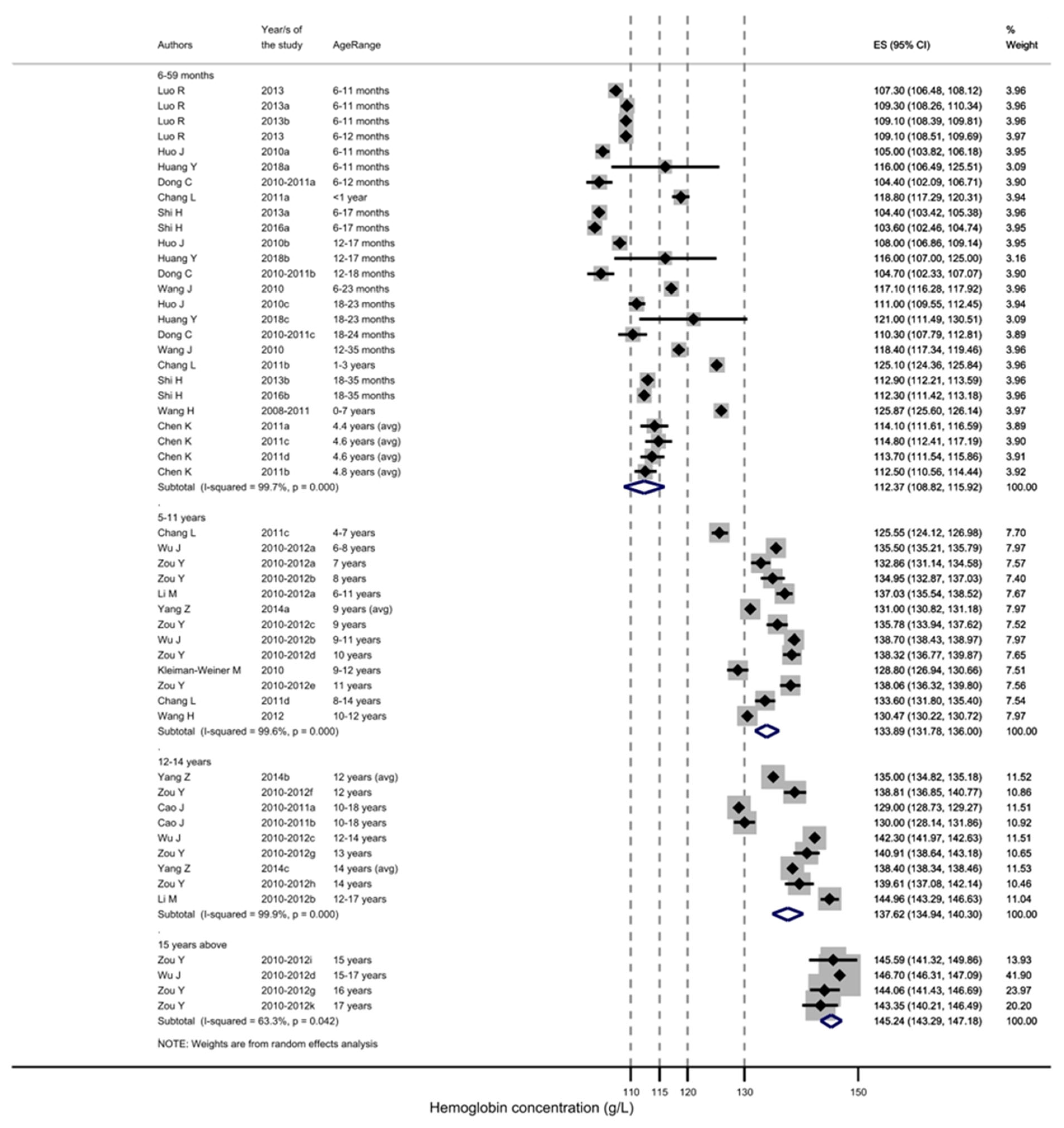
3.3.1. Anemia and Iron Status
3.3.2. Iron Intake
3.3.3. Zinc Status
3.3.4. Zinc Intake
3.3.5. Selenium Status
3.3.6. Selenium Intake
3.3.7. Calcium Intake
3.3.8. Magnesium Intake
3.3.9. Sodium Intake
3.3.10. Iodine Status
3.3.11. Phosphorus Intake
3.4. Vitamin intake and Status
3.4.1. Vitamin A Status
3.4.2. Vitamin A Intake
3.4.3. Vitamin B1 (Thiamin) Intake
3.4.4. Vitamin B2 (Riboflavin) Intake
3.4.5. Vitamin B3 (Niacin) Intake
3.4.6. Vitamin C Intake
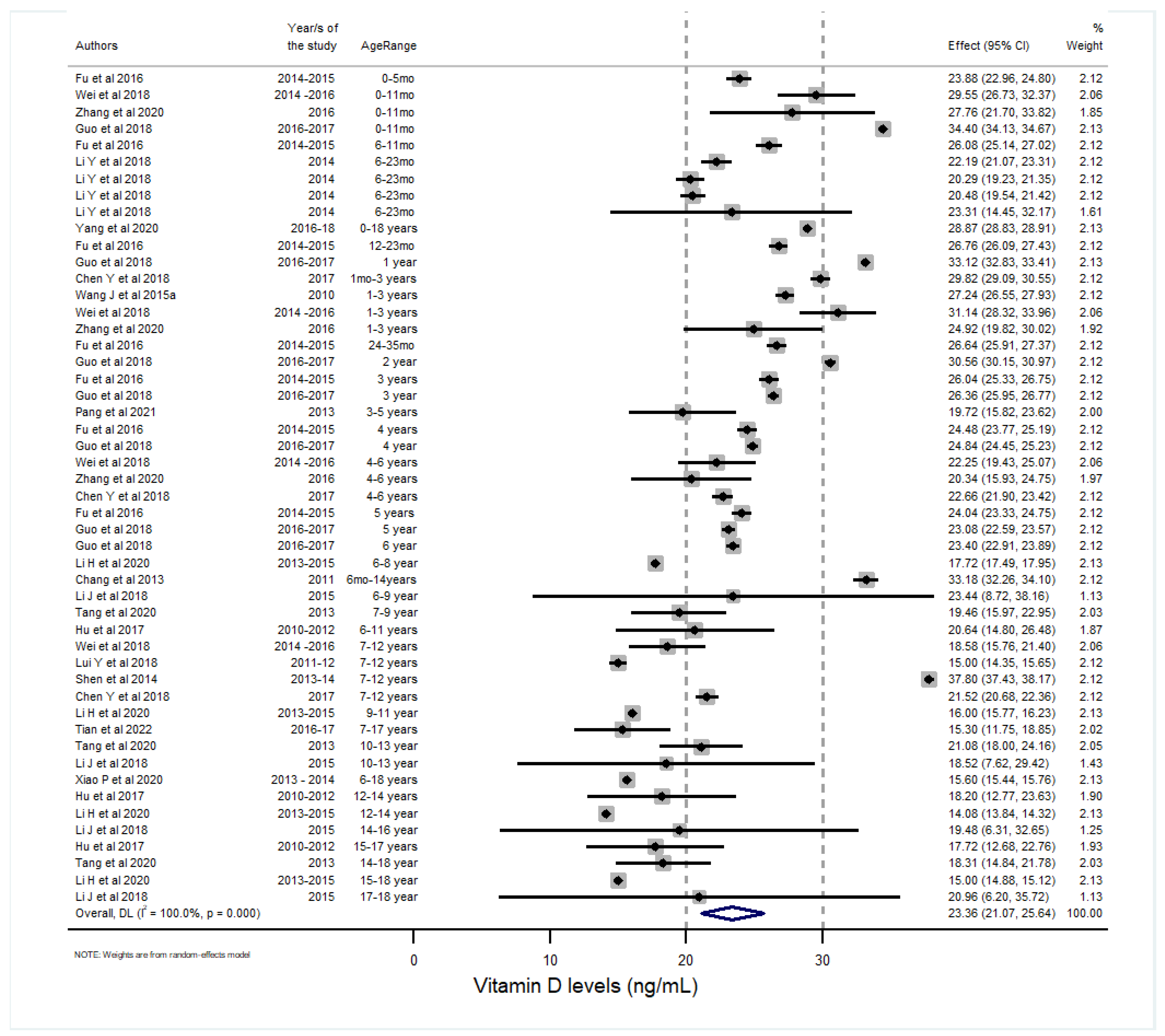
3.4.7. Vitamin D Status
3.4.8. Vitamin D Intake
3.4.9. Vitamin B12 Status
3.4.10. Folic Acid Status
3.4.11. Folic acid Intake
3.5. Food Group Intake
3.6. Diet Quality
4. Discussion
4.1. Strength and Limitations
4.2. Future Opportunities
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Keywords | (‘diet’ OR ‘nutrient’ OR ‘micronutrient’ OR ‘vitamin’ OR ‘mineral’) | AND |
| (‘malnutrition’ OR ‘intake’ OR deficiency’ OR ‘inadequate’ OR ‘anaemia’) | AND | |
| (‘infant’ OR ‘toddler’ OR ‘preschool’ OR ‘child’ OR ‘adolescent’) | AND | |
| (‘China’ OR ‘Chinese’) | AND | |
| (‘pregnant’ OR ‘maternal’) | NOT | |
| Parameter | Description | |
| Population | Healthy children (0–18 years old) living in China | |
| Intervention | Not applicable | |
| Comparison | Age-specific WHO/national cutoffs; regions in China | |
| Outcomes |
| |
| Setting/Design | Observational studies (i.e., cross-sectional, cohort, case–control and longitudinal studies, case reports), intervention baseline results. | |
Appendix B
| Diet Quality Measure | Study | Based on | Cutoff | Result | Population Group (Years; Region) |
|---|---|---|---|---|---|
| Minimum dietary diversity (MDD), minimum meal frequency (MMF), and minimum acceptable diet (MAD) | Zhao et al. (2020) [65] based on dedicated cross-sectional survey | WHO guidelines for measurement of infant and young child feeding; 1-time 24 h dietary recall | MMF, MMD, and MAD according to WHO and UNICEF, 2017 | 60.8% of children met MMF. 23.0% met MDD; 17.6% met MAD; Dietary Frequency: roots and tubers 80.1%; fruits 69.2%; meat 58.7%; dairy 47.2%; legumes and nuts 24.7%; egg 22.3%; Vitamin-A-rich foods 62%; 54% were breastfed | 6–23 months; from 6 rural counties in Shanxi and Guizhou provinces |
| Minimum dietary diversity (MDD), minimum meal frequency (MMF), and minimum acceptable diet (MAD) | Feng et al. (2022) [55]; data from the Nutrition Improvement Project on Children in Poor Areas of China (NIPCPAC) in 2018 | 24 h dietary recall | MMF, MMD, and MAD according to WHO and UNICEF, 2017 | % of children meeting indicators: MDD = 68.9%, MMF = 77.9%, and MAD = 46.4% | 6–23 months in rural communities in Guizhou, Henan, Xinjiang, Hubei, and Hebei provinces in 2018 |
| Continued breastfeeding; minimum dietary diversity (MDD); consumption of iron-rich foods; anemia | Yao et al. (2021) [59] baseline data from a community-based child health counselling intervention | 24 h dietary recall | Continued breastfeeding rate at 1 year, MMD, anemia | Continued breastfeeding rate at 1 year = 69.5%; MDD 49.5%; consumption of iron-rich foods = 55%; anemia: 52.1% | 6–23 months, poor rural areas in Liangshan in 2018 |
| Diet Diversity Score (DDS) | Meng et al. (2018) [38], using CHNS data (over a 3 day period) | 9 food groups from the Chinese Dietary Guideline | DDS score lower than 8 was considered below the recommendation | 6.14 | 3–12 years; National |
| 6.11 | 13–17 years; National | ||||
| DDS | One 24 h, Zhao et al. (2017) [78] | 10 food groups based on FAO; based on 10 g or more of food | No cutoff | 5.60 | 6–12 years |
| 17-food-group dietary diversity scores (SDDS) | One 24 h, Zhao et al. (2017) [78] | 17 food groups; based on 10 g or more of food | No cutoff | 7.5 | 6–12 years |
| Overall Food Variety Score (OFVS) | One 24 h, Zhao et al. (2017) [78] | Number of food items in 24 h. Single foods defined based on China Food composition table | No cutoff | 13.2 | 6–12 years |
| Healthy Diet Score | The Chinese Child and Adolescent Cardiovascular Health (CCACH) (Yan et al. (2019) [83] | This is defined by the American Heart Association to determine cardiovascular health status. | Daily fruit and vegetable consumption, fish or fish product consumption ≥ 2 times per week, daily bean or dairy products, fried or Western fast food ≤ 2 times per week, and sugar-sweetened beverages (SSB) ≤ 2 times per week. | 8.7% met the ‘Healthy Diet’ Score; the study reported that 43% of children met the goal for fruits and vegetables, 22% for seafood, 18% for beans and dairy, 60% for SSB, and 84.6% for fried/Western foods | 6–17 years |
| The Chinese Children Dietary Index | Cheng et al. (2016) [87], Zhang et al. (2019) [88] | 16 components with a maximum score of 160 points | No cutoff | 88 | 7–15 years old; Chengdu, Sichuan, western China |
| Minimum acceptable diet (MAD) | Last 24 h before the study, WHO indicators on Infant and Young Child Feeding, Zhang et al. (2016) [56] | Combination of minimum dietary diversity and minimum meal frequency | No cutoff | MAD was not met 93–95% | 6–23 months; rural Qinghai province; Guinan county and Huzhu county |
| % meeting dietary China Dietary Guidelines Index for Youth (CDGI-Y) | Ding et al. (2022) [43] using China National Nutrition and Health Survey (CNNHS) 2010–2012 | Food frequency questionnaire: the CDGI-Y is composed of 12 food groups and 2 nutrient-related components: energy balance and energy supply from carbohydrate | CDGI-Y | 20% of children met the guideline (21.9% girls and 18.2% boys) CDGI-Y score = 62.6 ± 11.0 (63.4 ± 10.9 girls and 61.8 ± 11.0 boys) | 9–15 years; National 2010–2012 |
| Dietary Diversity (DDS) and Dietary Frequency (DFS) | Tao et al. (2020) [98] using dedicated surveys in 90 rural primary schools | 24 h dietary recall; 9 food groups based on FAO guidelines | No cutoff | Overall DDS = 5.56. DFS: grains = 1.34; vegetables = 1.23; meat = 1.16; fruits = 1.03; tubers: 0.99; dairy: 0.98; beans and nuts = 0.96; eggs: 0.95; fish: 0.71 | 10–13 years; rural; 3 provinces in China in 2018 |
References
- Beluska-Turkan, K.; Korczak, R.; Hartell, B.; Moskal, K.; Maukonen, J.; Alexander, D.E.; Salem, N.; Harkness, L.; Ayad, W.; Szaro, J.; et al. Nutritional Gaps and Supplementation in the First 1000 Days. Nutrients 2019, 11, 2891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Fact Sheets—Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 12 July 2021).
- China (CHN)—Demographics, Health & Infant Mortality—UNICEF DATA. Available online: https://data.unicef.org/country/chn/ (accessed on 28 June 2021).
- Niseteo, T.; Hojsak, I. Editorial Commentary Impact of Rapid Socioeconomic Development in China on Nutritional Status in Children: Two Sides of a Coin. Ann. Transl. Med. 2019, 7, S301. [Google Scholar] [CrossRef] [PubMed]
- Zong, X.N.; Li, H.; Zhang, Y.Q.; Wu, H.H. Child Nutrition to New Stage in China: Evidence from a Series of National Surveys, 1985–2015. BMC Public Health 2019, 19, 402. [Google Scholar] [CrossRef] [PubMed]
- Development Initiatives Organisation. Global Nutrition Report; Development Initiatives: Bristol, UK, 2020; ISBN 9780896295841. Available online: https://globalnutritionreport.org/reports/2020-global-nutrition-report/ (accessed on 12 July 2021).
- Ministry of Foreign Affairs of the People’s Republic of China. Report on China’s Implementation of the Millennium Development Goals (2000–2015); Ministry of Foreign Affairs: Beijing, China, 2015.
- Piernas, C.; Wang, D.; Du, S.; Zhang, B.; Wang, Z.; Su, C.; Popkin, B.M. The Double Burden of Under- and Overnutrition and Nutrient Adequacy among Chinese Preschool and School-Aged Children in 2009–2011. Eur. J. Clin. Nutr. 2015, 69, 1323–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Huang, X.; Liu, Q.; Tang, S.; Story, M.; Chen, Y.; Zhou, M. Child Nutrition Trends over the Past Two Decades and Challenges for Achieving Nutrition SDGs and National Targets in China. Int. J. Environ. Res. Public Health 2020, 17, 1129. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.-F.; Wang, L.; Pan, A. Obesity in China 1 Epidemiology and Determinants of Obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373. [Google Scholar] [CrossRef]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing Studies with Diverse Designs: The Development and Evaluation of a New Tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef]
- Tardy, A.L.; Pouteau, E.; Marquez, D.; Yilmaz, C.; Scholey, A. Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. Nutrients 2020, 12, 228. [Google Scholar] [CrossRef] [Green Version]
- National Health Commission (NHC). Chinese Dietary Reference Intakes. Available online: http://www.nhc.gov.cn/wjw/yingyang/201710/fdade20feb8144ba921b412944ffb779/files/0fa10dfb812a48b483d931972df1ccb8.pdf (accessed on 25 August 2021).
- Chinese Nutrition Society. The Food Guide Pagoda for Chinese Residents. Available online: http://en.cnsoc.org/dGuideline/611921203.html (accessed on 23 August 2022).
- Wirt, A.; Collins, C.E. Diet Quality—What Is It and Does It Matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [Green Version]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; WHO: Geneva, Switzerland, 2011.
- WHO. Serum Transferrin Receptor Levels for the Assessment of Iron Status and Iron Deficiency in Populations; WHO: Geneva, Switzerland, 2014.
- WHO. Serum Retinol Concentrations for Determining the Prevalence of Vitamin A Deficiency in Populations; WHO: Geneva, Switzerland, 2011.
- Holick, M.; Binkley, N.; Bischoff-Ferrari, H.; Gordon, C.; Hanley, D.; Heaney, R.; Murad, M.; Weaver, C. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- WHO. Urinary Iodine Concentrations for Determining Iodine Status in Populations; WHO: Geneva, Switzerland, 2013.
- Hotz, C.; Peerson, J.M.; Brown, K.H. Suggested Lower Cutoffs of Serum Zinc Concentrations for Assessing Zinc Status: Reanalysis of the Second National Health and Nutrition Examination Survey Data (1976–1980). Am. J. Clin. Nutr. 2003, 78, 756–764. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Piao, J.; Li, M.; Zhang, Y.; Yun, C.; Yang, C.; Yang, X. Assessment of Selenium Nutritional Status of School-Age Children from Rural Areas of China in 2002 and 2012. Eur. J. Clin. Nutr. 2016, 70, 405–408. [Google Scholar] [CrossRef]
- World Health Organistaion (WHO). Serum and Red Blood Cell Folate Concentrations for Assessing Folate Status in Populations. In Vitamin and Mineral Nutrition Information System; WHO: Geneva, Switzerland, 2015; pp. 1–7. [Google Scholar]
- World Health Organization (WHO). Conclusions of a WHO Technical Consultation on Folate and Vitamin B12 Deficiencies. Food Nutr. Bull. 2008, 29, 238–244. [Google Scholar] [CrossRef]
- Duan, Y.; Pang, X.; Yang, Z.; Wang, J.; Jiang, S.; Bi, Y.; Wang, S.; Zhang, H.; Lai, J. Association between Dairy Intake and Linear Growth in Chinese Pre-School Children. Nutrients 2020, 12, 2576. [Google Scholar] [CrossRef]
- Pang, X.; Yang, Z.; Wang, J.; Duan, Y.; Zhao, L.; Yu, D.; Lai, J. Relationship between Serum 25OH-Vitamin D2 Level and Vitamin D Status of Children Aged 3–5 Years in China. Nutrients 2021, 13, 4135. [Google Scholar] [CrossRef]
- Jia, X.; Wang, D.; Eldridge, A.L.; Zhang, B.; Zhang, X.; Wang, H. Dairy Intake Would Reduce Nutrient Gaps in Chinese Young Children Aged 3–8 Years: A Modelling Study. Nutrients 2020, 12, 554. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Jiang, H.; Wang, H.; Zhang, B.; Zhang, J.; Jia, X.; Wang, L.; Wang, Z.; Ding, G. Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6–17 Years: Evidence from the China Health and Nutrition Survey 2015. Nutrients 2021, 13, 3097. [Google Scholar] [CrossRef]
- Zhao, J.; Zuo, L.; Sun, J.; Su, C.; Wang, H. Trends and Urban-Rural Disparities of Energy Intake and Macronutrient Composition among Chinese Children: Findings from the China Health and Nutrition Survey (1991 to 2015). Nutrients 2021, 13, 1933. [Google Scholar] [CrossRef]
- Li, M.; Hu, Y.; Mao, D.; Wang, R.; Chen, J.; Li, W.; Yang, X.; Piao, J.; Yang, L. Prevalence of Anemia among Chinese Rural Residents. Nutrients 2017, 9, 192. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Hu, Y.; Li, M.; Chen, J.; Mao, D.; Li, W.; Wang, R.; Yang, Y.; Piao, J.; Yang, L.; et al. Prevalence of Anemia in Chinese Children and Adolescents and Its Associated Factors. Int. J. Environ. Res. Public Health 2019, 16, 1416. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Chen, J.; Liu, Z.; Yun, C.; Li, Y.; Piao, J.; Yang, X.; Morales Suárez-Varela, M.M. Association of Vitamin A Status with Overnutrition in Children and Adolescents. Int. J. Environ. Res. Public Health 2015, 12, 15531–15539. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Chen, J.; Guo, N.; Liu, Z.; Yun, C.; Li, Y.; Piao, J.; Yang, X. Comparison on the Status of Vitamin A in 6- to 13- Year-Old Children between 2002 and 2012 in China. Nutr. J. 2016, 15, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Chen, J.; Wang, R.; Li, M.; Yun, C.; Li, W.; Yang, Y.; Piao, J.; Yang, X.; Yang, L. Vitamin D Nutritional Status and Its Related Factors for Chinese Children and Adolescents in 2010–2012. Nutrients 2017, 9, 1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Piao, J.; Zhang, Y.; He, Y.; Li, W.; Yang, L.; Yang, X. Assessment of Zinc Status in School-Age Children from Rural Areas in China Nutrition and Health Survey 2002 and 2012. Biol. Trace Elem. Res. 2017, 178, 194–200. [Google Scholar] [CrossRef]
- Wang, H.; Wang, D.; Ouyang, Y.; Huang, F.; Ding, G.; Zhang, B. Do Chinese Children Get Enough Micronutrients? Nutrients 2017, 9, 397. [Google Scholar] [CrossRef] [Green Version]
- Afeiche, M.C.; Koyratty, B.N.S.; Wang, D.; Jacquier, E.; Lê, K.A. Intakes and Sources of Total and Added Sugars among 4 to 13-Year-Old Children in China, Mexico and the United States. Pediatr. Obes. 2018, 13, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, D.; Eldridge, A.L.; Huang, F.; Ouyang, Y.; Wang, H.; Zhang, B. Urban–Rural Disparities in Energy Intake and Contribution of Fat and Animal Source Foods in Chinese Children Aged 4–17 Years. Nutrients 2017, 9, 526. [Google Scholar] [CrossRef] [Green Version]
- Yunzi, A.; Yu, L.; López-Olmedo, N.; Popkin, B.M.; Pac, A.; Clin, J.; Author, N. Analysis of Dietary Trends in Chinese Adolescents from 1991 to 2011. Asia Pac. J. Clin. Nutr. 2018, 27, 1106–1119. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.B.; Yang, L.C.; Chen, J.; Wang, R.; Yang, X.G.; Piao, J.H.; Mao, D.Q. Study on vitamin A nutritional status of 6- to 17-year-old urban children and adolescents between 2010 and 2012 in China. Zhonghua Yu Fang Yi Xue Za Zhi 2017, 51, 117–120. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Chen, J.; Wang, R.; Piao, J.; Yang, X.; Yang, L. Vitamin A nutritional status of Chinese rural children and adolescents in 2010-2012. Wei Sheng Yan Jiu 2017, 46, 345–349. [Google Scholar]
- Meng, L.; Wang, Y.; Li, T.; van Loo-Bouwman, C.A.; Zhang, Y.; Man-Yau Szeto, I. Dietary Diversity and Food Variety in Chinese Children Aged 3–17 Years: Are They Negatively Associated with Dietary Micronutrient Inadequacy? Nutrients 2018, 10, 1674. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.; Fan, J.; Yuan, F.; Feng, G.; Gong, W.; Song, C. Association between Physical Activity, Sedentary Behaviors, Sleep, Diet, and Adiposity among Children and Adolescents in China. Obes. Facts 2022, 15, 26–35. [Google Scholar] [CrossRef]
- Gui, Z.-H.; Zhu, Y.-N.; Cai, L.; Sun, F.-H.; Ma, Y.-H.; Jing, J.; Chen, Y.-J. Sugar-Sweetened Beverage Consumption and Risks of Obesity and Hypertension in Chinese Children and Adolescents: A National Cross-Sectional Analysis. Nutrients 2017, 9, 1302. [Google Scholar] [CrossRef] [Green Version]
- Liang, Z.; Xu, C.; Luo, Y.-J.J. Association of Iodized Salt with Goiter Prevalence in Chinese Populations: A Continuity Analysis over Time. Mil. Med. Res. 2017, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Su, X.; Liu, P.; Liu, S. Dynamic Changes in the Bivariable Distribution of Urinary Iodine Concentration and Thyroid Volume in Children Aged 8 to 10 Years in China. Asia Pac. J. Public Health 2017, 29, 288–295. [Google Scholar] [CrossRef]
- Yang, Z.; Li, Y.; Hu, P.; Ma, J.; Song, Y. Prevalence of Anemia and Its Associated Factors among Chinese 9-, 12-, and 14-Year-Old Children: Results from 2014 Chinese National Survey on Students Constitution and Health. Int. J. Environ. Res. Public Health 2020, 17, 1474. [Google Scholar] [CrossRef] [Green Version]
- Guo, Q.; Wang, B.; Cao, S.; Jia, C.; Yu, X.; Zhao, L.; Dellarco, M.; Duan, X. Association between Milk Intake and Childhood Growth: Results from a Nationwide Cross-Sectional Survey. Int. J. Obes. 2020, 44, 2194–2202. [Google Scholar] [CrossRef]
- Feng, J.; Gong, Z.; Wang, Y.; Huo, J.; Zhuo, Q. Complementary Feeding and Malnutrition among Infants and Young Children Aged 6-23 Months in Rural Areas of China. Nutrients 2022, 14, 1807. [Google Scholar] [CrossRef]
- Jia, N.N.; Zhang, S.; Li, T.; Tan, Z.; Yin, Y.; Chen, L.; Li, C.; Liu, A.; Bindels, J.G.J.G.; Dai, Y. Dietary Survey of Anaemic Infants and Young Children in Urban Areas of China: A Cross-Sectional Study. Asia Pac. J. Clin. Nutr. 2015, 24, 659–664. [Google Scholar] [CrossRef]
- Li, H.Z.; Jia, H.X.; Liang, D.; Deng, T.T.; Niu, L.T.; Han, J.H. [Study on the Contribution Rate of Follow-up Formula to the Nutrient Intake of Infants and Young Children Aged 7-24 Months in China]. Zhonghua Yu Fang Yi Xue Za Zhi 2017, 51, 65–69. [Google Scholar] [CrossRef]
- Huo, J.; Sun, J.; Fang, Z.; Chang, S.; Zhao, L.; Fu, P.; Wang, J.; Huang, J.; Wang, L.; Begin, F.; et al. Effect of Home-Based Complementary Food Fortification on Prevalence of Anemia Among Infants and Young Children Aged 6 to 23 Months in Poor Rural Regions of China. Food Nutr. Bull. 2015, 36, 405–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Huo, J.; Zhao, L.; Fu, P.; Wang, J.; Huang, J.; Wang, L.; Song, P.; Fang, Z.; Chang, S.; et al. The Nutritional Status of Young Children and Feeding Practices Two Years after the Wenchuan Earthquake in the Worst-Affected Areas in China. Asia Pac. J. Clin. Nutr. 2013, 22, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Scherpbier, R.W.; Huang, X.; Guo, S.; Yang, Y.; Josephs-Spaulding, J.; Ma, C.; Zhou, H.; Wang, Y. The Dietary Diversity and Stunting Prevalence in Minority Children under 3 Years Old: A Cross-Sectional Study in Forty-Two Counties of Western China. Br. J. Nutr. 2017, 118, 840–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Wang, L.; Huo, J.; Wu, Q.; Wang, W.; Chang, S.; Zhang, Y. Prevalence and Causes of Anaemia in Children Aged 6-23 Months in Rural Qinghai, China: Findings from a Cross-Sectional Study. BMJ Open 2019, 9, e031021. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wu, Q.; Wang, W.; van Velthoven, M.H.M.H.; Chang, S.; Han, H.; Xing, M.; Chen, L.; Scherpbier, R.W.R.W.R.W. Effectiveness of Complementary Food Supplements and Dietary Counselling on Anaemia and Stunting in Children Aged 6-23 Months in Poor Areas of Qinghai Province, China: A Controlled Interventional Study. BMJ Open 2016, 6, e011234. [Google Scholar] [CrossRef]
- Dong, C.; Ge, P.; Ren, X.; Wang, J.; Fan, H.; Yan, X.; Yin, S.A. Prospective Study on the Effectiveness of Complementary Food Supplements on Improving Status of Elder Infants and Young Children in the Areas Affected by Wenchuan Earthquake. PLoS ONE 2013, 8, e72711. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, Y.; Zhang, X.; Zhao, L.; Chen, L.; Sun, H. Vitamin D Status among Young Children Aged 6 to 23 Months from 4 Different Ethnic Groups in Yunnan, China. Food Nutr. Bull. 2018, 39, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Yao, S.; Xiao, S.; Jin, X.; Xiong, M.; Peng, J.; Jian, L.; Mei, Y.; Huang, Y.; Zhou, H.; Xu, T. Effect of a Community-Based Child Health Counselling Intervention on Health-Seeking Behaviours, Complementary Feeding and Nutritional Condition among Children Aged 6-23 Months in Rural China: A Pre-and Post-Comparison Study. Matern. Child Nutr. 2022, 18, e13289. [Google Scholar] [CrossRef]
- Zou, S.; Liu, Y.; Zheng, A.B.; Huang, Z. Associations between Dietary Patterns and Anaemia in 6- to 23-Month-Old Infants in Central South China. BMC Public Health 2021, 21, 699. [Google Scholar] [CrossRef]
- Luo, R.; Yue, A.A.; Zhou, H.; Shi, Y.; Zhang, L.; Martorell, R.; Medina, A.; Rozelle, S.; Sylvia, S. The Effect of a Micronutrient Powder Home Fortification Program on Anemia and Cognitive Outcomes among Young Children in Rural China: A Cluster Randomized Trial. BMC Public Health 2017, 17, 738. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; van der Horst, K.; Edelson-Fries, L.R.; Yu, K.; You, L.; Zhang, Y.; Vinyes-Pares, G.; Wang, P.; Ma, D.; Yang, X.; et al. Perceptions of Food Intake and Weight Status among Parents of Picky Eating Infants and Toddlers in China: A Cross-Sectional Study. Appetite 2017, 108, 456–463. [Google Scholar] [CrossRef] [Green Version]
- Ma, D.; Ning, Y.; Gao, H.; Li, W.; Wang, J.; Zheng, Y.; Zhang, Y.; Wang, P. Nutritional Status of Breast-Fed and Non-Exclusively Breast-Fed Infants from Birth to Age 5 Months in 8 Chinese Cities. Asia Pac. J. Clin. Nutr. 2014, 23, 282–292. [Google Scholar] [CrossRef]
- Wang, L.; Sun, Y.; Liu, B.; Zheng, L.; Li, M.; Bai, Y.; Osborn, A.; Lee, M.; Rozelle, S. Is Infant/Toddler Anemia a Problem across Rural China? A Mixed-Methods Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1825. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Zhang, J.; Du, Y.; Zhao, C.; Huang, X.; Wang, X. The Association between Parental Migration and Early Childhood Nutrition of Left-behind Children in Rural China. BMC Public Health 2020, 20, 246. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Guan, H.; Shi, H.; Zhang, J.; Huang, X.; Wang, X. Relationships between Dietary Diversity and Early Childhood Developmental Outcomes in Rural China. Matern. Child Nutr. 2021, 17, e13073. [Google Scholar] [CrossRef]
- Wang, J.; Wang, H.; Chang, S.; Zhao, L.; Fu, P.; Yu, W.; Man, Q.; Scherpbier, R.; Pan, L.; Duan, Y.; et al. The Influence of Malnutrition and Micronutrient Status on Anemic Risk in Children under 3 Years Old in Poor Areas in China. PLoS ONE 2015, 10, e0140840. [Google Scholar] [CrossRef]
- Wang, J.; Chang, S.; Zhao, L.; Yu, W.; Zhang, J.; Man, Q.; He, L.; Duan, Y.; Wang, H.; Scherpbier, R.; et al. Effectiveness of Community-Based Complementary Food Supplement (Yingyangbao) Distribution in Children Aged 6-23 Months in Poor Areas in China. PLoS ONE 2017, 12, e0174302. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Chen, Q.; Yu, L.; Yang, T.; Chen, J.; Miao, J.; Li, T. Changes in Vitamin A Levels and the Effect of Early Vitamin A Supplementation on Vitamin A Levels in Infants Throughout the First 6 Months of Life: A Prospective Cohort Study in Chongqing, China. Front. Public Health 2021, 9, 457. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Z.; Wei, Y.; Fu, J.; Feng, Y.; Chen, D.; Xu, D. Status and Influential Factors of Vitamin D among Children Aged 0 to 6 Years in a Chinese Population. BMC Public Health 2020, 20, 429. [Google Scholar] [CrossRef]
- Guo, Y.; Ke, H.J.; Liu, Y.; Fu, M.; Ning, J.; Yu, L.; Xiao, Y.; Che, D.; Chen, X.Y.; Deng, Y.H.; et al. Prevalence of Vitamin D Insufficiency among Children in Southern China: A Cross-Sectional Survey. Medicine 2018, 97, e11030. [Google Scholar] [CrossRef]
- Fu, Y.; Hu, Y.; Qin, Z.; Zhao, Y.; Yang, Z.; Li, Y.; Liang, G.; Lv, H.; Hong, H.; Song, Y.; et al. Association of Serum 25-Hydroxyvitamin D Status with Bone Mineral Density in 0-7 Year Old Children. Oncotarget 2016, 7, 80811–80819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, F.; Wang, Z.; Wang, J.; Xu, H.; Zhou, H. Serum Vitamin D Levels among Children Aged 0-12 Years in the First Affiliated Hospital of Harbin Medical University, China. J. Public Health 2018, 40, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Liu, M.; Mao, C.-Y.; Zhang, S.-H. An Investigation of Vitamin Levels Status in the Serum of Children in China. BioMed Res. Int. 2018, 2018, 6592757. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.L.; Liu, X.; Shi, H.; Dai, W.; Wang, H.; Jiang, Y. Association of 25-Hydroxyvitamin D with Hb and Lead in Children: A Chinese Population-Based Study. Public Health Nutr. 2014, 17, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Mao, M.; Ping, L.; Yu, D. Prevalence of Vitamin D Deficiency and Insufficiency among 460,537 Children in 825 Hospitals from 18 Provinces in Mainland China. Medicine 2020, 99, e22463. [Google Scholar] [CrossRef]
- Ma, Y.; Tan, J.; Tan, Z.; Shang, L. Validity and Reliability of Semiquantitative Food Frequency Questionnaires for Assessing Nutrient Intake among Preschool Children in Northwest China. J. Healthc. Eng. 2022, 2022, 1677252. [Google Scholar] [CrossRef]
- Chen, Q.; Liu, Y.; Chen, L.; Chen, J.; Yang, T.; Cheng, Q.; Li, T. Vitamin A Levels Among Pre-School Children of Central and Western China. Front. Public Health 2021, 9, 694106. [Google Scholar] [CrossRef]
- Tian, Z.; Wang, Y.; Zheng, J. Assessment of Exposure to Toxic Metals and Measures to Address Deficiency of Essential Trace Elements in Young Children in Rural Hubei, China. Environ. Sci. Pollut. Res. Int. 2020, 27, 21581–21589. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, L.; Luo, H.; Wang, J.; Li, Q.; Mao, M. No Enhancing Effect of Vitamin A Administration on Iron Absorption or Body Total Iron Content in Preschool Children from Chengdu, China. J. Nutr. Sci. Vitaminol. 2014, 60, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Peng, R.; Wei, X.; Liang, X.; Chen, J.; Liu, Y.; Zhang, T.; Li, T. Effect of dietary vitamin A intake on plasma vitamin A concentration in preschool children of Banan district, Chongqing, China. Beijing Da Xue Xue Bao Yi Xue Ban J. Peking Univ. Health Sci. 2014, 46, 366–372. [Google Scholar]
- Ma, D.; Zhang, Y.; You, L.; Tuo, Y.; Sheng, Q.; Wang, P. Analysis on the Iron Deficiency and the Rate of Anemia of 3-11 Year Old Children in 7 Cities and 2 Countryside in China. Wei Sheng Yan Jiu 2014, 43, 224–227. [Google Scholar]
- Zhao, W.; Yu, K.; Tan, S.; Zheng, Y.; Zhao, A.; Wang, P.; Zhang, Y. Dietary Diversity Scores: An Indicator of Micronutrient Inadequacy Instead of Obesity for Chinese Children. BMC Public Health 2017, 17, 440. [Google Scholar] [CrossRef] [Green Version]
- Xue, Y.; Zhao, A.; Cai, L.; Yang, B.; Szeto, I.M.Y.; Ma, D.; Zhang, Y.; Wang, P. Growth and Development in Chinese Pre-Schoolers with Picky Eating Behaviour: A Cross-Sectional Study. PLoS ONE 2015, 10, e0123664. [Google Scholar] [CrossRef]
- Liu, Y.; Li, X.; Zhao, A.; Zheng, W.; Guo, M.; Xue, Y.; Wang, P.; Zhang, Y. High Prevalence of Insufficient Vitamin D Intake and Serum 25-Hydroxyvitamin D in Chinese School-Age Children: A Cross-Sectional Study. Nutrients 2018, 10, 822. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Lou, X.; Ding, G.; Mo, Z.; Zhu, W.; Mao, G. A Cross-Sectional Comparison Study on the Iodine Nutritional Status between Rural and Urban Residents in Zhejiang Province, China. BMJ Open 2014, 4, 5484. [Google Scholar] [CrossRef] [Green Version]
- Shen, X.; Gao, X.; Tang, W.; Mao, X.; Huang, J.; Cai, W. Food Insecurity and Malnutrition in Chinese Elementary School Students. Br. J. Nutr. 2015, 114, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Yan, Y.; Liu, J.; Zhao, X.; Cheng, H.; Huang, G.; Hou, D.; Mi, J. Cardiovascular Health in Urban Chinese Children and Adolescents. Ann. Med. 2019, 51, 88–96. [Google Scholar] [CrossRef]
- Li, H.; Huang, T.; Xiao, P.; Zhao, X.; Liu, J.; Cheng, H.; Dong, H.; Morris, H.A.H.A.; Mi, J. Widespread Vitamin D Deficiency and Its Sex-Specific Association with Adiposity in Chinese Children and Adolescents. Nutrition 2020, 71, 110646. [Google Scholar] [CrossRef]
- Xiao, P.; Dong, H.; Li, H.; Yan, Y.; Cheng, H.; Liu, J.; Zhao, X.; Hou, D.; Mi, J. Adequate 25-Hydroxyvitamin D Levels Are Inversely Associated with Various Cardiometabolic Risk Factors in Chinese Children, Especially Obese Children. BMJ Open Diabetes Res. Care 2020, 8, 846. [Google Scholar] [CrossRef]
- Li, J.; Ding, W.; Cao, J.; Sun, L.; Liu, S.; Zhang, J.; Zhao, H. Serum 25-Hydroxyvitamin D and Bone Mineral Density among Children and Adolescents in a Northwest Chinese City. Bone 2018, 116, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Zhao, R.; Gan, Q.; Hu, Z.; Xu, P.; Li, L.; Yang, T.; Pan, H.; Hu, X.; Zhang, Q. Changes in Fitness of Rural Primary School Students from Southwest China after Two-Year’s Nutrition Intervention. Nutrients 2021, 13, 3544. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Duan, R.; Kranz, S.; Libuda, L.; Zhang, L. Development of a Dietary Index to Assess Overall Diet Quality for Chinese School-Aged Children: The Chinese Children Dietary Index. J. Acad. Nutr. Diet 2016, 116, 608–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Gong, Y.; Jia, P.; Zhang, J.; Xue, H.; Quan, L.; Tian, G.; Xiong, J.; Zheng, L.; Wang, Y.; et al. Monetary Diet Cost Is Positively Associated with Diet Quality and Obesity: An Analysis of School-Aged Children in Southwest China. J. Public Health 2019, 41, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Wang, Y.; Xie, W.; Zhang, J.; Ni, Y.; Peng, X.; Sun, G.; Dai, Y.; Zhou, Y. Multilevel Analysis of the Nutritional and Health Status among Children and Adolescents in Eastern China. Nutrients 2022, 14, 758. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, S.; Yin, H.; Chen, C.; Yang, Y.; Jiang, M.; Yang, L.; Guo, B.; Tang, H.; Zhang, Y.; et al. Nutrition and Health Survey of Children and Youth in Lishui District, Nanjing City. Wei Sheng Yan Jiu 2015, 44, 242–245+251. [Google Scholar]
- Zou, Y.; Zhang, R.-H.; Xia, S.-C.; Huang, L.-C.; Fang, Y.-Q.; Meng, J.; Chen, J.; Zhang, H.-X.; Zhou, B.; Ding, G.-Q. The Rural-Urban Difference in BMI and Anemia among Children and Adolescents. Int. J. Environ. Res. Public Health 2016, 13, 1020. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Zhang, R.; Huang, L.; Su, D.; He, M.; Fang, Y.; Zhao, D.; Wang, W.; Han, D. Sociodemographic Disparity in the Nutritional Status among Children and Adolescents in Zhejiang Province. Eur. J. Clin. Nutr. 2021, 75, 307–313. [Google Scholar] [CrossRef]
- Tang, Z.; Huang, S.; Ma, R.; Zheng, H.; Zhu, Y. Low Vitamin D Status Is Associated with Obesity but No Other Cardiovascular Risk Factors in Chinese Children and Adolescents. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1573–1581. [Google Scholar] [CrossRef]
- Lv, S.; Zhao, J.; Xu, D.; Chong, Z.; Jia, L.; Du, Y.; Ma, J.; Rutherford, S. An Epidemiological Survey of Children’s Iodine Nutrition and Goitre Status in Regions with Mildly Excessive Iodine in Drinking Water in Hebei Province, China. Public Health Nutr. 2012, 15, 1168–1173. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Ni Gedeli, A.; Fu, C.W.; Jiang, F.; Zhao, Q.; Wang, N.; Jiang, Q.W. A cohort study on the association between dynamics of thyroid volume and the changes of physical growth as well as the comparison of different thyroid volume indexes in school-aged children. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 1544–1548. [Google Scholar] [CrossRef]
- Kleiman-Weiner, M.; Luo, R.; Zhang, L.; Shi, Y.; Medina, A.; Rozelle, S. Eggs versus Chewable Vitamins: Which Intervention Can Increase Nutrition and Test Scores in Rural China? China Econ. Rev. 2013, 24, 165–176. [Google Scholar] [CrossRef]
- Wang, H.; Zhao, Q.; Boswell, M.; Rozelle, S. Can School Feeding Programs Reduce Malnutrition in Rural China? J. Sch. Health 2020, 90, 56–64. [Google Scholar] [CrossRef]
- Tao, C.; Zhao, Q.; Glauben, T.; Ren, Y. Does Dietary Diversity Reduce the Risk of Obesity? Empirical Evidence from Rural School Children in China. Int. J. Environ. Res. Public Health 2020, 17, 8122. [Google Scholar] [CrossRef]
- Cao, J.; Wei, X.; Tang, X.; Jiang, H.; Fan, Z.; Yu, Q.; Chen, J.; Liu, Y.; Li, T. Effects of Egg and Vitamin A Supplementation on Hemoglobin, Retinol Status and Physical Growth Levels of Primary and Middle School Students in Chongqing, China. Asia Pac. J. Clin. Nutr. 2013, 22, 214–221. [Google Scholar] [CrossRef]
- Shan, X.; Liu, C.; Luo, X.; Zou, Y.; Huang, L.; Zhou, W.; Qin, Q.; Mao, D.; Li, M.; Yang, L. Iodine Nutritional Status and Related Factors among Chinese School-Age Children in Three Different Areas: A Cross-Sectional Study. Nutrients 2021, 13, 1404. [Google Scholar] [CrossRef]
- Wang, X.; Hui, Z.; Dai, X.; Terry, P.D.; Zhang, Y.; Ma, M.; Wang, M.; Deng, F.; Gu, W.; Lei, S.; et al. Micronutrient-Fortified Milk and Academic Performance among Chinese Middle School Students: A Cluster-Randomized Controlled Trial. Nutrients 2017, 9, 226. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Ju, L.; Yang, Z.; Zhang, Q.; Gao, J.; Gong, D.; Guo, D.; Luo, S.; Zhao, W. Food Frequency Questionnaire for Chinese Children Aged 12-17 Years: Validity and Reliability. Biomed. Environ. Sci. 2019, 32, 486–495. [Google Scholar] [CrossRef]
- UNICEF. “Figure 1.1 Geographic Regions of China”. 2022. Available online: https://www.unicef.cn/en/figure-11-geographic-regions-china (accessed on 26 October 2021).
- Institute of Medicine (IOM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); National Academies Press: Washington, DC, USA, 2005; ISBN 030908525X. [Google Scholar]
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002.
- Moraleda, C.; Rabinovich, R.N.; Menéndez, C.; Menéndez, M. Perspective Piece Are Infants Less than 6 Months of Age a Neglected Group for Anemia Prevention in Low-Income Countries? Am. J. Trop. Med. Hyg. 2018, 98, 647–649. [Google Scholar] [CrossRef] [Green Version]
- Stevens, G.A.; Beal, T.; Mbuya, M.N.N.; Luo, H.; Neufeld, L.M.; Addo, O.Y.; Adu-Afarwuah, S.; Alayón, S.; Bhutta, Z.; Brown, K.H.; et al. Micronutrient Deficiencies among Preschool-Aged Children and Women of Reproductive Age Worldwide: A Pooled Analysis of Individual-Level Data from Population-Representative Surveys. Lancet Glob. Health 2022, 10, e1590–e1599. [Google Scholar] [CrossRef]
- Miniello, V.L.; Verga, M.C.; Miniello, A.; di Mauro, C.; Diaferio, L.; Francavilla, R. Complementary Feeding and Iron Status: “The Unbearable Lightness of Being” Infants. Nutrients 2021, 13, 4201. [Google Scholar] [CrossRef]
- Li, Q.; Tian, J.; Xu, F.; Binns, C. Breastfeeding in China: A Review of Changes in the Past Decade. Int. J. Environ. Res. Public Health 2020, 17, 8234. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Evaluating the Public Health Significance of Micronutrient Malnutrition. Part II; World Health Organization: Geneva, Switzerland, 2016.
- National Osteoporosis Society. A Practical Guide to Bone Densitometry in Children; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Zeng, Q.; Li, N.; Wang, Q.; Feng, J.; Sun, D.; Zhang, Q.; Huang, J.; Wen, Q.; Hu, R.; Wang, L.; et al. The Prevalence of Osteoporosis in China, a Nationwide, Multicenter DXA Survey. J. Bone Miner. Res. 2019, 34, 1789–1797. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.M.; Jakubikova, M.; Van’T Veer, P. Misreporting of Energy and Micronutrient Intake Estimated by Food Records and 24 Hour Recalls, Control and Adjustment Methods in Practice. Br. J. Nutr. 2009, 101 (Suppl. S2), S73–S85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biban, B.G.; Lichiardopol, C. Review Iodine Deficiency, Still a Global Problem? Curr. Health Sci. J. 2017, 43, 103–111. [Google Scholar] [CrossRef]
- FAO (Food Authority Organisation). Improving Diets and Nutrition: Food-Based Approaches; FAO: Rome, Italy, 2014. [Google Scholar]
- Geng, S.; Ma, J.; Liu, S.; Zhang, J.; Sheng, X. Lack of Dietary Diversity Contributes to the Gaps in Micronutrient Status and Physical Development between Urban and Rural Infants. Iran J. Public Health 2018, 47, 958–966. [Google Scholar]
- Chen, J.; Zhao, X.; Zhang, X.; Yin, S.; Piao, J.; Huo, J.; Yu, B.; Qu, N.; Lu, Q.; Wang, S.; et al. Studies on the Effectiveness of NaFeEDTA-Fortified Soy Sauce in Controlling Iron Deficiency: A Population-Based Intervention Trial. Food Nutr. Bull. 2005, 26, 177–186. [Google Scholar] [CrossRef]
- Gu, X.; Yin, S.; Xu, Q.; Gao, X.; Guangwen, T.; Russell, R.M. Vegetables Rich in Carotenoids on the Vitamin A Status of Children. J. Hyg. Res. 1999, 28, 224–226. [Google Scholar]
- Yin, S.; Gu, X.; Xu, Q.; Hu, S.; Zhao, X.; Gao, X.; Tang, G. Effect of Green and Yellow Vegetables on Serum Carotenoid in Children. Zhonghua Yu Fang Yi Xue Za Zhi 2000, 34, 89–91. [Google Scholar]
- FAO; Allen, L.; De Benoist, B.; Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients Food and Agricultural Organization of the United Nations Guidelines on Food Fortification with Micronutrients; FAO: Rome, Italy, 2006. [Google Scholar]




| Name of Study/Description/Reference | Year of Study | Provinces 1 | Age (yr) | Subject Number (n) | Outcome Indicator | Nutrients/Food |
|---|---|---|---|---|---|---|
| National studies | ||||||
| Chinese Nutrition and Health Surveillance (CNHS) 2013; Duan et al. (2020) [25], Pang et al. (2021) [26] | 2013 | Not named: 30 provinces | 2–4 | 14,850 |
|
|
| China Health and Nutrition Survey (CHNS) 2015; Jia et al. (2020) [27], Hu et al. (2021) [28], Zhao et al. (2021) [29] | 2015 | Beijing, Chongqing, Guangxi, Guizhou, Heilongjiang, Henan, Hubei, Hunan, Jiangsu, Liaoning, Shaanxi, Shandong, Shanghai, Yunnan, Zhejiang | 3–17 | 1122–1699 |
|
|
| Chinese Health Nutrition Survey (CHNS) 2010–2012 (Zhang et al. (2017), Younzi et al. (2018), Jinghuan et al. (2015), Li et al. (2017), Wang et al. (2017), Meng et al. (2018), Liu et al. (2017), Liu et al. (2016), Yang et al. (2015), Zhang et al. (2017), Zhang et al. (2017), Yang et al. (2017), Hu et al. (2017), Afeiche et al. (2018), Ding et al. (2022) [22,30,31,32,33,34,35,36,37,38,39,40,41,42,43] | 2010–2012 | Beijing, Chongqing, Guangxi, Guizhou, Heilongjiang, Henan, Hubei, Hunan, Jiangsu, Liaoning, Shaanxi, Shandong, Shanghai, Yunnan, Zhejiang | 3–18 | 335–33,016 |
|
|
| National School-based obesity intervention trial; Gui et al. (2017) [44] | 2013 | Liaoning, Tianjin, Ningxia, Shanghai, Chongqing, Hunan, Guangdong | 6–17 | 53,151 |
|
|
| National IDD surveillance (Liang et al. (2017), Wang et al. (2017) [45,46] | 2011 | Beijing, Chongqing, Guangxi, Guizhou, Heilongjiang, Henan, Hubei, Hunan, Jiangsu, Liaoning, Shaanxi, Shandong, Shanghai, Yunnan, Zhejiang | 8–10 | 15,003–130,000 |
|
|
| Chinese National Survey on Students Constitution and Health (CNSSCH) 2014; Yang et al. (2020) [47] | 2014 | Not named: 30 provinces | 9–14 | 48,537 |
|
|
| Chinese Environmental Exposure-Related Human Activity Patterns Survey (CEERHAPS-C); Guo et al. (2020) [48] | 2013–2016 | Not named: 30 provinces | 6–17 | 41,439 |
|
|
| Subnational | ||||||
| Nutrition Improvement Project on Children in Poor Areas of China (NIPCPAC); Feng et al. (2022) [49] | 2018 | Guizhou, Henan, Xinjiang, Hebei, and Hubei | 0.5–2 | 1522 |
|
|
| Maternal and health facility (Jia et al., 2015) [50] | 2012 | Beijing, Guangdong, Shanghai, Sichuan, Jiangsu | 0.5–2 | 750 |
|
|
| WFR, infants and young children, cross-sectional; Li et al. (2017) [51] | 2014 | Beijing, Guangdong, Hebei, Guangxi | 0.5–2 | 472 |
|
|
| Rural infants and young children intervention; Huo et al. (2015) [52] | 2010 | Sichuan, Shaanxi, Gansu | 0.5–2 | 1290 |
|
|
| Wenchuan Earthquake, infants and young children; Sun et al. (2013) [53] | 2010 | Sichuan, Shaanxi, Gansu | 0.5–2 | 1237 |
|
|
| Rural infants and young children, cross-sectional; Wang et al. (2017) [54] | 2011 | Gansu, Qinghai, Xinjiang, Sichuan, Guizhou, Yunnan, Tibet | 0.5–2 | 1938/3258 |
|
|
| Rural infants and toddlers, cross-sectional; Huang et al. (2019) [55] | 2018 | Qinghai | 0.5–2 | 856 |
|
|
| Rural infants and toddlers, complementary food supplements intervention; Zhang et al. (2016) [56] | 2012 | Qinghai | 0.5–2 | 804 |
|
|
| Rural infants and young children, complementary food supplements intervention; Dong et al. (2013) [57] | 2010–2011 | Gansu | 0.5–2 | 314 |
|
|
| Rural infants and young children, cross-sectional; Li et al. (2018) [58] | 2014 | Yunnan | 0.5–2 | 938 |
|
|
| Rural infants and young children, cross-sectional; (Yao et al., 2022) [59] | 2018 | Sichuan | 0.5–2 | 1522 |
|
|
| Dietary pattern and anemia; Zou et al. (2021) [60] | 2015 and 2018 | Hunan | 0.5–2 | 288 |
|
|
| Rural children, micronutrient powder intervention; Luo et al. (2017) [61] | 2013 | Shaanxi | 0.5–2.5 | 610 |
|
|
| Maternal and Infant Nutrition and Growth (MING) study; Li et al. (2017), Ma et al. (2014) [62,63] | 2011–2012 | Beijing, Guangdong, Shanghai, Sichuan, Gansu, Liaoning, Henan, Jiangsu | 0.5–3 | 1078 |
|
|
| Rural Mixed Methods Analysis Infants and Toddlers Study; Wang et al. (2018) [64] | 2015–2017 | Shaanxi, Hebei, Yunnan, Guizhou, Henan, Beijing | 0.5–3 | 20,909 |
|
|
| Rural early childhood development Intervention; Shi et al. (2020) [65], Zhao et al. (2021) [66] | 2013 | Guizhou, Shanxi | 0.5–3 | 2236 |
|
|
| Rural infants and young children, Yingyanboa intervention (Wang et al. (2015), Wang et al. (2017) [67,68] | 2010 | Yunnan, Guizhou, Shaanxi | 0–3 | 1370 |
|
|
| Vitamin A supplementation, Chongqing; Liu et al. (2021) [69] | 2018 | Chongqing | 0–5 | 1016 |
|
|
| Pre-school children, Health Examination Centers and Children Hospital; Zhang et al. (2020) [70] | 2016 | Chongqing | 0–6 | 6953 |
|
|
| Children, south China, cross-sectional; Guo et al. (2018) [71] | 2016–2017 | Guangdong | 0–6 | 16,755 |
|
|
| Children, association of Vit D with bone density; Fu et al. (2016) [72] | 2014–2015 | Jiangsu | 0–7 | 4532 |
|
|
| Outpatient children, hospital of Harbin; Wei et al. (2018) [73] | 2014–2016 | Heilongjiang | 0–12 | 9795 |
|
|
| Northeast Chinese Children, Serum cross-sectional; Chen et al. (2018) [74] | 2017 | Jilin | 0–12 | 2096 |
|
|
| Urban children, cross-sectional; Chang et al. (2014) [75] | 2011 | Sichuan | 0.5–14 | 1218 |
|
|
| Hospital-based cross-sectional study; 18 provinces; Yang et al. (2020) [76] | 2016–2018 | Inner Mongolia, Yunnan, Sichuan, Shaanxi, Guangxi, Beijing, Liaoning, Hebei, Shandong, Jiangsu, Zhejiang, Guangdong, Heilongjiang, Anhui, Hubei, Henan, Hunan | 0–18 | 460,567 |
|
|
| Semi-quantitative FFQ validation, young children, 24HR (3 days); Ma et al. (2022) [77] | 2019 | Shaanxi, Qinghai, Gansu | 2–6 | 326 |
|
|
| 12 cities central and western China; Chen et al. (2021) [78] | 2019 | Chongqing, Guizhou, Yunnan, Sichuan, Fujian, Shaanxi, Qinghai, Xinjiang | 2–16 | 2194 |
|
|
| Rural children, toxic metals, cross-sectional; Tian et al. (2020) [79] | 2013 | Hebei | 3–5 | 80 |
|
|
| Urban pre-school children, Vitamin A supplement intervention; Chen et al. (2014) [80] | 2011 | Sichuan | 3–6 | 500 |
|
|
| Pre-school children, cross-sectional; Peng et al. (2014) [81] | 2012 | Chongqing | 3–6 | 492 |
|
|
| Nutrition Study of Pre-school Children and School Child; Ma et al. (2014), Zhao et al. (2017), Xue et al. (2015), Liu et al. (2018) [82,83,84,85] | 2011–2012 | Beijing, Guangdong, Sichuan, Liaoning, Gansu, Henan, Jiangsu, Hebei | 3–12 | 423–1866 |
|
|
| Rural vs. urban, children and adolescents, universal salt iodization policy; Zou et al. (2014) [86] | 2014 | Zhejiang | 3–18 | 1970 |
|
|
| Rural school-children, food insecurity, cross-sectional; Shen et al. (2015) [87] | 2011 | Guangxi, Yunnan | 6–14 | 1583 |
|
|
| China Child and Adolescent Cardiovascular Health (CCACH) 2012–2015; Yan et al. (2019), Li et al. (2020), Xiao et al. (2020) [88,89,90] | 2012–2015 | Beijing, Jilin, Shandong, Ningxia, Shanghai, Chongqing, Sichuan | 6–18 | 10,696–12,618 |
|
|
| School children, northwest Chinese City, cross-sectional; Li et al. (2018) [91] | 2015 | Ningxia | 6–18 | 1582 |
|
|
| Rural, egg and milk supplementation; Zhao et al. (2021) [92] | 2013–2015 | Guangxi | 7–8 | 818 |
|
|
| The Dietary Quality During Childhood (DQDC), cross-sectional; Cheng et al. (2016), Zhang et al. (2019) [93,94] | 2013 | Sichuan | 7–14 | 1719–2043 |
|
|
| Chinese Nutrition and Health Surveillance 206-17, cross-sectional; Tian et al. (2022) [95] | 2016–2017 | Jiangsu | 7–17 | 335 |
|
|
| Rural, FFQ, cross-sectional; Zhou et al. (2015) [96] | 2012–2013 | Jiangsu | 7–17 | 516 |
|
|
| Rural vs. urban, children and adolescent, sub-set from CHNS 2011–2013; Zou et al. (2016) [97] | 2011–2012 | Zhejiang | 7–17 | 1534 |
|
|
| Rural vs. urban, sub-set from CHNS 2011–2013; Zou et al. (2021) [98] | 2016–2017 | Zhejiang | 6–12 | 2818 |
|
|
| Children and adolescents, sub-set of the national School Obesity Intervention; Tang et al. (2020) [99] | 2013 | Guangdong | 7–18 | 2680 |
|
|
| School-children, cross-sectional survey; Lv et al. (2012) [100] | 2010 | Hebei | 8–10 | 1200 |
|
|
| School-age children, cohort study; Wang et al. (2018) [101] | 2012 | Zhejiang | 8–10 | 784 |
|
|
| Rural children, eggs vs. chewable vitamins intervention; Weiner et al. (2013) [102] | 2010 | Gansu | 9–12 | 2000 |
|
|
| Rural school-children, school feeding program intervention; Wang et al. (2020) [103] | 2012 | Qinghai, Gansu, Shaanxi, Ningxia | 10–12 | 8411 |
|
|
| Rural school children, cross-sectional study; Tao et al. (2022) [104] | 2018 | Anhui, Yunnan, Henan | 10–13 | 8690 |
|
|
| Rural school-children, eggs vs. vitamin A supplement intervention; Cao et al. (2013) [105] | 2010–2011 | Chongqing | 10–18 | 288 |
|
|
| Iodine, 3 provinces; Shan et al. (2021) [106] | 2016 | Hebei, Guangxi, Zhejiang | 11–12 | 3808 |
|
|
| School-children, micronutrient-fortified milk intervention; Wang et al. (2017) [107] | 2015 | Shaanxi | 12–14 | 137 |
|
|
| Semi-quantitative FFQ validation, adolescents ; Liu et al. (2019) [108] | 2018 | Beijing, Chongqing | 12–17 | 160 |
|
|
| Age (yrs) | Energy Intake | Fat Intake | |||
|---|---|---|---|---|---|
| EER kcal/day (Female/Male) | Mean Intake (kcal/day) | Recommended % EI | Mean Intake (g/day) | %EI | |
| 0 | 549 b | 71–103 Ma et al. (2014) [63] | 48 (AI) | 24.7–28.3 Ma et al. (2014) [63] | 18–21 b,c |
| 0.5 | 684 b | 744 Li et al. (2017) [62] | 40 (AI) | 25.7 Li et al. (2017) [62] | 15 b,c |
| 1 | 900/800 | 1146 Li et al. (2017) [62] | 35(AI) | 39.4–44.6 + Li et al. (2017) [62], Ma et al. (2022) [77] | 18–19 b,c |
| 2 | 1100/1000 | 1184–1523 + (Li et al., 2017) [62], Ma et al. (2022) [77] | 20–30 | ||
| 3 | 1250/1200 | 1523 +–1553 Ma et al. (2022) [77], Meng et al. (2018) [42] | 20–30 | ||
| 4 | 1300/1250 | 1299–1628 a Zhang et al. (2017) [38], Meng et al. (2018) [42], Xue et al. (2015) [84], Ma et al. (2022) [77] | 20–30 | 44.6 + Ma et al. (2022) [77] | 37 a Zhang et al. (2017) [38] |
| 5 | 1400/1300 | 1299–1628 a Zhang et al. (2017) [38], Zhao et al. (2021) [29], Meng et al. (2018) [42], Xue et al. (2015) [84], Ma et al. (2022) [77] | 20–30 | ||
| 6 | 1600/1450 | 1299–1672 a Zhang et al. (2017) [38], Zhao et al. (2021) [29], Meng et al. (2018) [42], Xue et al. (2015) [84], Ma et al. (2022) [77] | 20–30 | ||
| 7 | 1700/1550 | 1416–1672 a Zhang et al. (2017) [38], Zhao et al. (2021) [29], Meng et al. (2018) [42] | 20–30 | 52.6–66.2 a Zhang et al. (2017) [38], Zhao et al. (2021) [29] | 37–38 a Zou et al. (2016) [97], Zhang et al. (2017) [38], Zhao et al. (2021) [29] |
| 8 | 1850/1700 | 1416–1672 a Zhang et al. (2017) [38], Zhao et al. (2021) [29], Meng et al. (2018) [42] | 20–30 | 30.5–39.4 Zhang et al. (2017) [38], Zhao et al. (2021) [29] | |
| 9 | 2000/1800 | 1416–1672 a Zhang et al. (2017) [38], Zhao et al. (2021) [29] | 20–30 | ||
| 10 | 2050/1900 | 1416–1672a Zhang et al. (2017) [38], Zhao et al. (2021) [29], Meng et al. (2018) [42] | 20–30 | ||
| 11 | 2350/2050 | 1417–2050 Zou et al. (2016) [97], Lui et al. (2019) [108], Zhang et al. (2017) [38] Zhao et al. (2021) [29], Yunzi et al. (2018) [39], Meng et al. (2018) [42] | 20–30 | 52.6–66.2 a | 36–37 a,c Zou et al. (2016) [97], Lui et al. (2019) [108], Zhang et al. (2017) [38], Zhao et al. (2021) [29] |
| 14–17 | 2850/2300 | 1416–2050 Zou et al. (2016) [97], Lui et al. (2019) [108], Zhang et al. (2017) [38], Zhao et al. (2021) [29], Yunzi et al. (2018) [39], Meng et al. (2018) [42] | 20–30 | 52.6–66.2 a | 32–37 a,c Zou et al. (2016) [97], Lui et al. (2019) [108], Zhang et al. (2017) [38] Zhao et al. (2021) [29] |
| Nutrient | Age (Years) | 0–0.4 | 0.5–0.9 | 1–3.9 | 4–6.9 | 7–10.9 | 11–13.9 | 14–17 |
|---|---|---|---|---|---|---|---|---|
| Anemia | % prevalence | 46 | 17–86 | 4–30 | 5.5 a–21 | 4.3 ab–21 | 7.2 ab–21 | 7.2 ab–21 |
| Iron | % deficiency | - | 48–62 | 10–62 | 10–38 | 8–18 | 7.3–9.4 | 7.3–8.3 |
| Mean intake (mg/day) | 3.1–4.8 | 6.6–8.7 | 8.8–23.7 + | 11.2 a–23.7 + | 14.0 a–30.4 | 17.4 a–30.4 | 19.5 a–30.4 | |
| % inadequacy | 9.7 a | 18 a | 24 a | 19 a | ||||
| Zinc | % deficiency | 4–10 a | 4 | 4 | ||||
| Mean intake (mg/day) | 3.1–4.5 | 4.0–4.8 | 4.8–7.7 | 6.3 ab–9.3 | 7.7 a–12.5 | 8.5 ab–12.5 | 8.5 ab–12.5 | |
| % inadequacy | 0.4–19 | 24 a | 28 a–56 | 30 a–56 | 30 a–56 | |||
| Selenium | % deficiency | 44 a | 3.1–3.6 | |||||
| Mean intake (mg/day) | 15.4–18.6 + | 27 ab–31.1 | 33.8 a–70.0 | 32.2 a–33.8 a | 33.8 a–38.1 a | 36 a–45.6 a | ||
| % inadequacy | 51 a | 53 a–64 a | 71 a | 73 a | ||||
| Calcium | Mean intake (mg/day) | 322–487 | 355–577 | 413–801 a | 236 a–642 | 273 a–741 | 306 a–741 | 306 a–741 |
| % inadequacy | 97 a | 98 a | 99 a | 97 a | ||||
| Magnesium | Mean intake (mg/day) | - | 112 | 153–369 + | 203 a–369 + | 203 a–214 a | 203 a–278 a | 214 a–278 a |
| Sodium | Mean intake (mg/day) | 57–76 | 518 | 571 +–2470 | 3148 ab–4370 | 3787 a–3360 ab | 4228 a–4400 | 3360–4849 a |
| Nutrient | Age (Years) | 0–0.4 b | 0.5–0.9 b | 1–3.9 | 4–6.9 | 7–10.9 | 11–13.9 | 14–17 |
|---|---|---|---|---|---|---|---|---|
| Vit A | % deficiency % VAI | 21–88 11.2–43 | 20–21 40–58 | 0–21 43–54 | 8.9–20 39–44 | 6.6 ac–27 a 17 ac–38 | 0.9–27 a 15 | 4.5–27 a 14 a–21 a |
| Mean intake (µg/day) | 620–709 | 455–670 | 432–867 | 482–522 a | 227–624 a | 223–661 a | 227–769 a | |
| % inadequacy | 0.4–24 | 25 a | 31 a–70 a | 42 a–70 a | 3–70 a | |||
| Vit B1 | Mean intake (mg/day) | 0.2–0.5 | 0.3–0.5 | 0.3–0.8 + | 0.5 a–0.8 | 0.9–0.7 a | 0.6–0.7 a | 0.8 a–1.2 |
| % inadequacy | 68 a | 75 a–79 a | 75 a–89 a | 75 a–92 a | ||||
| Vit B2 | Mean intake (mg/day) | 0.6–0.9 | 0.8–1.1 | 1.0–1.4 + | 0.5 a–1.4 + | 0.5–0.6 a | 0.67 a–1.0 | 0.67 a–1.0 |
| % inadequacy | 66 a | 77 a | 84 a | 86 a | ||||
| Vit B3 | Mean intake (mg/day) | 2.1–2.9 | 4.2–4.6 | 5.8–16 + | 11–16 + | 9.5–10 a | 9.5–10 a | 9.5–15 a |
| % inadequacy | ||||||||
| Vit C | Mean intake (mg/day) | 58–76 | 45–54 | 59–88 | 43 a–75 + | 28–61 a | 25–64 a | 25–66 a |
| % inadequacy | 54 a | 58 a–65 a | 65 a–69 a | 65 a–76 a | ||||
| Vit D | % deficiency | 0–28 | 0–28 | 0–34 | 1–58 | 1.8–41 a | 1.8–50 a | 1.8–52 a |
| Population Group (Years) | Measure | Milk and Milk Products | Beans, Nuts, and Seeds | Red Meat | Poultry | Seafood | Eggs | Fruits | Vegetables | Cereals, Tubers, and Legumes |
|---|---|---|---|---|---|---|---|---|---|---|
| Recommended g/day | 300 | 25–35 | 40–75 | 40–75 | 40–75 | 40–50 | 200–350 | 300–500 | 250–400 | |
| General (3–4) a [27] (5–8) a [27] (7–15) b [108] (7–17) e [93] | g/day (mean) | 61 | - | |||||||
| 41 | - | |||||||||
| 230 | 28 c | 113 | 24 | 0 | 20 | 96 | 127 | 277 d | ||
| 200 | - | 129 | - | 13 | 34 | 142 | 154 | 550 | ||
| (3–4) a [27] (5–8) a [27] | % below recommended | 96–99 | - | - | - | - | - | - | - | - |
| Highly urban (4–17) a [38] | g/day mean (SE) | 120 (4) | - | 223 (9) | 74 (4) | 40 (2) | 65 (2) | - | - | - |
| Moderately urban (4–17) a [38] | g/day mean (SE) | 116 (14) | - | 200 (0.4) | 72 (4) | 38 (2) | 51 (2) | - | - | - |
| Rural (4–17) a [38] | g/day mean (SE) | 99 (9) | - | 181 (5) | 71 (4) | 33 (1) | 50 (1) | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayling, K.; Li, R.; Muhardi, L.; Melse-Boonstra, A.; Sun, Y.; Chen, W.; Kudla, U. Systematic Literature Review of the Nutrient Status, Intake, and Diet Quality of Chinese Children across Different Age Groups. Nutrients 2023, 15, 1536. https://doi.org/10.3390/nu15061536
Ayling K, Li R, Muhardi L, Melse-Boonstra A, Sun Y, Chen W, Kudla U. Systematic Literature Review of the Nutrient Status, Intake, and Diet Quality of Chinese Children across Different Age Groups. Nutrients. 2023; 15(6):1536. https://doi.org/10.3390/nu15061536
Chicago/Turabian StyleAyling, Katie, Rongrong Li, Leilani Muhardi, Alida Melse-Boonstra, Ye Sun, Wei Chen, and Urszula Kudla. 2023. "Systematic Literature Review of the Nutrient Status, Intake, and Diet Quality of Chinese Children across Different Age Groups" Nutrients 15, no. 6: 1536. https://doi.org/10.3390/nu15061536
APA StyleAyling, K., Li, R., Muhardi, L., Melse-Boonstra, A., Sun, Y., Chen, W., & Kudla, U. (2023). Systematic Literature Review of the Nutrient Status, Intake, and Diet Quality of Chinese Children across Different Age Groups. Nutrients, 15(6), 1536. https://doi.org/10.3390/nu15061536